Immunogenic Effect of Hyperthermia on Enhancing Radiotherapeutic Efficacy

Abstract
:1. Current State of Radiotherapy and Immunotherapy
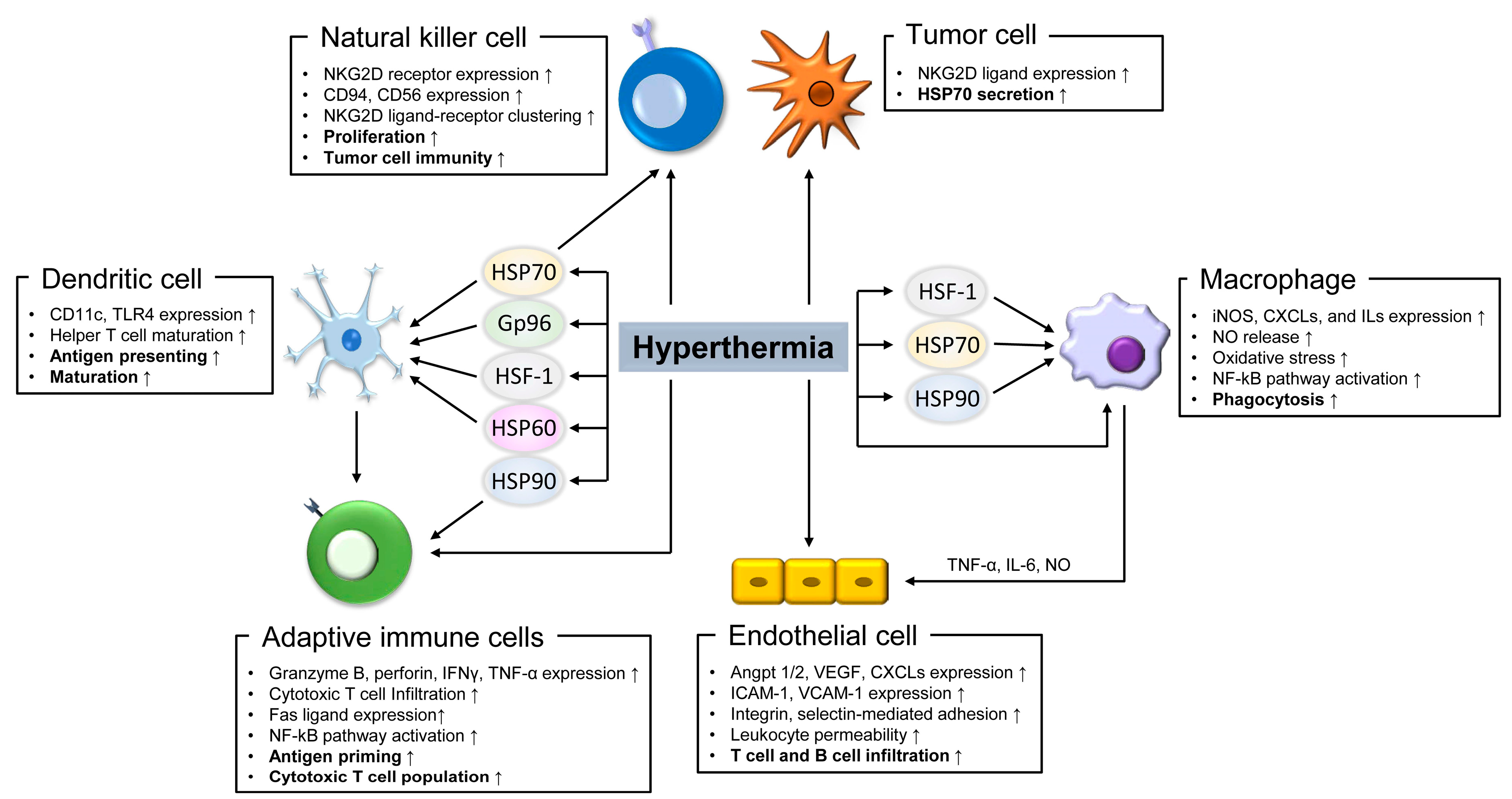
2. The Immunogenic Effect of Hyperthermia
2.1. Innate Immune Cells
2.2. Immune Cell Infiltration.
2.3. Adaptive Immune Cells
3. Molecular Mechanisms of Immunogenicity by Hyperthermia
3.1. DNA Repair
3.2. Cell Cycle Arrest and Apoptosis
3.3. Heat Shock Response
3.4. Abscopal Effect
4. Clinical Significance of the Immunogenic Effect of Hyperthermia
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| Angpt | angiopoietin; |
| ATM | ataxia telangiectasia mutated |
| BRCA | breast cancer gene |
| CTLA-4 | cytotoxic T-lymphocyte-associated protein 4 |
| CXCL | chemokine (C-C motif) ligand |
| DC | dendritic cell |
| DNA-PK | DNA-dependent protein kinase |
| FDA | Food and Drug Administration |
| HMGB1 | high motility group box protein B1 |
| HSF | heat shock transcription factor |
| Hsp | heat shock protein |
| ICAM | intracellular adhesion molecule |
| IFNγ | interferon gamma |
| iNOS | inducible nitric oxide synthase |
| NF-κB | nuclear factor kappa beta |
| NK | natural killer |
| NKG2D | natural killer lectin-like receptor gene 2D |
| NO | nitric oxide |
| PD-1 | programmed death 1 |
| PD-L1 | programmed death-ligand 1 |
| TLR | toll-like receptor |
| TNF-α | tumor necrosis factor α |
| VCAM | vascular cell adhesion molecule |
| VEGF | vascular endothelial growth factor |
References
- Santivasi, W.L.; Xia, F. Ionizing radiation-induced DNA damage, response, and repair. Antioxid. Redox Signal. 2014, 21, 251–259. [Google Scholar] [CrossRef] [PubMed]
- Lim, K.; Small, W., Jr.; Portelance, L.; Creutzberg, C.; Jurgenliemk-Schulz, I.M.; Mundt, A.; Mell, L.K.; Mayr, N.; Viswanathan, A.; Jhingran, A.; et al. Consensus guidelines for delineation of clinical target volume for intensity-modulated pelvic radiotherapy for the definitive treatment of cervix cancer. Int. J. Radiat. Oncol. Biol. Phys. 2011, 79, 348–355. [Google Scholar] [CrossRef] [PubMed]
- Bao, S.; Wu, Q.; McLendon, R.E.; Hao, Y.; Shi, Q.; Hjelmeland, A.B.; Dewhirst, M.W.; Bigner, D.D.; Rich, J.N. Glioma stem cells promote radioresistance by preferential activation of the DNA damage response. Nature 2006, 444, 756–760. [Google Scholar] [CrossRef] [PubMed]
- Diehn, M.; Cho, R.W.; Lobo, N.A.; Kalisky, T.; Dorie, M.J.; Kulp, A.N.; Qian, D.; Lam, J.S.; Ailles, L.E.; Wong, M.; et al. Association of reactive oxygen species levels and radioresistance in cancer stem cells. Nature 2009, 458, 780–783. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Boer, S.M.; Powell, M.E.; Mileshkin, L.; Katsaros, D.; Bessette, P.; Haie-Meder, C.; Ottevanger, P.B.; Ledermann, J.A.; Khaw, P.; Colombo, A.; et al. Toxicity and quality of life after adjuvant chemoradiotherapy versus radiotherapy alone for women with high-risk endometrial cancer (PORTEC-3): An open-label, multicentre, randomised, phase 3 trial. Lancet Oncol. 2016, 17, 1114–1126. [Google Scholar] [CrossRef]
- Sharabi, A.B.; Lim, M.; DeWeese, T.L.; Drake, C.G. Radiation and checkpoint blockade immunotherapy: Radiosensitisation and potential mechanisms of synergy. Lancet Oncol. 2015, 16, e498–e509. [Google Scholar] [CrossRef]
- Martin-Liberal, J.; Ochoa de Olza, M.; Hierro, C.; Gros, A.; Rodon, J.; Tabernero, J. The expanding role of immunotherapy. Cancer Treat. Rev. 2017, 54, 74–86. [Google Scholar] [CrossRef] [PubMed]
- Topalian, S.L.; Drake, C.G.; Pardoll, D.M. Immune checkpoint blockade: A common denominator approach to cancer therapy. Cancer Cell 2015, 27, 450–461. [Google Scholar] [CrossRef] [PubMed]
- Formenti, S.C.; Demaria, S. Combining radiotherapy and cancer immunotherapy: A paradigm shift. J. Natl. Cancer Inst. 2013, 105, 256–265. [Google Scholar] [CrossRef] [PubMed]
- Shi, H.; Qi, X.; Ma, B.; Cao, Y.; Wang, L.; Sun, L.; Niu, H. The status, limitation and improvement of adoptive cellular immunotherapy in advanced urologic malignancies. Chin. J. Cancer Res. 2015, 27, 128–137. [Google Scholar] [PubMed]
- Fan, Y.; Moon, J.J. Nanoparticle Drug Delivery Systems Designed to Improve Cancer Vaccines and Immunotherapy. Vaccines 2015, 3, 662–685. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pilones, K.A.; Vanpouille-Box, C.; Demaria, S. Combination of radiotherapy and immune checkpoint inhibitors. Semin. Radiat. Oncol. 2015, 25, 28–33. [Google Scholar] [CrossRef] [PubMed]
- Hato, S.V.; Khong, A.; de Vries, I.J.; Lesterhuis, W.J. Molecular pathways: The immunogenic effects of platinum-based chemotherapeutics. Clin. Cancer Res. 2014, 20, 2831–2837. [Google Scholar] [CrossRef] [PubMed]
- Garg, A.D.; Krysko, D.V.; Verfaillie, T.; Kaczmarek, A.; Ferreira, G.B.; Marysael, T.; Rubio, N.; Firczuk, M.; Mathieu, C.; Roebroek, A.J.; et al. A novel pathway combining calreticulin exposure and ATP secretion in immunogenic cancer cell death. EMBO J. 2012, 31, 1062–1079. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Workenhe, S.T.; Pol, J.G.; Lichty, B.D.; Cummings, D.T.; Mossman, K.L. Combining oncolytic HSV-1 with immunogenic cell death-inducing drug mitoxantrone breaks cancer immune tolerance and improves therapeutic efficacy. Cancer Immunol. Res. 2013, 1, 309–319. [Google Scholar] [CrossRef] [PubMed]
- Florea, A.M.; Busselberg, D. Cisplatin as an anti-tumor drug: Cellular mechanisms of activity, drug resistance and induced side effects. Cancers 2011, 3, 1351–1371. [Google Scholar] [CrossRef] [PubMed]
- Cassidy, J.; Misset, J.L. Oxaliplatin-related side effects: Characteristics and management. Semin. Oncol. 2002, 29, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Sun, W.; Wei, X.; Niu, A.; Ma, X.; Li, J.J.; Gao, D. Enhanced anti-colon cancer immune responses with modified eEF2-derived peptides. Cancer Lett. 2015, 369, 112–123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Menger, L.; Vacchelli, E.; Adjemian, S.; Martins, I.; Ma, Y.; Shen, S.; Yamazaki, T.; Sukkurwala, A.Q.; Michaud, M.; Mignot, G.; et al. Cardiac glycosides exert anticancer effects by inducing immunogenic cell death. Sci. Transl. Med. 2012, 4, 143ra99. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.M.; Wang, P.H.; Chen, S.S.; Wen, C.C.; Chen, Y.H.; Yang, W.C.; Yang, N.S. Shikonin induces immunogenic cell death in tumor cells and enhances dendritic cell-based cancer vaccine. Cancer Immunol. Immunother. 2012, 61, 1989–2002. [Google Scholar] [CrossRef] [PubMed]
- Mace, T.A.; Zhong, L.; Kokolus, K.M.; Repasky, E.A. Effector CD8+ T cell IFN-gamma production and cytotoxicity are enhanced by mild hyperthermia. Int. J. Hyperth. 2012, 28, 9–18. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.G.; Mehta, K.; Cohen, P.; Guha, C. Hyperthermia on immune regulation: A temperature’s story. Cancer Lett. 2008, 271, 191–204. [Google Scholar] [CrossRef] [PubMed]
