
Pneumococcus and the Elderly in Italy: A Summary of Available Evidence Regarding Carriage, Clinical Burden of Lower Respiratory Tract Infections and On-Field Effectiveness of PCV13 Vaccination

 and
and 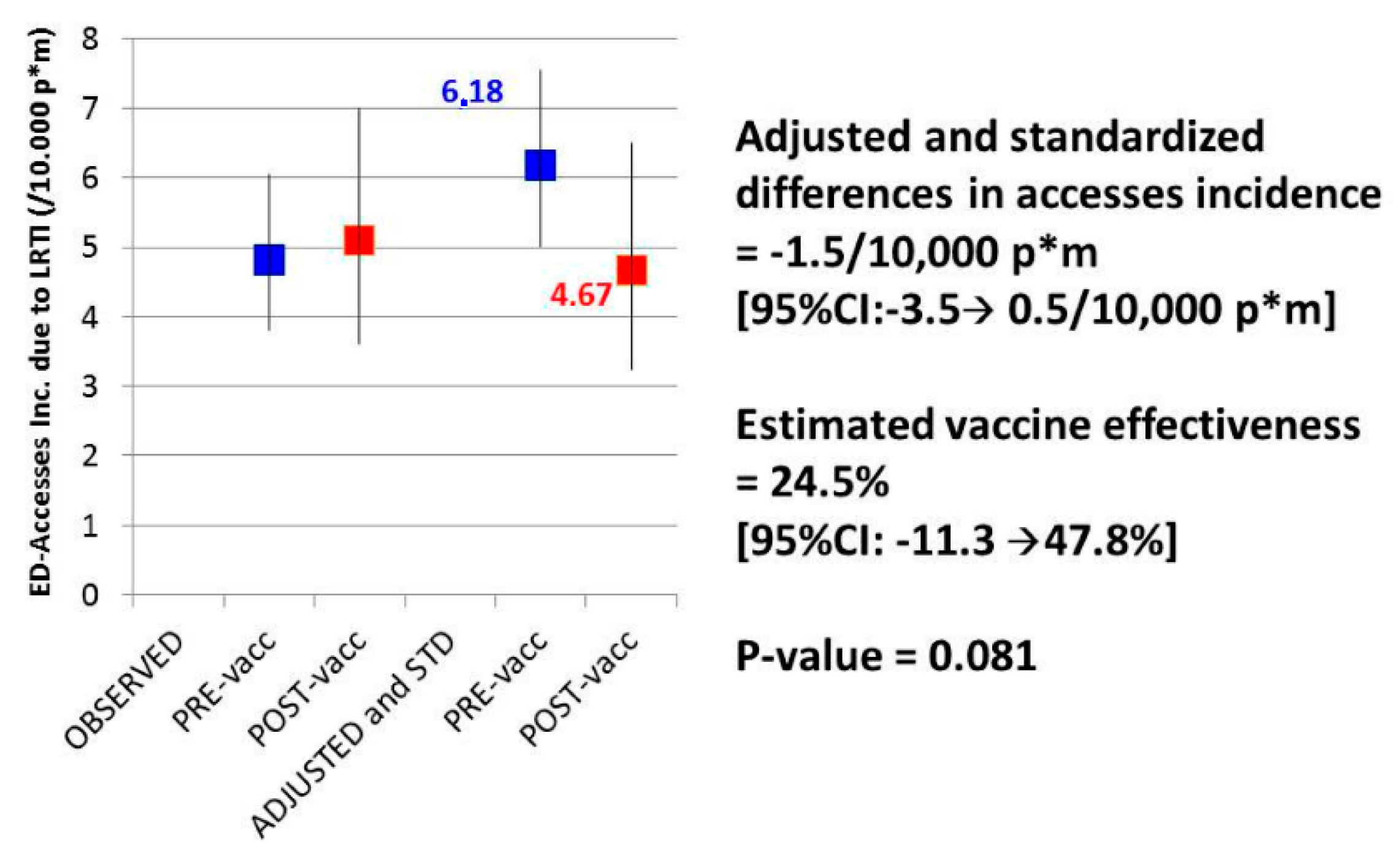{kind=link}
Abstract
:1. Introduction
2. Mechanisms of Protection Afforded by Pneumococcal Conjugate Vaccines
3. Estimates of Pneumococcal Carriage in Adults and the Elderly
4. Clinical Burden of CAP and LRTI in Adults
5. Evaluations of On-Field Effectiveness of PCV13 Immunization in Adults
6. Future Perspectives
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Weycker, D.; Strutton, D.; Edelsberg, J.; Sato, R.; Jackson, L.A. Clinical and economic burden of pneumococcal disease in older US adults. Vaccine 2010, 28, 4955–4960. [Google Scholar] [CrossRef] [PubMed]
- File, T.M., Jr.; Marrie, T.J. Burden of community-acquired pneumonia in North American adults. Postgrad. Med. 2010, 122, 130–141. [Google Scholar] [CrossRef] [PubMed]
- Millett, E.R.; Quint, J.K.; Smeeth, L.; Daniel, R.M.; Thomas, S.L. Incidence of community-acquired lower respiratory tract infections and pneumonia among older adults in the United Kingdom: A population-based study. PLoS ONE 2013, 8, e75131. [Google Scholar] [CrossRef] [PubMed]
- Bartlett, J.G.; Mundy, L.M. Community-acquired pneumonia. N. Engl. J. Med. 1995, 333, 1618–1624. [Google Scholar] [CrossRef] [PubMed]
- Macfarlane, J.; Holmes, W.; Gard, P.; Macfarlane, R.; Rose, D.; Weston, V.; Leinonen, M.; Saikku, P.; Myint, S. Prospective study of the incidence, aetiology and outcome of adult lower respiratory tract illness in the community. Thorax 2001, 56, 109–114. [Google Scholar] [CrossRef] [PubMed]
- Gueli, N.; Martinez, A.; Verrusio, W.; Linguanti, A.; Passador, P.; Martinelli, V.; Longo, G.; Marigliano, B.; Cacciafesta, F.; Cacciafesta, M. Empirical antibiotic therapy (ABT) of lower respiratory tract infections (LRTI) in the elderly: Application of artificial neural network (ANN). Preliminary results. Arch. Gerontol. Geriatr. 2012, 55, 499–503. [Google Scholar] [CrossRef] [PubMed]
- Torres, A.; Peetermans, W.E.; Viegi, G.; Blasi, F. Risk factors for community-acquired pneumonia in adults in Europe: A literature review. Thorax 2013, 68, 1057–1065. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Welte, T.; Torres, A.; Nathwani, D. Clinical and economic burden of community-acquired pneumonia among adults in Europe. Thorax 2012, 67, 71–79. [Google Scholar] [CrossRef] [PubMed]
- Lim, W.S.; Macfarlane, J.T.; Boswell, T.C.; Harrison, T.G.; Rose, D.; Leinonen, M.; Saikku, P. Study of community acquired pneumonia aetiology (SCAPA) in adults admitted to hospital: Implications for management guidelines. Thorax 2001, 56, 296–301. [Google Scholar] [CrossRef] [PubMed]
- Woodhead, M. Community-acquired pneumonia in Europe: Causative pathogens and resistance patterns. Eur. Respir. J. Suppl. 2002, 36, 20s–27s. [Google Scholar] [CrossRef] [PubMed]
