Instability of Non-Standard Microsatellites in Relation to Prognosis in Metastatic Colorectal Cancer Patients

 , , , , , , ,
, , , , , , ,  and
and
Abstract
:1. Introduction
2. Results
2.1. Patient Characteristics
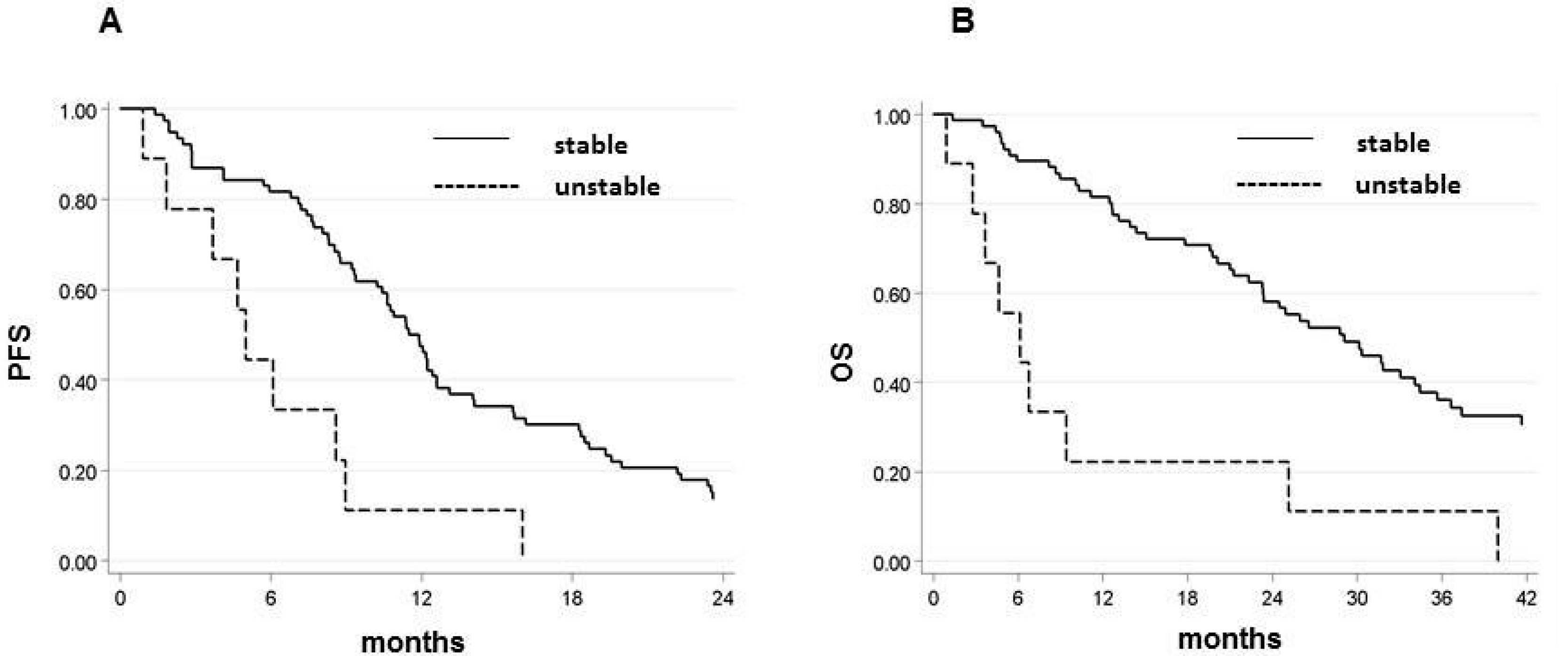
2.2. Microsatellite Status and Its Relation with Outcome
2.3. EMAST Frequency and Patient Outcomes
2.4. Amplification of VEGF-B Microsatellite Showed a Tendency to Associate with Decreased Survival in Response to Chemotherapy
3. Discussion
4. Materials and Methods
4.1. Case Series
4.2. Genomic DNA Extraction
4.3. Microsatellite Instability Assay
4.4. Elevate Microsatellite Alterations at Selected Tetranucleotide Repeats (EMAST) Assay
4.5. VEGF-B Frameshift Mutation and Microsatellite Instability
4.6. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 2015, 136, E359–E386. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Fedewa, S.A.; Ahnen, D.J.; Meester, R.G.S.; Barzi, A.; Jemal, A. Colorectal cancer statistics, 2017. CA Cancer J. Clin. 2017, 67, 177–193. [Google Scholar] [CrossRef] [PubMed]
- Nappi, A.; Berretta, M.; Romano, C.; Tafuto, S.; Cassata, A.; Casaretti, R.; Silvestro, L.; De Divitiis, C.; Alessandrini, L.; Fiorica, F.; et al. Metastatic colorectal cancer: Role of target therapies and future perspectives. Curr. Cancer Drug Targets 2018, 18, 421–429. [Google Scholar] [CrossRef] [PubMed]
- Cidon, E.U.; Alonso, P.; Masters, B. Markers of response to antiangiogenic therapies in colorectal cancer: Where are we now and what should be next? Clin. Med. Insights Oncol. 2016, 10, 41–55. [Google Scholar] [CrossRef] [Green Version]
- Aaltonen, L.A.; Peltomaki, P.; Leach, F.S.; Sistonen, P.; Pylkkanen, L.; Mecklin, J.P.; Jarvinen, H.; Powell, S.M.; Jen, J.; Hamilton, S.R. Clues to the pathogenesis of familial colorectal cancer. Science 1993, 260, 812–816. [Google Scholar] [CrossRef] [PubMed]
- Miyakura, Y.; Sugano, K.; Akasu, T.; Yoshida, T.; Maekawa, M.; Saitoh, S.; Sasaki, H.; Nomizu, T.; Konishi, F.; Fujita, S.; et al. Extensive but hemiallelic methylation of the hMLH1 promoter region in early-onset sporadic colon cancers with microsatellite instability. Clin. Gastroenterol. Hepatol. 2004, 2, 147–156. [Google Scholar] [CrossRef]
- Herman, J.G.; Baylin, S.B. Gene silencing in cancer in association with promoter hypermethylation. N. Engl. J. Med. 2003, 349, 2042–2054. [Google Scholar] [CrossRef] [PubMed]
- Koopman, M.; Kortman, G.A.M.; Mekenkamp, L.; Ligtenberg, M.J.L.; Hoogerbrugge, N.; Antonini, N.F.; Punt, C.J.A.; van Krieken, J.H.J.M. Deficient mismatch repair system in patients with sporadic advanced colorectal cancer. Br. J. Cancer 2009, 100, 266–273. [Google Scholar] [CrossRef] [Green Version]
