Effects of Mindfulness-Based Interventions on Biomarkers and Low-Grade Inflammation in Patients with Psychiatric Disorders: A Meta-Analytic Review

 ,
,  ,
,  , and
, and
Abstract
:1. Introduction
2. Methods
2.1. Eligibility Criteria
2.2. Search Strategy
2.3. Study Selection
2.4. Data Extraction
2.5. Assessment of Study Quality
2.6. Data Synthesis
3. Results
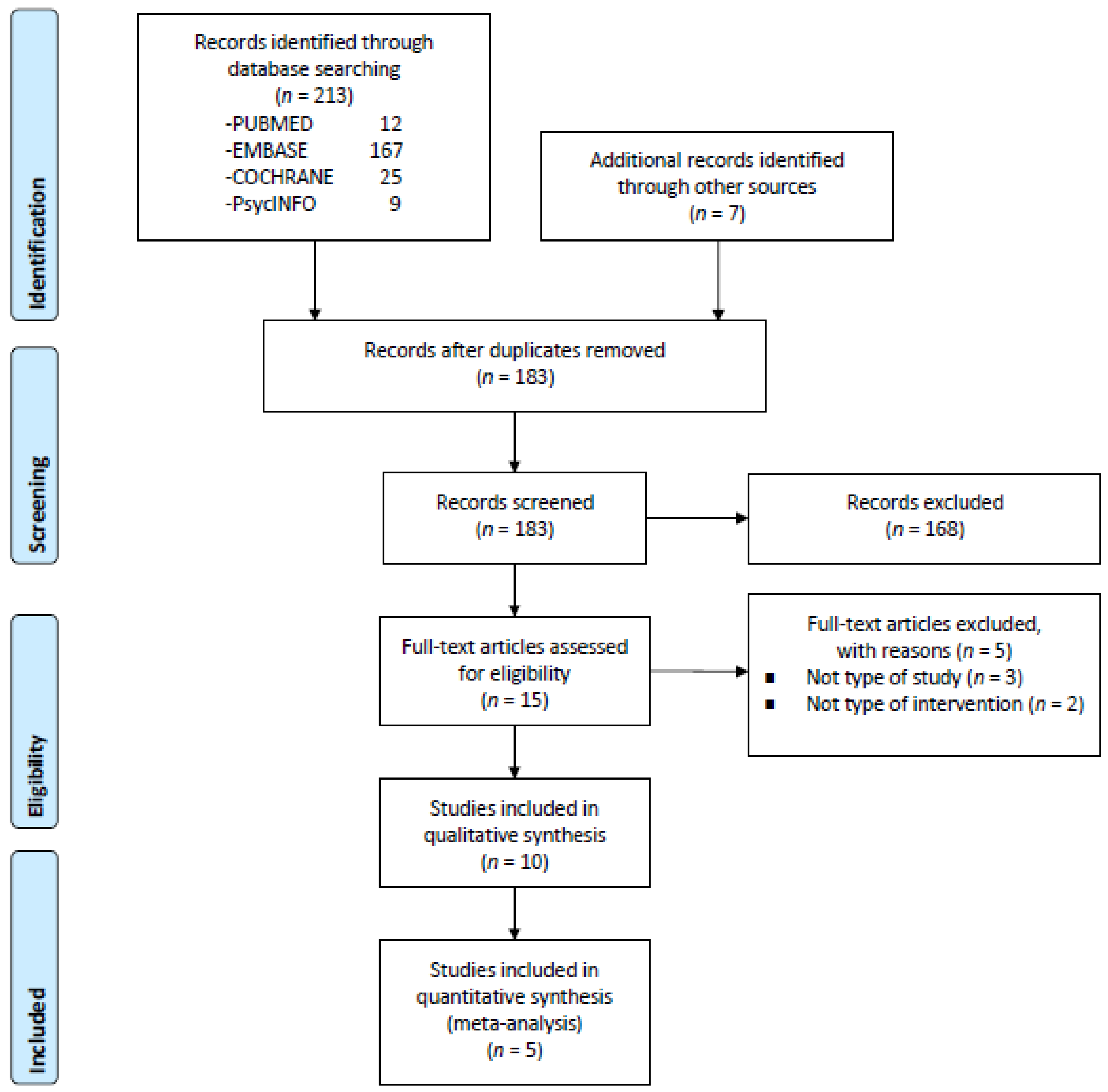
3.1. Search Results
3.2. Participants
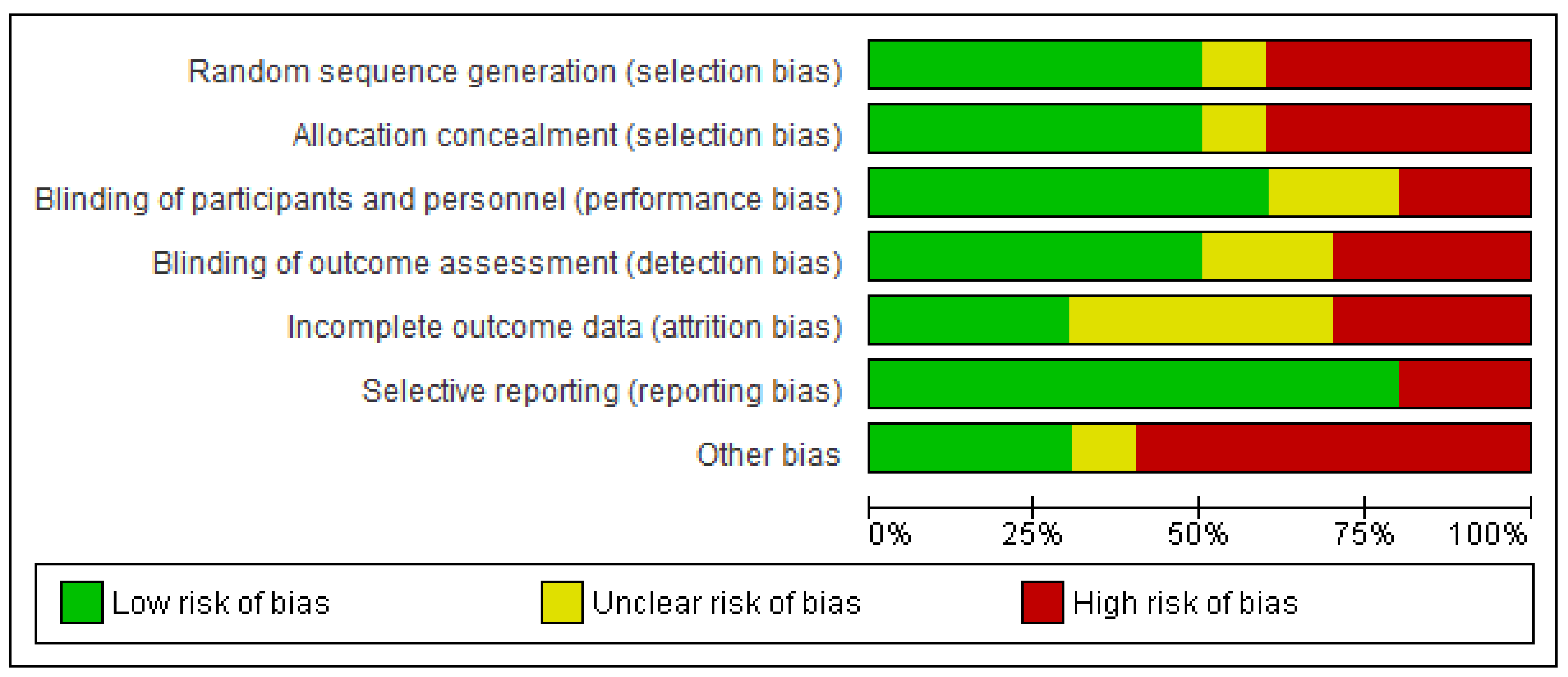
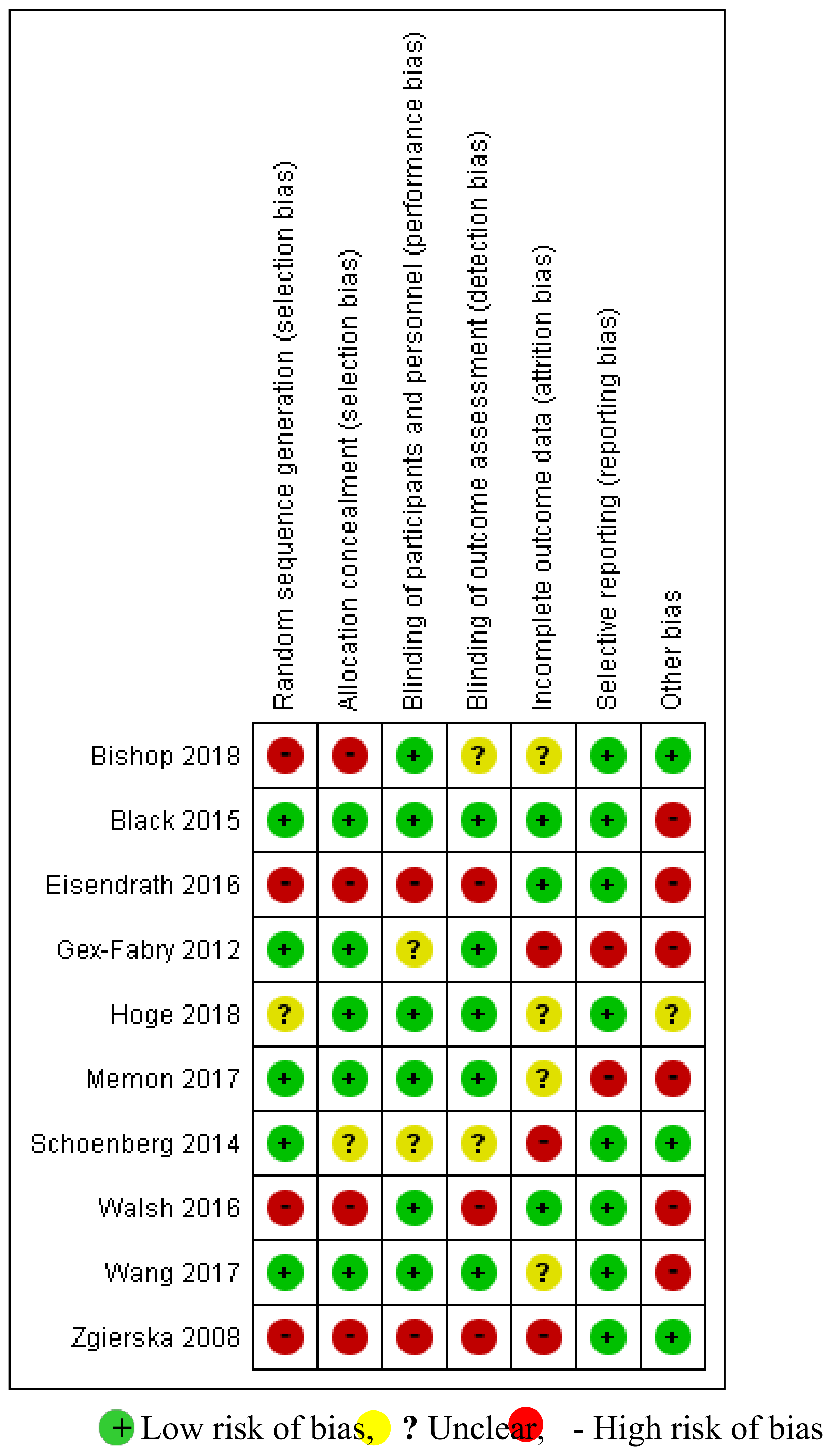
3.3. Quality of Studies and Interventions
3.4. Biomarkers
3.5. Mindfulness-Based Interventions (MBIs)
3.6. Effectiveness of MBIs on Biomarkers
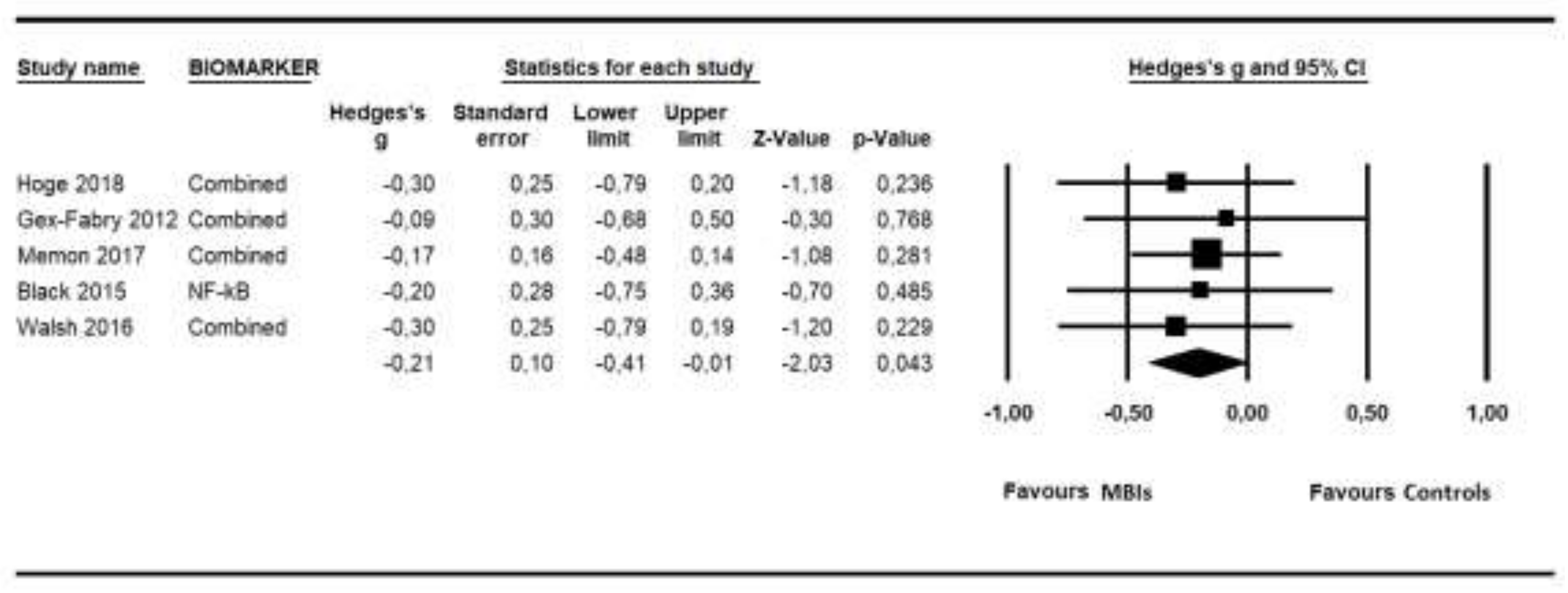
3.7. Low-Grade Inflammation Outcomes Synthesis
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Sanada, K.; Alda, D.M.; Salas, V.M.; Pérez-Yus, M.C.; Demarzo, M.M.; Montero-Marín, J.; García-Toro, M.; García-Campayo, J. Effects of mindfulness-based interventions on biomarkers in healthy and cancer populations: A systematic review. BMC Complement. Altern. Med. 2017, 17, 125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kabat-Zinn, J. Full Catastrophe Living: Using the Wisdom of Your Body and Mind to Face Stress, Pain, and Illness; Dell Publishing: New York, NY, USA, 1990. [Google Scholar]
- Kabat-Zinn, J. Mindfulness-based interventions in context: Past, present, and future. Clin. Psychol. 2003, 10, 144–156. [Google Scholar] [CrossRef]
- Kabat-Zinn, J. An outpatient program in behavioral medicine for chronic pain patients based on the practice of mindfulness meditation: Theoretical considerations and preliminary results. Gen. Hosp. Psychiatry 1982, 4, 33–47. [Google Scholar] [CrossRef]
- Segal, Z.; Williams, J.; Teasdale, J. Mindfulness-Based Cognitive Therapy for Depression: A New Approach to Preventing Relapse; Guilford Press: New York, NY, USA, 2002. [Google Scholar]
- Witkiewitz, K.; Marlatt, G.A.; Walker, D. Mindfulness-Based Relapse Prevention for Alcohol and Substance Use Disorders. J. Cogn. Psychother. 2005, 19, 211–228. [Google Scholar] [CrossRef]
- Bowen, S.; Chawla, N.; Marlatt, G. Mindfulness-Based Relapse Prevention for Addictive Behaviors: A Clinician’s Guide; Guilford Press: New York, NY, USA, 2010. [Google Scholar]
- Sanada, K.; Montero-Marin, J.; Alda, D.M.; Salas-Valero, M.; Pérez-Yus, M.C.; Morillo, H.; Demarzo, M.M.; García-Toro, M.; García-Campayo, J. Effects of Mindfulness-Based Interventions on Salivary Cortisol in Healthy Adults: A Meta-Analytical Review. Front. Physiol. 2016, 7, 471. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldberg, S.B.; Tucker, R.P.; Greene, P.A.; Davidson, R.J.; Wampold, B.E.; Kearney, D.J.; Simpson, T.L. Mindfulness-based interventions for psychiatric disorders: A systematic review and meta-analysis. Clin. Psychol. Rev. 2018, 59, 52–60. [Google Scholar] [CrossRef] [PubMed]
- Montero-Marin, J.; Garcia-Campayo, J.; Pérez-Yus, M.C.; Zabaleta-Del-Olmo, E.; Cuijpers, P. Meditation techniques v. relaxation therapies when treating anxiety: A meta-analytic review. Psychol. Med. 2019, 49, 2118–2133. [Google Scholar] [CrossRef]
- Kuyken, W.; Byford, S.; Taylor, R.S.; Watkins, E.; Holden, E.; White, K.; Barrett, B.; Byng, R.; Evans, A.; Mullan, E.; et al. Mindfulness-based cognitive therapy to prevent relapse in recurrent depression. J. Consult. Clin. Psychol. 2008, 76, 966–978. [Google Scholar] [CrossRef]
- Kogan, M.; Kligler, B. Mind-Body Medicine Therapies for a Range of Depression Severity: A Systematic Review. Psychosomatics 2012, 53, 407–423. [Google Scholar]
