Photodynamic Effect of Methylene Blue and Low Level Laser Radiation in Head and Neck Squamous Cell Carcinoma Cell Lines


 ,
,
Abstract
:1. Introduction
1.1. Mechanisms of PDT and Common Photosensitizer
1.2. Methylene Blue as A Photosensitizer
1.3. In Vitro Data
2. Results
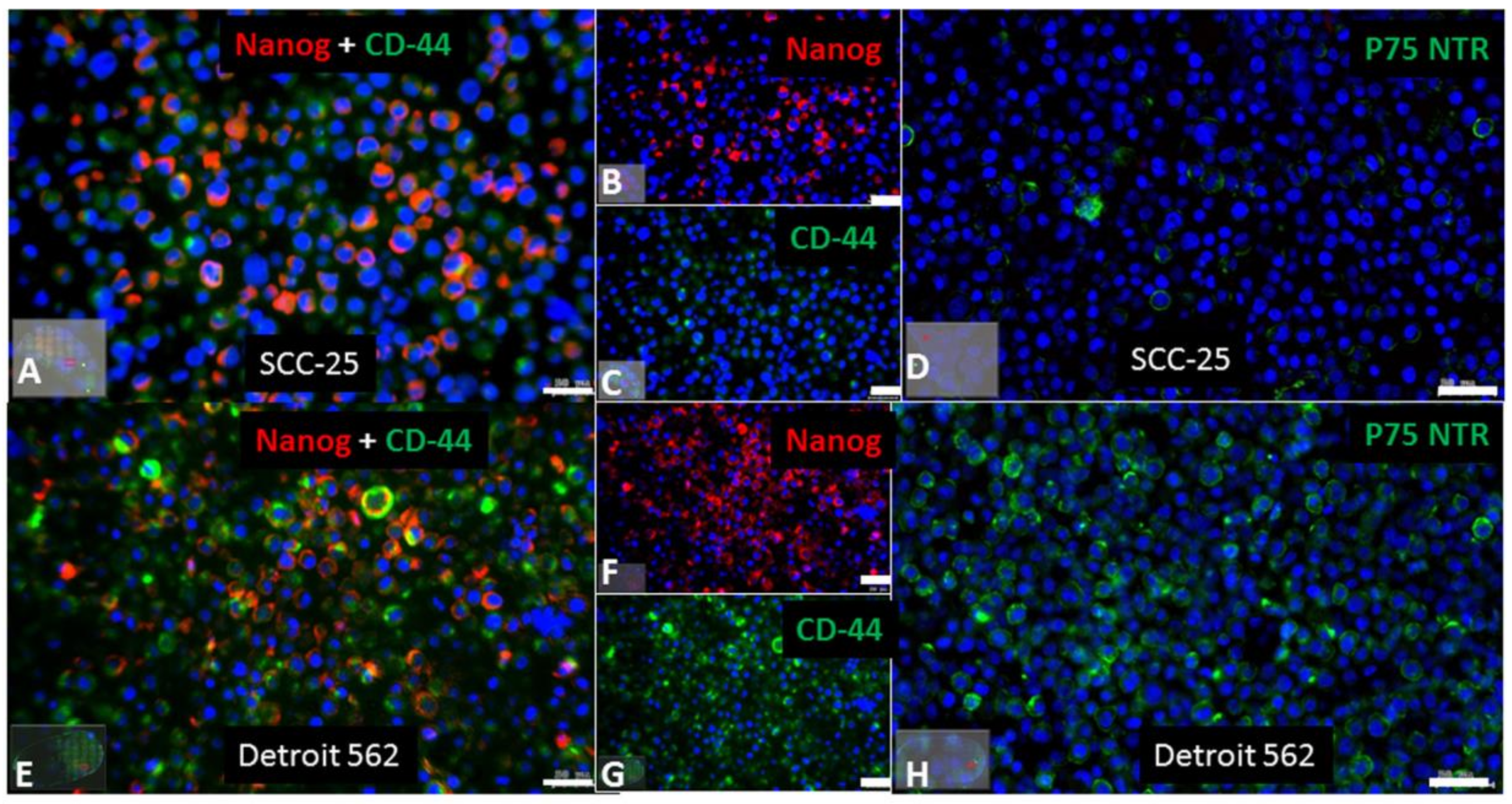
2.1. Stem Cell Characteristics in the SCC-25 and Detroit 562 Cell Lines
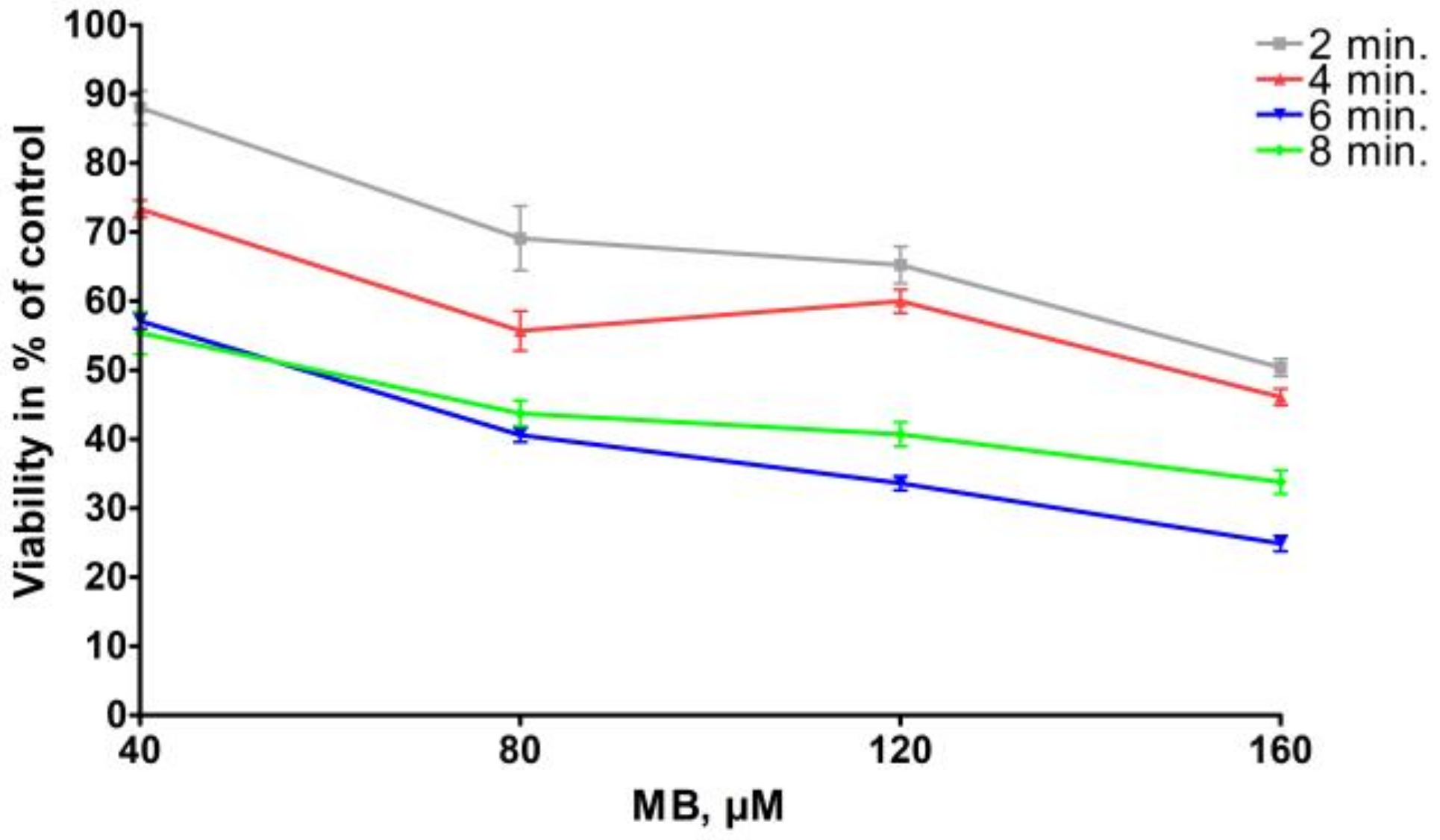
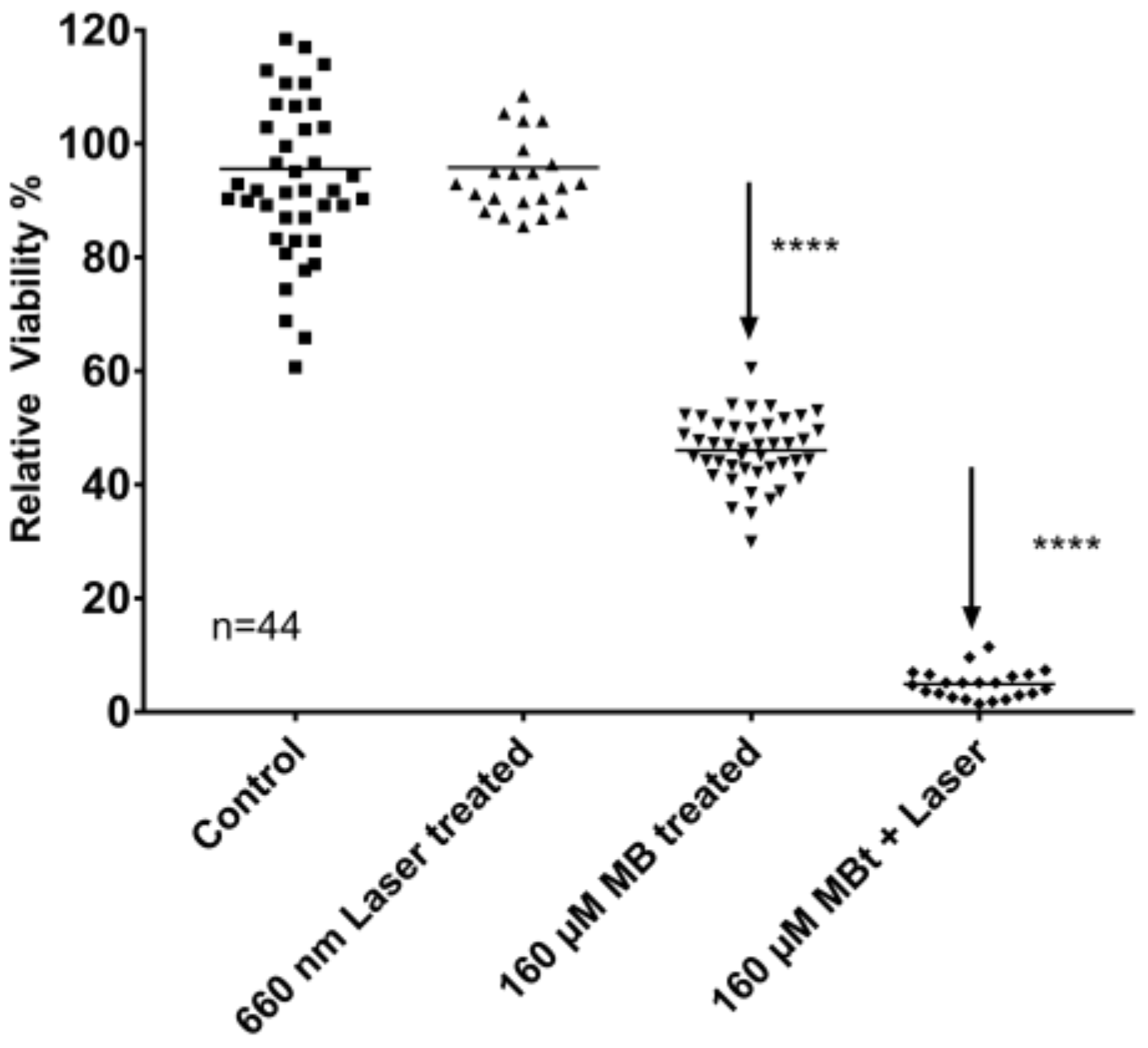
2.2. MB Effects on Cell Viability with and without Photoactivation
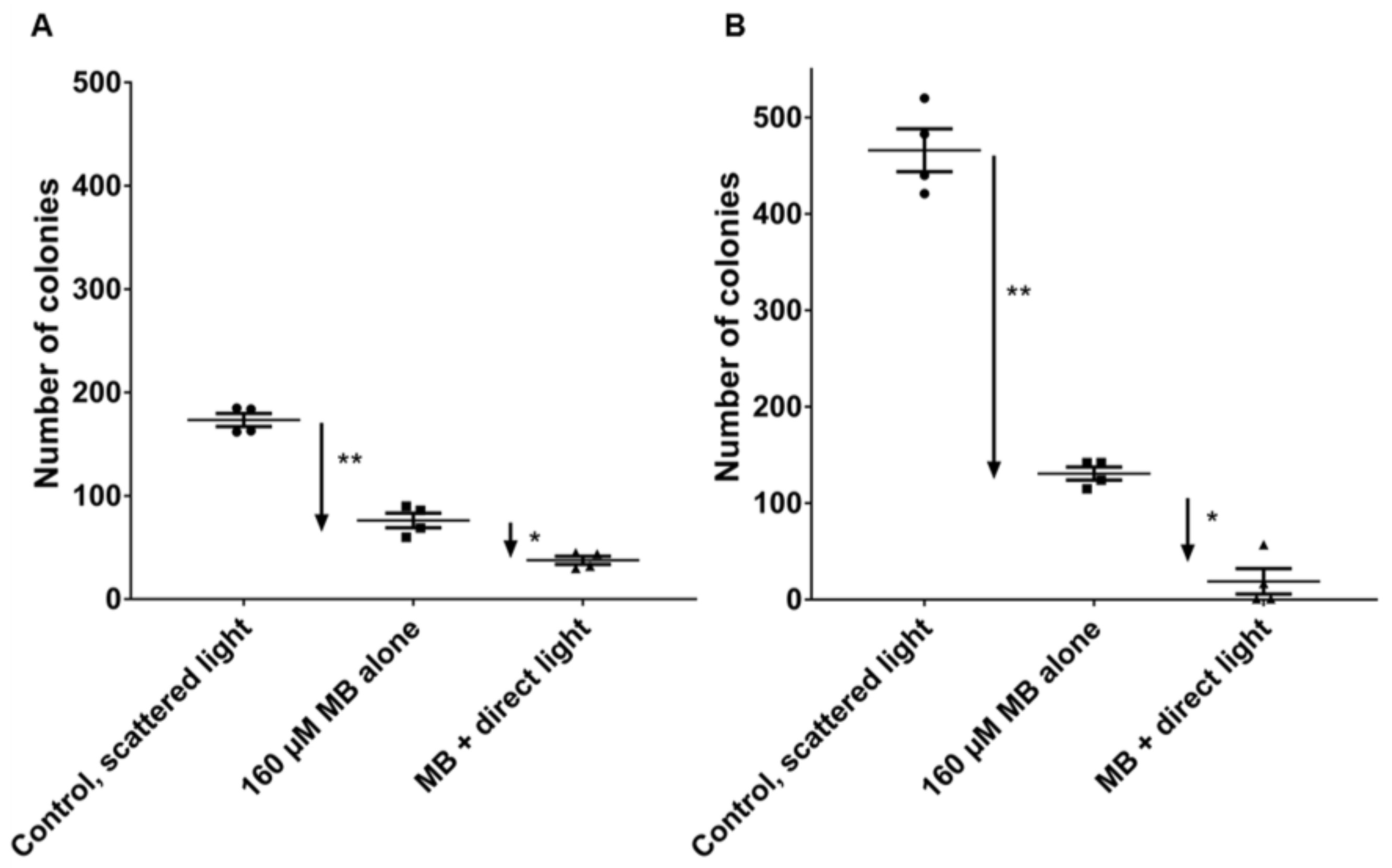
2.3. PDT Effects on Clonogenic Survival
3. Discussion
Toxicity of MB
4. Materials and Methods
4.1. Cell Lines
4.2. Evaluation of Cancer Stem Cells—Related Markers in Cultured Cell Lines
4.3. MB-Exposure
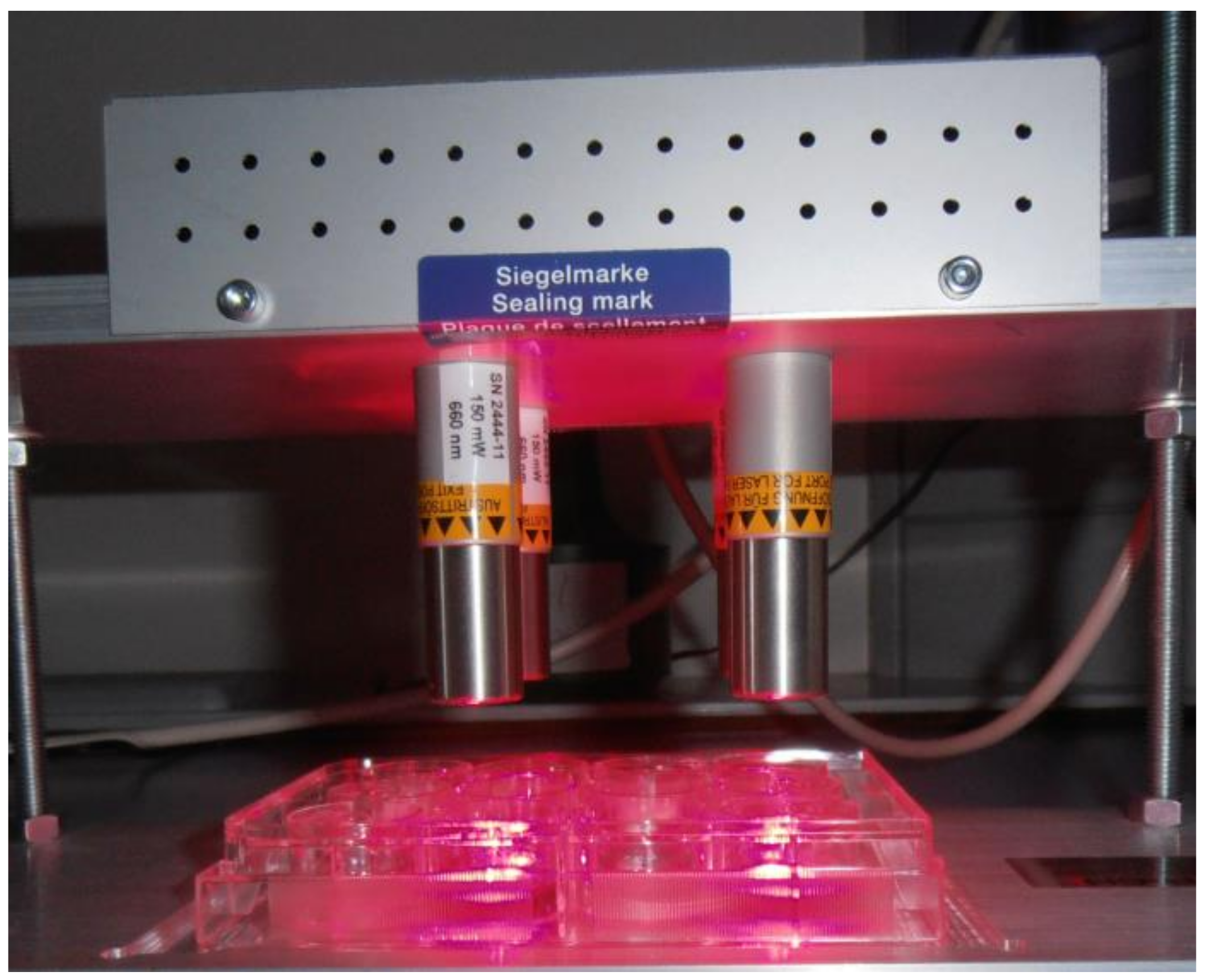
4.4. Laser Source and Treatment
4.5. MTT Assay
4.6. Clongenic Assay
4.7. Statistics
5. Conclusions
Acknowledgments
Authors Contributions
Conflicts of Interest
Abbreviations
| 5-ALA | 5-aminolevulinic acid hydrochloride |
| APDT | antimicrobial photodynamic therapy |
| DAPI | diamidino-2-phenylindole |
| DMEM/F-12 | Dulbecco’s Modified Eagle Medium/Nutrient Mixture F-12 |
| EDTA | ethylenediaminetetraacetic acid |
| FISH | fluorescence in situ hybridization |
| FBS | fetal bovine serum |
| HNSCC | head and neck squamous cell carcinoma |
| HPPH | 2-(1-Hexyloxyethyl)-2-devinyl pyropheophorbide |
| HPV | Human papilloma virus |
| LLL | low level laser |
| MB | methylene blue |
| mTHPC | meta-tetrahydroxyphenylchlorin |
| MTT | 3-(4,5-dimethylthiazol-2-yl)-2,5-diphenyltetrazolium bromide |
| PBS | Phosphate Buffered Saline |
| PDT | Photodynamic therapy |
| PPIX | protoporphyrin IX |
| SCC | squamous cell carcinoma |
| SCID | severe combined immunodeficiency |
| SRB | sulforhodamine B assay |
References
- Sunar, U. Monitoring photodynamic therapy of head and neck malignancies with optical spectroscopies. World J. Clin. Cases 2013, 1, 96–105. [Google Scholar] [CrossRef] [PubMed]
- Hopper, C.; Niziol, C.; Sidhu, M. The cost-effectiveness of Foscan mediated photodynamic therapy (Foscan-PDT) compared with extensive palliative surgery and palliative chemotherapy for patients with advanced head and neck cancer in the UK. Oral Oncol. 2004, 40, 372–382. [Google Scholar] [CrossRef] [PubMed]
- Menzin, J.; Lines, L.M.; Manning, L.N. The economics of squamous cell carcinoma of the head and neck. Curr. Opin. Otolaryngol. Head Neck Surg. 2007, 15, 68–73. [Google Scholar] [CrossRef] [PubMed]
- Wan, M.T.; Lin, J.Y. Current evidence and applications of photodynamic therapy in dermatology. Clin. Cosmet. Investig. Dermatol. 2014, 7, 145–163. [Google Scholar] [PubMed]
- Nelke, K.H.; Pawlak, W.; Leszczyszyn, J.; Gerber, H. Photodynamic therapy in head and neck cancer. Postepy Hig. Med. Dosw. (Online) 2014, 68, 119–128. [Google Scholar] [CrossRef] [PubMed]
