
How People’s COVID-19 Induced-Worries and Multiple Environmental Exposures Are Associated with Their Depression, Anxiety, and Stress during the Pandemic

Abstract
:1. Introduction
2. Dataset and Methods
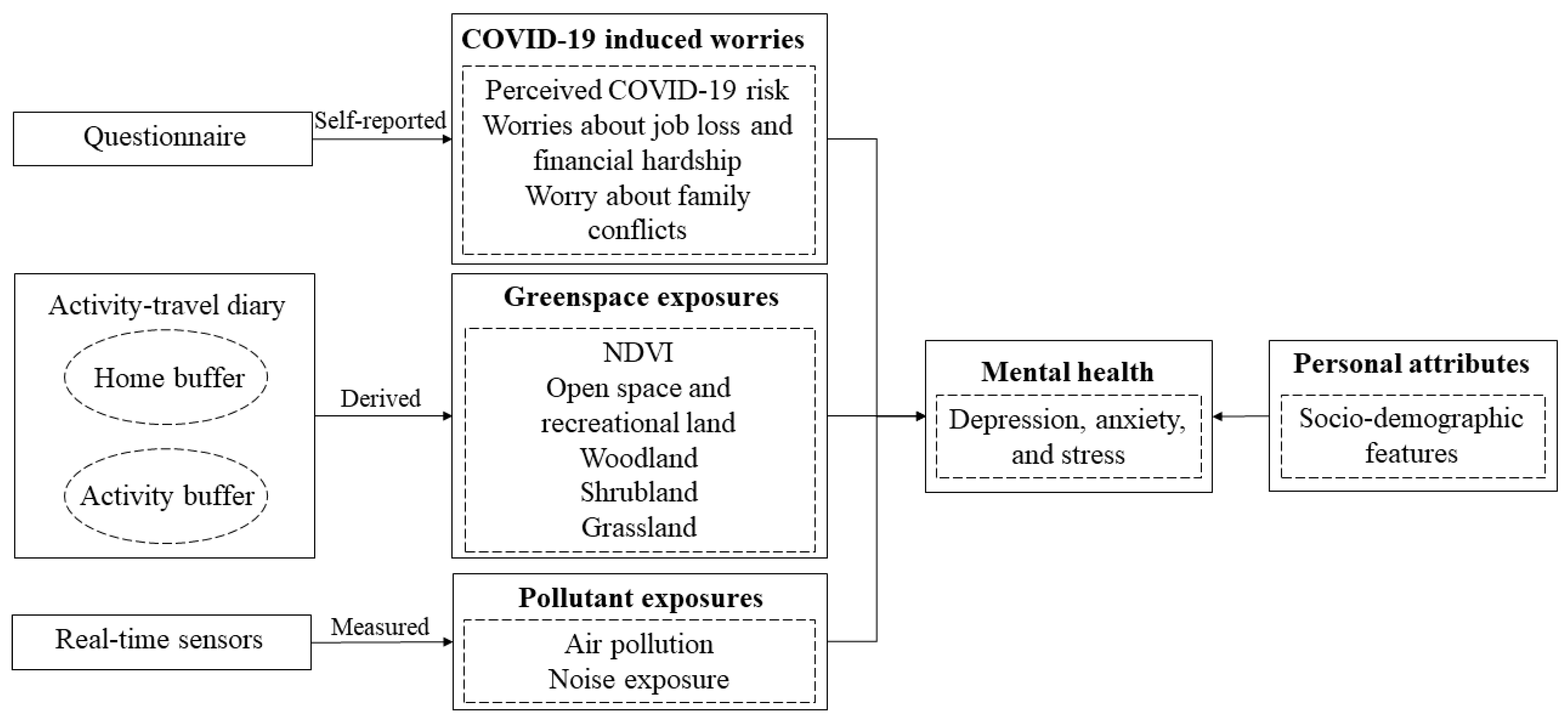
2.1. Study Design and Sampling
2.2. Depression, Anxiety, and Stress as Outcomes
2.3. COVID-19-Induced Worries
2.4. Greenspace Exposure Assessment
2.5. PM2.5 and Noise Exposures
2.6. Statistical Analyses
3. Results
3.1. Descriptive Statistics
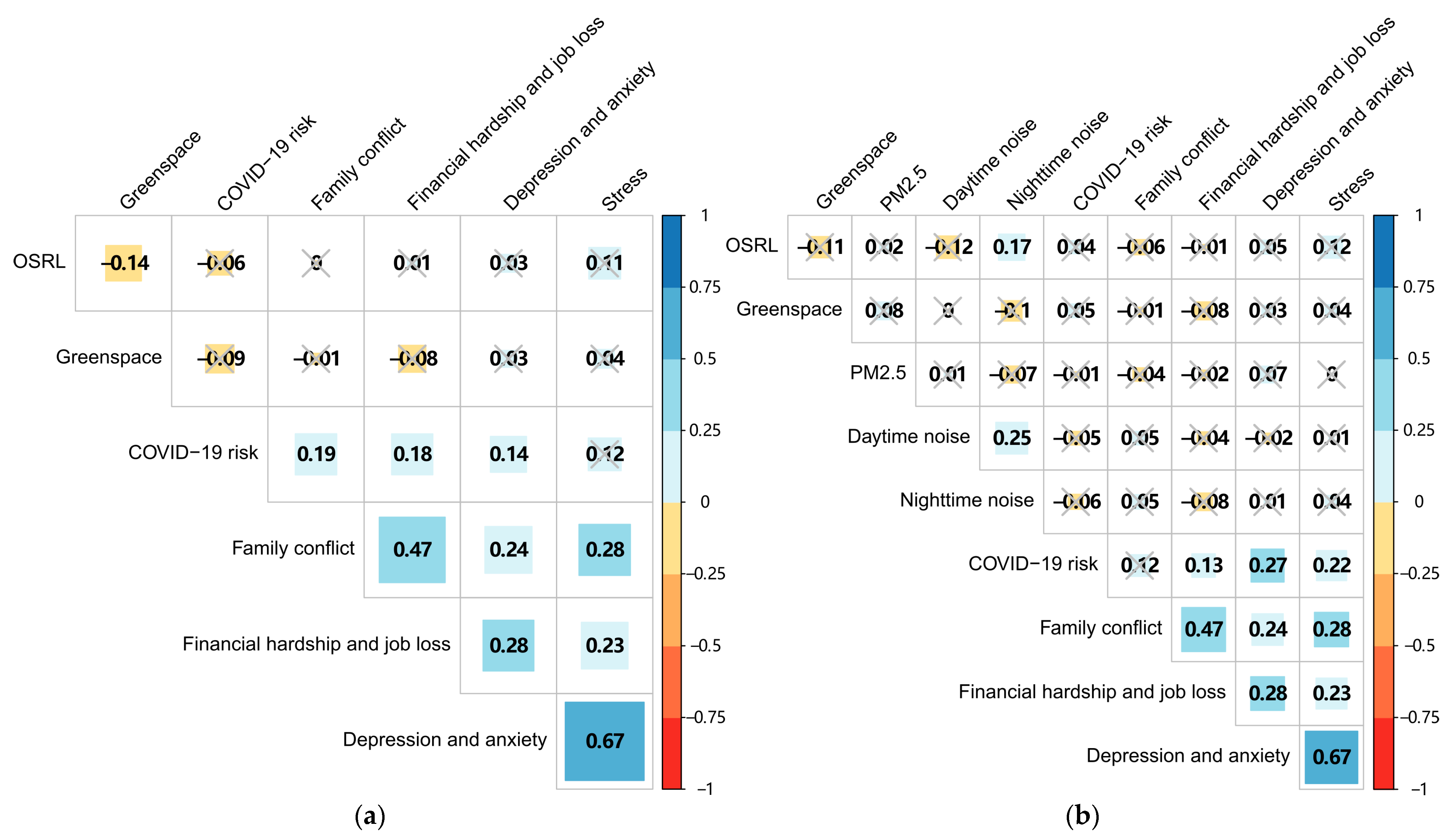
3.2. Bivariate Analysis
3.3. Regression Analysis
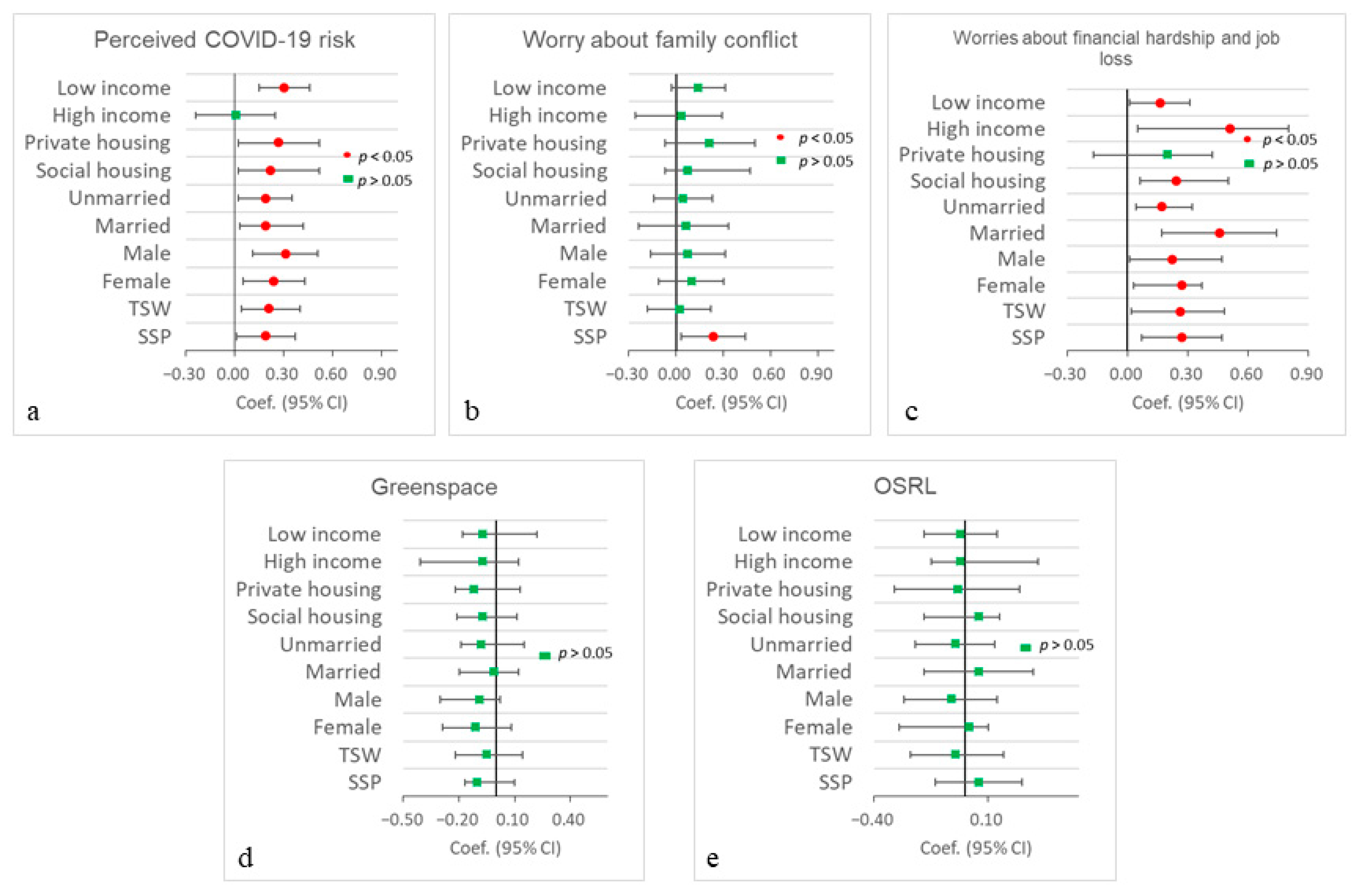
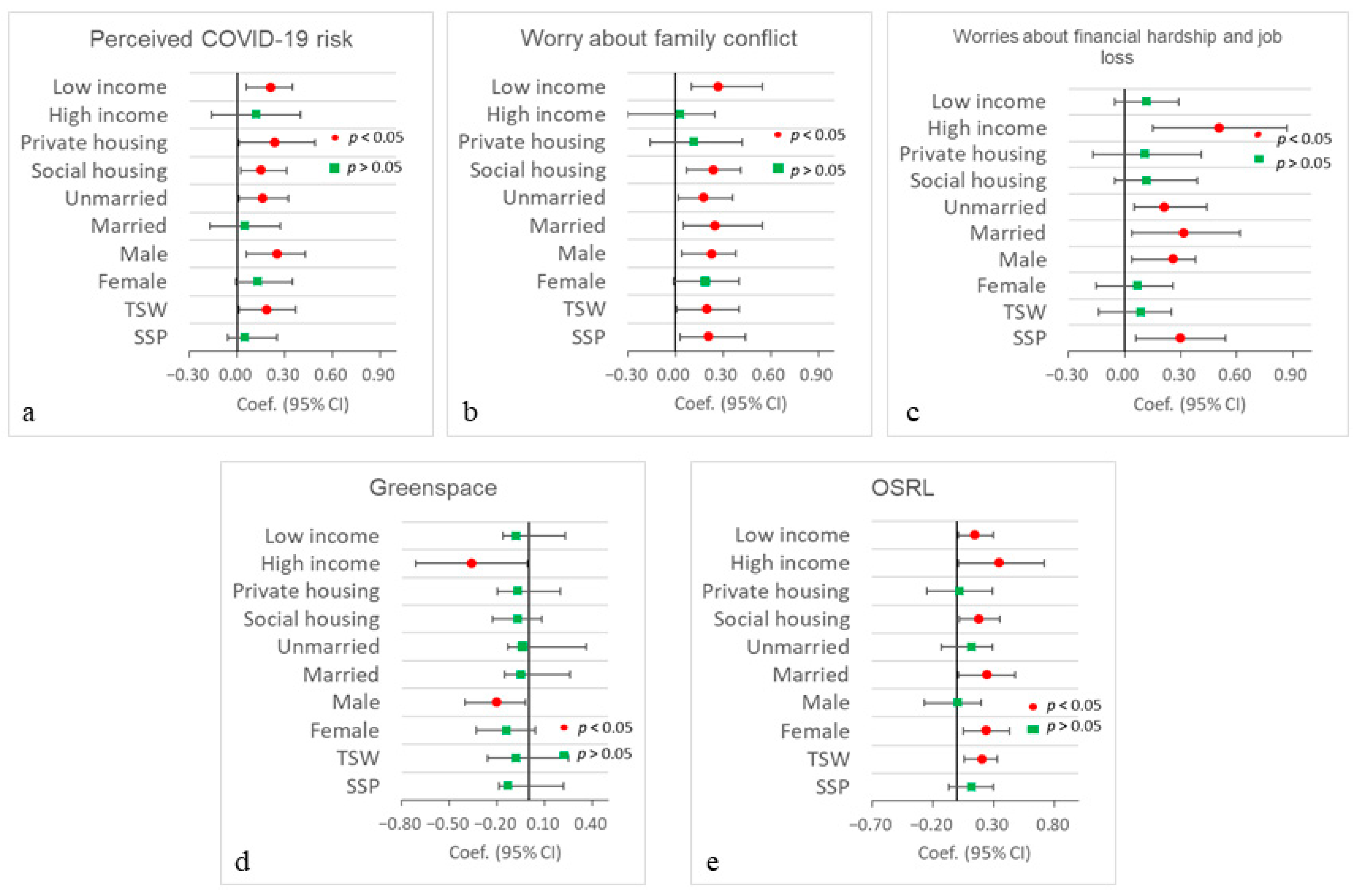
3.4. Stratified Analysis
4. Discussion
4.1. Main Findings
4.2. Comparisons with Previous Studies and Implications
4.3. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Davies, N.G.; Kucharski, A.J.; Eggo, R.M.; Gimma, A.; Edmunds, W.J.; Jombart, T.; O’Reilly, K.; Endo, A.; Hellewell, J.; Nightingale, E.S.; et al. Effects of non-pharmaceutical interventions on COVID-19 cases, deaths, and demand for hospital services in the UK: A modelling study. Lancet Public Health 2020, 5, e375–e385. [Google Scholar] [CrossRef]
- Alessandretti, L. What human mobility data tell us about COVID-19 spread. Nat. Rev. Phys 2022, 4, 12–13. [Google Scholar] [CrossRef]
- Bradshaw, W.J.; Alley, E.C.; Huggins, J.H.; Lloyd, A.L.; Esvelt, K.M. Bidirectional contact tracing could dramatically improve COVID-19 control. Nat. Commun. 2021, 12, 232. [Google Scholar] [CrossRef] [PubMed]
- Nouvellet, P.; Bhatia, S.; Cori, A.; Ainslie, K.E.; Baguelin, M.; Bhatt, S.; Boonyasiri, A.; Brazeau, N.F.; Cattarino, L.; Cooper, L.V.; et al. Reduction in mobility and COVID-19 transmission. Nat. Commun. 2021, 12, 1090. [Google Scholar] [CrossRef]
- Xiong, J.; Lipsitz, O.; Nasri, F.; Lui, L.M.; Gill, H.; Phan, L.; Chen-Li, D.; Iacobucci, M.; Ho, R.; Majeed, A.; et al. Impact of COVID-19 pandemic on mental health in the general population: A systematic review. J. Affect. Disord. 2020, 277, 55–64. [Google Scholar] [CrossRef]
- Passavanti, M.; Argentieri, A.; Barbieri, D.M.; Lou, B.; Wijayaratna, K.; Mirhosseini, A.S.F.; Wang, F.; Naseri, S.; Qamhia, I.; Tangerås, M.; et al. The psychological impact of COVID-19 and restrictive measures in the world. J. Affect. Disord. 2021, 283, 36–51. [Google Scholar] [CrossRef] [PubMed]
- Gadermann, A.C.; Thomson, K.C.; Richardson, C.G.; Gagné, M.; McAuliffe, C.; Hirani, S.; Jenkins, E. Examining the impacts of the COVID-19 pandemic on family mental health in Canada: Findings from a national cross-sectional study. BMJ Open 2021, 11, e042871. [Google Scholar] [CrossRef] [PubMed]
