Nanoparticle-Mediated Pulmonary Drug Delivery: A Review

Abstract
:
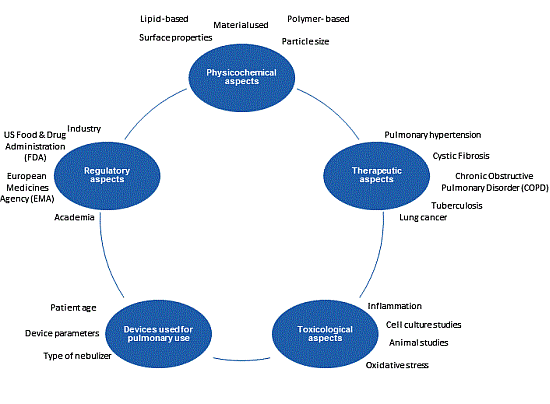
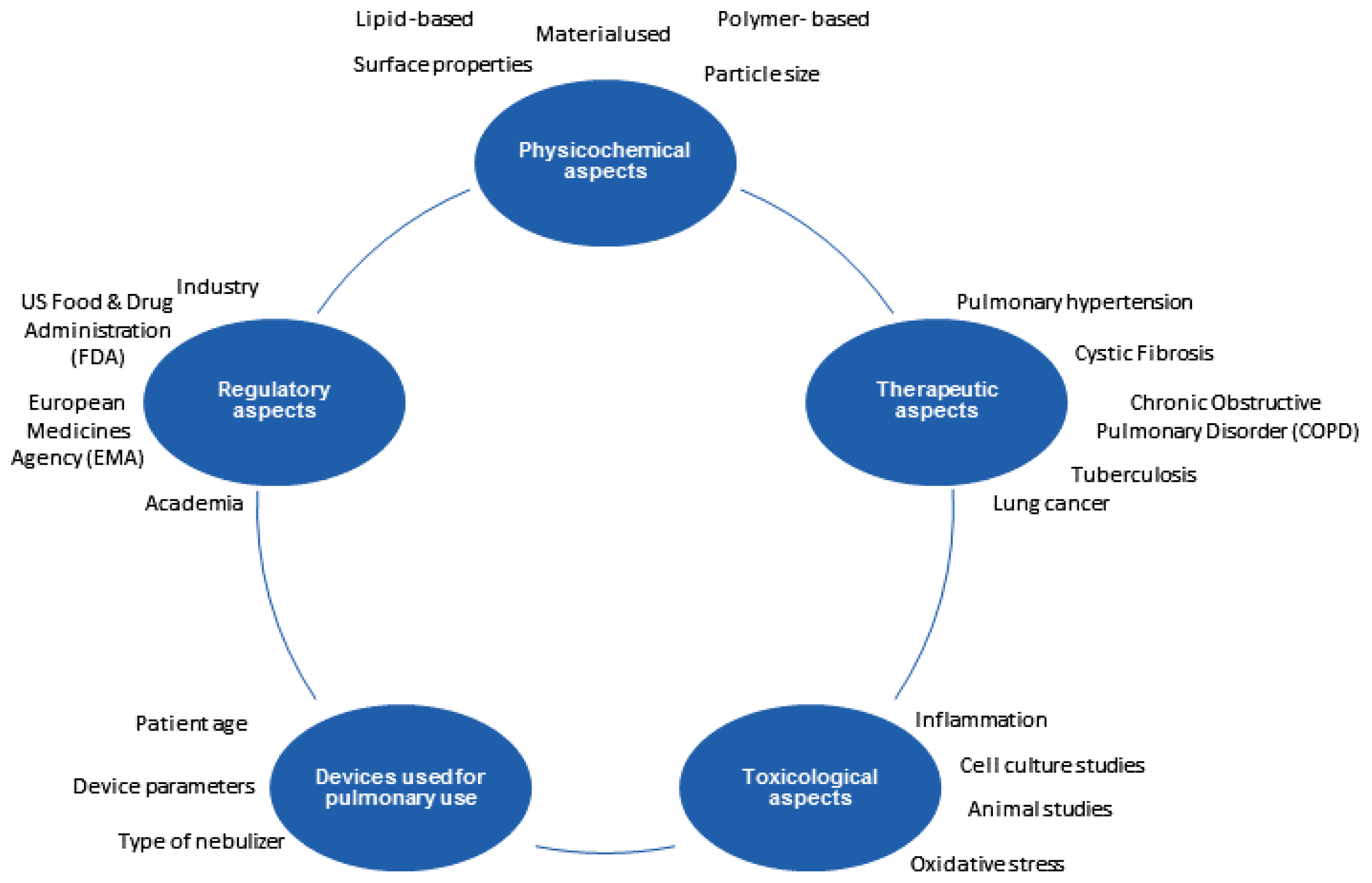
1. Introduction
2. Anatomy and Physiology of the Lungs
2.1. Anatomy of the Lungs
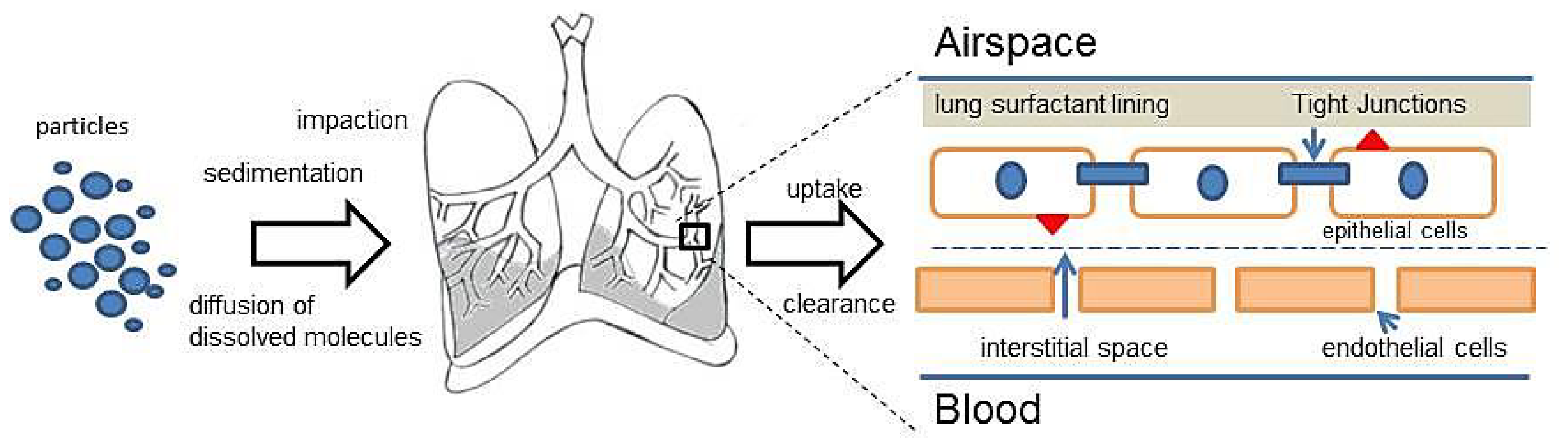
2.2. Deposition of the Particles
2.3. Clearance of the Particles
3. Nanoparticle-Based Systems for Pulmonary Application
3.1. Solid Lipid Nanoparticles (SLN) and Solid Lipid Microparticles (SLM)
3.2. Polymeric Nanoparticles
3.3. Liposomes
4. Physicochemical Characterization for Nanoparticle-Based Systems
4.1. Particle Size and Zeta Potential Measurements
4.2. Differential Scanning Calorimetry (DSC)
4.3. X-ray Diffraction
4.4. Microscopical Techniques/Particle Morphology
5. Cell- and Animal-Based Studies
5.1. In Vitro Lung Epithelial Cell Culture Models
5.2. Ex Vivo Lung Tissue Models
5.3. In Vivo Models
6. Toxicity Assays
7. Conclusions
Acknowledgments
Conflicts of Interest
References
- Azarmi, S.; Roa, W.H.; Löbenberg, R. Targeted delivery of nanoparticles for the treatment of lung diseases. Adv. Drug Deliv. Rev 2008, 60, 863–875. [Google Scholar]
- Sung, J.C.; Pulliam, B.L.; Edwards, D.A. Nanoparticles for drug delivery to the lungs. Trends Biotechnol 2007, 25, 563–570. [Google Scholar]
- Jaafar-Maalej, C.; Elaissari, A.; Fessi, H. Lipid-based carriers: Manufacturing and applications for pulmonary route. Expert Opin. Drug Deliv 2012, 9, 1111–1127. [Google Scholar]
- Beck-Broichsitter, M.; Gauss, J.; Packhaeuser, C.B.; Lahnstein, K.; Schmehl, T.; Seeger, W.; Kissel, T.; Gessler, T. Pulmonary drug delivery with aerosolizable nanoparticles in an ex vivo lung model. Int. J. Pharm 2009, 367, 169–178. [Google Scholar]
- Beck-Broichsitter, M.; Kleimann, P.; Gessler, T.; Seeger, W.; Kissel, T.; Schmehl, T. Nebulization performance of biodegradable sildenafil-loaded nanoparticles using the Aeroneb® Pro: Formulation aspects and nanoparticle stability to nebulization. Int. J. Pharm 2012, 422, 398–408. [Google Scholar]
- Mueller, R. Solid lipid nanoparticles (SLN) for controlled drug delivery—A review of the state of the art. Eur. J. Pharm. Biopharm 2000, 50, 161–177. [Google Scholar]
- Mueller, R. Lipid nanoparticles: Recent advances. Adv. Drug Deliv. Rev 2007, 59, 375–376. [Google Scholar]
- Nassimi, M.; Schleh, C.; Lauenstein, H.; Hussein, R.; Hoymann, H.; Koch, W.; Pohlmann, G.; Krug, N.; Sewald, K.; Rittinghausen, S.; et al. A toxicological evaluation of inhaled solid lipid nanoparticles used as a potential drug delivery system for the lung. Eur. J. Pharm. Biopharm 2010, 75, 107–116. [Google Scholar]