- Schildkopf, P.; Frey, B.; Mantel, F.; Ott, O.J.; Weiss, E.M.; Sieber, R.; Janko, C.; Sauer, R.; Fietkau, R.; Gaipl, U.S. Application of hyperthermia in addition to ionizing irradiation fosters necrotic cell death and HMGB1 release of colorectal tumor cells. Biochem. Biophys. Res. Commun. 2010, 391, 1014–1020. [Google Scholar] [CrossRef] [PubMed]
- Kasdorf, E.; Perlman, J.M. Hyperthermia, inflammation, and perinatal brain injury. Pediatr. Neurol. 2013, 49, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Singh, I.S.; Hasday, J.D. Fever, hyperthermia and the heat shock response. Int. J. Hyperth. 2013, 29, 423–435. [Google Scholar] [CrossRef] [PubMed]
- Richter, K.; Haslbeck, M.; Buchner, J. The heat shock response: Life on the verge of death. Mol. Cell 2010, 40, 253–266. [Google Scholar] [CrossRef] [PubMed]
- Frey, B.; Weiss, E.M.; Rubner, Y.; Wunderlich, R.; Ott, O.J.; Sauer, R.; Fietkau, R.; Gaipl, U.S. Old and new facts about hyperthermia-induced modulations of the immune system. Int. J. hyperth. 2012, 28, 528–542. [Google Scholar] [CrossRef] [PubMed]
- Falk, M.H.; Issels, R.D. Hyperthermia in oncology. Int. J. Hyperth. 2001, 17, 1–18. [Google Scholar] [CrossRef]
- Evans, S.S.; Repasky, E.A.; Fisher, D.T. Fever and the thermal regulation of immunity: The immune system feels the heat. Nat. Rev. Immunol. 2015, 15, 335–349. [Google Scholar] [CrossRef] [PubMed]
- Roth, J.; Blatteis, C.M. Mechanisms of fever production and lysis: Lessons from experimental LPS fever. Compr. Physiol. 2014, 4, 1563–1604. [Google Scholar] [PubMed]
- Slawinska, A.; Hsieh, J.C.; Schmidt, C.J.; Lamont, S.J. Heat stress and lipopolysaccharide stimulation of chicken macrophage-like cell line activates expression of distinct sets of genes. PLoS ONE 2016, 11, e0164575. [Google Scholar] [CrossRef] [PubMed]
- Goldring, C.E.; Reveneau, S.; Chantome, A.; Pance, A.; Fleury, C.; Hume, D.A.; Sester, D.; Mignotte, B.; Jeannin, J.F. Heat shock enhances transcriptional activation of the murine-inducible nitric oxide synthase gene. FASEB J. 2000, 14, 2393–2395. [Google Scholar] [CrossRef] [PubMed]
- Shanley, T.P.; Ryan, M.A.; Eaves-Pyles, T.; Wong, H.R. Heat shock inhibits phosphorylation of I-κBα. Shock 2000, 14, 447–450. [Google Scholar] [CrossRef] [PubMed]
- Vega, V.L.; Charles, W.; Crotty Alexander, L.E. Rescuing of deficient killing and phagocytic activities of macrophages derived from non-obese diabetic mice by treatment with geldanamycin or heat shock: Potential clinical implications. Cell Stress Chaperones 2011, 16, 573–581. [Google Scholar] [CrossRef] [PubMed]
- Vega, V.L.; De Maio, A. Increase in phagocytosis after geldanamycin treatment or heat shock: Role of heat shock proteins. J. Immunol. 2005, 175, 5280–5287. [Google Scholar] [CrossRef] [PubMed]
- Miller, L.; Qureshi, M.A. Induction of heat-shock proteins and phagocytic function of chicken macrophage following in vitro heat exposure. Vet. Immunol. Immunopathol. 1992, 30, 179–191. [Google Scholar] [CrossRef]
- Zhang, H.; Zhang, L.; Yu, F.; Liu, Y.; Liang, Q.; Deng, G.; Chen, G.; Liu, M.; Xiao, X. HSF1 is a transcriptional activator of IL-10 gene expression in RAW264.7 macrophages. Inflammation 2012, 35, 1558–1566. [Google Scholar] [CrossRef] [PubMed]
- Moore, K.W.; de Waal Malefyt, R.; Coffman, R.L.; O′Garra, A. Interleukin-10 and the interleukin-10 receptor. Ann. Rev. Immunol. 2001, 19, 683–765. [Google Scholar] [CrossRef] [PubMed]
- Kovalchin, J.T.; Wang, R.; Wagh, M.S.; Azoulay, J.; Sanders, M.; Chandawarkar, R.Y. In vivo delivery of heat shock protein 70 accelerates wound healing by up-regulating macrophage-mediated phagocytosis. Wound Repair Regen. 2006, 14, 129–137. [Google Scholar] [CrossRef] [PubMed]
- Antonova, O.Y.; Yurinskaya, M.M.; Funikov, S.Y.; Evgen’ev, M.B.; Vinokurov, M.G. Exogenous heat shock protein HSP70 modulates lipopolysaccharide-induced macrophage activation. Dokl. Biochem. Biophys. 2013, 452, 320–324. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Liu, Q.; Yuan, X.; Wang, T.; Luo, S.; Lei, H.; Xia, Y. Requirement of heat shock protein 70 for inducible nitric oxide synthase induction. Cell Signal. 2013, 25, 1310–1317. [Google Scholar] [CrossRef] [PubMed]
- Scholer, C.M.; Marques, C.V.; da Silva, G.S.; Heck, T.G.; de Oliveira Junior, L.P.; Homem de Bittencourt, P.I., Jr. Modulation of rat monocyte/macrophage innate functions by increasing intensities of swimming exercise is associated with heat shock protein status. Mol. Cell. Biochem. 2016, 421, 111–125. [Google Scholar] [CrossRef] [PubMed]
- Madrigal-Matute, J.; Lopez-Franco, O.; Blanco-Colio, L.M.; Munoz-Garcia, B.; Ramos-Mozo, P.; Ortega, L.; Egido, J.; Martin-Ventura, J.L. Heat shock protein 90 inhibitors attenuate inflammatory responses in atherosclerosis. Cardiovasc. Res. 2010, 86, 330–337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, F.; Yu, Y.; Qian, J.; Wang, Y.; Cheng, B.; Dimitropoulou, C.; Patel, V.; Chadli, A.; Rudic, R.D.; Stepp, D.W.; et al. Opposing actions of heat shock protein 90 and 70 regulate nicotinamide adenine dinucleotide phosphate oxidase stability and reactive oxygen species production. Arterioscler. Thromb. Vasc. Biol. 2012, 32, 2989–2999. [Google Scholar] [CrossRef] [PubMed]
- Basu, S.; Matsutake, T. Heat shock protein-antigen presenting cell interactions. Methods 2004, 32, 38–41. [Google Scholar] [CrossRef]
- Luo, S.; Wang, T.; Qin, H.; Lei, H.; Xia, Y. Obligatory role of heat shock protein 90 in iNOS induction. Am. J. Physiol. Cell Physiol. 2011, 301, C227–C233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raizman, J.E.; Chen, Y.X.; Seibert, T.; Hibbert, B.; Cuerrier, C.M.; Salari, S.; Zhao, X.; Hu, T.; Shi, C.; Ma, X.; et al. Heat shock protein-27 attenuates foam cell formation and atherogenesis by down-regulating scavenger receptor-A expression via NF-κB signaling. Biochim. Biophys. Acta 2013, 1831, 1721–1728. [Google Scholar] [CrossRef] [PubMed]
- Li, S.S.; Xu, X.T.; Liu, W.; Xu, Z.P.; Zhang, W.W.; Li, Y.; Dong, X.X.; Yang, X.W.; Liu, F.; Wang, Y.Z.; et al. Effects of Schistosoma japonicum heat-shock protein 40 on macrophage activation. Zhongguo Xue Xi Chong Bing Fang Zhi Za Zhi 2012, 24, 137–141. [Google Scholar] [PubMed]
- Liu, J.; Hong, S.; Feng, Z.; Xin, Y.; Wang, Q.; Fu, J.; Zhang, C.; Li, G.; Luo, L.; Yin, Z. Regulation of lipopolysaccharide-induced inflammatory response by heat shock protein 27 in THP-1 cells. Cell. Immunol. 2010, 264, 127–134. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Li, C.; Wang, X.; Zhang, J.; Chang, Z. Heat shock response inhibits IL-18 expression through the JNK pathway in murine peritoneal macrophages. Biochem. Biophys. Res. Commun. 2002, 296, 742–748. [Google Scholar] [CrossRef]
- Schell, M.T.; Spitzer, A.L.; Johnson, J.A.; Lee, D.; Harris, H.W. Heat shock inhibits NF-kB activation in a dose- and time-dependent manner. J. Surg. Res. 2005, 129, 90–93. [Google Scholar] [CrossRef] [PubMed]