- Strauss, C.; Cavanagh, K.; Oliver, A.; Pettman, D. Mindfulness-based interventions for people diagnosed with a current episode of an anxiety or depressive disorder: A meta-analysis of randomised controlled trials. PLoS ONE 2014, 9, e96110. [Google Scholar] [CrossRef]
- Hofmann, S.G.; Sawyer, A.T.; Witt, A.A.; Oh, D. The Effect of Mindfulness-Based Therapy on Anxiety and Depression: A Meta-Analytic Review. J. Consult. Clin. Psychol. 2010, 78, 169–183. [Google Scholar] [CrossRef] [PubMed]
- Vøllestad, J.; Nielsen, M.B.; Nielsen, G.H. Mindfulness- and acceptance-based interventions for anxiety disorders: A systematic review and meta-analysis. Br. J. Clin. Psychol. 2012, 51, 239–260. [Google Scholar] [CrossRef] [PubMed]
- Pascoe, M.C.; Thompson, D.R.; Jenkins, Z.M.; Ski, C.F. Mindfulness mediates the physiological markers of stress: Systematic review and meta-analysis. J. Psychiatry Res. 2017, 95, 156–178. [Google Scholar] [CrossRef] [PubMed]
- Karyadi, K.A.; Vanderveen, J.D.; Cyders, M.A. A Meta-Analysis of the Relationship between Trait Mindfulness and Substance Use Behaviors. Drug Alcohol Depend. 2014, 143, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Grant, S.; Colaiaco, B.; Motala, A.; Shanman, R.; Booth, M.; Sorbero, M.; Hempel, S. Mindfulness-based Relapse Prevention for Substance Use Disorders: A Systematic Review and Meta-analysis. J. Addict. Med. 2017, 11, 386–396. [Google Scholar] [CrossRef] [Green Version]
- Li, W.; Howard, M.O.; Garland, E.L.; Mcgovern, P.; Lazar, M. Mindfulness treatment for substance misuse: A systematic review and meta-analysis. J. Subst. Abuse Treat. 2017, 75, 62–96. [Google Scholar] [CrossRef]
- Winbush, N.Y.; Gross, C.R.; Kreitzer, M.J. The effects of Mindfulness-Based Stress Reduction on sleep disturbance: A systematic review. Explore 2007, 3, 585–591. [Google Scholar] [CrossRef]
- Gong, H.; Ni, C.; Liu, Y.; Zhang, Y.; Su, W.; Lian, Y.; Peng, W.; Jiang, C. Mindfulness meditation for insomnia: A meta-analysis of randomized controlled trials. J. Psychosom. Res. 2016, 89, 1–6. [Google Scholar] [CrossRef]
- Lakhan, S.E.; Schofield, K.L. Mindfulness-Based Therapies in the Treatment of Somatization Disorders: A Systematic Review and Meta-Analysis. PLoS ONE 2013, 8, e71834. [Google Scholar] [CrossRef] [Green Version]
- Memon, A.A.; Sundquist, K.; Ahmad, A.; Wang, X.; Hedelius, A.; Sundquist, J. Role of IL-8, CRP and epidermal growth factor in depression and anxiety patients treated with mindfulness-based therapy or cognitive behavioral therapy in primary health care. Psychiatry Res. 2017, 254, 311–316. [Google Scholar] [CrossRef]
- Reich, R.R.; Lengacher, C.A.; Klein, T.W.; Newton, C.; Shivers, S.; Ramesar, S.; Alinat, C.B.; Paterson, C.; Le, A.; Park, J.Y.; et al. A Randomized Controlled Trial of the Effects of Mindfulness-Based Stress Reduction (MBSR[BC]) on Levels of Inflammatory Biomarkers Among Recovering Breast Cancer Survivors. Biol. Res. Nurs. 2017, 19, 456–464. [Google Scholar] [CrossRef] [PubMed]
- Dada, T.; Mittal, D.; Mohanty, K.; Faiq, M.A.; Bhat, M.A.; Yadav, R.K.; Sihota, R.; Sidhu, T.; Velpandian, T.; Kalaivani, M.; et al. Mindfulness Meditation Reduces Intraocular Pressure, Lowers Stress Biomarkers and Modulates Gene Expression in Glaucoma: A Randomized Controlled Trial. J. Glaucoma 2018, 27, 1061–1067. [Google Scholar] [CrossRef] [PubMed]
- Hoge, E.A.; Bui, E.; Palitz, S.A.; Schwarz, N.R.; Owens, M.E.; Johnston, J.M.; Pollack, M.H.; Simon, N.M. The effect of mindfulness meditation training on biological acute stress responses in generalized anxiety disorder. Psychiatry Res. 2018, 262, 328–332. [Google Scholar] [CrossRef]