- Vilar, E.; Gruber, S.B. Microsatellite instability in colorectal cancer-the stable evidence. Nat. Rev. Clin. Oncol. 2010, 7, 153–162. [Google Scholar] [CrossRef] [Green Version]
- Sinicrope, F.A.; Rego, R.L.; Foster, N.; Sargent, D.J.; Windschitl, H.E.; Burgart, L.J.; Witzig, T.E.; Thibodeau, S.N. Microsatellite instability accounts for tumor site-related differences in clinicopathologic variables and prognosis in human colon cancers. Am. J. Gastroenterol. 2006, 101, 2818–2825. [Google Scholar] [CrossRef]
- Gryfe, R.; Kim, H.; Hsieh, E.T.; Aronson, M.D.; Holowaty, E.J.; Bull, S.B.; Redston, M.; Gallinger, S. Tumor microsatellite instability and clinical outcome in young patients with colorectal cancer. N. Engl. J. Med. 2000, 342, 69–77. [Google Scholar] [CrossRef] [PubMed]
- Popat, S.; Hubner, R.; Houlston, R.S. Systematic review of microsatellite instability and colorectal cancer prognosis. J. Clin. Oncol. 2005, 23, 609–618. [Google Scholar] [CrossRef] [PubMed]
- Jover, R.; Castells, A.; Llor, X.; Andreu, M. Predictive value of microsatellite instability for benefit from adjuvant fluorouracil chemotherapy in colorectal cancer. Gut 2006, 55, 1819–1820. [Google Scholar] [CrossRef] [PubMed]
- Pogue-Geile, K.; Yothers, G.; Taniyama, Y.; Tanaka, N.; Gavin, P.; Colangelo, L.; Blackmon, N.; Lipchik, C.; Kim, S.R.; Sharif, S.; et al. Defective mismatch repair and benefit from bevacizumab for colon cancer: Findings from NSABP C-08. J. Natl. Cancer Inst. 2013, 105, 989–992. [Google Scholar] [CrossRef] [Green Version]
- Kerr, R.S.; Love, S.; Segelov, E.; Johnstone, E.; Falcon, B.; Hewett, P.; Weaver, A.; Church, D.; Scudder, C.; Pearson, S.; et al. Adjuvant capecitabine plus bevacizumab versus capecitabine alone in patients with colorectal cancer (QUASAR 2): An open-label, randomised phase 3 trial. Lancet. Oncol. 2016, 17, 1543–1557. [Google Scholar] [CrossRef]
- Kim, S.T.; Kim, H.K.; Lee, J.; Park, S.H.; Lim, H.Y.; Park, Y.S.; Kang, W.K.; Park, J.O. The impact of microsatellite instability status and sidedness of the primary tumor on the effect of bevacizumab-containing chemotherapy in patients with metastatic colorectal cancer. J. Cancer 2018, 9, 1791–1796. [Google Scholar] [CrossRef] [Green Version]
- Innocenti, F.; Ou, F.-S.; Qu, X.; Zemla, T.J.; Niedzwiecki, D.; Tam, R.; Mahajan, S.; Goldberg, R.M.; Bertagnolli, M.M.; Blanke, C.D.; et al. Mutational analysis of patients with colorectal cancer in CALGB/SWOG 80405 identifies new roles of microsatellite instability and tumor mutational burden for patient outcome. J. Clin. Oncol. 2019, 37, 1217–1227. [Google Scholar] [CrossRef]