- Posel, D.; Oyenubi, A.; Kollamparambil, U. Job loss and mental health during the COVID-19 lockdown: Evidence from South Africa. PLoS ONE 2021, 16, e0249352. [Google Scholar] [CrossRef]
- Pierce, M.; Hope, H.; Ford, T.; Hatch, S.; Hotopf, M.; John, A.; Kontopantelis, E.; Webb, R.; Wessely, S.; McManus, S.; et al. Mental health before and during the COVID-19 pandemic: A longitudinal probability sample survey of the UK population. Lancet Psychiatry 2020, 7, 883–892. [Google Scholar] [CrossRef]
- Goularte, J.F.; Serafim, S.D.; Colombo, R.; Hogg, B.; Caldieraro, M.A.; Rosa, A.R. COVID-19 and mental health in Brazil: Psychiatric symptoms in the general population. J. Psychiatr. Res. 2021, 132, 32–37. [Google Scholar] [CrossRef]
- Généreux, M.; Schluter, P.J.; Landaverde, E.; Hung, K.K.; Wong, C.S.; Mok, C.P.Y.; Blouin-Genest, G.; O’sullivan, T.; David, M.D.; Carignan, M.E.; et al. The evolution in anxiety and depression with the progression of the pandemic in adult populations from eight countries and four continents. Int. J. Environ. Res. Public Health 2021, 18, 4845. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, E.K.; McAuliffe, C.; Hirani, S.; Richardson, C.; Thomson, K.C.; McGuinness, L.; Morris, J.; Kousoulis, A.; Gadermann, A. A portrait of the early and differential mental health impacts of the COVID-19 pandemic in Canada: Findings from the first wave of a nationally representative cross-sectional survey. Prev. Med. 2021, 145, 106333. [Google Scholar] [CrossRef] [PubMed]
- Markevych, I.; Schoierer, J.; Hartig, T.; Chudnovsky, A.; Hystad, P.; Dzhambov, A.M.; De Vries, S.; Triguero-Mas, M.; Brauer, M.; Nieuwenhuijsen, M.J.; et al. Exploring pathways linking greenspace to health: Theoretical and methodological guidance. Environ. Res. 2017, 158, 301–317. [Google Scholar] [CrossRef] [PubMed]
- Kondo, M.C.; Fluehr, J.M.; McKeon, T.; Branas, C.C. Urban green space and its impact on human health. Int. J. Environ. Res. Public Health 2018, 15, 445. [Google Scholar] [CrossRef]
- Bratman, G.N.; Anderson, C.B.; Berman, M.G.; Cochran, B.; De Vries, S.; Flanders, J.; Folke, C.; Frumkin, H.; Gross, J.J.; Hartig, T.; et al. Nature and mental health: An ecosystem service perspective. Sci. Adv. 2019, 5, eaax0903. [Google Scholar] [CrossRef]
- Klompmaker, J.O.; Hoek, G.; Bloemsma, L.D.; Wijga, A.H.; van den Brink, C.; Brunekreef, B.; Lebret, E.; Gehring, U.; Janssen, N.A. Associations of combined exposures to surrounding green, air pollution and traffic noise on mental health. Environ. Int. 2019, 129, 525–537. [Google Scholar] [CrossRef]
- Ribeiro, A.I.; Triguero-Mas, M.; Santos, C.J.; Gómez-Nieto, A.; Cole, H.; Anguelovski, I.; Silva, F.M.; Baró, F. Exposure to nature and mental health outcomes during COVID-19 lockdown. A comparison between Portugal and Spain. Environ. Int. 2021, 154, 106664. [Google Scholar] [CrossRef]