- Nassimi, M.; Schleh, C.; Lauenstein, H.-D.; Hussein, R.; Lübbers, K.; Pohlmann, G.; Switalla, S.; Sewald, K.; Müller, M.; Krug, N.; et al. Low cytotoxicity of solid lipid nanoparticles in in vitro and ex vivo lung models. Inhal. Toxicol 2009, 21, 104–109. [Google Scholar]
- Paranjpe, M.; Neuhaus, V.; Finke, J.H.; Richter, C.; Gothsch, T.; Kwade, A.; Büttgenbach, S.; Braun, A.; Müller-Goymann, C.C. In vitro and ex vivo toxicological testing of sildenafil-loaded solid lipid nanoparticles. Inhal. Toxicol 2013, 25, 536–543. [Google Scholar]
- Menon, J.U.; Ravikumar, P.; Pise, A.; Gyawali, D.; Hsia, C.C.W.; Nguyen, K.T. Polymeric nanoparticles for pulmonary protein and DNA delivery. Acta Biomater 2014, in press. [Google Scholar] [CrossRef]
- Menon, J.U.; Wadajkar, A.S.; Xie, Z.; Nguyen, K.T. Nanomaterials for management of lung disorders and drug delivery. In Nanomaterials in Drug Delivery, Imaging, and Tissue Engineering; Tiwari, A., Tiwari, A., Eds.; John Wiley & Sons, Inc: Hoboken, NJ, USA, 2013; pp. 167–202. [Google Scholar]
- Patel, P.; Soni, T.; Thakkar, V.; Gandhi, T. Nanoparticle as an emerging tool in pulmonary drug delivery system. MNS 2013, 5, 288–302. [Google Scholar]
- Rang, H.P.; Dale, M.M.; Ritter, J.M.; Flower, R.J. Pharmacology, Sixth ed.; Churchill Livingstone: New York, NY, USA, 2007; Section 3; Volume Chapter 22. [Google Scholar]
- Kelly, L. Essentials of Human Physiology for Pharmacy; CRC Press: Boca Raton, FL, USA, 2004. [Google Scholar]
- Tena, A.F.; Clarà, P.C. Deposition of inhaled particles in the lungs. Arch Bronconeumol 2012, 48, 240–246. [Google Scholar]
- Yang, W.; Peters, J.I.; Williams, R.O. Inhaled nanoparticles—A current review. Int. J. Pharm 2008, 356, 239–247. [Google Scholar]
- Patton, J.S. Mechanisms of macromolecule absorption by the lungs. Adv. Drug Deliv. Rev 1996, 19, 3–36. [Google Scholar]
- Patton, J.S.; Brain, J.D.; Davies, L.A.; Fiegel, J.; Gumbleton, M.; Kim, K.-J.; Sakagami, M.; Vanbever, R.; Ehrhardt, C. The particle has landed—Characterizing the fate of inhaled pharmaceuticals. J. Aerosol Med. Pulm. Drug Deliv 2010, 23, S71–S87. [Google Scholar]
- Beck-Broichsitter, M.; Ruppert, C.; Schmehl, T.; Guenther, A.; Betz, T.; Bakowsky, U.; Seeger, W.; Kissel, T.; Gessler, T. Biophysical investigation of pulmonary surfactant surface properties upon contact with polymeric nanoparticles in vitro. Nanomed. Nanotechnol. Biol. Med. 2011, 7, 341–350. [Google Scholar]