- Carethers, J.M. Microsatellite instability pathway and EMAST in colorectal cancer. Curr. Colorectal Cancer Rep. 2017, 13, 73–80. [Google Scholar] [CrossRef] [Green Version]
- Devaraj, B.; Lee, A.; Cabrera, B.L.; Miyai, K.; Luo, L.; Ramamoorthy, S.; Keku, T.; Sandler, R.S.; McGuire, K.L.; Carethers, J.M. Relationship of EMAST and microsatellite instability among patients with rectal cancer. J. Gastrointest. Surg. 2010, 14, 1521–1528. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.-Y.; Chung, H.; Devaraj, B.; Iwaizumi, M.; Han, H.S.; Hwang, D.-Y.; Seong, M.K.; Jung, B.H.; Carethers, J.M. Microsatellite alterations at selected tetranucleotide repeats are associated with morphologies of colorectal neoplasias. Gastroenterology 2010, 139, 1519–1525. [Google Scholar] [CrossRef] [Green Version]
- Garcia, M.; Choi, C.; Kim, H.-R.; Daoud, Y.; Toiyama, Y.; Takahashi, M.; Goel, A.; Boland, C.R.; Koi, M. Association between recurrent metastasis from stage II and III primary colorectal tumors and moderate microsatellite instability. Gastroenterology 2012, 143, 48–50.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carethers, J.M.; Koi, M.; Tseng-Rogenski, S.S. EMAST is a form of microsatellite instability that is initiated by inflammation and modulates colorectal cancer progression. Genes 2015, 6, 185–205. [Google Scholar] [CrossRef] [Green Version]
- Watson, M.M.; Lea, D.; Rewcastle, E.; Hagland, H.R.; Soreide, K. Elevated microsatellite alterations at selected tetranucleotides in early-stage colorectal cancers with and without high-frequency microsatellite instability: Same, same but different? Cancer Med. 2016, 5, 1580–1587. [Google Scholar] [CrossRef] [Green Version]
- Hamaya, Y.; Guarinos, C.; Tseng-Rogenski, S.S.; Iwaizumi, M.; Das, R.; Jover, R.; Castells, A.; Llor, X.; Andreu, M.; Carethers, J.M. Efficacy of adjuvant 5-fluorouracil therapy for patients with EMAST-positive stage II/III colorectal cancer. PLoS ONE 2015, 10, e0127591. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Zhang, Y.; Hosaka, K.; Andersson, P.; Wang, J.; Tholander, F.; Cao, Z.; Morikawa, H.; Tegner, J.; Yang, Y.; et al. VEGF-B promotes cancer metastasis through a VEGF-A-independent mechanism and serves as a marker of poor prognosis for cancer patients. Proc. Natl. Acad. Sci. USA 2015, 112, E2900–E2909. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhattacharya, R.; Fan, F.; Wang, R.; Ye, X.; Xia, L.; Boulbes, D.; Ellis, L.M. Intracrine VEGF signalling mediates colorectal cancer cell migration and invasion. Br. J. Cancer 2017, 117, 848–855. [Google Scholar] [CrossRef] [Green Version]