- Jerjes, W.; Upile, T.; Hamdoon, Z.; Alexander Mosse, C.; Morcos, M.; Hopper, C. Photodynamic therapy outcome for T1/T2 N0 oral squamous cell carcinoma. Lasers. Surg. Med. 2011, 43, 463–469. [Google Scholar] [CrossRef] [PubMed]
- Karakullukcu, B.; van Oudenaarde, K.; Copper, M.P.; Klop, W.M.; van Veen, R.; Wildeman, M.; Bing Tan, I. Photodynamic therapy of early stage oral cavity and oropharynx neoplasms: An outcome analysis of 170 patients. Eur. Arch. Otorhinolaryngol. 2011, 268, 281–288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rigual, N.R.; Thankappan, K.; Cooper, M.; Sullivan, M.A.; Dougherty, T.; Popat, S.R.; Loree, T.R.; Biel, M.A.; Henderson, B. Photodynamic therapy for head and neck dysplasia and cancer. Arch. Otolaryngol. Head Neck Surg. 2009, 135, 784–788. [Google Scholar] [CrossRef] [PubMed]
- Shafirstein, G.; Rigual, N.R.; Arshad, H.; Cooper, M.T.; Bellnier, D.A.; Wilding, G.; Tan, W.; Merzianu, M.; Henderson, B.W. Photodynamic Therapy with 3-(1′-hexyloxyethyl) pyropheophorbide a (HPPH) for Early Stage Cancer of the Larynx—Phase Ib Study. Head Neck 2016. [Google Scholar] [CrossRef] [PubMed]
- Lu, K.; He, C.; Lin, W. Nanoscale metal-organic framework for highly effective photodynamic therapy of resistant head and neck cancer. J. Am. Chem. Soc. 2014, 136, 16712–16715. [Google Scholar] [CrossRef] [PubMed]
- Dolmans, D.E.; Fukumura, D.; Jain, R.K. Photodynamic therapy for cancer. Nat. Rev. Cancer 2003, 3, 380–387. [Google Scholar] [CrossRef] [PubMed]
- Dougherty, T.J.; Gomer, C.J.; Henderson, B.W.; Jori, G.; Kessel, D.; Korbelik, M.; Moan, J.; Peng, Q. Photodynamic therapy. J. Natl. Cancer Inst. 1998, 90, 889–905. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, J.C.; Marcus, S.L.; Pottier, R.H. Photodynamic therapy (PDT) and photodiagnosis (PD) using endogenous photosensitization induced by 5-aminolevulinic acid (ALA): Mechanisms and clinical results. J. Clin. Laser Med. Surg. 1996, 14, 289–304. [Google Scholar] [PubMed]
- Wang, J.D.; Quan, Z.W.; Shen, J.; Zhou, X.P.; Luo, F.H.; Wang, S.Y.; Yan, J.H.; Yang, D. Pharmacokinetics of photosensitizer m-THPC in rat models of liver cancer via orthotropic implantation using Walker-256. Zhonghua Wai Ke Za Zhi 2011, 49, 341–345. [Google Scholar] [PubMed]
- Sharman, W.M.; Allen, C.M.; van Lier, J.E. Photodynamic therapeutics: Basic principles and clinical applications. Drug. Discov. Today 1999, 4, 507–517. [Google Scholar] [CrossRef]
- Chen, C.W.; Chan, Y.C.; Hsiao, M.; Liu, R.S. Plasmon-Enhanced Photodynamic Cancer Therapy by Upconversion Nanoparticles Conjugated with Au Nanorods. ACS Appl. Mater. Interfaces 2016, 8, 32108–32119. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Arriagada, W.A.; Ramos, L.M.A.; Andrade, M.A.C.; Lopes, M.A. Efficacy of low-level laser therapy as an auxiliary tool for management of acute side effects of head and neck radiotherapy. J. Cosmet. Laser Ther. 2017. [Google Scholar] [CrossRef] [PubMed]