- Whitney, C.G.; Farley, M.M.; Hadler, J.; Harrison, L.H.; Bennett, N.M.; Lynfield, R.; Reingold, A.; Cieslak, P.R.; Pilishvili, T.; Jackson, D.; et al. Active bacterial core surveillance of the emerging infections program network. Decline in invasive pneumococcal disease after the introduction of protein-polysaccharide conjugate vaccine. N. Engl. J. Med. 2003, 348, 1737–1746. [Google Scholar] [CrossRef] [PubMed]
- Hicks, L.A.; Harrison, L.H.; Flannery, B.; Hadler, J.L.; Schaffner, W.; Craig, A.S.; Jackson, D.; Thomas, A.; Beall, B.; Lynfield, R.; et al. Incidence of pneumococcal disease due to non-pneumococcal conjugate vaccine (PCV7) serotypes in the United States during the era of widespread PCV7 vaccination, 1998–2004. J. Infect. Dis. 2007, 196, 1346–1354. [Google Scholar] [CrossRef] [PubMed]
- Rose, M.; Zielen, S. Impact of infant immunization programs with pneumococcal conjugate vaccine in Europe. Expert. Rev. Vaccines 2009, 8, 1351–1364. [Google Scholar] [CrossRef] [PubMed]
- Pírez, M.C.; Algorta, G.; Cedrés, A.; Sobrero, H.; Varela, A.; Giachetto, G.; Montano, A. Impact of universal pneumococcal vaccination on hospitalizations for pneumonia and meningitis in children in Montevideo, Uruguay. Pediatr. Infect. Dis. J. 2011, 30, 669–674. [Google Scholar] [CrossRef] [PubMed]
- Simonsen, L.; Taylor, R.J.; Young-Xu, Y.; Haber, M.; May, L.; Klugman, K.P. Impact of pneumococcal conjugate vaccination of infants on pneumonia and influenza hospitalization and mortality in all age groups in the United States. MBio 2011, 2, e00309–e00310. [Google Scholar] [CrossRef] [PubMed]
- Grijalva, C.G.; Nuorti, J.P.; Arbogast, P.G.; Martin, S.W.; Edwards, K.M.; Griffin, M.R. Decline in pneumonia admissions after routine childhood immunisation with pneumococcal conjugate vaccine in the USA: A time-series analysis. Lancet 2007, 369, 1179–1186. [Google Scholar] [CrossRef]
- Pichichero, M.E. Protein carriers of conjugate vaccines: Characteristics, development, and clinical trials. Hum. Vaccin. Immunother. 2013, 9, 2505–2523. [Google Scholar] [CrossRef] [PubMed]
- Goldblatt, D.; Southern, J.; Ashton, L.; Richmond, P.; Burbidge, P.; Tasevska, J.; Crowley-Luke, A.; Andrews, N.; Morris, R.; Borrow, R.; et al. Immunogenicity and boosting after a reduced number of doses of a pneumococcal conjugate vaccine in infants and toddlers. Pediatr. Infect. Dis. J. 2006, 25, 312–319. [Google Scholar] [CrossRef] [PubMed]
- Anderson, E.L.; Kennedy, D.J.; Geldmacher, K.M.; Donnelly, J.; Mendelman, P.M. Immunogenicity of heptavalent pneumococcal conjugate vaccine in infants. J. Pediatr. 1996, 128, 649–653. [Google Scholar] [CrossRef]
- Dagan, R.; Melamed, R.; Zamir, O.; Leroy, O. Safety and immunogenicity of tetravalent pneumococcal vaccines containing 6B, 14, 19F and 23F polysaccharides conjugated to either tetanus toxoid or diphtheria toxoid in young infants and their boosterability by native polysaccharide antigens. Pediatr. Infect. Dis. J. 1997, 16, 1053–1059. [Google Scholar] [CrossRef] [PubMed]