- Poortinga, W.; Bird, N.; Hallingberg, B.; Phillips, R.; Williams, D. The role of perceived public and private green space in subjective health and wellbeing during and after the first peak of the COVID-19 outbreak. Landsc. Urban Plan. 2021, 211, 104092. [Google Scholar] [CrossRef]
- Tiako, M.J.N.; South, E.; Shannon, M.M.; McCarthy, C.; Meisel, Z.F.; Elovitz, M.A.; Burris, H.H. Urban residential tree canopy and perceived stress among pregnant women. Environ. Res. 2021, 201, 111620. [Google Scholar] [CrossRef]
- Larson, L.R.; Mullenbach, L.E.; Browning, M.H.; Rigolon, A.; Thomsen, J.; Metcalf, E.C.; Reigner, N.P.; Sharaievska, I.; McAnirlin, O.; D’Antonio, A.; et al. Greenspace and park use associated with less emotional distress among college students in the United States during the COVID-19 pandemic. Environ. Res. 2022, 204, 112367. [Google Scholar] [CrossRef]
- da Schio, N.; Phillips, A.; Fransen, K.; Wolff, M.; Haase, D.; Ostoić, S.K.; Živojinović, I.; Vuletić, D.; Derks, J.; Davies, C.; et al. The impact of the COVID-19 pandemic on the use of and attitudes towards urban forests and green spaces: Exploring the instigators of change in Belgium. Urban For. Urban Green 2021, 65, 127305. [Google Scholar] [CrossRef] [PubMed]
- Mouratidis, K.; Yiannakou, A. COVID-19 and urban planning: Built environment, health, and well-being in Greek cities before and during the pandemic. Cities 2022, 121, 103491. [Google Scholar] [CrossRef] [PubMed]
- Allard-Poesi, F.; Matos, L.B.; Massu, J. Not all types of nature have an equal effect on urban residents’ well-being: A structural equation model approach. Health Place 2022, 74, 102759. [Google Scholar] [CrossRef] [PubMed]
- Tzivian, L.; Winkler, A.; Dlugaj, M.; Schikowski, T.; Vossoughi, M.; Fuks, K.; Weinmayr, G.; Hoffmann, B. Effect of long-term outdoor air pollution and noise on cognitive and psychological functions in adults. Int. J. Hyg. Environ. Health 2015, 218, 1–11. [Google Scholar] [CrossRef]
- Dzhambov, A.M.; Markevych, I.; Tilov, B.; Arabadzhiev, Z.; Stoyanov, D.; Gatseva, P.; Dimitrova, D.D. Pathways linking residential noise and air pollution to mental ill-health in young adults. Environ. Res. 2018, 166, 458–465. [Google Scholar] [CrossRef]
- van den Bosch, M.; Meyer-Lindenberg, A. Environmental exposures and depression: Biological mechanisms and epidemiological evidence. Annu. Rev. Public Health 2019, 40, 239–259. [Google Scholar] [CrossRef] [PubMed]
- Recio, A.; Linares, C.; Banegas, J.R.; Díaz, J. Road traffic noise effects on cardiovascular, respiratory, and metabolic health: An integrative model of biological mechanisms. Environ. Res. 2016, 146, 359–370. [Google Scholar] [CrossRef]