- De Souza, S.C.; Junqueira, J.C.; Balducci, I.; Koga-Ito, C.Y.; Munin, E.; Jorge, A.O. Photosensitization of different Candida species by low power laser light. J. Photochem. Photobiol. B 2006, 83, 34–38. [Google Scholar] [CrossRef] [PubMed]
- Usacheva, M.N.; Teichert, M.C.; Biel, M.A. Comparison of the methylene blue and toluidine blue photobactericidal efficacy against gram-positive and gram-negative microorganisms. Lasers Surg. Med. 2001, 29, 165–173. [Google Scholar] [CrossRef] [PubMed]
- Biel, M.A.; Pedigo, L.; Gibbs, A.; Loebel, N. Photodynamic therapy of antibiotic-resistant biofilms in a maxillary sinus model. Int. Forum. Allergy Rhinol. 2013, 3, 468–473. [Google Scholar] [CrossRef] [PubMed]
- Betsy, J.; Prasanth, C.S.; Baiju, K.V.; Prasanthila, J.; Subhash, N. Efficacy of antimicrobial photodynamic therapy in the management of chronic periodontitis: A randomized controlled clinical trial. J. Clin. Periodontol. 2014, 41, 573–581. [Google Scholar] [CrossRef] [PubMed]
- Leal, C.R.L.; Alvarenga, L.H.; Oliveira-Silva, T.; Kato, I.T.; Godoy-Miranda, B.; Bussadori, S.K.; Ribeiro, M.S.; Prates, R.A. Antimicrobial photodynamic therapy on Streptococcus mutans is altered by glucose in the presence of methylene blue and red LED. Photodiagn. Photodyn. Ther. 2017, 19, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Dos Santos, A.F.; Terra, L.F.; Wailemann, R.A.; Oliveira, T.C.; Gomes, V.M.; Mineiro, M.F.; Meotti, F.C.; Bruni-Cardoso, A.; Baptista, M.S.; Labriola, L. Methylene blue photodynamic therapy induces selective and massive cell death in human breast cancer cells. BMC Cancer 2017, 17, 194. [Google Scholar] [CrossRef] [PubMed]
- Da Silva Barbosa, P.; Duarte, D.A.; Leite, M.F.; de Sant’ Anna, G.R. Photodynamic therapy in pediatric dentistry. Case Rep. Dent. 2014, 2014, 217172. [Google Scholar] [CrossRef] [PubMed]
- Figueiredo Souza, L.W.; Souza, S.V.; Botelho, A.C. Randomized controlled trial comparing photodynamic therapy based on methylene blue dye and fluconazole for toenail onychomycosis. Dermatol. Ther. 2014, 27, 43–47. [Google Scholar] [CrossRef] [PubMed]
- Christian, S.; Pilch, J.; Akerman, M.E.; Porkka, K.; Laakkonen, P.; Ruoslahti, E. Nucleolin expressed at the cell surface is a marker of endothelial cells in angiogenic blood vessels. J. Cell Biol. 2003, 163, 871–878. [Google Scholar] [CrossRef] [PubMed]
- Porkka, K.; Laakkonen, P.; Hoffman, J.A.; Bernasconi, M.; Ruoslahti, E. A fragment of the HMGN2 protein homes to the nuclei of tumor cells and tumor endothelial cells in vivo. Proc. Natl. Acad. Sci. USA 2002, 99, 7444–7449. [Google Scholar] [CrossRef] [PubMed]