- Prestes-Carneiro, L.E.; Shio, M.T.; Fernandes, P.D.; Jancar, S. Cross-regulation of iNOS and COX-2 by its products in murine macrophages under stress conditions. Cell. Physiol. Biochem. 2007, 20, 283–292. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, K.; Yamamoto, N.; Hagiwara, S.; Saito, M.; Furue, H.; Shigetomi, T.; Narita, Y.; Mitsudo, K.; Tohnai, I.; Kobayashi, T.; et al. Optimization of hyperthermia and dendritic cell immunotherapy for squamous cell carcinoma. Oncol. Rep. 2011, 25, 1525–1532. [Google Scholar] [PubMed]
- Knippertz, I.; Stein, M.F.; Dorrie, J.; Schaft, N.; Muller, I.; Deinzer, A.; Steinkasserer, A.; Nettelbeck, D.M. Mild hyperthermia enhances human monocyte-derived dendritic cell functions and offers potential for applications in vaccination strategies. Int. J. Hyperth. 2011, 27, 591–603. [Google Scholar] [CrossRef] [PubMed]
- Zhao, W.; An, H.; Zhou, J.; Xu, H.; Yu, Y.; Cao, X. Hyperthermia differentially regulates TLR4 and TLR2-mediated innate immune response. Immunol. Lett. 2007, 108, 137–142. [Google Scholar] [CrossRef] [PubMed]
- Zheng, H.; Benjamin, I.J.; Basu, S.; Li, Z. Heat shock factor 1-independent activation of dendritic cells by heat shock: Implication for the uncoupling of heat-mediated immunoregulation from the heat shock response. Eur. J. Immunol. 2003, 33, 1754–1762. [Google Scholar] [CrossRef] [PubMed]
- DeFillipo, A.M.; Dai, J.; Li, Z. Heat shock-induced dendritic cell maturation is coupled by transient aggregation of ubiquitinated proteins independently of heat shock factor 1 or inducible heat shock protein 70. Mol. Immunol. 2004, 41, 785–792. [Google Scholar] [CrossRef] [PubMed]
- Redzovic, A.; Gulic, T.; Laskarin, G.; Eminovic, S.; Haller, H.; Rukavina, D. Heat-Shock Proteins 70 Induce Pro-inflammatory maturation program in decidual CD1a+ dendritic cells. Am. J. Reprod. Immunol. 2015, 74, 38–53. [Google Scholar] [CrossRef] [PubMed]
- Meng, F.D.; Sui, C.G.; Tian, X.; Li, Y.; Yang, C.M.; Ma, P.; Liu, Y.P.; Jiang, Y.H. Heat-shock protein 70 as a tumor antigen for in vitro dendritic cell pulsing in renal cell carcinoma cases. Asian Pac. J. Cancer Prev. 2014, 15, 8947–8950. [Google Scholar] [CrossRef] [PubMed]
- Fang, H.; Ang, B.; Xu, X.; Huang, X.; Wu, Y.; Sun, Y.; Wang, W.; Li, N.; Cao, X.; Wan, T. TLR4 is essential for dendritic cell activation and anti-tumor T-cell response enhancement by DAMPs released from chemically stressed cancer cells. Cell. Mol. Immunol. 2014, 11, 150–159. [Google Scholar] [CrossRef] [PubMed]
- Etminan, N.; Peters, C.; Lakbir, D.; Bunemann, E.; Borger, V.; Sabel, M.C.; Hanggi, D.; Steiger, H.J.; Stummer, W.; Sorg, R.V. Heat-shock protein 70-dependent dendritic cell activation by 5-aminolevulinic acid-mediated photodynamic treatment of human glioblastoma spheroids in vitro. Br. J. Cancer 2011, 105, 961–969. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gao, J.; Luo, S.M.; Peng, M.L.; Deng, T. Enhanced immunity against hepatoma induced by dendritic cells pulsed with Hsp70-H22 peptide complexes and CD40L. J. Cancer Res. Clin. Oncol. 2012, 138, 917–926. [Google Scholar] [CrossRef] [PubMed]
- Knudsen, S.; Schardt, A.; Buhl, T.; Boeckmann, L.; Schon, M.P.; Neumann, C.; Haenssle, H.A. Enhanced T-cell activation by immature dendritic cells loaded with HSP70-expressing heat-killed melanoma cells. Exp. Dermatol. 2010, 19, 108–116. [Google Scholar] [CrossRef] [PubMed]
- Jie, X.; Hua, L.; Jiang, W.; Feng, F.; Feng, G.; Hua, Z. Clinical application of a dendritic cell vaccine raised against heat-shocked glioblastoma. Cell Biochem. Biophys. 2012, 62, 91–99. [Google Scholar] [CrossRef] [PubMed]
- Weng, D.; Calderwood, S.K.; Gong, J. Preparation of a heat-shock protein 70-based vaccine from DC-tumor fusion cells. Methods Mol. Biol. 2011, 787, 255–265. [Google Scholar] [PubMed]
- Basu, S.; Srivastava, P.K. Fever-like temperature induces maturation of dendritic cells through induction of hsp90. Int. Immunol. 2003, 15, 1053–1061. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trojandt, S.; Reske-Kunz, A.B.; Bros, M. Geldanamycin-mediated inhibition of heat shock protein 90 partially activates dendritic cells, but interferes with their full maturation, accompanied by impaired upregulation of RelB. J. Exp. Clin. Cancer Res. 2014, 33, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Byrd, C.A.; Bornmann, W.; Erdjument-Bromage, H.; Tempst, P.; Pavletich, N.; Rosen, N.; Nathan, C.F.; Ding, A. Heat shock protein 90 mediates macrophage activation by Taxol and bacterial lipopolysaccharide. Proc. Natl. Acad. Sci. USA 1999, 96, 5645–5650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanaka, T.; Okuya, K.; Kutomi, G.; Takaya, A.; Kajiwara, T.; Kanaseki, T.; Tsukahara, T.; Hirohashi, Y.; Torigoe, T.; Hirata, K.; et al. Heat shock protein 90 targets a chaperoned peptide to the static early endosome for efficient cross-presentation by human dendritic cells. Cancer Sci. 2015, 106, 18–24. [Google Scholar] [CrossRef] [PubMed]
- Murshid, A.; Gong, J.; Calderwood, S.K. Heat shock protein 90 mediates efficient antigen cross presentation through the scavenger receptor expressed by endothelial cells-I. J. Immunol. 2010, 185, 2903–2917. [Google Scholar] [CrossRef] [PubMed]
- Ichiyanagi, T.; Imai, T.; Kajiwara, C.; Mizukami, S.; Nakai, A.; Nakayama, T.; Udono, H. Essential role of endogenous heat shock protein 90 of dendritic cells in antigen cross-presentation. J. Immunol. 2010, 185, 2693–2700. [Google Scholar] [CrossRef] [PubMed]
- Imai, T.; Kato, Y.; Kajiwara, C.; Mizukami, S.; Ishige, I.; Ichiyanagi, T.; Hikida, M.; Wang, J.Y.; Udono, H. Heat shock protein 90 (HSP90) contributes to cytosolic translocation of extracellular antigen for cross-presentation by dendritic cells. Proc. Natl. Acad. Sci. USA 2011, 108, 16363–16368. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Korba, V.D.; Heil, C.G., Jr. Eight years of fertility control with norgestrel-ethinyl estradiol (Ovral): An updated clinical review. Fertil. Steril. 1975, 26, 973–981. [Google Scholar] [CrossRef]
- Kol, A.; Bourcier, T.; Lichtman, A.H.; Libby, P. Chlamydial and human heat shock protein 60s activate human vascular endothelium, smooth muscle cells, and macrophages. J. Clin. Investig. 1999, 103, 571–577. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Radosevic-Stasic, B.; Jakovac, H.; Grebic, D.; Trobonjaca, Z.; Mrakovcic-Sutic, I.; Cuk, M. Heat shock protein Gp96 as potential regulator of morphostasis after partial hepatectomy in mice. Curr. Aging Sci. 2012, 5, 254–262. [Google Scholar] [CrossRef] [PubMed]
- Tamura, Y.; Torigoe, T.; Kukita, K.; Saito, K.; Okuya, K.; Kutomi, G.; Hirata, K.; Sato, N. Heat-shock proteins as endogenous ligands building a bridge between innate and adaptive immunity. Immunotherapy 2012, 4, 841–852. [Google Scholar] [CrossRef] [PubMed]
- Thery, C.; Regnault, A.; Garin, J.; Wolfers, J.; Zitvogel, L.; Ricciardi-Castagnoli, P.; Raposo, G.; Amigorena, S. Molecular characterization of dendritic cell-derived exosomes. Selective accumulation of the heat shock protein hsc73. J. Cell Biol. 1999, 147, 599–610. [Google Scholar] [CrossRef] [PubMed]