- Silva, L.F.C.; Kasten, G.; de Campos, C.E.M.; Chinelatto, A.L.; Lemos-Senna, E. Preparation and characterization of quercetin-loaded solid lipid microparticles for pulmonary delivery. Powder Technol 2013, 239, 183–192. [Google Scholar]
- Wang, W.; Zhu, R.; Xie, Q.; Li, A.; Xiao, Y.; Liu, H.; Wang, S.; Cui, D. Enhanced bioavailability and efficiency of curcumin for the treatment of asthma by its formulation in solid lipid nanoparticles. IJN 2012, 7, 3667–3677. [Google Scholar]
- Varshosaz, J.; Ghaffari, S.; Mirshojaei, S.F.; Jafarian, A.; Atyabi, F.; Kobarfard, F.; Azarmi, S. Biodistribution of amikacin solid lipid nanoparticles after pulmonary delivery. BioMed. Res. Int 2013, 2013, 1–8. [Google Scholar]
- Mussi, S.V.; Silva, R.C.; Oliveira, M.C.; Lucci, C.M.; Azevedo, R.B.; Ferreira, L.A.M. New approach to improve encapsulation and antitumor activity of doxorubicin loaded in solid lipid nanoparticles. Eur. J. Pharm. Sci 2013, 48, 282–290. [Google Scholar]
- Chiraz, J.-M.; Andrieu, V.; Elaissari, A.; Fessi, H. Beclomethasone-loaded lipidic nanocarriers for pulmonary drug delivery: Preparation, characterization and in vitro drug release. J. Nanosci. Nanotechnol 2011, 11, 1841–1851. [Google Scholar]
- Elhissi, A.; Islam, M.A.; Arafat, B.; Taylor, M.; Ahmed, W. Development and characterisation of freeze-dried liposomes containing two anti-asthma drugs. Micro Nano Lett 2010, 5, 184. [Google Scholar]
- Zhang, P.-R.; Xie, Y.; Li, M. Preparation and characterization of budesonide-loaded solid lipid nanoparticles for pulmonary delivery. J. Chin. Pharm. Sci 2011, 20, 390–396. [Google Scholar]
- Kumar, S.S.D.; Surianarayanan, M.; Vijayaraghavan, R.; Mandal, A.B.; MacFarlane, D.R. Curcumin loaded poly(2-hydroxyethyl methacrylate) nanoparticles from gelled ionic liquid—In vitro cytotoxicity and anti-cancer activity in SKOV-3 cells. Eur. J. Pharm. Sci 2014, 51, 34–44. [Google Scholar]
- Castelli, F.; Puglia, C.; Sarpietro, M.G.; Rizza, L.; Bonina, F. Characterization of indomethacin-loaded lipid nanoparticles by differential scanning calorimetry. Int. J. Pharm 2005, 304, 231–238. [Google Scholar]
- Ali, R.; Mittal, G.; Ali, R.; Kumar, M.; Kishan Khar, R.; Ahmad, F.J.; Bhatnagar, A. Development, characterisation and pharmacoscintigraphic evaluation of nano-fluticasone propionate dry powder inhalation as potential antidote against inhaled toxic gases. J. Microencapsul 2013, 30, 546–558. [Google Scholar]