- Apte, R.S.; Chen, D.S.; Ferrara, N. VEGF in signaling and disease: Beyond discovery and development. Cell 2019, 176, 1248–1264. [Google Scholar] [CrossRef] [Green Version]
- Giannakis, M.; Mu, X.J.; Shukla, S.A.; Qian, Z.R.; Cohen, O.; Nishihara, R.; Bahl, S.; Cao, Y.; Amin-Mansour, A.; Yamauchi, M.; et al. Genomic correlates of immune-cell infiltrates in colorectal carcinoma. Cell Rep. 2016, 15, 857–865. [Google Scholar] [CrossRef] [Green Version]
- Jass, J.R.; Do, K.A.; Simms, L.A.; Iino, H.; Wynter, C.; Pillay, S.P.; Searle, J.; Radford-Smith, G.; Young, J.; Leggett, B. Morphology of sporadic colorectal cancer with DNA replication errors. Gut 1998, 42, 673–679. [Google Scholar] [CrossRef]
- Liang, J.-T.; Huang, K.-C.; Lai, H.-S.; Lee, P.-H.; Cheng, Y.-M.; Hsu, H.-C.; Cheng, A.-L.; Hsu, C.-H.; Yeh, K.-H.; Wang, S.-M.; et al. High-frequency microsatellite instability predicts better chemosensitivity to high-dose 5-fluorouracil plus leucovorin chemotherapy for stage IV sporadic colorectal cancer after palliative bowel resection. Int. J. Cancer 2002, 101, 519–525. [Google Scholar] [CrossRef]
- Fallik, D.; Borrini, F.; Boige, V.; Viguier, J.; Jacob, S.; Miquel, C.; Sabourin, J.-C.; Ducreux, M.; Praz, F. Microsatellite instability is a predictive factor of the tumor response to irinotecan in patients with advanced colorectal cancer. Cancer Res. 2003, 63, 5738–5744. [Google Scholar] [PubMed]
- Des Guetz, G.; Lecaille, C.; Mariani, P.; Bennamoun, M.; Uzzan, B.; Nicolas, P.; Boisseau, A.; Sastre, X.; Cucherousset, J.; Lagorce, C.; et al. Prognostic impact of microsatellite instability in colorectal cancer patients treated with adjuvant FOLFOX. Anticancer Res. 2010, 30, 4297–4301. [Google Scholar] [PubMed]
- Serrano, P.E.; Gu, C.-S.; Husien, M.; Jalink, D.; Ritter, A.; Martel, G.; Tsang, M.E.; Law, C.H.; Hallet, J.; McAlister, V.; et al. Risk factors for survival following recurrence after first liver resection for colorectal cancer liver metastases. J. Surg. Oncol. 2019, 120, 1420–1426. [Google Scholar] [CrossRef] [PubMed]
- Tseng-Rogenski, S.S.; Chung, H.; Wilk, M.B.; Zhang, S.; Iwaizumi, M.; Carethers, J.M. Oxidative stress induces nuclear-to-cytosol shift of hMSH3, a potential mechanism for EMAST in colorectal cancer cells. PLoS ONE 2012, 7, e50616. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jia, W.-H.; Zhang, B.; Matsuo, K.; Shin, A.; Xiang, Y.-B.; Jee, S.H.; Kim, D.-H.; Ren, Z.; Cai, Q.; Long, J.; et al. Genome-wide association analyses in East Asians identify new susceptibility loci for colorectal cancer. Nat. Genet. 2013, 45, 191–196. [Google Scholar] [CrossRef]