- Liu, A.; Ming, J.Y.; Fiskesund, R.; Ninio, E.; Karabina, S.A.; Bergmark, C.; Frostegard, A.G.; Frostegard, J. Induction of dendritic cell-mediated T-cell activation by modified but not native low-density lipoprotein in humans and inhibition by annexin a5: Involvement of heat shock proteins. Arterioscler. Thromb. Vasc. Biol. 2015, 35, 197–205. [Google Scholar] [CrossRef] [PubMed]
- Smyth, M.J.; Thia, K.Y.; Street, S.E.; Cretney, E.; Trapani, J.A.; Taniguchi, M.; Kawano, T.; Pelikan, S.B.; Crowe, N.Y.; Godfrey, D.I. Differential tumor surveillance by natural killer (NK) and NKT cells. J. Exp. Med. 2000, 191, 661–668. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ostberg, J.R.; Dayanc, B.E.; Yuan, M.; Oflazoglu, E.; Repasky, E.A. Enhancement of natural killer (NK) cell cytotoxicity by fever-range thermal stress is dependent on NKG2D function and is associated with plasma membrane NKG2D clustering and increased expression of MICA on target cells. J. Leukoc. Biol. 2007, 82, 1322–1331. [Google Scholar] [CrossRef] [PubMed]
- Farjadian, S.; Norouzian, M.; Younesi, V.; Ebrahimpour, A.; Lotfi, R. Hyperthermia increases natural killer cell cytotoxicity against SW-872 liposarcoma cell line. Iran.J. Immunol. 2013, 10, 93–102. [Google Scholar] [PubMed]
- Bae, J.H.; Kim, J.Y.; Kim, M.J.; Chang, S.H.; Park, Y.S.; Son, C.H.; Park, S.J.; Chung, J.S.; Lee, E.Y.; Kim, S.H.; et al. Quercetin enhances susceptibility to NK cell-mediated lysis of tumor cells through induction of NKG2D ligands and suppression of HSP70. J. Immunother. 2010, 33, 391–401. [Google Scholar] [CrossRef] [PubMed]
- Galazka, G.; Jurewicz, A.; Domowicz, M.; Cannella, B.; Raine, C.S.; Selmaj, K. HINT1 peptide/Hsp70 complex induces NK-cell-dependent immunoregulation in a model of autoimmune demyelination. Eur. J. Immunol. 2014, 44, 3026–3044. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.Y.; Son, Y.O.; Park, S.W.; Bae, J.H.; Chung, J.S.; Kim, H.H.; Chung, B.S.; Kim, S.H.; Kang, C.D. Increase of NKG2D ligands and sensitivity to NK cell-mediated cytotoxicity of tumor cells by heat shock and ionizing radiation. Exp. Mol. Med. 2006, 38, 474–484. [Google Scholar] [CrossRef] [PubMed]
- Multhoff, G.; Mizzen, L.; Winchester, C.C.; Milner, C.M.; Wenk, S.; Eissner, G.; Kampinga, H.H.; Laumbacher, B.; Johnson, J. Heat shock protein 70 (Hsp70) stimulates proliferation and cytolytic activity of natural killer cells. Exp. Hematol. 1999, 27, 1627–1636. [Google Scholar] [CrossRef]
- Xie, Y.; Bai, O.; Zhang, H.; Yuan, J.; Zong, S.; Chibbar, R.; Slattery, K.; Qureshi, M.; Wei, Y.; Deng, Y.; et al. Membrane-bound HSP70-engineered myeloma cell-derived exosomes stimulate more efficient CD8+ CTL- and NK-mediated antitumour immunity than exosomes released from heat-shocked tumour cells expressing cytoplasmic HSP70. J. Cell. Mol. Med. 2010, 14, 2655–2666. [Google Scholar] [CrossRef] [PubMed]
- Gross, C.; Schmidt-Wolf, I.G.; Nagaraj, S.; Gastpar, R.; Ellwart, J.; Kunz-Schughart, L.A.; Multhoff, G. Heat shock protein 70-reactivity is associated with increased cell surface density of CD94/CD56 on primary natural killer cells. Cell Stress Chaperones 2003, 8, 348–360. [Google Scholar] [CrossRef]
- Bae, J.; Munshi, A.; Li, C.; Samur, M.; Prabhala, R.; Mitsiades, C.; Anderson, K.C.; Munshi, N.C. Heat shock protein 90 is critical for regulation of phenotype and functional activity of human T lymphocytes and NK cells. J. Immunol. 2013, 190, 1360–1371. [Google Scholar] [CrossRef] [PubMed]
- Huyan, T.; Li, Q.; Dong, D.D.; Yang, H.; Zhang, J.; Huang, Q.S.; Yin, D.C.; Shang, P. Heat shock protein 90 inhibitors induce functional inhibition of human natural killer cells in a dose-dependent manner. Immunopharmacol. Immunotoxicol. 2016, 38, 77–86. [Google Scholar] [CrossRef] [PubMed]
- Botzler, C.; Issels, R.; Multhoff, G. Heat-shock protein 72 cell-surface expression on human lung carcinoma cells in associated with an increased sensitivity to lysis mediated by adherent natural killer cells. Cancer Immunol. Immunother. 1996, 43, 226–230. [Google Scholar] [CrossRef] [PubMed]
- Newman, R.G.; Dee, M.J.; Malek, T.R.; Podack, E.R.; Levy, R.B. Heat shock protein vaccination and directed IL-2 therapy amplify tumor immunity rapidly following bone marrow transplantation in mice. Blood 2014, 123, 3045–3055. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dayanc, B.E.; Bansal, S.; Gure, A.O.; Gollnick, S.O.; Repasky, E.A. Enhanced sensitivity of colon tumour cells to natural killer cell cytotoxicity after mild thermal stress is regulated through HSF1-mediated expression of MICA. Int. J. Hyperth. 2013, 29, 480–490. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, M.; Fuchs, S.; Bose, T.; Schmidt, H.; Hofmann, A.; Tonak, M.; Unger, R.; Kirkpatrick, C.J. Mild heat stress enhances angiogenesis in a co-culture system consisting of primary human osteoblasts and outgrowth endothelial cells. Tissue Eng. Part C Methods 2014, 20, 328–339. [Google Scholar] [CrossRef] [PubMed]
- Martin-Saavedra, F.M.; Wilson, C.G.; Voellmy, R.; Vilaboa, N.; Franceschi, R.T. Spatiotemporal control of vascular endothelial growth factor expression using a heat-shock-activated, rapamycin-dependent gene switch. Hum. Gene Ther. Methods 2013, 24, 160–170. [Google Scholar] [CrossRef] [PubMed]
- Hoeppner, L.H.; Phoenix, K.N.; Clark, K.J.; Bhattacharya, R.; Gong, X.; Sciuto, T.E.; Vohra, P.; Suresh, S.; Bhattacharya, S.; Dvorak, A.M.; et al. Revealing the role of phospholipase Cβ3 in the regulation of VEGF-induced vascular permeability. Blood 2012, 120, 2167–2173. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.T.; Repasky, E.A. Opposing roles for heat and heat shock proteins in macrophage functions during inflammation: A function of cell activation state? Front. Immunol. 2012, 3, 140. [Google Scholar] [CrossRef] [PubMed]
- Shevtsov, M.; Multhoff, G. Heat shock protein-peptide and HSP-based immunotherapies for the treatment of cancer. Front. Immunol. 2016, 7, 171. [Google Scholar] [CrossRef] [PubMed]
- Desreumaux, P. Specific targeting of IL-6 signalling pathway: A new way to treat IBD? Gut 2000, 47, 465–466. [Google Scholar] [CrossRef] [PubMed]
- Fonseca, S.F.; Mendonca, V.A.; Teles, M.C.; Ribeiro, V.G.; Tossige-Gomes, R.; Neves, C.D.; Rocha-Vieira, E.; Leite, L.H.; Soares, D.D.; Coimbra, C.C.; et al. Inflammatory cytokines and plasma redox status responses in hypertensive subjects after heat exposure. Braz. J. Med. Biol. Res. 2016, 49, e5026. [Google Scholar] [CrossRef] [PubMed]
- Maruo, N.; Morita, I.; Shirao, M.; Murota, S. IL-6 increases endothelial permeability in vitro. Endocrinology 1992, 131, 710–714. [Google Scholar] [PubMed]
- King, M.A.; Leon, L.R.; Morse, D.A.; Clanton, T.L. Unique cytokine and chemokine responses to exertional heat stroke in mice. J. Appl. Physiol. 2017, 122, 296–306. [Google Scholar] [CrossRef] [PubMed]