- Qin, M.; Hah, H.J.; Kim, G.; Nie, G.; Lee, Y.E.; Kopelman, R. Methylene blue covalently loaded polyacrylamide nanoparticles for enhanced tumor-targeted photodynamic therapy. Photochem. Photobiol. Sci. 2011, 10, 832–841. [Google Scholar] [CrossRef] [PubMed]
- Fan, Z.; Dai, X.; Lu, Y.; Yu, E.; Brahmbatt, N.; Carter, N.; Tchouwou, C.; Singh, A.K.; Jones, Y.; Yu, H.; et al. Enhancing targeted tumor treatment by near IR light-activatable photodynamic-photothermal synergistic therapy. Mol. Pharm. 2014, 11, 1109–1116. [Google Scholar] [CrossRef] [PubMed]
- El-Khatib, M.; Tepe, C.; Senger, B.; Dibue-Adjei, M.; Riemenschneider, M.J.; Stummer, W.; Steiger, H.J.; Cornelius, J.F. Aminolevulinic Acid-mediated photodynamic therapy of human meningioma: An in vitro study on primary cell lines. Int. J. Mol. Sci. 2015, 16, 9936–9948. [Google Scholar] [CrossRef] [PubMed]
- Mirzaei, H.; Djavid, G.E.; Hadizadeh, M.; Jahanshiri-Moghadam, M.; Hajian, P. The efficacy of Radachlorin-mediated photodynamic therapy in human hepatocellular carcinoma cells. J. Photochem. Photobiol. B 2015, 142, 86–91. [Google Scholar] [CrossRef] [PubMed]
- Betz, C.S.; Lai, J.P.; Xiang, W.; Janda, P.; Heinrich, P.; Stepp, H.; Baumgartner, R.; Leunig, A. In vitro photodynamic therapy of nasopharyngeal carcinoma using 5-aminolevulinic acid. Photochem. Photobiol. Sci. 2002, 1, 315–319. [Google Scholar] [CrossRef] [PubMed]
- Guan, J.; Lai, X.; Wang, X.; Leung, A.W.; Zhang, H.; Xu, C. Photodynamic action of methylene blue in osteosarcoma cells in vitro. Photodiagn. Photodyn. Ther. 2014, 11, 13–19. [Google Scholar] [CrossRef] [PubMed]
- Dudas, J.; Bitsche, M.; Schartinger, V.; Falkeis, C.; Sprinzl, G.M.; Riechelmann, H. Fibroblasts produce brain-derived neurotrophic factor and induce mesenchymal transition of oral tumor cells. Oral Oncol. 2011, 47, 98–103. [Google Scholar] [CrossRef] [PubMed]
- Rheinwald, J.G.; Beckett, M.A. Tumorigenic keratinocyte lines requiring anchorage and fibroblast support cultured from human squamous cell carcinomas. Cancer Res. 1981, 41, 1657–1663. [Google Scholar] [PubMed]
- Chen, Y.W.; Lin, G.J.; Chia, W.T.; Lin, C.K.; Chuang, Y.P.; Sytwu, H.K. Triptolide exerts anti-tumor effect on oral cancer and KB cells in vitro and in vivo. Oral Oncol. 2009, 45, 562–568. [Google Scholar] [CrossRef] [PubMed]
- Sinha, U.K.; Schorn, V.J.; Hochstim, C.; Chinn, S.B.; Zhu, S.; Masood, R. Increased radiation sensitivity of head and neck squamous cell carcinoma with sphingosine kinase 1 inhibition. Head Neck 2011, 33, 178–188. [Google Scholar] [CrossRef] [PubMed]
- Sano, D.; Xie, T.X.; Ow, T.J.; Zhao, M.; Pickering, C.R.; Zhou, G.; Sandulache, V.C.; Wheeler, D.A.; Gibbs, R.A.; Caulin, C.; et al. Disruptive TP53 mutation is associated with aggressive disease characteristics in an orthotopic murine model of oral tongue cancer. Clin. Cancer Res. 2011, 17, 6658–6670. [Google Scholar] [CrossRef] [PubMed]