- Zheng, X.; Wang, L.; Zhu, Y.; Guan, Q.; Li, H.; Xiong, Z.; Deng, L.; Lu, J.; Miao, X.; Cheng, L. The SNP rs961253 in 20p12.3 is associated with colorectal cancer risk: A case-control study and a meta-analysis of the published literature. PLoS ONE 2012, 7, e34625. [Google Scholar] [CrossRef]
- Tanskanen, T.; van den Berg, L.; Valimaki, N.; Aavikko, M.; Ness-Jensen, E.; Hveem, K.; Wettergren, Y.; Bexe Lindskog, E.; Tonisson, N.; Metspalu, A.; et al. Genome-wide association study and meta-analysis in Northern European populations replicate multiple colorectal cancer risk loci. Int. J. Cancer 2018, 142, 540–546. [Google Scholar] [CrossRef]
- Kambara, T.; Sharp, G.B.; Nagasaka, T.; Takeda, M.; Sasamoto, H.; Nakagawa, H.; Isozaki, H.; MacPhee, D.G.; Jass, J.R.; Tanaka, N.; et al. Allelic loss of a common microsatellite marker MYCL1: A useful prognostic factor of poor outcomes in colorectal cancer. Clin. Cancer Res. 2004, 10, 1758–1763. [Google Scholar] [CrossRef] [Green Version]
- Ogunbiyi, O.A.; Goodfellow, P.J.; Gagliardi, G.; Swanson, P.E.; Birnbaum, E.H.; Fleshman, J.W.; Kodner, I.J.; Moley, J.F. Prognostic value of chromosome 1p allelic loss in colon cancer. Gastroenterology 1997, 113, 761–766. [Google Scholar] [CrossRef]
- Jass, J.R.; Young, J.; Leggett, B.A. Biological significance of microsatellite instability-low (MSI-L) status in colorectal tumors. Am. J. Pathol. 2001, 158, 779–781. [Google Scholar] [CrossRef] [Green Version]
- Hatch, S.B.; Farber, R.A. Mutation rates in the complex microsatellite MYCL1 and related simple repeats in cultured human cells. Mutat. Res. 2004, 545, 117–126. [Google Scholar] [CrossRef] [PubMed]
- Vauhkonen, H.; Vauhkonen, M.; Sajantila, A.; Sipponen, P.; Knuutila, S. Characterizing genetically stable and unstable gastric cancers by microsatellites and array comparative genomic hybridization. Cancer Genet. Cytogenet. 2006, 170, 133–139. [Google Scholar] [CrossRef] [PubMed]
- Koch, S.; Claesson-Welsh, L. Signal transduction by vascular endothelial growth factor receptors. Cold Spring Harb. Perspect. Med. 2012, 2, a006502. [Google Scholar] [CrossRef] [PubMed]
- Boucher, J.M.; Clark, R.P.; Chong, D.C.; Citrin, K.M.; Wylie, L.A.; Bautch, V.L. Dynamic alterations in decoy VEGF receptor-1 stability regulate angiogenesis. Nat. Commun. 2017, 8, 15699. [Google Scholar] [CrossRef]