- Barrett, B.; Hayney, M.S.; Muller, D.; Rakel, D.; Brown, R.; Zgierska, A.E.; Barlow, S.; Hayer, S.; Barnet, J.H.; Torres, E.R.; et al. Meditation or exercise for preventing acute respiratory infection (MEPARI-2): A randomized controlled trial. PLoS ONE 2018, 13, e0197778. [Google Scholar] [CrossRef] [PubMed]
- Carlson, L.E.; Speca, M.; Faris, P.; Patel, K.D. One year pre-post intervention follow-up of psychological, immune, endocrine and blood pressure outcomes of mindfulness-based stress reduction (MBSR) in breast and prostate cancer outpatients. Brain Behav. Immun. 2007, 21, 1038–1049. [Google Scholar] [CrossRef] [PubMed]
- Witek-Janusek, L.; Albuquerque, K.; Chroniak, K.R.; Chroniak, C.; Durazo-Arvizu, R.; Mathews, H.L. Effect of mindfulness based stress reduction on immune function, quality of life and coping in women newly diagnosed with early stage breast cancer. Brain Behav. Immun. 2008, 22, 969–981. [Google Scholar] [CrossRef] [Green Version]
- Lengacher, C.A.; Kip, K.E.; Post-White, J.; Fitzgerald, S.; Newton, C.; Barta, M.; Jacobsen, P.B.; Shelton, M.M.; Moscoso, M.; Johnson-Mallard, V.; et al. Lymphocyte recovery after breast cancer treatment and mindfulness-based stress reduction (MBSR) therapy. Biol. Res. Nurs. 2013, 15, 37–47. [Google Scholar] [CrossRef]
- Johnson, D.C.; Thom, N.J.; Stanley, E.A.; Haase, L.; Simmons, A.N.; Shih, P.A.; Thompson, W.K.; Potterat, E.G.; Minor, T.R.; Paulus, M.P. Modifying resilience mechanisms in at-risk individuals: A controlled study of mindfulness training in Marines preparing for deployment. Am. J. Psychiatry 2014, 171, 844–853. [Google Scholar] [CrossRef] [Green Version]
- Villalba, D.K.; Lindsay, E.K.; Marsland, A.L.; Greco, C.M.; Young, S.; Brown, K.W.; Smyth, J.M.; Walsh, C.P.; Gray, K.; Chin, B.; et al. Mindfulness training and systemic low-grade inflammation in stressed community adults: Evidence from two randomized controlled trials. PLoS ONE 2019, 14, e0219120. [Google Scholar] [CrossRef]
- Lopresti, A.L.; Maker, G.L.; Hood, S.D.; Drummond, P.D. A review of peripheral biomarkers in major depression: The potential of inflammatory and oxidative stress biomarkers. Prog. Neuropsychopharmacol. Biol. Psychiatry 2014, 48, 102–111. [Google Scholar] [CrossRef] [Green Version]
- Yao, H.; Mizoguchi, Y.; Monji, A.; Yakushiji, Y.; Takashima, Y.; Uchino, A.; Yuzuriha, T.; Hashimoto, M. Low-Grade Inflammation Is Associated with Apathy Indirectly via Deep White Matter Lesions in Community-Dwelling Older Adults: The Sefuri Study. Int. J. Mol. Sci. 2019, 20, 1905. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Osimo, E.F.; Cardinal, R.N.; Jones, P.B.; Khandaker, G.M. Prevalence and correlates of low-grade systemic inflammation in adult psychiatric inpatients: An electronic health record-based study. Psychoneuroendocrinology 2018, 91, 226–234. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Int. J. Surg. 2010, 8, 336–341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions; Version 5.1.0. (Updated March 2011); The Cochrane Collaboration: Oxford, UK, 2011. [Google Scholar]
- Lahera, G.; Bayón, C.; Bravo-Ortiz, M.F.; Rodríguez-Vega, B.; Barbeito, S.; Sáenz, M.; Avedillo, C.; Villanueva, R.; Ugarte, A.; González-Pinto, A.; et al. Mindfulness-based cognitive therapy versus psychoeducational intervention in bipolar outpatients with sub-threshold depressive symptoms: A randomized controlled trial. BMC Psychiatry 2014, 14, 215. [Google Scholar] [CrossRef] [Green Version]