- Peterson, W.D., Jr.; Stulberg, C.S.; Simpson, W.F. A permanent heteroploid human cell line with type B glucose-6-phosphate dehydrogenase. Proc. Soc. Exp. Biol. Med. 1971, 136, 1187–1191. [Google Scholar] [CrossRef] [PubMed]
- Peterson, W.D., Jr.; Stulberg, C.S.; Swanborg, N.K.; Robinson, A.R. Glucose-6-phosphate dehydrogenase isoenzymes in human cell cultures determined by sucrose-agar gel and cellulose acetate zymograms. Proc. Soc. Exp. Biol. Med. 1968, 128, 772–776. [Google Scholar] [CrossRef] [PubMed]
- Martin, D.; Abba, M.C.; Molinolo, A.A.; Vitale-Cross, L.; Wang, Z.; Zaida, M.; Delic, N.C.; Samuels, Y.; Lyons, J.G.; Gutkind, J.S. The head and neck cancer cell oncogenome: A platform for the development of precision molecular therapies. Oncotarget 2014, 5, 8906–8923. [Google Scholar] [CrossRef] [PubMed]
- Marynka-Kalmani, K.; Treves, S.; Yafee, M.; Rachima, H.; Gafni, Y.; Cohen, M.A.; Pitaru, S. The lamina propria of adult human oral mucosa harbors a novel stem cell population. Stem. Cells 2010, 28, 984–995. [Google Scholar] [CrossRef] [PubMed]
- Schartinger, V.H.; Galvan, O.; Riechelmann, H.; Dudas, J. Differential responses of fibroblasts, non-neoplastic epithelial cells, and oral carcinoma cells to low-level laser therapy. Support Care Cancer 2012, 20, 523–529. [Google Scholar] [CrossRef] [PubMed]
- Bernas, T.; Dobrucki, J. Mitochondrial and nonmitochondrial reduction of MTT: Interaction of MTT with TMRE, JC-1, and NAO mitochondrial fluorescent probes. Cytometry 2002, 47, 236–242. [Google Scholar] [CrossRef] [PubMed]
- Morton, C.A.; Szeimies, R.M.; Sidoroff, A.; Braathen, L.R. European guidelines for topical photodynamic therapy part 1: Treatment delivery and current indications—Actinic keratoses, Bowen's disease, basal cell carcinoma. J. Eur. Acad. Dermatol. Venereol. 2013, 27, 536–544. [Google Scholar] [CrossRef] [PubMed]
- Truchuelo, M.; Fernandez-Guarino, M.; Fleta, B.; Alcantara, J.; Jaen, P. Effectiveness of photodynamic therapy in Bowen's disease: An observational and descriptive study in 51 lesions. J. Eur. Acad. Dermatol. Venereol. 2012, 26, 868–874. [Google Scholar] [CrossRef] [PubMed]
- Hodgkinson, N.; Kruger, C.A.; Abrahamse, H. Targeted photodynamic therapy as potential treatment modality for the eradication of colon cancer and colon cancer stem cells. Tumor Biol. 2017, 39, 1010428317734691. [Google Scholar] [CrossRef] [PubMed]
- Usacheva, M.; Swaminathan, S.K.; Kirtane, A.R.; Panyam, J. Enhanced photodynamic therapy and effective elimination of cancer stem cells using surfactant-polymer nanoparticles. Mol. Pharm. 2014, 11, 3186–3195. [Google Scholar] [CrossRef] [PubMed]
- Karakullukcu, B.; Stoker, S.D.; Wildeman, A.P.; Copper, M.P.; Wildeman, M.A.; Tan, I.B. A matched cohort comparison of mTHPC-mediated photodynamic therapy and trans-oral surgery of early stage oral cavity squamous cell cancer. Eur. Arch. Otorhinolaryngol. 2013, 270, 1093–1097. [Google Scholar] [CrossRef] [PubMed]