- Trivedi, R.; Redente, E.F.; Thakur, A.; Riches, D.W.H.; Kompella, U.B. Local delivery of biodegradable pirfenidone nanoparticles ameliorates bleomycin-induced pulmonary fibrosis in mice. Nanotechnology 2012, 23, 505101. [Google Scholar]
- Rao, A.K.; Shrikhande, S.; Bajaj, A. Development of cisplatin nanoparticles as dry powder inhalers for lung cancer. Curr. Nanosci 2013, 9, 447–450. [Google Scholar]
- Roa, W.H.; Azarmi, S.; Al-Hallak, M.K.; Finlay, W.H.; Magliocco, A.M.; Löbenberg, R. Inhalable nanoparticles, a non-invasive approach to treat lung cancer in a mouse model. J. Control. Release 2011, 150, 49–55. [Google Scholar]
- Li, M. Methotrexate-conjugated and hyperbranched polyglycerol-grafted Fe3O4 magnetic nanoparticles for targeted anticancer effects. Eur. J. Pharm. Sci 2013, 48, 111–120. [Google Scholar]
- Gill, K.K.; Nazzal, S.; Kaddoumi, A. Paclitaxel loaded PEG5000–DSPE micelles as pulmonary delivery platform: Formulation characterization, tissue distribution, plasma pharmacokinetics, and toxicological evaluation. Eur. J. Pharm. Biopharm 2011, 79, 276–284. [Google Scholar]
- Chen, H.; Zhao, T.; Dong, Y.; Zhang, J.; Huang, H.; Zhu, J. Paclitaxel-loaded poly(glycolide-co-ɛ-caprolactone)-b-d-α-tocopheryl polyethylene glycol 2000 succinate nanoparticles for lung cancer therapy. IJN 2013, 8, 1947–1957. [Google Scholar]
- Yang, R.; Yang, S.-G.; Shim, W.-S.; Cui, F.; Cheng, G.; Kim, I.-W.; Kim, D.-D.; Chung, S.-J.; Shim, C.-K. Lung-specific delivery of paclitaxel by chitosan-modified PLGA nanoparticles via transient formation of microaggregates. J. Pharm. Sci 2009, 98, 970–984. [Google Scholar]
- Xu, P.; Yin, Q.; Shen, J.; Chen, L.; Yu, H.; Zhang, Z.; Li, Y. Synergistic inhibition of breast cancer metastasis by silibinin-loaded lipid nanoparticles containing TPGS. Int. J. Pharm 2013, 454, 21–30. [Google Scholar]
- Yoo, D.; Guk, K.; Kim, H.; Khang, G.; Wu, D.; Lee, D. Antioxidant polymeric nanoparticles as novel therapeutics for airway inflammatory diseases. Int. J. Pharm 2013, 450, 87–94. [Google Scholar]
- Hoesel, L.M.; Flierl, M.A.; Niederbichler, A.D.; Rittirsch, D.; McClintock, S.D.; Reuben, J.S.; Pianko, M.J.; Stone, W.; Yang, H.; Smith, M.; et al. Ability of antioxidant liposomes to prevent acute and progressive pulmonary injury. Antioxid. Redox Signal 2008, 10, 963–972. [Google Scholar]
- Arikace Website Source. Available online: http://www.insmed.com/product-candidates/about-arikace (accessed on 9 January 2014).