- Ruffault, A.; Carette, C.; Lurbe, I.; Puerto, K.; Juge, N.; Beauchet, A.; Benoliel, J.J.; Lacorte, J.M.; Fournier, J.F.; Czernichow, S.; et al. Randomized controlled trial of a 12-month computerized mindfulness-based intervention for obese patients with binge eating disorder: The MindOb study protocol. Contemp. Clin. Trials. 2016, 49, 126–133. [Google Scholar] [CrossRef] [Green Version]
- Ashton, N.J.; Hye, A.; Leckey, C.A.; Jones, A.R.; Gardner, A.; Elliott, C.; Wetherell, J.L.; Lenze, E.J.; Killick, R.; Marchant, N.L. Plasma REST: A novel candidate biomarker of Alzheimer’s disease is modified by psychological intervention in an at-risk population. Transl. Psychiatry 2017, 7, e1148. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Chambless, D.L.; Hollon, S.D. Defining empirically supported therapies. J. Consult. Clin. Psychol. 1998, 66, 7–18. [Google Scholar] [CrossRef]
- Evans, J.F.; Ragolia, L. Systemic and local ACTH produced during inflammatory states promotes osteochondrogenic mesenchymal cell differentiation contributing to the pathologic progression of calcified atherosclerosis. Med. Hypotheses 2012, 79, 823–826. [Google Scholar] [CrossRef] [Green Version]
- Brown, E.S.; Varghese, F.P.; McEwen, B.S. Association of depression with medical illness: Does cortisol play a role? Biol. Psychiatry 2004, 55, 1–9. [Google Scholar] [CrossRef]
- Lovell, B.; Moss, M.; Wetherell, M.A. Perceived stress, on health complaints and diurnal patterns of cortisol secretion in young, otherwise healthy individuals. Horm. Behav. 2011, 60, 301–305. [Google Scholar] [CrossRef] [PubMed]
- Clow, A.; Thorn, L.; Evans, P.; Hucklebridge, F. The awakening cortisol response: Methodological issues and significance. Stress 2004, 7, 29–37. [Google Scholar] [CrossRef] [PubMed]
- Chida, Y.; Steptoe, A. Cortisol awakening response and psychosocial factors: A systematic review and meta-analysis. Biol. Psychol. 2009, 80, 265–278. [Google Scholar] [CrossRef] [PubMed]
- Hsiao, F.H.; Yang, T.T.; Ho, R.T.; Jow, G.M.; Ng, S.M.; Chan, C.L.; Lai, Y.M.; Chen, Y.T.; Wang, K.C. The self-perceived symptom distress and health-related conditions associated with morning to evening diurnal cortisol patterns in outpatients with major depressive disorder. Psychoneuroendocrinology 2010, 35, 503–515. [Google Scholar] [CrossRef] [PubMed]
- Stawski, R.S.; Almeida, D.M.; Lachman, M.E.; Tun, P.A.; Rosnick, C.B.; Seeman, T. Associations between cognitive function and naturally occurring daily cortisol during middle adulthood: Timing is everything. J. Gerontol. B. Psychol. Sci. Soc. Sci. 2011, 66, i71–i81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malcangio, M.; Bowery, N.G.; Flower, R.J.; Perretti, M. Effect of interleukin-1 beta on the release of substance P from rat isolated spinal cord. Eur. J. Pharmacol. 1996, 299, 113–118. [Google Scholar] [CrossRef]
- Wallace, D.J.; Linker-Israeli, M.; Hallegua, D.; Silverman, S.; Silver, D.; Weisman, M.H. Cytokines play an aetiopathogenetic role in fibromyalgia: A hypothesis and pilot study. Rheumatology 2001, 40, 743–749. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, H.; Moser, M.; Schiltenwolf, M.; Buchner, M. Circulating cytokine levels compared to pain in patients with fibromyalgia—A prospective longitudinal study over 6 months. J. Rheumatol. 2008, 35, 1366–1370. [Google Scholar] [PubMed]
- Sethi, G.G.; Sung, B.; Aggarwal, B.B. Nuclear factor-kappaB activation: From bench to bedside. Exp. Biol. Med. 2008, 233, 21–31. [Google Scholar] [CrossRef] [PubMed]