- Wung, B.S.; Ni, C.W.; Wang, D.L. ICAM-1 induction by TNFα and IL-6 is mediated by distinct pathways via Rac in endothelial cells. J. Biomed. Sci. 2005, 12, 91–101. [Google Scholar] [CrossRef] [PubMed]
- Harris, T.A.; Yamakuchi, M.; Ferlito, M.; Mendell, J.T.; Lowenstein, C.J. MicroRNA-126 regulates endothelial expression of vascular cell adhesion molecule 1. Proc. Natl. Acad. Sci. USA 2008, 105, 1516–1521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shah, A.; Unger, E.; Bain, M.D.; Bruce, R.; Bodkin, J.; Ginnetti, J.; Wang, W.C.; Seon, B.; Stewart, C.C.; Evans, S.S. Cytokine and adhesion molecule expression in primary human endothelial cells stimulated with fever-range hyperthermia. Int. J. Hyperth. 2002, 18, 534–551. [Google Scholar] [CrossRef] [PubMed]
- Eskilsson, A.; Mirrasekhian, E.; Dufour, S.; Schwaninger, M.; Engblom, D.; Blomqvist, A. Immune-induced fever is mediated by IL-6 receptors on brain endothelial cells coupled to STAT3-dependent induction of brain endothelial prostaglandin synthesis. J. Neurosci. 2014, 34, 15957–15961. [Google Scholar] [CrossRef] [PubMed]
- Engstrom, L.; Ruud, J.; Eskilsson, A.; Larsson, A.; Mackerlova, L.; Kugelberg, U.; Qian, H.; Vasilache, A.M.; Larsson, P.; Engblom, D.; et al. Lipopolysaccharide-induced fever depends on prostaglandin E2 production specifically in brain endothelial cells. Endocrinology 2012, 153, 4849–4861. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.C.; Goldman, L.M.; Schleider, D.M.; Appenheimer, M.M.; Subjeck, J.R.; Repasky, E.A.; Evans, S.S. Fever-range hyperthermia enhances L-selectin-dependent adhesion of lymphocytes to vascular endothelium. J. Immunol. 1998, 160, 961–969. [Google Scholar] [PubMed]
- Evans, S.S.; Bain, M.D.; Wang, W.C. Fever-range hyperthermia stimulates α4β7 integrin-dependent lymphocyte-endothelial adhesion. Int. J. Hyperth. 2000, 16, 45–59. [Google Scholar] [CrossRef]
- Tang, L.; Wang, K. Chronic Inflammation in Skin Malignancies. J. Mol. Signal. 2016, 11, 2. [Google Scholar]
- Takahashi, A.; Torigoe, T.; Tamura, Y.; Kanaseki, T.; Tsukahara, T.; Sasaki, Y.; Kameshima, H.; Tsuruma, T.; Hirata, K.; Tokino, T.; et al. Heat shock enhances the expression of cytotoxic granule proteins and augments the activities of tumor-associated antigen-specific cytotoxic T lymphocytes. Cell Stress Chaperones 2012, 17, 757–763. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Evans, S.S.; Wang, W.C.; Bain, M.D.; Burd, R.; Ostberg, J.R.; Repasky, E.A. Fever-range hyperthermia dynamically regulates lymphocyte delivery to high endothelial venules. Blood 2001, 97, 2727–2733. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fisher, D.T.; Chen, Q.; Skitzki, J.J.; Muhitch, J.B.; Zhou, L.; Appenheimer, M.M.; Vardam, T.D.; Weis, E.L.; Passanese, J.; Wang, W.C.; et al. IL-6 trans-signaling licenses mouse and human tumor microvascular gateways for trafficking of cytotoxic T cells. J. Clin. Investig. 2011, 121, 3846–3859. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bouchier-Hayes, L.; McBride, S.; van Geelen, C.M.; Nance, S.; Lewis, L.K.; Pinkoski, M.J.; Beere, H.M. Fas ligand gene expression is directly regulated by stress-inducible heat shock transcription factor-1. Cell Death Differ. 2010, 17, 1034–1046. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murapa, P.; Ward, M.R.; Gandhapudi, S.K.; Woodward, J.G.; D’Orazio, S.E. Heat shock factor 1 protects mice from rapid death during Listeria monocytogenes infection by regulating expression of tumor necrosis factor α during fever. Infect. Immun. 2011, 79, 177–184. [Google Scholar] [CrossRef] [PubMed]
- de Jong, H.; Koffeman, E.C.; Meerding, J.M.; Scholman, R.C.; Wieten, L.; de Jager, W.; Klein, M.; Otten, H.; van Wijk, F.; van der Zee, R.; et al. T cell recognition of naturally presented epitopes of self-heat shock protein 70. Cell Stress Chaperones 2014, 19, 569–578. [Google Scholar] [CrossRef] [PubMed]
- Li, R.; Qian, J.; Zhang, W.; Fu, W.; Du, J.; Jiang, H.; Zhang, H.; Zhang, C.; Xi, H.; Yi, Q.; et al. Human heat shock protein-specific cytotoxic T lymphocytes display potent antitumour immunity in multiple myeloma. Br. J. Haematol. 2014, 166, 690–701. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Collins, C.B.; Strassheim, D.; Aherne, C.M.; Yeckes, A.R.; Jedlicka, P.; de Zoeten, E.F. Targeted inhibition of heat shock protein 90 suppresses tumor necrosis factor-α and ameliorates murine intestinal inflammation. Inflamm. Bowel Dis. 2014, 20, 685–694. [Google Scholar] [CrossRef] [PubMed]
- Ju, Y.; Fan, H.; Liu, J.; Hu, J.; Li, X.; Li, C.; Chen, L.; Gao, Q.; Gao, G.F.; Meng, S. Heat shock protein gp96 adjuvant induces T cell responses and cross-protection to a split influenza vaccine. Vaccine 2014, 32, 2703–2711. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Song, H.; Li, J.; Wang, Y.; Yan, X.; Zhao, B.; Zhang, X.; Wang, S.; Chen, L.; Qiu, B.; et al. Hansenula polymorpha expressed heat shock protein gp96 exerts potent T cell activation activity as an adjuvant. J. Biotechnol. 2011, 151, 343–349. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Qiu, L.; Liu, G.; Li, Y.; Zhang, X.; Jin, W.; Gao, G.F.; Kong, X.; Meng, S. Heat shock protein gp96 enhances humoral and T cell responses, decreases Treg frequency and potentiates the anti-HBV activity in BALB/c and transgenic mice. Vaccine 2011, 29, 6342–6351. [Google Scholar] [CrossRef] [PubMed]
- Pawaria, S.; Binder, R.J. CD91-dependent programming of T-helper cell responses following heat shock protein immunization. Nat. Commun. 2011, 2, 521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, X.Y.; Yi, H.; Yu, X.; Zuo, D.; Subjeck, J.R. Enhancing antigen cross-presentation and T-cell priming by complexing protein antigen to recombinant large heat-shock protein. Methods Mol. Biol. 2011, 787, 277–287. [Google Scholar] [PubMed]
- Chen, W.; Wang, J.; An, H.; Zhou, J.; Zhang, L.; Cao, X. Heat shock up-regulates TLR9 expression in human B cells through activation of ERK and NF-κB signal pathways. Immunol. Lett. 2005, 98, 153–159. [Google Scholar] [CrossRef] [PubMed]
- Gandhapudi, S.K.; Murapa, P.; Threlkeld, Z.D.; Ward, M.; Sarge, K.D.; Snow, C.; Woodward, J.G. Heat shock transcription factor 1 is activated as a consequence of lymphocyte activation and regulates a major proteostasis network in T cells critical for cell division during stress. J. Immunol. 2013, 191, 4068–4079. [Google Scholar] [CrossRef] [PubMed]
- Hardy, L.; Goodman, M.; Vasquez, A.; Chauhan, D.; Anderson, K.C.; Voellmy, R.; Spector, N.L. Activation signals regulate heat shock transcription factor 1 in human B lymphocytes. J. Cell. Physiol. 1997, 170, 235–240. [Google Scholar] [CrossRef]
- Tukaj, S.; Tiburzy, B.; Manz, R.; de Castro Marques, A.; Orosz, A.; Ludwig, R.J.; Zillikens, D.; Kasperkiewicz, M. Immunomodulatory effects of heat shock protein 90 inhibition on humoral immune responses. Exp. Dermatol. 2014, 23, 585–590. [Google Scholar] [CrossRef] [PubMed]