- Guski, R.; Schreckenberg, D.; Schuemer, R. WHO environmental noise guidelines for the European region: A systematic review on environmental noise and annoyance. Int. J. Environ. Res. Public Health 2017, 14, 1539. [Google Scholar] [CrossRef]
- Shepherd, D.; Dirks, K.; Welch, D.; McBride, D.; Landon, J. The covariance between air pollution annoyance and noise annoyance, and its relationship with health-related quality of life. Int. J. Environ. Res. Public Health 2016, 13, 792. [Google Scholar] [CrossRef] [PubMed]
- Tao, Y.; Kou, L.; Chai, Y.; Kwan, M.P. Associations of co-exposures to air pollution and noise with psychological stress in space and time: A case study in Beijing, China. Environ. Res. 2021, 196, 110399. [Google Scholar] [CrossRef]
- Kwan, M.P. The uncertain geographic context problem. Ann. Assoc. Am. Geogr. 2012, 102, 958–968. [Google Scholar] [CrossRef]
- Kwan, M.P. The neighborhood effect averaging problem (NEAP): An elusive confounder of the neighborhood effect. Int. J. Environ. Res. Public Health 2018, 15, 1841. [Google Scholar] [CrossRef] [PubMed]
- Dewulf, B.; Neutens, T.; Lefebvre, W.; Seynaeve, G.; Vanpoucke, C.; Beckx, C.; Van de Weghe, N. Dynamic assessment of exposure to air pollution using mobile phone data. Int. J. Health Geogr. 2016, 15, 14. [Google Scholar] [CrossRef] [PubMed]
- James, P.; Berrigan, D.; Hart, J.E.; Hipp, J.A.; Hoehner, C.M.; Kerr, J.; Major, J.M.; Oka, M.; Laden, F. Effects of buffer size and shape on associations between the built environment and energy balance. Health Place 2014, 27, 162–170. [Google Scholar] [CrossRef] [PubMed]
- Seidler, A.; Hegewald, J.; Seidler, A.L.; Schubert, M.; Wagner, M.; Dröge, P.; Haufe, E.; Schmitt, J.; Swart, E.; Zeeb, H. Association between aircraft, road and railway traffic noise and depression in a large case-control study based on secondary data. Environ. Res. 2017, 152, 263–271. [Google Scholar] [CrossRef]
- Gascon, M.; Sánchez-Benavides, G.; Dadvand, P.; Martínez, D.; Gramunt, N.; Gotsens, X.; Cirach, M.; Vert, C.; Molinuevo, J.L.; Crous-Bou, M.; et al. Long-term exposure to residential green and blue spaces and anxiety and depression in adults: A cross-sectional study. Environ. Res. 2018, 162, 231–239. [Google Scholar] [CrossRef]
- Klompmaker, J.O.; Janssen, N.A.; Bloemsma, L.D.; Gehring, U.; Wijga, A.H.; van den Brink, C.; Lebret, E.; Brunekreef, B.; Hoek, G. Residential surrounding green, air pollution, traffic noise and self-perceived general health. Environ. Res. 2019, 179, 108751. [Google Scholar] [CrossRef]
- Yu, H.; Russell, A.; Mulholland, J.; Huang, Z. Using cell phone location to assess misclassification errors in air pollution exposure estimation. Environ. Pollut. 2018, 233, 261–266. [Google Scholar] [CrossRef]