- Yousuf, O.; Mohanty, B.D.; Martin, S.S.; Joshi, P.H.; Blaha, M.J.; Nasir, K.; Blumenthal, R.S.; Budoff, M.J. High-sensitivity C-reactive protein and cardiovascular disease: A resolute belief or an elusive link? J. Am. Coll. Cardiol. 2013, 62, 397–408. [Google Scholar] [CrossRef] [Green Version]
- Wallensten, J.; Åsberg, M.; Nygren, Å.; Szulkin, R.; Wallén, H.; Mobarrez, F.; Nager, A. Possible biomarkers of chronic stress induced exhaustion—A longitudinal study. PLoS ONE 2016, 11, e0153924. [Google Scholar] [CrossRef] [PubMed]
- Yamamori, H.; Ishima, T.; Yasuda, Y.; Fujimoto, M.; Kudo, N.; Ohi, K.; Hashimoto, K.; Takeda, M.; Hashimoto, R. Assessment of multi-assay biological diagnostic test for mood disorders in a Japanese population. Neurosci. Lett. 2016, 612, 167–171. [Google Scholar] [CrossRef]
- Hedges, L.V. Distribution theory for Glass’s estimator of effect size and related estimators. J. Educ. Behav. Stat. 1981, 6, 107–128. [Google Scholar] [CrossRef]
- Furukawa, T.A.; Leucht, S. How to obtain NNT from Cohen’s d: Comparison of two methods. PLoS ONE 2011, 6, e19070. [Google Scholar] [CrossRef] [Green Version]
- Laupacis, A.; Sackett, D.L.; Roberts, R.S. An assessment of clinically useful measures of the consequences of treatment. N. Engl. J. Med. 1988, 318, 1728–1733. [Google Scholar] [CrossRef] [PubMed]
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.T.; Rothstein, H.R. Introduction to Meta-Analysis; John Wiley & Sons, Ltd: Chichester, UK, 2009. [Google Scholar]
- Vevea, J.L.; Woods, C.M. Publication bias in research synthesis: Sensitivity analysis using a priori weight functions. Psychol. Methods. 2005, 10, 428–443. [Google Scholar] [CrossRef]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detect by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [Green Version]
- Duval, S.; Tweedie, R. Trim and fill: A simple funnel-plot-based method. Biometrics 2000, 56, 455–463. [Google Scholar] [CrossRef]
- Begg, C.B.; Mazumbar, M. Operating characteristics of a rank correlation test for publication bias. Biometrics 1994, 50, 1088–1101. [Google Scholar] [CrossRef]
- Gex-Fabry, M.; Jermann, F.; Kosel, M.; Rossier, M.F.; Van der Linden, M.; Bertschy, G.; Bondolfi, G.; Aubry, J.M. Salivary cortisol profiles in patients remitted from recurrent depression: One-year follow-up of a mindfulness-based cognitive therapy trial. J. Psychiatr. Res. 2012, 46, 80–86. [Google Scholar] [CrossRef]
- Schoenberg, P.L.; Hepark, S.; Kan, C.C.; Barendregt, H.P.; Buitelaar, J.K.; Speckens, A.E. Effects of mindfulness-based cognitive therapy on neurophysiological correlates of performance monitoring in adult attention-deficit/hyperactivity disorder. Clin. Neurophysiol. 2014, 125, 1407–1416. [Google Scholar] [CrossRef] [PubMed]
- Black, D.S.; O’Reilly, G.A.; Olmstead, R.; Breen, E.C.; Irwin, M.R. Mindfulness meditation and improvement in sleep quality and daytime impairment among older adults with sleep disturbances: A randomized clinical trial. JAMA Intern. Med. 2015, 175, 494–501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walsh, E.; Eisenlohr-Moul, T.; Baer, R. Brief mindfulness training reduces salivary IL-6 and TNF-α in young women with depressive symptomatology. J. Consult. Clin. Psychol. 2016, 84, 887–897. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Sundquist, K.; Hedelius, A.; Palmér, K.; Memon, A.A.; Sundquist, J. Leukocyte telomere length and depression, anxiety and stress and adjustment disorders in primary health care patients. BMC Psychiatry 2017, 17, 148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zgierska, A.; Rabago, D.; Zuelsdorff, M.; Coe, C.; Miller, M.; Fleming, M. Mindfulness meditation for alcohol relapse prevention: A feasibility pilot study. J. Addict. Med. 2008, 2, 165–173. [Google Scholar] [CrossRef] [PubMed]