- Houlihan, J.L.; Metzler, J.J.; Blum, J.S. HSP90α and HSP90β isoforms selectively modulate MHC class II antigen presentation in B cells. J. Immunol. 2009, 182, 7451–7458. [Google Scholar] [CrossRef] [PubMed]
- Cohen-Sfady, M.; Pevsner-Fischer, M.; Margalit, R.; Cohen, I.R. Heat shock protein 60, via MyD88 innate signaling, protects B cells from apoptosis, spontaneous and induced. J. Immunol. 2009, 183, 890–896. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Liu, D.; Yuan, Y.; Huang, S.; Shi, M.; Tao, K.; Feng, W. Overexpression of Apg-2 increases cell proliferation and protects from oxidative damage in BaF3-BCR/ABL cells. Int. J. Oncol. 2010, 36, 899–904. [Google Scholar] [PubMed]
- Overgaard, J.; Gonzalez Gonzalez, D.; Hulshof, M.C.; Arcangeli, G.; Dahl, O.; Mella, O.; Bentzen, S.M. Randomised trial of hyperthermia as adjuvant to radiotherapy for recurrent or metastatic malignant melanoma. European Society for Hyperthermic Oncology. Lancet 1995, 345, 540–543. [Google Scholar] [CrossRef]
- Kim, J.H. Combined hyperthermia and radiation therapy in cancer treatment: Current status. Cancer Investing. 1984, 2, 69–80. [Google Scholar] [CrossRef]
- Datta, N.R.; Ordonez, S.G.; Gaipl, U.S.; Paulides, M.M.; Crezee, H.; Gellermann, J.; Marder, D.; Puric, E.; Bodis, S. Local hyperthermia combined with radiotherapy and-/or chemotherapy: Recent advances and promises for the future. Cancer Treat. Rev. 2015, 41, 742–753. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Q.; Memezawa, H.; Smith, M.L.; Siesjo, B.K. Hyperthermia complicates middle cerebral artery occlusion induced by an intraluminal filament. Brain Res. 1994, 649, 253–259. [Google Scholar] [CrossRef]
- Gottlieb, C.F.; Hagmann, M.J.; Babij, T.M.; Abitbol, A.A.; Lewin, A.A.; Houdek, P.V.; Schwade, J.G. Interstitial microwave hyperthermia applicators having submillimetre diameters. Int. J. Hyperth. 1990, 6, 707–714. [Google Scholar] [CrossRef]
- Van der Zee, J.; Vujaskovic, Z.; Kondo, M.; Sugahara, T. The Kadota Fund International Forum 2004--clinical group consensus. Int. J. Hyperth. 2008, 24, 111–122. [Google Scholar] [CrossRef] [PubMed]
- Yahara, K.; Ohguri, T.; Yamaguchi, S.; Imada, H.; Narisada, H.; Ota, S.; Tomura, K.; Sakagami, M.; Fujimoto, N.; Korogi, Y. Definitive radiotherapy plus regional hyperthermia for high-risk and very high-risk prostate carcinoma: Thermal parameters correlated with biochemical relapse-free survival. Int. J. Hyperth. 2015, 31, 600–608. [Google Scholar]
- Burfeindt, M.J.; Zastrow, E.; Hagness, S.C.; Van Veen, B.D.; Medow, J.E. Microwave beamforming for non-invasive patient-specific hyperthermia treatment of pediatric brain cancer. Phys. Med. Biol. 2011, 56, 2743–2754. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, J.I.; Park, H.C.; Oh, D.; Noh, J.M.; Jung, S.H.; Kim, H.Y.; Shin, S.W.; Cho, S.K.; Sinn, D.H.; Paik, Y.H.; et al. Combination treatment of trans-arterial chemo-embolisation, radiotherapy and hyperthermia (CERT) for hepatocellular carcinoma with portal vein tumour thrombosis: Interim analysis of prospective phase II trial. Int. J. Hyperth. 2016, 32, 331–338. [Google Scholar] [CrossRef] [PubMed]
- Botsa, E.; Poulou, L.S.; Koutsogiannis, I.; Ziakas, P.D.; Koundouraki, A.; Alexopoulou, E.; Thanos, L. CT-guided radiofrequency tumor ablation in children. Pediatr. Radiol. 2014, 44, 1421–1425. [Google Scholar] [CrossRef] [PubMed]
- Facciorusso, A.; Di Maso, M.; Muscatiello, N. Microwave ablation versus radiofrequency ablation for the treatment of hepatocellular carcinoma: A systematic review and meta-analysis. Int. J. Hyperth. 2016, 32, 339–344. [Google Scholar] [CrossRef] [PubMed]
- Dovedi, S.J.; Adlard, A.L.; Lipowska-Bhalla, G.; McKenna, C.; Jones, S.; Cheadle, E.J.; Stratford, I.J.; Poon, E.; Morrow, M.; Stewart, R.; et al. Acquired resistance to fractionated radiotherapy can be overcome by concurrent PD-L1 blockade. Cancer Res. 2014, 74, 5458–5468. [Google Scholar] [CrossRef] [PubMed]
- Zeng, Z.C.; Jiang, G.L.; Wang, G.M.; Tang, Z.Y.; Curran, W.J.; Iliakis, G. DNA-PKcs subunits in radiosensitization by hyperthermia on hepatocellular carcinoma hepG2 cell line. World J. Gastroenterol. 2002, 8, 797–803. [Google Scholar] [CrossRef] [PubMed]
- Franken, N.A.; Van Bree, C.; Veltmaat, M.A.; Rodermond, H.M.; Haveman, J.; Barendsen, G.W. Radiosensitization by bromodeoxyuridine and hyperthermia: Analysis of linear and quadratic parameters of radiation survival curves of two human tumor cell lines. J. Radiat. Res. 2001, 42, 179–190. [Google Scholar] [CrossRef] [PubMed]
- Zolzer, F.; Streffer, C. Quiescence in S-phase and G1 arrest induced by irradiation and/or hyperthermia in six human tumour cell lines of different p53 status. Int. J. Radiat. Biol. 2000, 76, 717–725. [Google Scholar] [PubMed]
- Garg, A.D.; Dudek, A.M.; Agostinis, P. Cancer immunogenicity, danger signals, and DAMPs: What, when, and how? BioFactors 2013, 39, 355–367. [Google Scholar] [CrossRef] [PubMed]
- Van Oorschot, B.; Granata, G.; Di Franco, S.; Ten Cate, R.; Rodermond, H.M.; Todaro, M.; Medema, J.P.; Franken, N.A. Targeting DNA double strand break repair with hyperthermia and DNA-PKcs inhibition to enhance the effect of radiation treatment. Oncotarget 2016, 7, 65504–65513. [Google Scholar] [CrossRef] [PubMed]
- Xu, M.; Myerson, R.J.; Hunt, C.; Kumar, S.; Moros, E.G.; Straube, W.L.; Roti Roti, J.L. Transfection of human tumour cells with Mre11 siRNA and the increase in radiation sensitivity and the reduction in heat-induced radiosensitization. Int. J. Hyperth. 2004, 20, 157–162. [Google Scholar] [CrossRef]
- Xu, M.; Myerson, R.J.; Xia, Y.; Whitehead, T.; Moros, E.G.; Straube, W.L.; Roti, J.L. The effects of 41 degrees C hyperthermia on the DNA repair protein, MRE11, correlate with radiosensitization in four human tumor cell lines. Int. J. Hyperth. 2007, 23, 343–351. [Google Scholar] [CrossRef] [PubMed]
- Gerashchenko, B.I.; Gooding, G.; Dynlacht, J.R. Hyperthermia alters the interaction of proteins of the Mre11 complex in irradiated cells. Cytometry Part A 2010, 77, 940–952. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, W.G.; Seno, J.D.; Beck, B.D.; Dynlacht, J.R. Translocation of MRE11 from the nucleus to the cytoplasm as a mechanism of radiosensitization by heat. Radiat. Res. 2001, 156, 95–102. [Google Scholar] [CrossRef]
- Kaneko, H.; Igarashi, K.; Kataoka, K.; Miura, M. Heat shock induces phosphorylation of histone H2AX in mammalian cells. Biochem. Biophys. Res. Commun. 2005, 328, 1101–1106. [Google Scholar] [CrossRef] [PubMed]
- Bergs, J.W.; Oei, A.L.; Ten Cate, R.; Rodermond, H.M.; Stalpers, L.J.; Barendsen, G.W.; Franken, N.A. Dynamics of chromosomal aberrations, induction of apoptosis, BRCA2 degradation and sensitization to radiation by hyperthermia. Int. J. Mol. Med. 2016, 38, 243–250. [Google Scholar] [CrossRef] [PubMed]
- Genet, S.C.; Fujii, Y.; Maeda, J.; Kaneko, M.; Genet, M.D.; Miyagawa, K.; Kato, T.A. Hyperthermia inhibits homologous recombination repair and sensitizes cells to ionizing radiation in a time- and temperature-dependent manner. J. Cell. Physiol. 2013, 228, 1473–1481. [Google Scholar] [CrossRef] [PubMed]