- Ahman, H.; Käyhty, H.; Lehtonen, H.; Leroy, O.; Froeschle, J.; Eskola, J. Streptococcus pneumonia capsular polysaccharide-diphtheria toxoid conjugate vaccine is immunogenic in early infancy and able to induce immunologic memory. Pediatr. Infect. Dis. J. 1998, 17, 211–216. [Google Scholar] [CrossRef] [PubMed]
- Rennels, M.B.; Edwards, K.M.; Keyserling, H.L.; Reisinger, K.S.; Hogerman, D.A.; Madore, D.V.; Chang, I.; Paradiso, P.R.; Malinoski, F.J.; Kimura, A. Safety and immunogenicity of heptavalent pneumococcal vaccine conjugated to CRM197 in United States infants. Pediatrics 1998, 101, 604–611. [Google Scholar] [CrossRef] [PubMed]
- Knuf, M.; Pankow-Culot, H.; Grunert, D.; Rapp, M.; Panzer, F.; Köllges, R.; Fanic, A.; Habib, A.; Borys, D.; Dieussaert, I.; et al. Induction of immunologic memory following primary vaccination with the 10-valent pneumococcal nontypeable Haemophilus influenzae protein D conjugate vaccine in infants. Pediatr. Infect. Dis. J. 2012, 31, e31–e36. [Google Scholar] [CrossRef] [PubMed]
- Dagan, R.; Givon-Lavi, N.; Fraser, D.; Lipsitch, M.; Siber, G.R.; Kohberger, R. Serum serotype-specific pneumococcal anticapsular immunoglobulin g concentrations after immunization with a 9-valent conjugate pneumococcal vaccine correlate with nasopharyngeal acquisition of pneumococcus. J. Infect. Dis. 2005, 192, 367–376. [Google Scholar] [CrossRef] [PubMed]
- Rodenburg, G.D.; de Greeff, S.C.; Jansen, A.G.; de Melker, H.E.; Schouls, L.M.; Hak, E.; Spanjaard, L.; Sanders, E.A.; van der Ende, A. Effects of pneumococcal conjugate vaccine 2 years after its introduction, The Netherlands. Emerg. Infect. Dis. 2010, 16, 816–823. [Google Scholar] [CrossRef] [PubMed]
- Black, S.; Shinefield, H.; Baxter, R.; Austrian, R.; Bracken, L.; Hansen, J.; Lewis, E.; Fireman, B. Postlicensure surveillance for pneumococcal invasive disease after use of heptavalent pneumococcal conjugate vaccine in Northern California Kaiser Permanente. Pediatr. Infect. Dis. J. 2004, 23, 485–489. [Google Scholar] [CrossRef] [PubMed]
- Nelson, J.C.; Jackson, M.; Yu, O.; Whitney, C.G.; Bounds, L.; Bittner, R.; Zavitkovsky, A.; Jackson, L.A. Impact of the introduction of pneumococcal conjugate vaccine on rates of community acquired pneumonia in children and adults. Vaccine 2008, 26, 4947–4954. [Google Scholar] [CrossRef] [PubMed]
- Castiglia, P. Recommendations for pneumococcal immunization outside routine childhood immunization programs in Western Europe. Adv. Ther. 2014, 31, 1011–1044. [Google Scholar] [CrossRef] [PubMed]
- Tomczyk, S.; Bennett, N.M.; Stoecker, C.; Gierke, R.; Moore, M.R.; Whitney, C.G.; Hadler, S.; Pilishvili, T.; Centers for Disease Control and Prevention (CDC). Use of 13-valent pneumococcal conjugate vaccine and 23-valent pneumococcal polysaccharide vaccine among adults aged ≥65 years: Recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Morb. Mortal. Wkly. Rep. 2014, 63, 822–825. [Google Scholar] [PubMed]