- Cipolla, D.; Gonda, I.; Chan, H.-K. Liposomal formulations for inhalation. Ther. Deliv 2013, 4, 1047–1072. [Google Scholar]
- Adler-Moore, J.; Proffitt, R.T. AmBisome: Liposomal formulation, structure, mechanism of action and pre-clinical experience. J. Antimicrob. Chemother 2002, 49, 21–30. [Google Scholar]
- Pandey, R. Antitubercular inhaled therapy: Opportunities, progress and challenges. J. Antimicrob. Chemother 2005, 55, 430–435. [Google Scholar]
- Zhang, L.; Pornpattananangkul, D.; Hu, C.-M.; Huang, C.-M. Development of nanoparticles for antimicrobial drug delivery. CMC 2010, 17, 585–594. [Google Scholar]
- Behr, J.; Zimmermann, G.; Baumgartner, R.; Leuchte, H.; Neurohr, C.; Brand, P.; Herpich, C.; Sommerer, K.; Seitz, J.; Menges, G.; et al. Lung deposition of a liposomal cyclosporine a inhalation solution in patients after lung transplantation. J. Aerosol Med. Pulm. Drug Deliv 2009, 22, 121–130. [Google Scholar]
- Muttil, P.; Kaur, J.; Kumar, K.; Yadav, A.B.; Sharma, R.; Misra, A. Inhalable microparticles containing large payload of anti-tuberculosis drugs. Eur. J. Pharm. Sci 2007, 32, 140–150. [Google Scholar]
- Salomon, J.J.; Galeron, P.; Schulte, N.; Morow, P.R.; Severynse-Stevens, D.; Huwer, H.; Daum, N.; Lehr, C.-M.; Hickey, A.J.; Ehrhardt, C. Biopharmaceutical in vitro characterization of CPZEN-45, a drug candidate for inhalation therapy of tuberculosis. Ther. Deliv 2013, 4, 915–923. [Google Scholar]
- Manca, M.; Sinico, C.; Maccioni, A.; Diez, O.; Fadda, A.; Manconi, M. Composition influence on pulmonary delivery of rifampicin liposomes. Pharmaceutics 2012, 4, 590–606. [Google Scholar]
- Chimote, G.; Banerjee, R. In vitro evaluation of inhalable isoniazid-loaded surfactant liposomes as an adjunct therapy in pulmonary tuberculosis. J. Biomed. Mater. Res 2010, 94B, 1–10. [Google Scholar]
- Chuan, J.; Li, Y.; Yang, L.; Sun, X.; Zhang, Q.; Gong, T.; Zhang, Z. Enhanced rifampicin delivery to alveolar macrophages by solid lipid nanoparticles. J. Nanopart. Res 2013, 15. [Google Scholar] [CrossRef]
- Hadinoto, K.; Cheow, W.S. Nano-antibiotics in chronic lung infection therapy against Pseudomonas aeruginosa. Colloids Surf. B Biointerfaces 2014, in press. [Google Scholar] [CrossRef]
- Gupta, A.; Pandya, S.M.; Mohammad, I.; Agrawal, A.K.; Mohan, M.; Misra, A. Particulate pulmonary delivery systems containing anti-tuberculosis agents. Crit. Rev. Ther. Drug Carr. Syst 2013, 30, 277–291. [Google Scholar]
- Pulmaquin Website Source. Available online: http://investor.aradigm.com/releasedetail.cfm?releaseid=630968 (accessed on 9 January 2014).
- Liu, C.; Shi, J.; Dai, Q.; Yin, X.; Zhang, X.; Zheng, A. In-vitro and in-vivo evaluation of ciprofloxacin liposome for pulmonary administration. Drug Dev. Ind. Pharm 2013, 1–7. [Google Scholar] [CrossRef]
- Duan, J.; Vogt, F.G.; Li, X.; Hayes, D.; Mansour, H.M. Design, characterization, and aerosolization of organic solution advanced spray-dried moxifloxacin and ofloxacin dipalmitoylphosphatidylcholine (DPPC) microparticulate/nanoparticulate powders for pulmonary inhalation aerosol delivery. Int. J. Nanomed 2013, 8, 3489–3505. [Google Scholar]
- Pilcer, G.; Rosière, R.; Traina, K.; Sebti, T.; Vanderbist, F.; Amighi, K. New co-spray-dried tobramycin nanoparticles-clarithromycin inhaled powder systems for lung infection therapy in cystic fibrosis patients. J. Pharm. Sci 2013, 102, 1836–1846. [Google Scholar]
- Park, C.-W.; Li, X.; Vogt, F.G.; Hayes, D.; Zwischenberger, J.B.; Park, E.-S.; Mansour, H.M. Advanced spray-dried design, physicochemical characterization, and aerosol dispersion performance of vancomycin and clarithromycin multifunctional controlled release particles for targeted respiratory delivery as dry powder inhalation aerosols. Int. J. Pharm 2013, 455, 374–392. [Google Scholar]