- Helbich, M. Toward dynamic urban environmental exposure assessments in mental health research. Environ. Res. 2018, 161, 129–135. [Google Scholar] [CrossRef]
- Huang, J.; Kwan, M.P. Uncertainties in the assessment of COVID-19 risk: A Study of people’s exposure to high-risk environments using individual-level activity data. Ann. Assoc. Am. Geogr. 2022, 112, 968–987. [Google Scholar] [CrossRef]
- Huang, J.; Kwan, M.P. Associations between COVID-19 risk, multiple environmental exposures, and housing conditions: A study using individual-level GPS-based real-time sensing data. Appl. Geogr. 2023, 153, 102904. [Google Scholar] [CrossRef] [PubMed]
- Yu, Z.; Liu, X. Spatial variations of the third and fourth COVID-19 waves in Hong Kong: A comparative study using built environment and socio-demographic characteristics. Environ. Plan. B Urban Anal. City Sci. 2023, 50, 1144–1160. [Google Scholar] [CrossRef]
- Kan, Z.; Kwan, M.P.; Ng, M.K.; Tieben, H. The impacts of housing characteristics and built-environment features on mental health. Int. J. Environ. Res. Public Health 2022, 19, 5143. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Kwan, M.P. Examining the influence of housing conditions and daily greenspace exposure on people’s perceived COVID-19 risk and distress. Int. J. Environ. Res. Public Health 2022, 19, 8876. [Google Scholar] [CrossRef]
- Huang, J.; Kwan, M.P.; Kan, Z. The superspreading places of COVID-19 and the associated built-environment and socio-demographic features: A study using a spatial network framework and individual-level activity data. Health Place 2021, 72, 102694. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.; Löwe, B. An ultra-brief screening scale for anxiety and depression: The PHQ–4. Psychosomatics 2009, 50, 613–621. [Google Scholar] [CrossRef]
- Huang, J.; Kwan, M.P.; Cai, J.; Song, W.; Yu, C.; Kan, Z.; Yim, S.H.L. Field evaluation and calibration of low-cost air pollution sensors for environmental exposure research. Sensors 2022, 22, 2381. [Google Scholar] [CrossRef]
- Choi, E.P.H.; Hui, B.P.H.; Wan, E.Y.F. Depression and anxiety in Hong Kong during COVID-19. Int. J. Environ. Res. Public Health 2020, 17, 3740. [Google Scholar] [CrossRef]
- Robillard, R.; Saad, M.; Edwards, J.; Solomonova, E.; Pennestri, M.H.; Daros, A.; Veissière, S.P.L.; Quilty, L.; Dion, K.; Nixon, A.; et al. Social, financial and psychological stress during an emerging pandemic: Observations from a population survey in the acute phase of COVID-19. BMJ Open 2020, 10, e043805. [Google Scholar] [CrossRef]