- Yin, H.L.; Suzuki, Y.; Matsumoto, Y.; Tomita, M.; Furusawa, Y.; Enomoto, A.; Morita, A.; Aoki, M.; Yatagai, F.; Suzuki, T.; et al. Radiosensitization by hyperthermia in the chicken B-lymphocyte cell line DT40 and its derivatives lacking nonhomologous end joining and/or homologous recombination pathways of DNA double-strand break repair. Radiat. Res. 2004, 162, 433–441. [Google Scholar] [CrossRef] [PubMed]
- Blasiak, J.; Widera, K.; Pertynski, T. Hyperthermia can differentially modulate the repair of doxorubicin-damaged DNA in normal and cancer cells. Acta Biochim. Pol. 2003, 50, 191–195. [Google Scholar] [PubMed]
- Tomita, M. Involvement of DNA-PK and ATM in radiation- and heat-induced DNA damage recognition and apoptotic cell death. J. Radiat. Res. 2010, 51, 493–501. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, A.; Ota, I.; Tamamoto, T.; Asakawa, I.; Nagata, Y.; Nakagawa, H.; Kondo, N.; Ohnishi, K.; Furusawa, Y.; Matsumoto, H.; et al. p53-dependent hyperthermic enhancement of tumour growth inhibition by X-ray or carbon-ion beam irradiation. Int. J. Hyperth. 2003, 19, 145–153. [Google Scholar] [CrossRef]
- Mackey, M.A.; Ianzini, F. Enhancement of radiation-induced mitotic catastrophe by moderate hyperthermia. Int. J. Radiat. Biol. 2000, 76, 273–280. [Google Scholar] [PubMed]
- Kang, J.; Kim, W.; Lee, S.; Kwon, D.; Chun, J.; Son, B.; Kim, E.; Lee, J.M.; Youn, H.; Youn, B. TFAP2C promotes lung tumorigenesis and aggressiveness through miR-183- and miR-33a-mediated cell cycle regulation. Oncogene 2017, 36, 1585–1596. [Google Scholar] [CrossRef] [PubMed]
- Schildkopf, P.; Holmer, R.; Sieber, R.; Ott, O.J.; Janko, C.; Mantel, F.; Frey, B.; Fietkau, R.; Gaipl, U.S. Hyperthermia in combination with X-irradiation induces inflammatory forms of cell death. Autoimmunity 2009, 42, 311–313. [Google Scholar] [CrossRef] [PubMed]
- Cui, Y.H.; Liang, H.J.; Zhang, Q.Q.; Li, S.Q.; Li, X.R.; Huo, X.Q.; Yang, Q.H.; Li, W.W.; Gu, J.F.; Hua, Q.L.; et al. Radiosensitivity enhancement by arsenic trioxide in conjunction with hyperthermia in the EC-1 esophageal carcinoma cell line. Asian Pac. J. Cancer Prev. 2012, 13, 1693–1697. [Google Scholar] [CrossRef] [PubMed]
- Milanovic, D.; Firat, E.; Grosu, A.L.; Niedermann, G. Increased radiosensitivity and radiothermosensitivity of human pancreatic MIA PaCa-2 and U251 glioblastoma cell lines treated with the novel Hsp90 inhibitor NVP-HSP990. Radiat. Oncol. 2013, 8, 42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Werthmoller, N.; Frey, B.; Ruckert, M.; Lotter, M.; Fietkau, R.; Gaipl, U.S. Combination of ionising radiation with hyperthermia increases the immunogenic potential of B16-F10 melanoma cells in vitro and in vivo. Int. J. Hyperth. 2016, 32, 23–30. [Google Scholar] [CrossRef] [PubMed]
- Liang, H.; Zhan, H.J.; Wang, B.G.; Pan, Y.; Hao, X.S. Change in expression of apoptosis genes after hyperthermia, chemotherapy and radiotherapy in human colon cancer transplanted into nude mice. World J. Gastroenterol. 2007, 13, 4365–4371. [Google Scholar] [CrossRef] [PubMed]
- Nijhuis, E.H.; Poot, A.A.; Feijen, J.; Vermes, I. Induction of apoptosis by heat and gamma-radiation in a human lymphoid cell line; role of mitochondrial changes and caspase activation. Int. J. Hyperth. 2006, 22, 687–698. [Google Scholar] [CrossRef]
- Liu, W.; Kang, M.; Qin, Y.; Wei, Z.; Wang, R. Apoptosis-inducing effects of cetuximab combined with radiotherapy and hypothermia on human nasopharyngeal carcinoma CNE cells. Int. J. Clin. Exp. Med. 2015, 8, 2182–2189. [Google Scholar] [PubMed]
- Curry, H.A.; Clemens, R.A.; Shah, S.; Bradbury, C.M.; Botero, A.; Goswami, P.; Gius, D. Heat shock inhibits radiation-induced activation of NF-κB via inhibition of I-κB kinase. J. Biol. Chem. 1999, 274, 23061–23067. [Google Scholar] [CrossRef] [PubMed]
- Man, J.; Shoemake, J.D.; Ma, T.; Rizzo, A.E.; Godley, A.R.; Wu, Q.; Mohammadi, A.M.; Bao, S.; Rich, J.N.; Yu, J.S. Hyperthermia sensitizes glioma stem-like cells to radiation by inhibiting AKT signaling. Cancer Res. 2015, 75, 1760–1769. [Google Scholar] [CrossRef] [PubMed]
- Youn, H.; Son, B.; Kim, W.; Jun, S.Y.; Lee, J.S.; Lee, J.M.; Kang, C.; Kim, J.; Youn, B. Dissociation of MIF-rpS3 complex and sequential NF-κB activation is involved in IR-induced metastatic conversion of NSCLC. J. Cell. Biochem. 2015, 116, 2504–2516. [Google Scholar] [CrossRef] [PubMed]
- Kang, J.; Kim, W.; Kwon, T.; Youn, H.; Kim, J.S.; Youn, B. Plasminogen activator inhibitor-1 enhances radioresistance and aggressiveness of non-small cell lung cancer cells. Oncotarget 2016, 7, 23961–23974. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gabai, V.L.; Budagova, K.R.; Sherman, M.Y. Increased expression of the major heat shock protein Hsp72 in human prostate carcinoma cells is dispensable for their viability but confers resistance to a variety of anticancer agents. Oncogene 2005, 24, 3328–3338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johannsen, M.; Thiesen, B.; Gneveckow, U.; Taymoorian, K.; Waldofner, N.; Scholz, R.; Deger, S.; Jung, K.; Loening, S.A.; Jordan, A. Thermotherapy using magnetic nanoparticles combined with external radiation in an orthotopic rat model of prostate cancer. Prostate 2006, 66, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Lin, F.C.; Hsu, C.H.; Lin, Y.Y. Nano-therapeutic cancer immunotherapy using hyperthermia-induced heat shock proteins: Insights from mathematical modeling. Int. J. Nanomed. 2018, 13, 3529–3539. [Google Scholar] [CrossRef] [PubMed]
- Brondani Da Rocha, A.; Regner, A.; Grivicich, I.; Pretto Schunemann, D.; Diel, C.; Kovaleski, G.; Brunetto De Farias, C.; Mondadori, E.; Almeida, L.; Braga Filho, A.; et al. Radioresistance is associated to increased Hsp70 content in human glioblastoma cell lines. Int. J. Oncol. 2004, 25, 777–785. [Google Scholar] [CrossRef] [PubMed]
- Gibbons, N.B.; Watson, R.W.; Coffey, R.N.; Brady, H.P.; Fitzpatrick, J.M. Heat-shock proteins inhibit induction of prostate cancer cell apoptosis. Prostate 2000, 45, 58–65. [Google Scholar] [CrossRef]
- Postow, M.A.; Callahan, M.K.; Barker, C.A.; Yamada, Y.; Yuan, J.; Kitano, S.; Mu, Z.; Rasalan, T.; Adamow, M.; Ritter, E.; et al. Immunologic correlates of the abscopal effect in a patient with melanoma. N. Eng. J. Med. 2012, 366, 925–931. [Google Scholar] [CrossRef] [PubMed]