- Rigual, N.; Shafirstein, G.; Cooper, M.T.; Baumann, H.; Bellnier, D.A.; Sunar, U.; Tracy, E.C.; Rohrbach, D.J.; Wilding, G.; Tan, W.; et al. Photodynamic therapy with 3-(1′-hexyloxyethyl) pyropheophorbide a for cancer of the oral cavity. Clin. Cancer Res. 2013, 19, 6605–6613. [Google Scholar] [CrossRef] [PubMed]
- Rigual, N.R.; Shafirstein, G.; Frustino, J.; Seshadri, M.; Cooper, M.; Wilding, G.; Sullivan, M.A.; Henderson, B. Adjuvant intraoperative photodynamic therapy in head and neck cancer. JAMA Otolaryngol. Head Neck Surg. 2013, 139, 706–711. [Google Scholar] [CrossRef] [PubMed]
- Ikeda, H.; Tobita, T.; Ohba, S.; Uehara, M.; Asahina, I. Treatment outcome of Photofrin-based photodynamic therapy for T1 and T2 oral squamous cell carcinoma and dysplasia. Photodiagn. Photodyn. Ther. 2013, 10, 229–235. [Google Scholar] [CrossRef] [PubMed]
- de Visscher, S.A.; Melchers, L.J.; Dijkstra, P.U.; Karakullukcu, B.; Tan, I.B.; Hopper, C.; Roodenburg, J.L.; Witjes, M.J. mTHPC-mediated photodynamic therapy of early stage oral squamous cell carcinoma: A comparison to surgical treatment. Ann. Surg. Oncol. 2013, 20, 3076–3082. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, M.; Fujita, H.; Katase, N.; Inoue, K.; Nagatsuka, H.; Utsumi, K.; Sasaki, J.; Ohuchi, H. Improvement of the efficacy of 5-aminolevulinic acid-mediated photodynamic treatment in human oral squamous cell carcinoma HSC-4. Acta Med. Okayama 2013, 67, 153–164. [Google Scholar] [PubMed]
- Peng, Q.; Warloe, T.; Moan, J.; Godal, A.; Apricena, F.; Giercksky, K.E.; Nesland, J.M. Antitumor effect of 5-aminolevulinic acid-mediated photodynamic therapy can be enhanced by the use of a low dose of photofrin in human tumor xenografts. Cancer Res. 2001, 61, 5824–5832. [Google Scholar] [PubMed]
- Wagner, M.; Suarez, E.R.; Theodoro, T.R.; Machado Filho, C.D.; Gama, M.F.; Tardivo, J.P.; Paschoal, F.M.; Pinhal, M.A. Methylene blue photodynamic therapy in malignant melanoma decreases expression of proliferating cell nuclear antigen and heparanases. Clin. Exp. Dermatol. 2012, 37, 527–533. [Google Scholar] [CrossRef] [PubMed]
- Lim, E.J.; Oak, C.H.; Heo, J.; Kim, Y.H. Methylene blue-mediated photodynamic therapy enhances apoptosis in lung cancer cells. Oncol. Rep. 2013, 30, 856–862. [Google Scholar] [CrossRef] [PubMed]
- Kirszberg, C.; Rumjanek, V.M.; Capella, M.A. Methylene blue is more toxic to erythroleukemic cells than to normal peripheral blood mononuclear cells: A possible use in chemotherapy. Cancer Chemother. Pharmacol. 2005, 56, 659–665. [Google Scholar] [CrossRef] [PubMed]
- Wainwright, M.; Phoenix, D.A.; Rice, L.; Burrow, S.M.; Waring, J. Increased cytotoxicity and phototoxicity in the methylene blue series via chromophore methylation. J. Photochem. Photobiol. B 1997, 40, 233–239. [Google Scholar] [CrossRef]