- Wilson, J.M.; Lee, J.; Fitzgerald, H.N.; Oosterhoff, B.; Sevi, B.; Shook, N.J. Job insecurity and financial concern during the COVID-19 pandemic are associated with worse mental health. Int. J. Occup. Environ. Med. 2020, 62, 686–691. [Google Scholar] [CrossRef]
- Zhao, S.Z.; Wong, J.Y.H.; Luk, T.T.; Wai, A.K.C.; Lam, T.H.; Wang, M.P. Mental health crisis under COVID-19 pandemic in Hong Kong, China. Int. J. Infect. Dis. 2020, 100, 431–433. [Google Scholar] [CrossRef] [PubMed]
- Miconi, D.; Li, Z.Y.; Frounfelker, R.L.; Santavicca, T.; Cénat, J.M.; Venkatesh, V.; Rousseau, C. Ethno-cultural disparities in mental health during the COVID-19 pandemic: A cross-sectional study on the impact of exposure to the virus and COVID-19-related discrimination and stigma on mental health across ethno-cultural groups in Quebec (Canada). BJPsych Open 2021, 7, E14. [Google Scholar] [CrossRef] [PubMed]
- Singh, R.; Subedi, M. COVID-19 and stigma: Social discrimination towards frontline healthcare providers and COVID-19 recovered patients in Nepal. Asian J. Psychiatr. 2020, 53, 102222. [Google Scholar] [CrossRef]
- Fan, W.; Qian, Y.; Jin, Y. Stigma, Perceived Discrimination, and Mental Health during China’s COVID-19 Outbreak: A Mixed-Methods Investigation. J. Health Soc. Behav. 2021, 62, 562–581. [Google Scholar] [CrossRef]
- Saiz, J.; Muñoz, M.; Ausín, B.; González-Sanguino, C.; Ángel Castellanos, M.; Vaquero, C.; Ugidos, C.; López-Gómez, A. Effects of COVID-19 lockdown on perceived discrimination and internalized stigma in people with previous mental disorder diagnoses in Spain. Am. J. Orthopsychiatry 2021, 91, 407. [Google Scholar] [CrossRef]
- Liu, Y.; Finch, B.K.; Brenneke, S.G.; Thomas, K.; Le, P.D. Perceived discrimination and mental distress amid the COVID-19 pandemic: Evidence from the understanding America study. Am. J. Prev. Med. 2020, 59, 481–492. [Google Scholar] [CrossRef]
- Melton, H.C.; Belknap, J. He hits, she hits: Assessing gender differences and similarities in officially reported intimate partner violence. Crim. Justice Behav. 2003, 30, 328–348. [Google Scholar] [CrossRef]
- Caldwell, J.E.; Swan, S.C.; Woodbrown, V.D. Gender differences in intimate partner violence outcomes. Psychol. Violence 2012, 2, 42. [Google Scholar] [CrossRef]
- Winstok, Z.; Straus, M.A. Bridging the two sides of a 30-year controversy over gender differences in perpetration of physical partner violence. J. Fam. Violence 2016, 31, 933–935. [Google Scholar] [CrossRef]
- Roberts, H.; Helbich, M. Multiple environmental exposures along daily mobility paths and depressive symptoms: A smartphone-based tracking study. Environ. Int. 2021, 156, 106635. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Category | SSP (n = 107) | TSW (n = 110) | |