- Hansen, T.F.; Jensen, L.H.; Spindler, K.L.G.; Lindebjerg, J.; Brandslund, I.; Jakobsen, A. The relationship between serum vascular endothelial growth factor A and microsatellite instability in colorectal cancer. Color. Dis. 2011, 13, 984–988. [Google Scholar] [CrossRef]
- De Smedt, L.; Lemahieu, J.; Palmans, S.; Govaere, O.; Tousseyn, T.; Van Cutsem, E.; Prenen, H.; Tejpar, S.; Spaepen, M.; Matthijs, G.; et al. Microsatellite instable vs stable colon carcinomas: Analysis of tumour heterogeneity, inflammation and angiogenesis. Br. J. Cancer 2015, 113, 500–509. [Google Scholar] [CrossRef] [Green Version]
- Kloor, M.; Staffa, L.; Ahadova, A.; Von Knebel Doeberitz, M. Clinical significance of microsatellite instability in colorectal cancer. Langenbeck’s Arch. Surg. 2014, 399, 23–31. [Google Scholar] [CrossRef]
- Choi, M.R.; Yoo, N.J.; Lee, S.H.; An, C.H. Frameshift Mutation of an Angiogenesis Factor VEGFB and its Mutational Heterogeneity in Colorectal Cancers. Pathol. Oncol. Res. 2015, 21, 853–855. [Google Scholar] [CrossRef]
- Umar, A.; Boland, C.R.; Terdiman, J.P.; Syngal, S.; de la Chapelle, A.; Ruschoff, J.; Fishel, R.; Lindor, N.M.; Burgart, L.J.; Hamelin, R.; et al. Revised Bethesda Guidelines for hereditary nonpolyposis colorectal cancer (Lynch syndrome) and microsatellite instability. J. Natl. Cancer Inst. 2004, 96, 261–268. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Overall (n = 141) | CT + B Arm (n = 90) | CT Arm (n = 51) | |
|---|---|---|---|
| No. (%) | No. (%) | No. (%) | |
| Median age, years (range) | 68 (34–85) | 69 (34–85) | 66 (37–82) |
| Gender | |||
| Male | 86 (61.0) | 57 (63.3) | 29 (56.9) |
| Female | 55 (39.0) | 33 (36.7) | 22 (43.1) |
| ECOG PS | |||
| 0 | 113 (81.3) | 70 (79.6) | 43 (84.3) |
| 1–2 | 26 (18.7) | 18 (20.4) | 8 (15.7) |
| Unknown/missing | 2 | 2 | 0 |
| Tumor location | |||
| Colon | 109 (77.3) | 69 (76.7) | 40 (78.4) |
| Rectum | 32 (22.7) | 21 (23.3) | 11 (21.6) |
| Left-sided | 75 (56.4) | 47 (56.6) | 28 (56.0) |
| Right-sided | 58 (43.6) | 36 (43.4) | 22 (44.0) |
| Unknown/missing | 8 | 7 | 1 |
| Stage at diagnosis | |||
| I-III | 20 (14.2) | 8 (8.9) | 12 (23.5) |
| IV | 121 (85.8) | 82 (91.1) | 39 (76.5) |
| CT regimen | |||
| Oxaliplatin-based | 89 (63.1) | 59 (65.6) | 30 (58.8) |
| FOLFIRI | 52 (36.9) | 31 (34.4) | 21 (41.2) |
| KRAS | |||
| Wild type | 87 (61.7) | 52 (57.8) | 35 (68.6) |
| Mutated | 54 (38.3) | 38 (42.2) | 16 (31.4) |
| NRAS | |||
| Wild type | 41 (95.4) | 29 (93.6) | 12 (100) |
| Mutated | 2 (4.7) | 2 (6.5) | - |
| BRAF | |||
| Wild type | 40 (88.9%) | 29 (90.6%) | 11 (84.6%) |
| Mutated | 5 (11.1%) | 3 (9.4%) | 2 (15.4%) |