- Lee, Y.S.; Wurster, R.D. Methylene blue induces cytotoxicity in human brain tumor cells. Cancer Lett. 1995, 88, 141–145. [Google Scholar] [CrossRef]
- National Toxicology Program. Toxicology and carcinogenesis studies of methylene blue trihydrate (Cas No. 7220-79-3) in F344/N rats and B6C3F1 mice (gavage studies). Natl. Toxicol. Program Tech. Rep. Ser. 2008, 540, 1–224. [Google Scholar]
- Chang, Y.S.; Tseng, S.Y.; Tseng, S.H. Comparison of dyes for cataract surgery. Part 2: Efficacy of capsule staining in a rabbit model. J. Cataract Refract. Surg. 2005, 31, 799–804. [Google Scholar] [CrossRef] [PubMed]
- Dudás, J.; Fullár, A.; Bitsche, M.; Schartinger, V.; Kovalszky, I.; Sprinzl, G.M.; Riechelmann, H. Tumor-produced, active interleukin-1β regulates gene expression in carcinoma-associated fibroblasts. Exp. Cell Res. 2011, 317, 2222–2229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dudás, J.; Fullár, A.; Romani, A.; Pritz, C.; Kovalszky, I.; Hans Schartinger, V.; Mathias Sprinzl, G.; Riechelmann, H. Curcumin targets fibroblast-tumor cell interactions in oral squamous cell carcinoma. Exp. Cell Res. 2013, 319, 800–809. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fullár, A.; Kovalszky, I.; Bitsche, M.; Romani, A.; Schartinger, V.H.; Sprinzl, G.M.; Riechelmann, H.; Dudás, J. Tumor cell and carcinoma-associated fibroblast interaction regulates matrix metalloproteinases and their inhibitors in oral squamous cell carcinoma. Exp. Cell Res. 2012, 318, 1517–1527. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steinbichler, T.B.; Metzler, V.; Pritz, C.; Riechelmann, H.; Dudas, J. Tumor-associated fibroblast-conditioned medium induces CDDP resistance in HNSCC cells. Oncotarget 2015, 7, 2508. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.J.; Choi, Y.I.; Kim, L.; Park, I.S.; Han, J.Y.; Kim, J.M.; Chu, Y.C. Preparation of compact agarose cell blocks from the residues of liquid-based cytology samples. Korean J. Pathol. 2014, 48, 351–360. [Google Scholar] [CrossRef] [PubMed]
- Dudas, J.; Schartinger, V.H.; Romani, A.; Schweigl, G.; Kordsmeyer, K.; Marta, P.I.; Url, C.; Kral, F.; Riechelmann, H. Cell cycle association and hypoxia regulation of excision repair cross complementation group 1 protein (ERCC1) in tumor cells of head and neck cancer. Tumor Biol. 2014, 35, 7807–7819. [Google Scholar] [CrossRef] [PubMed]
- Schindelin, J.; Arganda-Carreras, I.; Frise, E.; Kaynig, V.; Longair, M.; Pietzsch, T.; Preibisch, S.; Rueden, C.; Saalfeld, S.; Schmid, B.; et al. Fiji: An open-source platform for biological-image analysis. Nat. Methods 2012, 9, 676–682. [Google Scholar] [CrossRef] [PubMed]
- Montironi, R.; Mazzucchelli, R. Reflection on the past, present and future of analytical and quantitative cytology and histology. Anal. Quant. Cytol. Histol. 2008, 30, 249–253. [Google Scholar] [PubMed]