- O’Halloran, A.C.; Lu, P.J.; Pilishvili, T. Pneumococcal vaccination coverage among persons ≥65 years—United States, 2013. Vaccine 2015, 33, 5503–5506. [Google Scholar] [CrossRef] [PubMed]
- Williams, W.W.; Lu, P.J.; O’Halloran, A.; Bridges, C.B.; Kim, D.K.; Pilishvili, T.; Hales, C.M.; Markowitz, L.E. Centers for Disease Control and Prevention (CDC). Vaccination coverage among adults, excluding influenza vaccination—United States, 2013. MMWR Morb. Mortal. Wkly. Rep. 2015, 64, 95–102. [Google Scholar] [PubMed]
- Alicino, C.; Barberis, I.; Orsi, A.; Durando, P. Pneumococcal vaccination strategies in adult population: Perspectives with the pneumococcal 13—Valent polysaccharide conjugate vaccine. Minerva. Med. 2014, 105, 89–97. [Google Scholar] [PubMed]
- Ministero Della Salute. Piano Nazionale Vaccini 2005–2007. 2005. Available online: http://www.salute.gov.it/portale/documentazione/p6_2_2_1.jsp?lingua=italiano&id=543 (accessed on 29 January 2016). [Google Scholar]
- Ansaldi, F.; de Florentis, D.; Canepa, P.; Bandettini, R.; Diana, M.C.; Martini, M.; Durando, P.; Icardi, G. Epidemiological changes after PCV7 implementation in Italy: Perspective for new Vaccines. Hum. Vaccines 2011, 7, 211–216. [Google Scholar] [CrossRef] [PubMed]
- Ansaldi, F.; Turello, V.; Lai, P.; Bastone, G.; de Luca, S.; Rosselli, R.; Durando, P.; Sticchi, L.; Gasparini, R.; Delfino, E.; et al. Effectiveness of a 23-valent polysaccharide vaccine in preventing pneumonia and non-invasive pneumococcal infection in elderly people: A large-scale retrospective cohort study. J. Int. Med. Res. 2005, 33, 490–500. [Google Scholar] [CrossRef] [PubMed]
- Orsi, A.; Ansaldi, F.; Durando, P.; Turello, V.; Icardi, G. Gruppo di studio ligure sullo pneumococco. Immunization campaign with 13-valent Pneumococcal Conjugate Vaccine in adults in Liguria Region, Italy: One year post-introduction preliminary results. Epidemiol. Prev. 2014, 38, 66–72. [Google Scholar] [PubMed]
- Pollard, A.J.; Perrett, K.P.; Beverley, P.C. Maintaining protection against invasive bacteria with protein-polysaccharide conjugate Vaccines Nat. Rev. Immunol. 2009, 9, 213–220. [Google Scholar] [CrossRef] [PubMed]
- Avci, F.Y.; Li, X.; Tsuji, M.; Kasper, D.L. A mechanism for glycoconjugate vaccine activation of the adaptive immune system and its implications for vaccine design. Nat. Med. 2011, 17, 1602–1609. [Google Scholar] [CrossRef] [PubMed]
- Bogaert, D.; de Groot, R.; Hermans, P.W. Streptococcus pneumoniae colonisation: The key to pneumococcal disease. Lancet Infect Dis. 2004, 4, 144–154. [Google Scholar] [CrossRef]
- Simell, B.; Auranen, K.; Käyhty, H.; Goldblatt, D.; Dagan, R.; O’Brien, K.L. Pneumococcal Carriage Group. The fundamental link between pneumococcal carriage and disease. Expert. Rev. Vaccines 2012, 11, 841–855. [Google Scholar] [CrossRef] [PubMed]