|---|---|---|---|---|
| N (%) | N (%) | |||
| Socio-demographic status and housing conditions | Sex | Male | 44% | 46% |
| Female | 56% | 54% | ||
| Age | 18–24 years | 17% | 22% | |
| 25–44 years | 47% | 47% | ||
| 45–65 years | 36% | 31% | ||
| Education status | With higher education | 65% | 65% | |
| without higher education degree | 35% | 35% | ||
| Monthly household income level (HKD) | Less than 20,000 | 45% | 29% | |
| 20,000–39,999 | 32% | 43% | ||
| 40,000 or over | 23% | 28% | ||
| Employment Status | Housewife | 7% | 12% | |
| Employed | 82% | 74% | ||
| Student | 9% | 13% | ||
| Marital Status | Married | 38% | 35% | |
| Single, widowed, or divorced | 62% | 65% | ||
| Homeownership | Rented | 63% | 56% | |
| Owned | 37% | 44% | ||
| House type | Social housing | 47% | 85% | |
| Private housing | 50% | 15% | ||
| COVID-19 worries | - | Worry about family conflict (Mean (SD)) | 3.23 (1.30) | 2.85 (1.32) |
| Worries about financial hardship and job loss (Mean (SD)) | 7.07 (2.81) | 5.55 (2.62) | ||
| Residence-based perceived COVID-19 risk (Mean (SD)) | 3.37 (0.95) | 2.94 (0.77) | ||
| Mobility-based perceived COVID-19 risk (Mean (SD)) | 2.48 (0.88) | 2.50 (0.90) | ||
| Outcome | - | Depression and anxiety (Mean (SD)) | 13.80 (3.82) | 13.75 (4.11) |
| Stress (Mean (SD)) | 8.30 (1.67) | 8.20 (1.83) |
| Variables | Category | Residence-Based | Mobility-Based | p-Value a |
|---|---|---|---|---|
| Green space | Open Space and Recreational land [Mean (SD)] | 0.10 (0.06) | 0.12 (0.09) | 0.000 *** |
| Greenspace [Mean (SD)] | 0.09 (0.03) | 0.11 (0.07) | 0.000 ** | |
| PM2.5 and noise exposure | PM2.5 (ug/m3) [Mean (SD)] | - | 12.43 (5.57) | - |
| Daytime Noise (dBA) [Mean (SD)] | - | 63.79 (6.60) | 0.000 *** | |
| Nighttime Noise (dBA) [Mean (SD)] | - | 49.15 (6.82) |
| Depression and Anxiety | ||||||
|---|---|---|---|---|---|---|
| Residence-Based | Mobility-Based | |||||
| Variables | Model 1 | Model 2 | Model 3 | Model 4 | Model 5 | Model 6 |
| Coef. (SE.) | Coef. (SE.) | Coef. (SE.) | Coef. (SE.) | Coef. (SE.) | Coef. (SE.) | |
| PCR 1 | 0.12 * (0.07) | 0.13 * (0.06) | 0.15 * (0.07) | 0.22 *** (0.06) | 0.23 *** (0.06) | 0.23 ** (0.07) |
| WFC 2 | 0.11 (0.07) | 0.11 (0.08) | 0.08 (0.08) | 0.10 (0.07) | 0.10 (0.08) | 0.09 (0.08) |
| WFHJL 3 | 0.21 ** (0.07) | 0.21 ** (0.07) | 0.23 ** (0.07) | 0.19 ** (0.07) | 0.20 ** (0.07) | 0.20 ** (0.07) |
| OSRL 4 | 0.05 (0.06) | 0.05 (0.07) | −0.01 (0.06) | 0.01 (0.07) | ||
| Greenspace | −0.04 (0.07) | −0.05 (0.07) | −0.02 (0.06) | −0.03 (0.07) | ||
| PM2.5 | 0.11 * (0.06) | 0.09 (0.06) | ||||
| Daytime Noise | 0.01 (0.07) | 0.01 (0.07) | ||||
| Nighttime Noise | 0.04 (0.07) | 0.04 (0.07) | ||||
| PCR × Greenspace | 0.09 (0.07) | −0.08 (0.06) | ||||
