1. Introduction
Fire-related mortality and morbidity represent the third leading causes of residential unintentional injuries globally [
1,
2,
3]. Fires contribute to the global burden of disease, accounting for approximately 9 million injuries, 120,000 deaths, and 7.46 million Disability-Adjusted Life Years (DALYs) lost annually [
2,
4]. These estimates of fire-related fatal and non-fatal injuries may be underrated due to inconsistent and incomplete reporting of incidents, particularly in low- and middle-income countries [
5]. Further to their high casualty rates, fires impose considerable economic loss, including nearly USD 8.6 billion in the US in 2020 [
6]. Similar estimates of fire-related human and economic burdens emerge from Australia and Canada [
7,
8].
Residential fires remain a major health concern, accounting for a high proportion of injuries and deaths globally [
5]. The existing literature has examined several factors associated with residential fires and their health outcomes, particularly those related to population characteristics and residential structures. Risk factors include low socio-economic status, residing in older buildings, male sex, age below 6 years of age or over 64, unemployment, lower levels of education attainment, consuming alcohol, and smoking [
1,
9]. Populations with unique characteristics and vulnerabilities tend to sustain an increased risk of fire-related morbidity and mortality [
10,
11]. Identifying and targeting high-risk groups within a population is critical to developing tailored fire safety messaging and smoke alarm installations, and, consequently, improving public safety behaviors and practices to reduce occurrences of fire incidents [
12].
To mitigate the burden of residential fires, several intervention strategies and best practices have been adopted and implemented globally [
13]. Evidence consistently indicates the relevance of effective community-based fire safety initiatives in curtailing the prevalence of residential fires and related injuries and fatalities [
14,
15,
16,
17]. Interventions, such as home visits, provision of fire safety educational messages, inspections, and installation of smoke alarms, are particularly effective in decreasing the frequency of fire incidents and casualty rates [
14,
18]. Further to the environmental safety modifications, the effectiveness and sustainability of fire prevention programs are strongly influenced by human cognitive and psychological factors. The ‘knowing–doing gap’ (uptake), which refers to the challenge of translating knowledge into effective actions in fire prevention, and the ‘wear-off effect’ (decay), which signifies the decreased effectiveness of interventions over time due to the lack of maintenance, constitute two factors that significantly influence the long-term effect of any implemented safety intervention [
19]. To be mindful of the cycle of uptake and decay requires continuous monitoring and retreating with the intervention when decay or adverse effects are observed. Acknowledging the apparent effect of these factors on the attenuation of gained knowledge is critical and calls for timely refreshment to retain the acquired fire safety behaviors and practices over long time periods.
Inspired by successful fire prevention programs globally [
17], the ‘HomeSafe’ initiative was implemented in the city of Surrey, British Columbia in 2008 with the aim of decreasing the occurrence and impact of residential fires. An initial needs assessment was conducted prior to HomeSafe implementation, which served primarily to identify populations at high risk and to support program prioritization based on population characteristics, including young children, older adults, single parents, and individuals with low socio-economic status. Preliminary data revealed a steady increase in fire rates from 1988 to 2007 (80–88 fires per year per 100,000 population), with the majority being residential fires (75.5%) mainly occurring in single-family dwellings (87.5%) and caused by cooking (39.9%) and open flames (17%) [
20] The assessment further showed the low prevalence of smoke alarm ownership and function, as nearly 36.5% of households had no smoke alarm installed and 49.5% had malfunctioning smoke alarms. Further to fire-related property damages, human suffering was substantial; nearly one in ten residential fires resulted in injuries (9.8%) and fatalities (0.8%). A considerable proportion of the reported injuries (58.2%) and deaths (83.3%) occurred in households that lacked a functioning smoke alarm. The needs assessment provided data-driven evidence to support the implementation of the proposed HomeSafe program. The various approaches and initiatives adopted within the HomeSafe program were inspired by the latest research on socio-economic factors and fire risks [
21].