- Davis, S.M.; Deloria-Knoll, M.; Kassa, H.T.; O’Brien, K.L. Impact of pneumococcal conjugate vaccines on nasopharyngeal carriage and invasive disease among unvaccinated people: Review of evidence on indirect effects. Vaccine 2013, 32, 133–145. [Google Scholar] [CrossRef] [PubMed]
- Ridda, I.; Macintyre, C.R.; Lindley, R.; McIntyre, P.B.; Brown, M.; Oftadeh, S. Lack of pneumococcal carriage in the hospitalised elderly. Vaccine 2010, 28, 3902–3904. [Google Scholar] [CrossRef] [PubMed]
- Flasche, S.; van Hoek, A.J.; Sheasby, E.; Waight, P.; Andrews, N.; Sheppard, C. Effect of pneumococcal conjugate vaccination on serotype-specific carriage and invasive disease in England: A cross-sectional study. PLoS Med. 2011, 8, e1001017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palmu, A.A.; Kaijalainen, T.; Saukkoriipi, A.; Leinonen, M.; Kilpi, T.M. Nasopharyngeal carriage of Streptococcus pneumoniae and pneumococcal urine antigen testing healthy elderly subjects. Scand. J. Infect. Dis. 2012, 44, 433–438. [Google Scholar] [CrossRef] [PubMed]
- Da Gloria, C.M.; Pimenta, F.C.; Jackson, D.; Roundtree, A.; Ahmad, Y.; Millar, E.V. Revisiting pneumococcal carriage by use of broth enrichment and PCR techniques for enhanced detection of carriage and serotypes. J. Clin. Microbiol. 2010, 48, 1611–1618. [Google Scholar]
- Pai, R.; Gertz, R.E.; Beall, B. Sequential multiplex PCR approach for determining capsular serotypes of Streptococcus pneumoniae isolates. J. Clin. Microbiol. 2006, 44, 124–131. [Google Scholar] [CrossRef] [PubMed]
- Krone, C.L.; Wyllie, A.L.; van Beek, J.; Rots, N.Y.; Oja, A.E.; Chu, M.L. Carriage of Streptococcus pneumoniae in aged adults with influenza-like-illness. PLoS ONE 2015, 10, e0119875. [Google Scholar] [CrossRef] [PubMed]
- Ansaldi, F.; de Florentiis, D.; Canepa, P.; Ceravolo, A.; Rappazzo, E.; Iudici, R.; Martini, M.; Botti, G.; Orsi, A.; Icardi, G.; et al. Carriage of Streptoccoccus pneumoniae in healthy adults aged 60 years or over in a population with very high and long-lasting pneumococcal conjugate vaccine coverage in children: Rationale and perspectives for PCV13 implementation. Hum. Vaccines Immunother. 2013, 9, 614–620. [Google Scholar] [CrossRef]
- Esposito, S.; Mari, D.; Bergamaschini, L.; Orenti, A.; Terranova, L.; Ruggiero, L.; Ierardi, V.; Gambino, M.; Croce, F.D.; Principi, N. Pneumococcal colonization in older adults. Immun. Ageing 2016, 13, 2. [Google Scholar] [CrossRef] [PubMed]
- Gutiérrez, F.; Masiá, M.; Mirete, C.; Soldán, B.; Rodríguez, J.C.; Padilla, S.; Hernández, I.; Royo, G.; Martin-Hidalgo, A. The influence of age and gender on the population-based incidence of community-acquired pneumonia caused by different microbial pathogens. J. Infect. 2006, 53, 166–174. [Google Scholar] [CrossRef] [PubMed]
- Ochoa-Gondar, O.; Vila-Córcoles, A.; de Diego, C.; Arija, V.; Maxenchs, M.; Grive, M.; Martin, E.; Pinyol, J.L. EVAN-65 Study Group. The burden of community-acquired pneumonia in the elderly: The Spanish EVAN-65 study. BMC Public Health 2008, 8, 222. [Google Scholar] [CrossRef] [PubMed]