- Eisendrath, S.J.; Gillung, E.; Hartzler, A.; James-Myers, M.; Wolkowitz, O.; Sipe, W.; Ramanatham, D.; Delucchi, K. Mindfulness-based cognitive therapy associated with decreases in C-reactive protein in major depressive disorder: A pilot study. J. Altern. Complement. Integr. Med. 2016, 2, 010. [Google Scholar] [CrossRef] [Green Version]
- Bishop, J.R.; Lee, A.M.; Mills, L.J.; Thuras, P.D.; Eum, S.; Clancy, D.; Erbes, C.R.; Polusny, M.A.; Lamberty, G.J.; Lim, K.O. Methylation of FKBP5 and SLC6A4 in relation to treatment response to mindfulness based stress reduction for posttraumatic stress disorder. Front. Psychiatry 2018, 9, 418. [Google Scholar] [CrossRef]
- Johnstone, S.J.; Barry, R.J. Auditory event-related potentials in a two-tone discrimination paradigm in attention deficit hyperactivity disorder. Psychiatry Res. 1996, 64, 179–192. [Google Scholar] [CrossRef]
- Karayanidis, F.; Robaey, P.; Bourassa, M.; de Koning, D.; Geoffroy, G.; Pelletier, G. ERP differences in visual attention processing between attention-deficit hyperactivity disorder and control boys in the absence of performance differences. Psychophysiology 2000, 37, 319–333. [Google Scholar] [CrossRef]
- Benikos, N.; Johnstone, S.J. Arousal-state modulation in children with AD/HD. Clin. Neurophysiol. 2009, 120, 30–40. [Google Scholar] [CrossRef]
- Kaunhoven, R.J.; Dorjee, D. How does mindfulness modulate self-regulation in pre-adolescent children? An integrative neurocognitive review. Neurosci. Biobehav. Rev. 2017, 74, 163–184. [Google Scholar] [CrossRef] [PubMed]
- Stechschulte, L.A.; Sanchez, E.R. FKBP51―A selective modulator of glucocorticoid and androgen sensitivity. Curr. Opin. Pharmacol. 2011, 11, 332–337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zannas, A.S.; Binder, E.B. Gene-environment interactions at the FKBP5 locus: Sensitive periods, mechanisms and pleiotropism. Genes Brain Behav. 2014, 13, 25–37. [Google Scholar] [CrossRef]
- Binder, E.B.; Salyakina, D.; Lichtner, P.; Wochnik, G.M.; Ising, M.; Pütz, B.; Papiol, S.; Seaman, S.; Lucae, S.; Kohli, M.A.; et al. Polymorphisms in FKBP5 are associated with increased recurrence of depressive episodes and rapid response to antidepressant treatment. Nat. Genet. 2004, 36, 1319–1325. [Google Scholar] [CrossRef]
- Yehuda, R.; Daskalakis, N.P.; Desarnaud, F.; Makotkine, I.; Lehrner, A.L.; Koch, E.; Flory, J.D.; Buxbaum, J.D.; Meaney, M.J.; Bierer, L.M. Epigenetic biomarkers as predictors and correlates of symptom improvement following psychotherapy in combat veterans with PTSD. Front. Psychiatry 2013, 4, 118. [Google Scholar] [CrossRef] [Green Version]
- Black, D.S.; Slavich, G.M. Mindfulness meditation and the immune system: A systematic review of randomized controlled trials. Ann. N. Y. Acad. Sci. 2016, 1373, 13–24. [Google Scholar] [CrossRef]
- Kim, S.H.; Schneider, S.M.; Bevans, M.; Kravitz, L.; Mermier, C.; Qualls, C.; Burge, M.R. PTSD symptom reduction with mindfulness-based stretching and deep breathing exercise: Randomized controlled clinical trial of efficacy. J. Clin. Endocrinol. Metab. 2013, 98, 2984–2992. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria | |
|---|---|---|