- Demaria, S.; Ng, B.; Devitt, M.L.; Babb, J.S.; Kawashima, N.; Liebes, L.; Formenti, S.C. Ionizing radiation inhibition of distant untreated tumors (abscopal effect) is immune mediated. Int. J. Radiat. Oncol. Biol. Phys. 2004, 58, 862–870. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Zhang, L.; Shi, Y.; Javidiparsijani, S.; Wang, G.; Li, X.; Ouyang, W.; Zhou, J.; Zhao, L.; Wang, X.; et al. Abscopal antitumor immune effects of magnet-mediated hyperthermia at a high therapeutic temperature on Walker-256 carcinosarcomas in rats. Oncol. Lett. 2014, 7, 764–770. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qin, W.; Akutsu, Y.; Andocs, G.; Suganami, A.; Hu, X.; Yusup, G.; Komatsu-Akimoto, A.; Hoshino, I.; Hanari, N.; Mori, M.; et al. Modulated electro-hyperthermia enhances dendritic cell therapy through an abscopal effect in mice. Oncol. Rep. 2014, 32, 2373–2379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Leeuwen, C.M.; Crezee, J.; Oei, A.L.; Franken, N.A.P.; Stalpers, L.J.A.; Bel, A.; Kok, H.P. The effect of time interval between radiotherapy and hyperthermia on planned equivalent radiation dose. Int. J. Hyperth. 2018, 34, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Myerson, R.J.; Straube, W.L.; Moros, E.G.; Emami, B.N.; Lee, H.K.; Perez, C.A.; Taylor, M.E. Simultaneous superficial hyperthermia and external radiotherapy: Report of thermal dosimetry and tolerance to treatment. Int. J. Hyperth. 1999, 15, 251–266. [Google Scholar]
- Feyerabend, T.; Wiedemann, G.J.; Jager, B.; Vesely, H.; Mahlmann, B.; Richter, E. Local hyperthermia, radiation, and chemotherapy in recurrent breast cancer is feasible and effective except for inflammatory disease. Int. J. Radiat. Oncol. Biol. Phys. 2001, 49, 1317–1325. [Google Scholar] [CrossRef]
- Harima, Y.; Nagata, K.; Harima, K.; Oka, A.; Ostapenko, V.V.; Shikata, N.; Ohnishi, T.; Tanaka, Y. Bax and Bcl-2 protein expression following radiation therapy versus radiation plus thermoradiotherapy in stage IIIB cervical carcinoma. Cancer 2000, 88, 132–138. [Google Scholar] [CrossRef] [Green Version]
- Harima, Y.; Nagata, K.; Harima, K.; Ostapenko, V.V.; Tanaka, Y.; Sawada, S. A randomized clinical trial of radiation therapy versus thermoradiotherapy in stage IIIB cervical carcinoma. Int. J. Hyperth. 2001, 17, 97–105. [Google Scholar] [CrossRef] [PubMed]
- Sakurai, H.; Hayakawa, K.; Mitsuhashi, N.; Tamaki, Y.; Nakayama, Y.; Kurosaki, H.; Nasu, S.; Ishikawa, H.; Saitoh, J.I.; Akimoto, T.; et al. Effect of hyperthermia combined with external radiation therapy in primary non-small cell lung cancer with direct bony invasion. Int. J. Hyperth. 2002, 18, 472–483. [Google Scholar] [CrossRef] [PubMed]
- Verduijn, G.M.; de Wee, E.M.; Rijnen, Z.; Togni, P.; Hardillo, J.A.U.; Ten Hove, I.; Franckena, M.; van Rhoon, G.C.; Paulides, M.M. Deep hyperthermia with the HYPERcollar system combined with irradiation for advanced head and neck carcinoma—A feasibility study. Int. J. Hyperth. 2018, 34, 1–8. [Google Scholar] [CrossRef] [PubMed]
- van der Zee, J.; Gonzalez Gonzalez, D.; van Rhoon, G.C.; van Dijk, J.D.; van Putten, W.L.; Hart, A.A. Comparison of radiotherapy alone with radiotherapy plus hyperthermia in locally advanced pelvic tumours: A prospective, randomised, multicentre trial. Lancet 2000, 355, 1119–1125. [Google Scholar] [CrossRef]
- Jones, E.L.; Oleson, J.R.; Prosnitz, L.R.; Samulski, T.V.; Vujaskovic, Z.; Yu, D.; Sanders, L.L.; Dewhirst, M.W. Randomized trial of hyperthermia and radiation for superficial tumors. J. Clin. Oncol. 2005, 23, 3079–3085. [Google Scholar] [CrossRef] [PubMed]
- Mitsumori, M.; Zeng, Z.F.; Oliynychenko, P.; Park, J.H.; Choi, I.B.; Tatsuzaki, H.; Tanaka, Y.; Hiraoka, M. Regional hyperthermia combined with radiotherapy for locally advanced non-small cell lung cancers: A multi-institutional prospective randomized trial of the International Atomic Energy Agency. Int. J. Clin. Oncol. 2007, 12, 192–198. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, I.; Emi, Y.; Hasuda, S.; Kakeji, Y.; Maehara, Y.; Sugimachi, K. Clinical application of hyperthermia combined with anticancer drugs for the treatment of solid tumors. Surgery 2002, 131, S78–S84. [Google Scholar] [CrossRef] [PubMed]
- Westermann, A.M.; Jones, E.L.; Schem, B.C.; van der Steen-Banasik, E.M.; Koper, P.; Mella, O.; Uitterhoeve, A.L.; de Wit, R.; van der Velden, J.; Burger, C.; et al. First results of triple-modality treatment combining radiotherapy, chemotherapy, and hyperthermia for the treatment of patients with stage IIB, III, and IVA cervical carcinoma. Cancer 2005, 104, 763–770. [Google Scholar] [CrossRef] [PubMed]
- Gofrit, O.N.; Shapiro, A.; Pode, D.; Sidi, A.; Nativ, O.; Leib, Z.; Witjes, J.A.; van der Heijden, A.G.; Naspro, R.; Colombo, R. Combined local bladder hyperthermia and intravesical chemotherapy for the treatment of high-grade superficial bladder cancer. Urology 2004, 63, 466–471. [Google Scholar] [CrossRef] [PubMed]
- Issels, R.D.; Lindner, L.H.; Verweij, J.; Wust, P.; Reichardt, P.; Schem, B.C.; Abdel-Rahman, S.; Daugaard, S.; Salat, C.; Wendtner, C.M.; et al. Neo-adjuvant chemotherapy alone or with regional hyperthermia for localised high-risk soft-tissue sarcoma: A randomised phase 3 multicentre study. Lancet Oncol. 2010, 11, 561–570. [Google Scholar] [CrossRef]
- Atanackovic, D.; Nierhaus, A.; Neumeier, M.; Hossfeld, D.K.; Hegewisch-Becker, S. 41.8 degrees C whole body hyperthermia as an adjunct to chemotherapy induces prolonged T cell activation in patients with various malignant diseases. Cancer Immunol. Immunother. 2002, 51, 603–613. [Google Scholar] [CrossRef] [PubMed]
- Takeda, T.; Takeda, H.; Tanaka, C.; Maruhashi, S.; Takeda, T. The effect of immunotherapy and hyperthermia for advanced or recurrent head and neck cancer—74 clinical cases. Gan Kagaku Ryoho 2014, 41, 1283–1285. [Google Scholar]
- Takeda, T.; Takeda, T.; Kobayashi, S.; Takeda, H. Immunotherapy with hyperthermia for advanced or recurrent breast cancer patients in whom standard therapy showed no effect or was refused. Gan Kagaku Ryoho 2012, 39, 1766–1769. [Google Scholar]


{kind=link}
| Signaling Pathway | Protein | Reference |
|---|---|---|
| DNA repair | DNA-PK | [135,139,147] |
| γH2AX | [139,144] | |
| MRE11 | [140,141,142,143] | |
| Rad50 | [143] | |
| NBS1 | [143] | |
| Rad51 | [145] | |
| BRCA2 | [146] | |
| Ku70 | [147] | |
| Cell cycle/Apoptosis | p53 | [149,157] |
| Cyclin-B1 | [151] | |
| HMGB1 | [152,156] | |
| Bax/Bcl-2 | [157,158,159] | |
| NF-κB | [160] | |
| Akt | [161] | |
| Heat shock response | Hsp90 | [155] |
| Hsp70 | [156,167] | |
| Hsp72 | [164,168] |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, S.; Son, B.; Park, G.; Kim, H.; Kang, H.; Jeon, J.; Youn, H.; Youn, B. Immunogenic Effect of Hyperthermia on Enhancing Radiotherapeutic Efficacy. Int. J. Mol. Sci. 2018, 19, 2795. https://doi.org/10.3390/ijms19092795
Lee S, Son B, Park G, Kim H, Kang H, Jeon J, Youn H, Youn B. Immunogenic Effect of Hyperthermia on Enhancing Radiotherapeutic Efficacy. International Journal of Molecular Sciences. 2018; 19(9):2795. https://doi.org/10.3390/ijms19092795
Chicago/Turabian StyleLee, Sungmin, Beomseok Son, Gaeul Park, Hyunwoo Kim, Hyunkoo Kang, Jaewan Jeon, HyeSook Youn, and BuHyun Youn. 2018. "Immunogenic Effect of Hyperthermia on Enhancing Radiotherapeutic Efficacy" International Journal of Molecular Sciences 19, no. 9: 2795. https://doi.org/10.3390/ijms19092795