- Moghaddam, P.H.; Ramezani, V.; Esfandi, E.; Vatanara, A.; Nabi-Meibodi, M.; Darabi, M.; Gilani, K.; Najafabadi, A.R. Development of a nano–micro carrier system for sustained pulmonary delivery of clarithromycin. Powder Technol 2013, 239, 478–483. [Google Scholar]
- Sinha, B.; Mukherjee, B.; Pattnaik, G. Poly-lactide-co-glycolide nanoparticles containing voriconazole for pulmonary delivery: In vitro and in vivo study. Nanomedicine 2013, 9, 94–104. [Google Scholar]
- Wu, X.; Hayes, D.; Zwischenberger, J.B.; Kuhn, R.J.; Mansour, H.M. Design and physicochemical characterization of advanced spray-dried tacrolimus multifunctional particles for inhalation. Drug Des. Dev. Ther 2013, 7, 59–72. [Google Scholar]
- Pardeike, J.; Weber, S.; Haber, T.; Wagner, J.; Zarfl, H.P.; Plank, H.; Zimmer, A. Development of an Itraconazole-loaded nanostructured lipid carrier (NLC) formulation for pulmonary application. Int. J. Pharm 2011, 419, 329–338. [Google Scholar]
- Duret, C.; Wauthoz, N.; Sebti, T.; Vanderbist, F.; Amighi, K. New inhalation-optimized itraconazole nanoparticle-based dry powders for the treatment of invasive pulmonary aspergillosis. Int. J. Nanomed 2012, 7, 5475–5489. [Google Scholar]
- Takeuchi, H.; Sugihara, H. Absorption of calcitonin in oral and pulmonary administration with polymer-coated liposomes. Yakugaku Zasshi 2010, 130, 1135–1142. [Google Scholar]
- Murata, M.; Yonamine, T.; Tanaka, S.; Tahara, K.; Tozuka, Y.; Takeuchi, H. Surface modification of liposomes using polymer-wheat germ agglutinin conjugates to improve the absorption of peptide drugs by pulmonary administration. J. Pharm. Sci 2013, 102, 1281–1289. [Google Scholar]
- Trapani, A.; di Gioia, S.; Ditaranto, N.; Cioffi, N.; Goycoolea, F.M.; Carbone, A.; Garcia-Fuentes, M.; Conese, M.; Alonso, M.J. Systemic heparin delivery by the pulmonary route using chitosan and glycol chitosan nanoparticles. Int. J. Pharm 2013, 447, 115–123. [Google Scholar]
- Liu, J.; Gong, T.; Fu, H.; Wang, C.; Wang, X.; Chen, Q.; Zhang, Q.; He, Q.; Zhang, Z. Solid lipid nanoparticles for pulmonary delivery of insulin. Int. J. Pharm 2008, 356, 333–344. [Google Scholar]
- Zhao, Y.-Z.; Li, X.; Lu, C.-T.; Xu, Y.-Y.; Lv, H.-F.; Dai, D.-D.; Zhang, L.; Sun, C.-Z.; Yang, W.; Li, X.-K.; et al. Experiment on the feasibility of using modified gelatin nanoparticles as insulin pulmonary administration system for diabetes therapy. Acta Diabetol 2012, 49, 315–325. [Google Scholar]
- Lee, C.; Choi, J.S.; Kim, I.; Oh, K.T.; Lee, E.S.; Park, E.-S.; Lee, K.C.; Youn, Y.S. Long-acting inhalable chitosan-coated poly(lactic-co-glycolic acid) nanoparticles containing hydrophobically modified exendin-4 for treating type 2 diabetes. Int. J. Nanomed 2013, 8, 2975–2983. [Google Scholar]
- Kleemann, E.; Schmehl, T.; Gessler, T.; Bakowsky, U.; Kissel, T.; Seeger, W. Iloprost-containing liposomes for aerosol application in pulmonary arterial hypertension: Formulation aspects and stability. Pharm. Res 2007, 24, 277–287. [Google Scholar]
- Beck-Broichsitter, M.; Schmehl, T.; Gessler, T.; Seeger, W.; Kissel, T. Development of a biodegradable nanoparticle platform for sildenafil: Formulation optimization by factorial design analysis combined with application of charge-modified branched polyesters. J. Control. Release 2012, 157, 469–477. [Google Scholar]
- Varshosaz, J.; Taymouri, S.; Hamishehkar, H. Fabrication of polymeric nanoparticles of poly(ethylene-co-vinyl acetate) coated with chitosan for pulmonary delivery of carvedilol. J. Appl. Polym. Sci 2014, 131. [Google Scholar] [CrossRef]
- Park, S.; Jeong, E.J.; Lee, J.; Rhim, T.; Lee, S.K.; Lee, K.Y. Preparation and characterization of nonaarginine-modified chitosan nanoparticles for siRNA delivery. Carbohydr. Polym 2013, 92, 57–62. [Google Scholar]
- Sharma, K.; Somavarapu, S.; Colombani, A.; Govind, N.; Taylor, K.M.G. Nebulised siRNA encapsulated crosslinked chitosan nanoparticles for pulmonary delivery. Int. J. Pharm 2013, 455, 241–247. [Google Scholar]