| Participants | Patients with psychiatric disorders according to either a formal diagnosis interview and/or a cut-off for clinical symptoms in a rating scale; No restrictions were placed on age. | Patients with other disorders, and only healthy subjects. |
| Interventions | Mindfulness-based interventions (MBIs) | Other non-pharmacological interventions. |
| Outcome | At least one biomarker. | No biomarkers. |
| Study design | RCTs, Non-RCTs, Open trials with a pre-post analysis. | Study protocols, cross-sectional studies, qualitative studies |
| Publications | Published as full-text articles in peer-reviewed scientific journals. | Published as reviews, case reports, conference abstracts, or letters. |
| ("psychiatric disorders"[All Fields] OR "psychiatric disturbances"[All Fields] OR "psychiatric"[All Fields]) AND ("mindfulness"[MeSH Terms] OR "mindfulness"[All Fields] OR mbct[tiab] OR mbsr[tiab] OR "Mindfulness-Based Cognitive Therapy"[tiab] OR "Mindfulness Based Stress Reduction"[tiab] OR "MBI"[tiab] OR "mindfulness-based interventions"[tiab] OR meditation[tiab]) AND ("biomarkers"[MeSH Terms] OR "biomarkers"[All Fields] OR "biomarker"[All Fields] OR "biological markers"[All Fields] OR "biological marker"[All Fields]). |
| Study | Population | Age Mean (SD) or IQR | Sex (%F) | Outcomes | MBI Program | Controls | Follow Up (M) | Results | Definition of Psychiatric Disorders | Sd | In |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Zgierska | Alcohol | 38.4 (8.6) | 52.6 | IL-6, cortisol | MM | None | 4 | IL-6 levels decreased from baseline to 16-week follow-up (p = | DSM-IV | Open | + |
| 2008 [70] | dependence | serum, salivary | (n = 19) | 0.052). | + | ||||||
| US | 8 weeks | There were no significant changes in salivary cortisol levels | + | ||||||||
| from baseline to 16-week follow-up. | |||||||||||
| Gex-Fabry | Remitted from | 24–66 | 71.4 | cortisol | MBCT + TAU | TAU | 12 | No significant changes in cortisol indices from baseline to the | DSM-IV | RCT | + |
| 2012 [65] | recurrent MDD | salivary | (n = 28) | (n = 28) | end of intervention were observed between both groups. | MADRS ≤13 | + | ||||
| Switzerland | 8 weeks | 8 weeks | + | ||||||||
| Schoenberg | ADHD | 19–53 | 52.3 | ERP | MBCT | WL | No | In the MBCT group, there was a significant increase in Pe and | DSM-IV | RCT | ? |
| 2014 [66] | (n = 24) | (n = 20) | NoGo-P3 amplitudes (p = 0.02 and p = 0.02, respectively). | + | |||||||
| Netherlands | 12 weeks | - | |||||||||
| Black | Sleep | 66.3 (7.4) | 67.3 | NF-kB | MAPs | Education | No | There was a significant reduction overtime in the levels of NF- | PSQI ≥5 | RCT | - |
| 2015 [67] | disturbance | plasma | (n = 24) | (n = 25) | kB in both groups (p = 0.26). | + | |||||
| US | 6 weeks | 6 weeks | No significant difference in NF-kB concentrations was observed | - | |||||||
| between the groups. | |||||||||||
| Eisendrath | MDD | 34.9 (7.9) | 72.7 | CRP | MBCT | None | No | There was not significantly decrease in CRP levels from pre- to | SCID DSM-IV | Open | ? |
| 2016 [71] | serum | (n = 11) | post-intervention (p = 0.0517). | HAMD17 | + | ||||||
| US | 8 weeks | - | |||||||||
| Walsh | Depressive | 19.1 (0.1) | 100 | IL-6, TNF-α | Mindfulness | Contact | 3 | Mindfulness training predicted significant decreases in the | CES-D ≥ 16 | RCT | + |
| 2016 [68] | symptoms | salivary | (n = 31) | Control | levels of IL-6 and TNF-α (p < 0.001 and p = 0.013, respectively). | + | |||||
| US | 4 weeks | (n = 33)4 weeks | - | ||||||||