- Obstoy, B.; Salaun, M.; Bohn, P.; Veresezan, L.; Sesboue, R.; Thiberville, L. Photodynamic therapy using methylene blue in lung adenocarcinoma xenograft and hamster cheek pouch induced squamous cell carcinoma. Photodiagn. Photodyn. Ther. 2016, 15, 109–114. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| MB-Exposure (min) | 40 | 80 | 120 | 160 | |
|---|---|---|---|---|---|
| % Viability | 2 | 88 | 69 | 65 | 50 |
| 4 | 73 | 56 | 60 | 46 | |
| 6 | 57 | 41 | 34 | 25 | |
| 8 | 55 | 44 | 41 | 34 |
| 660 nm Laser Exposure (min) | MB-Exposure (min) | MB Concentration, µM | ||||
|---|---|---|---|---|---|---|
| 40 | 80 | 120 | 160 | |||
| % of viable cells | 0 | 2 | 88 | 69 | 65 | 50 |
| 0 | 4 | 73 | 56 | 60 | 46 | |
| 0 | 6 | 57 | 41 | 34 | 25 | |
| 0 | 8 | 55 | 44 | 41 | 34 | |
| 2 | 2 | 66 | 54 | 41 | 31 | |
| 2 | 4 | 51 | 39 | 34 | 29 | |
| 2 | 6 | 40 | 14 | 10 | 22 | |
| 2 | 8 | 28 | 23 | 18 | 12 | |
| 4 | 2 | 52 | 39 | 31 | 27 | |
| 4 | 4 | 64 | 44 | 35 | 24 | |
| 4 | 6 | 30 | 14 | 7 | 3 | |
| 4 | 8 | 21 | 14 | 8 | 8 | |
| 6 | 2 | 49 | 38 | 30 | 30 | |
| 6 | 4 | 69 | 55 | 33 | 25 | |
| 6 | 6 | 31 | 6 | 8 | 4 | |
| 6 | 8 | 19 | 14 | 7 | 6 | |
| 8 | 2 | 46 | 38 | 36 | 27 | |
| 8 | 4 | 39 | 8 | 8 | 5 | |
| 8 | 6 | 26 | 3 | 2 | 2 | |
| 8 | 8 | 19 | 11 | 5 | 3 | |
| Viablility % difference to t = 0 min Laser exposure | 2 | 2 | 22 | 16 | 24 | 19 |
| 2 | 4 | 22 | 16 | 26 | 17 | |
| 2 | 6 | 17 | 27 | 24 | 3 | |
| 2 | 8 | 28 | 20 | 23 | 22 | |
| 4 | 2 | 36 | 30 | 34 | 23 | |
| 4 | 4 | 9 | 12 | 25 | 22 | |
| 4 | 6 | 27 | 27 | 27 | 22 | |
| 4 | 8 | 35 | 29 | 32 | 26 | |
| 6 | 2 | 39 | 31 | 35 | 20 | |
| 6 | 4 | 5 | 0 | 27 | 21 | |
| 6 | 6 | 26 | 35 | 26 | 21 | |
| 6 | 8 | 36 | 30 | 34 | 28 | |
| 8 | 2 | 42 | 31 | 30 | 24 | |
| 8 | 4 | 34 | 47 | 52 | 41 | |
| 8 | 6 | 31 | 38 | 32 | 23 | |
| 8 | 8 | 36 | 32 | 36 | 30 | |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kofler, B.; Romani, A.; Pritz, C.; Steinbichler, T.B.; Schartinger, V.H.; Riechelmann, H.; Dudas, J. Photodynamic Effect of Methylene Blue and Low Level Laser Radiation in Head and Neck Squamous Cell Carcinoma Cell Lines. Int. J. Mol. Sci. 2018, 19, 1107. https://doi.org/10.3390/ijms19041107
Kofler B, Romani A, Pritz C, Steinbichler TB, Schartinger VH, Riechelmann H, Dudas J. Photodynamic Effect of Methylene Blue and Low Level Laser Radiation in Head and Neck Squamous Cell Carcinoma Cell Lines. International Journal of Molecular Sciences. 2018; 19(4):1107. https://doi.org/10.3390/ijms19041107
Chicago/Turabian StyleKofler, Barbara, Angela Romani, Christian Pritz, Teresa Bernadette Steinbichler, Volker Hans Schartinger, Herbert Riechelmann, and Jozsef Dudas. 2018. "Photodynamic Effect of Methylene Blue and Low Level Laser Radiation in Head and Neck Squamous Cell Carcinoma Cell Lines" International Journal of Molecular Sciences 19, no. 4: 1107. https://doi.org/10.3390/ijms19041107