- Beck-Broichsitter, M.; Ruppert, C.; Schmehl, T.; Günther, A.; Seeger, W. Biophysical inhibition of synthetic vs. naturally-derived pulmonary surfactant preparations by polymeric nanoparticles. Biochim. Biophys. Acta 2013, 1838, 474–481. [Google Scholar]
- Rudiger, M. Naturally derived commercial surfactants differ in composition of surfactant lipids and in surface viscosity. AJP: Lung Cell. Mol. Physiol 2004, 288, L379–L383. [Google Scholar]
- Veldhuizen, R.; Nag, K.; Orgeig, S.; Possmayer, F. The role of lipids in pulmonary surfactant. Biochim. Biophys. Acta 1998, 1408, 90–108. [Google Scholar]
- Wood, A.J.; Jobe, A.H. Pulmonary surfactant therapy. N. Engl. J. Med 1993, 328, 861–868. [Google Scholar]
- Willis, L.; Hayes, D.; Mansour, H.M. Therapeutic liposomal dry powder inhalation aerosols for targeted lung delivery. Lung 2012, 190, 251–262. [Google Scholar]
- Ribeiro, A.M.; Souza, A.C.O.; Amaral, A.C.; Vasconcelos, N.M.; Jerônimo, M.S.; Carneiro, F.P.; Faccioli, L.H.; Felipe, M.S.S.; Silva, C.L.; Bocca, A.L. Nanobiotechnological approaches to delivery of DNA vaccine against fungal infection. J. Biomed. Nanotechnol 2013, 9, 221–230. [Google Scholar]
- Srinivasan, A.R.; Shoyele, S.A. Self-associated submicron IgG1 particles for pulmonary delivery: Effects of non-ionic surfactants on size, shape, stability, and aerosol performance. AAPS PharmSciTech 2013, 14, 200–210. [Google Scholar]
- Rampino, A.; Borgogna, M.; Blasi, P.; Bellich, B.; Cesàro, A. Chitosan nanoparticles: Preparation, size evolution and stability. Int. J. Pharm 2013, 455, 219–228. [Google Scholar]
- Gaspar, M.M.; Bakowsky, U.; Ehrhardt, C. Inhaled liposomes–Current strategies and future challenges. J. Biomed. Nanotechnol 2008, 4, 245–257. [Google Scholar]
- Cipolla, D.; Wu, H.; Eastman, S.; Redelmeier, T.; Gonda, I.; Chan, H.-K. Development and characterization of an in vitro release assay for liposomal ciprofloxacin for inhalation. J. Pharm. Sci 2014, 103, 314–327. [Google Scholar]
- Clancy, J.P.; Dupont, L.; Konstan, M.W.; Billings, J.; Fustik, S.; Goss, C.H.; Lymp, J.; Minic, P.; Quittner, A.L.; Rubenstein, R.C.; et al. Phase II studies of nebulised Arikace in CF patients with Pseudomonas aeruginosa infection. Thorax 2013, 68, 818–825. [Google Scholar]
- Hood, E.D.; Chorny, M.; Greineder, C.F.; Alferiev, I.S.; Levy, R.J.; Muzykantov, V.R. Endothelial targeting of nanocarriers loaded with antioxidant enzymes for protection against vascular oxidative stress and inflammation. Biomaterials 2014, 35, 3708–3715. [Google Scholar]
- Bunjes, H. Lipid nanoparticles for the delivery of poorly water-soluble drugs. J. Pharm. Pharmacol 2010, 62, 1637–1645. [Google Scholar]
- Bunjes, H. Structural properties of solid lipid based colloidal drug delivery systems. Curr. Opin. Colloid Interface Sci 2011, 16, 405–411. [Google Scholar]
- Bunjes, H.; Unhruh, T. Characterization of lipid nanoparticles by differential scanning calorimetry, X-ray and neutron scattering. Adv. Drug Deliv. Rev 2007, 59, 379–402. [Google Scholar]
- Ehrhardt, C.; Kim, K.-J.; Lehr, C.-M. Human cell culture protocols: Isolation and culture of human alveolar epithelial cells. Methods Mol. Med 2004, 15, 207–216. [Google Scholar]
- Ehrhardt, C.; Laue, M.; Kim, K.-J. In vitro models of the alveolar epithelial barrier. In Drug Absorption Studies; Springer US: Boston, MA, USA, 2008; pp. 258–282. [Google Scholar]
- Forbes, B.; Shah, A.; Martin, G.P.; Lansley, A.B. The human bronchial epithelial cell line 16HBE14o− as a model system of the airways for studying drug transport. Int. J. Pharm 2003, 257, 161–167. [Google Scholar]
- Scherließ, R. The MTT assay as tool to evaluate and compare excipient toxicity in vitro on respiratory epithelial cells. Int. J. Pharm 2011, 411, 98–105. [Google Scholar]
- Sakagami, M. In vivo, in vitro and ex vivo models to assess pulmonary absorption and disposition of inhaled therapeutics for systemic delivery. Adv. Drug Deliv. Rev 2006, 58, 1030–1060. [Google Scholar]