- Vila-Corcoles, A.; Ochoa-Gondar, O.; Rodriguez-Blanco, T.; Raga-Luria, X.; Gomez-Bertomeu, F. EPIVAC Study Group. Epidemiology of community-acquired pneumonia in older adults: A population-based study. Respir. Med. 2009, 103, 309–316. [Google Scholar] [CrossRef] [PubMed]
- Said, M.A.; Johnson, H.L.; Nonyane, B.A. Estimating the burden of pneumococcal pneumonia among adults: A systematic review and meta-analysis of diagnostic techniques. PLoS ONE 2013, 8, e60273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gross, A.E.; van Schooneveld, T.C.; Olsen, K.M. Epidemiology and predictors of multidrug-resistant community-acquired and health care-associated pneumonia. Antimicrob. Agents Chemother. 2014, 58, 5262–5268. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Pneumococcal Vaccines WHO position paper 2012. Wkly. Epidemiol. Rec. 2012, 87, 129–144. [Google Scholar]
- Ewig, S.; Birkner, N.; Strauss, R.; Schaefer, E.; Pauletzki, J.; Bischoff, H.; Schraeder, P.; Welte, T.; Hoeffken, G. New perspectives on community-acquired pneumonia in 388 406 patients. Results from a nationwide mandatory performance measurement programme in healthcare quality. Thorax 2009, 64, 1062–1069. [Google Scholar] [CrossRef] [PubMed]
- Bewick, T.; Sheppard, C.; Greenwood, S.; Slack, M.; Trotter, C.; George, R.; Lim, W.S. Serotype prevalence in adults hospitalised with pneumococcal non invasive community-acquired pneumonia. Thorax 2012, 67, 540–545. [Google Scholar] [CrossRef] [PubMed]
- Marston, B.J.; Plouffe, J.F.; File, T.M., Jr.; Hackman, B.A.; Salstrom, S.J.; Lipman, H.B.; Kolczak, M.S.; Breiman, R.F. The Community-Based Pneumonia Incidence Study Group. Incidence of community-acquired pneumonia requiring hospitalization. Results of a population based active surveillance Study in Ohio. Arch. Intern. Med. 1997, 157, 1709–1718. [Google Scholar] [CrossRef] [PubMed]
- Kornum, J.B.; Due, K.M.; Nørgaard, M.; Tjønneland, A.; Overvad, K.; Sørensen, H.T.; Thomsen, R.W. Alcohol drinking and risk of subsequent hospitalisation with pneumonia. Eur. Respir. J. 2012, 39, 149–155. [Google Scholar] [CrossRef] [PubMed]
- Trucchi, C.; Paganino, C.; Ansaldi, F. Methodological criticisms in the evaluation of Pneumococcal Conjugate Vaccine effectiveness. J. Prev. Med. Hyg. 2015, 56, E144–E149. [Google Scholar] [PubMed]
- Viegi, G.; Pistelli, R.; Cazzola, M.; Falcone, F.; Cerveri, I.; Rossi, A.; Ugo Di Maria, G. Epidemiological survey on incidence and treatment of community acquired pneumonia in Italy. Respir. Med. 2006, 100, 46–55. [Google Scholar] [CrossRef] [PubMed]
- Giorgi Rossi, P.; Agabiti, N.; Faustini, A.; Ancona, C.; Tancioni, V.; Forastiere, F.; Perucci, C.A. The burden of hospitalised pneumonia in Lazio, Italy, 1997–1999. Int. J. Tuberc. Lung Dis. 2004, 8, 528–536. [Google Scholar] [PubMed]