| Memon | MDD, AD or SD | 41.5 (11.0) | 87.3 | IL-6, IL-8, EGF, | Mindfulness | TAU (CBT) | No | EGF levels were significantly decreased from baseline to post- | ICD-10 | RCT | - |
| 2017 [23] | and adjustment | hsCRP | (n = 81) | (n = 85) | intervention in both groups (p < 0.001, both). | PHQ-9 ≥10 or | + | ||||
| Sweden | disorders | plasma | 8 weeks | 8 weeks | No significant changes in the levels of IL-8 and hsCRP from | HADS-D ≥7 | - | ||||
| baseline to post-intervention were found in both groups. | or HADS-A ≥7 | ||||||||||
| or 13≤ MADRS ≤34 | |||||||||||
| Wang | MDD, AD or SD | Pt: | Pt: | LTL | Mindfulness | TAU (CBT) | No | At baseline, telomere length was significantly shorter in the | ICD-10 | RCT | - |
| 2017 [69] | and adjustment | 41.9 (11.1) | 87.8 | (n = 88) | (n = 89) | patients compared to the controls (p = 0.006). | PHQ-9 ≥10 or | + | |||
| Sweden | disorders | Ct: | Ct: | 8weeks | 8weeks | There were no significant changes in the telomere length from | HADS-D ≥7 | - | |||
| 44.6 (12.5) | 38.4 | HCs | baseline to post-intervention in both the Mindfulness and the | or HADS-A ≥7 | |||||||
| (n = 320) | TAU groups, and was no significant difference between the | or 13≤ MADRS ≤34 | |||||||||
| groups. | |||||||||||
| Bishop | PTSD | Res: | Res: | SLC6A4 | MBSR | None | No | There was a significant time x responder group interaction for | DSM-IV | Open | + |
| 2018 [72] | 60.4 (14.5) | 18.0 | FKBP5 | (Res: n = 11) | methylation in FKBP5 intron 7 bin 2 (p = 0.013). | PCL, CAPS | + | ||||
| US | Non-Res: | Non-Res: | (Non-Res: n = 11) | A significant correlation between FKBP5 intron 7 bin 2 | + | ||||||
| 58.2 (10.2) | 18.0 | 9 weeks | methylation change and PCL change from before to after | ||||||||
| treatment was observed (r = −0.451, p = 0.04). | |||||||||||
| There was no effect of time for methylation changing in the | |||||||||||
| Primary component of SLC6A4. | |||||||||||
| Hoge | GAD | 39.2 (12.8) | 45.7 | cortisol, ACTH, IL-6 | MBSR | Education | No | MBSR group showed a greater reduction in ACTH, TNF-α and | SCID DSM-IV | RCT | + |
| 2018 [26] | TNF-α during TSST | (n = 42) | (n = 28) | IL-6 Area Under the Curve (AUC) concentrations compared to | + | ||||||
| US | plasma | 8 weeks | 8 weeks | control group (p =0.007, p = 0.033, p = 0.036, respectively). | + |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sanada, K.; Montero-Marin, J.; Barceló-Soler, A.; Ikuse, D.; Ota, M.; Hirata, A.; Yoshizawa, A.; Hatanaka, R.; Valero, M.S.; Demarzo, M.; et al. Effects of Mindfulness-Based Interventions on Biomarkers and Low-Grade Inflammation in Patients with Psychiatric Disorders: A Meta-Analytic Review. Int. J. Mol. Sci. 2020, 21, 2484. https://doi.org/10.3390/ijms21072484
Sanada K, Montero-Marin J, Barceló-Soler A, Ikuse D, Ota M, Hirata A, Yoshizawa A, Hatanaka R, Valero MS, Demarzo M, et al. Effects of Mindfulness-Based Interventions on Biomarkers and Low-Grade Inflammation in Patients with Psychiatric Disorders: A Meta-Analytic Review. International Journal of Molecular Sciences. 2020; 21(7):2484. https://doi.org/10.3390/ijms21072484
Chicago/Turabian StyleSanada, Kenji, Jesus Montero-Marin, Alberto Barceló-Soler, Daisuke Ikuse, Marie Ota, Akihito Hirata, Akira Yoshizawa, Rieko Hatanaka, Montserrat Salas Valero, Marcelo Demarzo, and et al. 2020. "Effects of Mindfulness-Based Interventions on Biomarkers and Low-Grade Inflammation in Patients with Psychiatric Disorders: A Meta-Analytic Review" International Journal of Molecular Sciences 21, no. 7: 2484. https://doi.org/10.3390/ijms21072484