- Foster, K.A.; Avery, M.L.; Yazdanian, M.; Audus, K.L. Characterization of the Calu-3 cell line as a tool to screen pulmonary drug delivery. Int. J. Pharm 2000, 208, 1–11. [Google Scholar]
- Neuhaus, V.; Schwarz, K.; Klee, A.; Seehase, S.; Förster, C.; Pfennig, O.; Jonigk, D.; Fieguth, H.-G.; Koch, W.; Warnecke, G.; et al. Functional testing of an inhalable nanoparticle based influenza vaccine using a human precision cut lung slice technique. PLoS One 2013, 8, e71728. [Google Scholar]
- Kaneko, M.; Coppen, S.R. Histological validation of heart slices as a model in cardiac research. J. Cell Sci. Ther 2012, 3. [Google Scholar] [CrossRef]
- Wang, T.; Liu, Y.; Chen, L.; Wang, X.; Hu, X.-R.; Feng, Y.-L.; Liu, D.-S.; Xu, D.; Duan, Y.-P.; Lin, J.; et al. Effect of sildenafil on acrolein-induced airway inflammation and mucus production in rats. Eur. Respir. J 2009, 33, 1122–1132. [Google Scholar]
- Knapp, S. LPS and bacterial lung inflammation models. Drug Discov. Today: Dis. Models 2009, 6, 113–118. [Google Scholar]
- Marsboom, G.R.; Janssens, S.P. Models for pulmonary hypertension. Drug Discov. Today: Dis. Models 2004, 1, 289–296. [Google Scholar]
- Arora, S.; Rajwade, J.M.; Paknikar, K.M. Nanotoxicology and in vitro studies: The need of the hour. Toxicol. Appl. Pharm 2012, 258, 151–165. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Location | Size | Mechanism |
|---|---|---|
| Primary Bronchi | 5–10 μm | Impaction |
| Secondary Bronchi | 1–5 μm | Sedimentation |
| Bronchioles | 1–3 μm | Sedimentation |
| Alveoli | 0.5–1 μm | Brownian motion |
| Disease/API category | Type of particles | Reference |
|---|---|---|
| Anti-asthma/anti-inflammatory | ||
| Beclomethasone | Lipid NC | [25] |
| Budesonide | SLN, liposomes | [26,27] |
| Curcumin | SLN, polymeric NP | [22,28] |
| Indomethacin | Lipid NP | [29] |
| Fluticasone | Dried NP | [30] |
| Pirfenidone | Polymeric NP | [31] |
| Anti-cancer | ||
| Cisplatin | Dried NP | [32,33] |
| Methotrexate | Polymeric NP | [34] |
| Paclitaxel | Polymeric NP | [35–37] |
| Silibinin | SLN | [38] |
| Anti-oxidants | ||
| Antioxidants-multiple types | Liposomes, polymeric NP, SLM | [21,39,40] |
| Lung infections | ||
| Amikacin | Liposomes, SLN | [23,41,42] |
| Amphotericin B (Ambisome®) | Liposomes (parenteral) | [43] |
| Anti-tuberculosis drugs | SLN, polymeric NP, Liposomes | [27,44–53] |
| Ciprofloxacin | Liposomes | [54,55] |
| Moxifloxacin-Ofloxacin | Dried NP, MP | [56] |
| Tobramycin-Clarithromycin-Vancomycin | Spray dried NP, MP | [57–59] |
| Voriconazole | Polymeric NP | [60] |
| Tacrolimus | Lipid NP | [61] |
| Itraconazole | Lipid NC, dried NP | [62,63] |
| Proteins, peptides and macromolecules | ||
| Calcitonin | Polymeric liposomes | [64,65] |
| Heparin | Polymeric NP | [66] |
| Insulin | SLN | [67,68] |
| Exendin-4 | Polymeric NP | [69] |
| Pulmonary arterial hypertension/Congestive heart failure | ||
| Iloprost | Liposomes | [70] |
| Sildenafil | Polymeric NP, SLN | [10,71] |
| Carvedilol | Polymeric NP | [72] |
| Surfactant, gene and antibody delivery | ||
| siRNA/gene | Polymeric NP | [73,74] |
| Surfactant therapy | Liposomes | [75–79] |
| DNA vaccine | Polymeric liposomes | [80] |
| IgG1 | Self-assembly NP | [81] |
© 2014 by the authors; licensee MDPI, Basel, Switzerland This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Paranjpe, M.; Müller-Goymann, C.C. Nanoparticle-Mediated Pulmonary Drug Delivery: A Review. Int. J. Mol. Sci. 2014, 15, 5852-5873. https://doi.org/10.3390/ijms15045852
Paranjpe M, Müller-Goymann CC. Nanoparticle-Mediated Pulmonary Drug Delivery: A Review. International Journal of Molecular Sciences. 2014; 15(4):5852-5873. https://doi.org/10.3390/ijms15045852
Chicago/Turabian StyleParanjpe, Mukta, and Christel C. Müller-Goymann. 2014. "Nanoparticle-Mediated Pulmonary Drug Delivery: A Review" International Journal of Molecular Sciences 15, no. 4: 5852-5873. https://doi.org/10.3390/ijms15045852