Initial evaluation results demonstrated positive effects of this program over the first few years [
22]. Building on these findings, the main objective of this study is to provide a summary understanding of the fire prevention initiatives included within the HomeSafe program over 12 years in the city of Surrey, British Columbia. More importantly, this study provides a longitudinal analysis of the effectiveness of various initiatives within the HomeSafe program and evaluates their impacts on reducing the frequency and severity of residential fires and mitigating fire casualties. To achieve these objectives, this study addresses two main research questions: (1) What were the key fire prevention initiatives implemented within the HomeSafe program in the city of Surrey during the study period, and how effective were these initiatives in reducing the frequency and severity of residential fires? (2) What impact did these initiatives have on mitigating fire-related casualties, and what are the implications of the effective outreach and longevity of these initiatives for fire prevention strategies? The implications of the effective HomeSafe outreach initiatives and the longevity of their successful implementations are discussed in this paper, particularly with respect to the importance of ongoing, positive, collegial relationships between firefighters, fire service managers, and city management more broadly.
3. Results
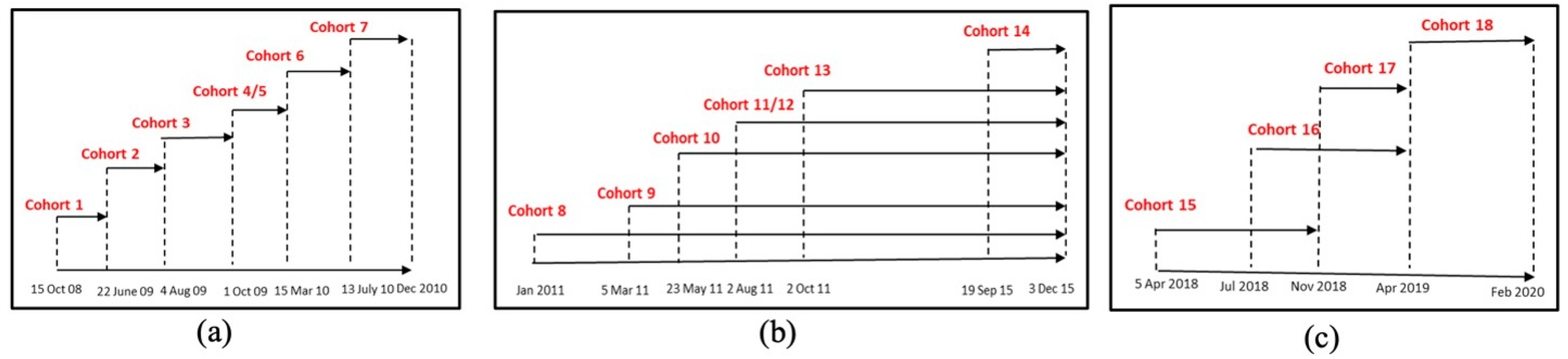
A total of 120,349 households participated in the 12-year period of the HomeSafe program (18,757 in HomeSafe1-HS1, 91,799 in HomeSafe2-HS2, and 9793 in HomeSafe3-HS3,
Figure 3).
The implemented HomeSafe initiatives yielded a substantial increase in functioning smoke alarms and a significant decrease in residential fire occurrences and fatalities. This was achieved through cohort visits conducted by firefighters, inspection and installation of smoke alarms conducted upon request, and validation of smoke alarms by fire crews during incidents. Nonetheless, a reverse pattern was reported in relation to the interventions related to distributing information packages and door-to-door hangers, which failed to show any effectiveness in reducing fire rates.
The HomeSafe1 (HS1) initiative led to a 91% reduction in residential fires, with a 50% reduction still apparent 5 years post-intervention. Among the 91 smoke alarm functioning verifications completed by fire crews at residential fire incidents, only 2.2% had post-visit fires (
Table 1). Pre- and post-visits showed a 64% decrease in fire rates in the intervention group and a 14.6% decrease in the control group.
The HomeSafe2 (HS2) initiative demonstrated a positive impact on reducing residential fire rates by 75% with smoke alarm installations by request, and a reduction of 66% where fire crew smoke alarm verifications took place at incidents. There was an increasing trend in the percentage of functional smoke alarms, 61.5%, at locations where smoke alarms were installed, as well as an increase of 6.1% where crews verified the presence of functioning smoke alarms (
Table 1). In contrast, door hangers and drop-off information packages without the presence of a fire representative did not yield the expected results. A negative impact manifested in a proportional decrease in functional smoke alarms (−46.4% and −16.5%, respectively), and a relative increase in residential fires (+12% and +15%, respectively;
Table 1).