| No. Patients | No. Events | Median PFS (Months) (95% CI) | p | No. Events | Median OS (Months) (95% CI) | p | |
|---|---|---|---|---|---|---|---|
| Overall | |||||||
| Stable | 124 | 117 | 11.4 (9.4–12.6) | 95 | 27.3 (23.4–33.1) | ||
| Unstable | 11 | 10 | 5.0 (0.9–9.0) | 0.060 | 10 | 6.1 (1.5–25.2) | 0.006 |
| CT + B | |||||||
| Stable | 76 | 71 | 11.7 (9.4–12.6) | 57 | 29.1 (23.3–34.5)) | ||
| Unstable | 9 | 9 | 5.0 (0.9–9.0) | 0.0006 | 9 | 6.1 (0.9–25.2) | <0.0001 |
| CT | |||||||
| Stable | 48 | 46 | 9.8 (8.3–14.2) | 38 | 27.1 (20.8–36.7) | ||
| Unstable | 2 | 1 | nr | 0.486 | 1 | nr | 0.697 |
| No. Patients | No. Events | Median PFS (Months) (95% CI) | p | No. Events | Median OS (Months) (95% CI) | p | |
|---|---|---|---|---|---|---|---|
| Overall | |||||||
| D20S82 | |||||||
| Stable | 108 | 102 | 10.6 (9.0–12.2) | 86 | 26.0 (23.2–30.2) | ||
| Unstable | 21 | 20 | 9.0 (3.7–11.5) | 0.793 | 17 | 14.0 (6.1–40.0) | 0.925 |
| D20S85 | |||||||
| Stable | 123 | 115 | 10.8 (9.2–12.2) | 93 | 28.6 (23.4–34.1) | ||
| Unstable | 12 | 12 | 7.3 (2.9–13.7) | 0.022 | 12 | 8.1 (4.4–24.0) | <0.0001 |
| D8S321 | |||||||
| Stable | 108 | 104 | 10.5 (9.0–12.1) | 83 | 28.8 (23.3–35.7)) | ||
| Unstable | 11 | 10 | 8.6 (4.7–16.0) | 0.576 | 10 | 17.8 (4.7–26.4) | 0.029 |
| D9S242 | |||||||
| Stable | 119 | 113 | 10.8 (9.3–12.4) | 94 | 26.4 (23.3–31.7) | ||
| Unstable | 9 | 8 | 6.5 (0.7–97.4) | 0.427 | 6 | 27.1 (1.5–nr) | 0.680 |
| MYCL1 | |||||||
| Stable | 107 | 100 | 11.4 (9.4–12.6) | 82 | 28.6 (23.2–34.5) | ||
| Unstable | 15 | 14 | 6.1 (1.8–9.1) | 0.007 | 13 | 11.5 (2.8–34.1) | 0.030 |
| CT + B | |||||||
| D20S82 | |||||||
| Stable | 65 | 61 | 11.9 (9.4–12.6) | 50 | 26.0 (21.3–34.1) | ||
| Unstable | 17 | 17 | 7.4 (2.5–10.8) | 0.078 | 16 | 12.7 (4.7–33.1) | 0.113 |
| D20S85 | |||||||
| Stable | 75 | 70 | 11.4 (9.3–12.4) | 56 | 30.2 (23.4–35.7) | ||
| Unstable | 10 | 10 | 5.5 (0.9–12.6) | 0.015 | 10 | 6.5 (0.9–15.1) | <0.0001 |
| D8S321 | |||||||
| Stable | 74 | 71 | 11.1 (9.0–12.2) | 57 | 28.8 (21.3–34.5) | ||
| Unstable | 8 | 7 | 7.3 (1.8–16.0) | 0.599 | 7 | 8.1 (2.8–25.2) | 0.075 |
| D9S242 | |||||||
| Stable | 75 | 71 | 11.4 (9.2–12.4) | 59 | 26.0 (21.0–31.9) | ||
| Unstable | 4 | 4 | 7.0 (4.7–19.3) | 0.338 | 3 | 23.1 (4.7–40.0) | 0.518 |
| MYCL1 | |||||||
| Stable | 67 | 63 | 11.5 (9.2–12.6) | 52 | 28.8 (21.0–34.5) | ||
| Unstable | 10 | 9 | 7.3 (1.8–12.2) | 0.224 | 8 | 18.0 (2.8–49.4) | 0.408 |
| CT | |||||||
| D20S82 | |||||||
| Stable | 43 | 41 | 9.1 (6.5–13.7) | 36 | 26.4 (20.2–36.7) | ||
| Unstable | 4 | 3 | 71.6 (9.8–88.6) | 0.017 | 1 | nr | 0.048 |