| WFC × Greenspace | 0.02 (0.07) | −0.02 (0.08) | ||||
| WFHJL × Greenspace | −0.07 (0.07) | −0.03 (0.08) | ||||
| PCR × OSRL | 0.02 (0.08) | 0.02 (0.07) | ||||
| WFC × OSRL | −0.04 (0.08) | −0.08 (0.07) | ||||
| WFHJL × OSRL | −0.03 (0.08) | −0.05 (0.07) | ||||
| AIC | 608.4 | 611.6 | 620.6 | 599.3 | 605.6 | 613.4 |
| Adjusted R2 | 0.13 | 0.13 | 0.15 | 0.13 | 0.12 | 0.11 |
| Stress | ||||||
|---|---|---|---|---|---|---|
| Residence-Based | Mobility-Based | |||||
| Variables | Model 7 | Model 8 | Model 9 | Model 10 | Model 11 | Model 12 |
| Coef. (SE.) | Coef. (SE.) | Coef. (SE.) | Coef. (SE.) | Coef. (SE.) | Coef. (SE.) | |
| PCR 1 | 0.08 (0.07) | 0.10 (0.06) | 0.10 (0.07) | 0.18 ** (0.06) | 0.17 ** (0.06) | 0.17 * (0.07) |
| WFC 2 | 0.21 ** (0.07) | 0.21 ** (0.07) | 0.16 * (0.07) | 0.20 ** (0.07) | 0.20 ** (0.07) | 0.21 ** (0.08) |
| WFHJL 3 | 0.14 * (0.07) | 0.15 * (0.07) | 0.18 * (0.07) | 0.13 * (0.07) | 0.14 * (0.07) | 0.13 * (0.08) |
| OSRL 4 | 0.14 * (0.07) | 0.14 (0.08) | 0.15 * (0.07) | 0.15 * (0.07) | ||
| Greenspace | 0.03 (0.07) | 0.01 (0.07) | 0.01 (0.06) | 0.01 (0.07) | ||
| PM2.5 | 0.06 (0.07) | 0.05 (0.06) | ||||
| Daytime Noise | 0.02 (0.07) | 0.02 (0.07) | ||||
| Nighttime Noise | −0.01 (0.06) | −0.01 (0.07) | ||||
| PCR × Greenspace | 0.08 (0.07) | −0.03 (0.08) | ||||
| WFC × Greenspace | 0.13 (0.07) | 0.10 (0.08) | ||||
| WFHJL × Greenspace | −0.08 (0.07) | −0.09 (0.06) | ||||
| PCR × OSRL | 0.13 (0.07) | −0.01 (0.08) | ||||
| WFC × OSRL | 0.01 (0.08) | −0.04 (0.07) | ||||
| WFHJL × OSRL | −0.13 (0.08) | −0.02 (0.07) | ||||
| AIC | 604.7 | 604.3 | 606.2 | 598.3 | 601.9 | 611.5 |
| Adjusted R2 | 0.11 | 0.11 | 0.13 | 0.13 | 0.13 | 0.12 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, J.; Kwan, M.-P.; Tse, L.A.; He, S.Y. How People’s COVID-19 Induced-Worries and Multiple Environmental Exposures Are Associated with Their Depression, Anxiety, and Stress during the Pandemic. Int. J. Environ. Res. Public Health 2023, 20, 6620. https://doi.org/10.3390/ijerph20166620
Huang J, Kwan M-P, Tse LA, He SY. How People’s COVID-19 Induced-Worries and Multiple Environmental Exposures Are Associated with Their Depression, Anxiety, and Stress during the Pandemic. International Journal of Environmental Research and Public Health. 2023; 20(16):6620. https://doi.org/10.3390/ijerph20166620
Chicago/Turabian StyleHuang, Jianwei, Mei-Po Kwan, Lap Ah Tse, and Sylvia Y. He. 2023. "How People’s COVID-19 Induced-Worries and Multiple Environmental Exposures Are Associated with Their Depression, Anxiety, and Stress during the Pandemic" International Journal of Environmental Research and Public Health 20, no. 16: 6620. https://doi.org/10.3390/ijerph20166620