- Amodio, E.; Costantino, C.; Boccalini, S.; Tramuto, F.; Maida, C.M.; Vitale, F. Estimating the burden of hospitalization for pneumococcal pneumonia in a general population aged 50 years or older and implications for vaccination strategies. Hum. Vaccines Immunother. 2014, 10, 1337–1342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bechini, A.; Taddei, C.; Barchielli, A.; Levi, M.; Tiscione, E.; Santini, M.G.; Niccolini, F.; Mechi, M.T.; Panatto, D.; Amicizia, D.; et al. A retrospective analysis of hospital discharge records for S. pneumoniae diseases in the elderly population of Florence, Italy, 2010–2012. Hum. Vaccines Immunother. 2015, 11, 156–165. [Google Scholar] [CrossRef] [PubMed]
- Ansaldi, F.; Orsi, A.; Trucchi, C.; de Florentiis, D.; Ceravolo, A.; Coppelli, M.; Schiaffino, S.; Turello, V.; Rosselli, R.; Carloni, R.; et al. Potential effect of PCV13 introduction on Emergency Department accesses for lower respiratory tract infections in elderly and at risk adults. Hum. Vaccines Immunother. 2015, 11, 166–171. [Google Scholar] [CrossRef] [PubMed]
- Bonten, M.J.; Huijts, S.M.; Bolkenbaas, M.; Webber, C.; Patterson, S.; Gault, S.; van Werkhoven, C.H.; van Deursen, A.M.; Sanders, E.A.; Verheij, T.J.; et al. Polysaccharide conjugate vaccine against pneumococcal pneumonia in adults. N. Engl. J. Med. 2015, 372, 1114–1125. [Google Scholar] [CrossRef] [PubMed]
- Van Werkhoven, C.H.; Bonten, M.J. The Community-Acquired Pneumonia immunization Trial in Adults (CAPiTA): What is the future of pneumococcal conjugate vaccination in elderly? Future Microbiol. 2015, 10, 1405–1413. [Google Scholar] [CrossRef] [PubMed]
- Pilishvili, T.; Gierke, R.; Kim, L.; Stoecker, C. Potential public health impact of 13-valent pneumococcal conjugate vaccine use among adults 65 years of age or older. In Open Forum Infectious Diseases; Oxford University Press: Oxford, UK, 2014; Volume 1, p. S24. [Google Scholar]

© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Orsi, A.; Ansaldi, F.; Trucchi, C.; Rosselli, R.; Icardi, G. Pneumococcus and the Elderly in Italy: A Summary of Available Evidence Regarding Carriage, Clinical Burden of Lower Respiratory Tract Infections and On-Field Effectiveness of PCV13 Vaccination. Int. J. Mol. Sci. 2016, 17, 1140. https://doi.org/10.3390/ijms17071140
Orsi A, Ansaldi F, Trucchi C, Rosselli R, Icardi G. Pneumococcus and the Elderly in Italy: A Summary of Available Evidence Regarding Carriage, Clinical Burden of Lower Respiratory Tract Infections and On-Field Effectiveness of PCV13 Vaccination. International Journal of Molecular Sciences. 2016; 17(7):1140. https://doi.org/10.3390/ijms17071140
Chicago/Turabian StyleOrsi, Andrea, Filippo Ansaldi, Cecilia Trucchi, Roberto Rosselli, and Giancarlo Icardi. 2016. "Pneumococcus and the Elderly in Italy: A Summary of Available Evidence Regarding Carriage, Clinical Burden of Lower Respiratory Tract Infections and On-Field Effectiveness of PCV13 Vaccination" International Journal of Molecular Sciences 17, no. 7: 1140. https://doi.org/10.3390/ijms17071140