| D20S85 | |||||||
| Stable | 48 | 45 | 9.5 (8.3–15.0) | 37 | 27.1 (20.4–36.7) | ||
| Unstable | 2 | 2 | 12.5 (11.4–13.7) | 0.847 | 2 | 30.8 (24.0–37.6) | 0.778 |
| D8S321 | |||||||
| Stable | 34 | 33 | 9.2 (6.5–14.2) | 26 | 29.1 (20.4–48.7) | ||
| Unstable | 3 | 3 | 13.1 (6.2–20.1) | 0.7550 | 3 | 26.4 (20.1–28.6) | 0.329 |
| D9S242 | |||||||
| Stable | 44 | 42 | 9.8 (8.3-15.0) | 35 | 27.3 (20.4–37.3) | ||
| Unstable | 5 | 4 | 6.5 (0.7–97.4) | 0.232 | 3 | 27.1 (1.5–nr) | 0.594 |
| MYCL1 | |||||||
| Stable | 40 | 37 | 10.2 (8.3–18.2) | 30 | 28.6 (20.4–48.7) | ||
| Unstable | 5 | 5 | 3.1 (0.6–9.1) | 0.002 | 5 | 11.5 (0.6–36.7) | 0.014 |
| No. Patients | No. Events | Median PFS (Months) (95% CI) | p | No. Events | Median OS (Months) (95% CI) | p | |
|---|---|---|---|---|---|---|---|
| Overall | |||||||
| VEGF-B stable | 88 | 82 | 10.0 (8.9–12.2) | 69 | 23.3 (20.1–31.7) | ||
| AG shortened | 12 | 12 | 14.5 (2.3–77.9) | 10 | 27.7 (14.0–79.5) | ||
| AG amplified | 17 | 17 | 12.2 (7.4–19.3) | 0.050 | 12 | 36.7 (9.4–71.7) | 0.406 |
| CT + B | |||||||
| VEGF-B stable | 53 | 50 | 10.0 (7.7–12.2) | 43 | 21.4 (13.7–31.9) | ||
| AG shortened | 3 | 3 | 8.7 (2.3–10.2) | 3 | 26.0 (13.9–46.1) | ||
| AG amplified | 13 | 13 | 18.3 (8.6–22.2) | 0.132 | 8 | 44.0 (9.4–71.7) | 0.159 |
| CT | |||||||
| VEGF-B stable | 35 | 32 | 10.2 (6.3–15.0) | 26 | 26.5 (20.2–39.7) | ||
| AG shortened | 9 | 9 | 28.0 (2.0–88.6) | 7 | 28.0 (4.3–nr) | ||
| AG amplified | 4 | 4 | 7.0 (0.6–9.1) | 0.005 | 4 | 22.6 (0.6–36.7) | 0.268 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pirini, F.; Pasini, L.; Tedaldi, G.; Scarpi, E.; Marisi, G.; Molinari, C.; Calistri, D.; Passardi, A.; Ulivi, P. Instability of Non-Standard Microsatellites in Relation to Prognosis in Metastatic Colorectal Cancer Patients. Int. J. Mol. Sci. 2020, 21, 3532. https://doi.org/10.3390/ijms21103532
Pirini F, Pasini L, Tedaldi G, Scarpi E, Marisi G, Molinari C, Calistri D, Passardi A, Ulivi P. Instability of Non-Standard Microsatellites in Relation to Prognosis in Metastatic Colorectal Cancer Patients. International Journal of Molecular Sciences. 2020; 21(10):3532. https://doi.org/10.3390/ijms21103532
Chicago/Turabian StylePirini, Francesca, Luigi Pasini, Gianluca Tedaldi, Emanuela Scarpi, Giorgia Marisi, Chiara Molinari, Daniele Calistri, Alessandro Passardi, and Paola Ulivi. 2020. "Instability of Non-Standard Microsatellites in Relation to Prognosis in Metastatic Colorectal Cancer Patients" International Journal of Molecular Sciences 21, no. 10: 3532. https://doi.org/10.3390/ijms21103532