The HomeSafe3 (HS3) initiative revealed a favorable impact on increasing the rate of functioning smoke alarms from 35% to 100% through home visits by volunteers, as well as the proportion of fires confined to the object of origin (67%). Additionally, this initiative successfully reduced fire rates by 33% for smoke alarm installation upon request and by 87% for verification of smoke alarms by the fire crew at incidents (
Table 1).
3.1. Intervention Group Outcomes
Over the period of the HomeSafe1 initiative, intervention groups sustained a residential fire each 97.3 and 193.1 days before and after the intervention, respectively, compared to the control group, which experienced a residential fire every 64.1 and 68.8 days pre- and post-intervention, respectively [
15] (
Table 2).
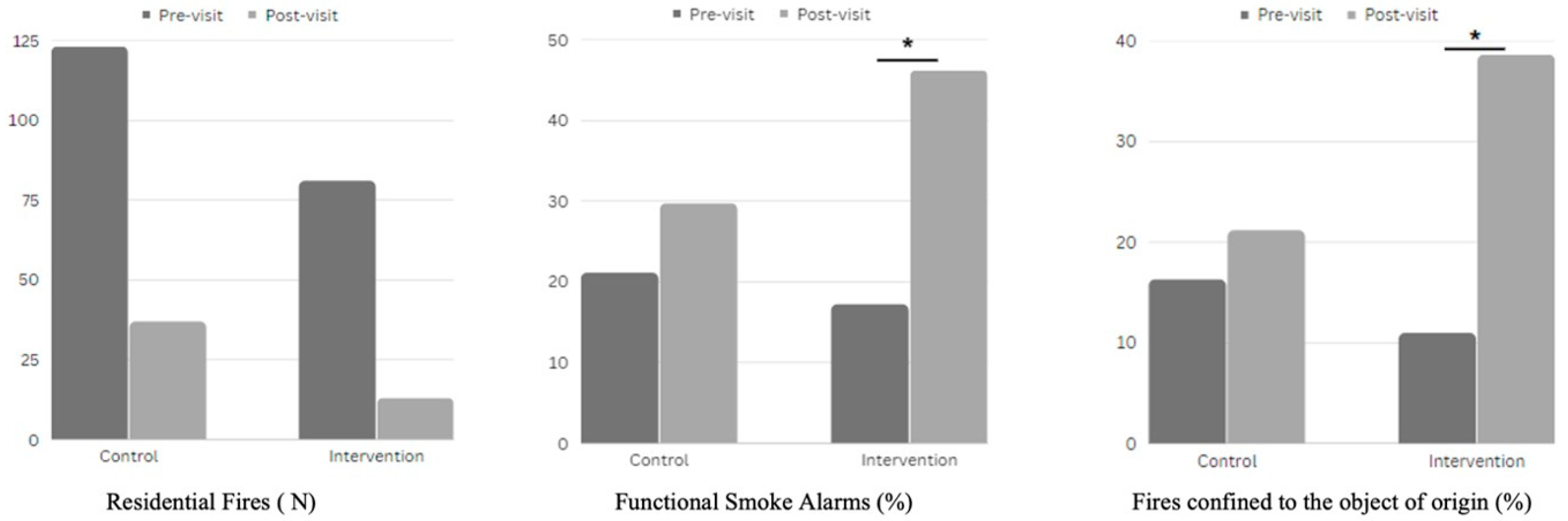
Evaluating the severity of residential fires during HomeSafe1 showed that the proportion of functioning smoke alarms and fires confined to the object of origin significantly increased pre- and post-visit in the intervention group (X
2 (1, N = 94) = 5.57,
p-value < 0.05 and X
2 (1, N = 94) = 6.61,
p-value < 0.02, respectively). The ANOVA demonstrated the impact of in-home visits on the fire rates, resulting in a significant between-group effect F (1, 12) = 8.31, (
p-value < 0.02). Post hoc analysis showed substantial differences in post-intervention fire rates between the intervention and control groups F (1, 12) = 6.56, (
p-value < 0.03) (
Figure 4 and
Table 3).
During HomeSafe2, a 57% decrease in residential fires was reported in the intervention cohorts following the door-to-door visits, in addition to a noticeable rise in the proportion of functional smoke alarms (23%) and residential fires contained within the object of origin (12%) (
Table 4).
During HomeSafe3, the residential fire rate in cohorts 15–18 decreased by 80% to reach 0.31 fires per 1000 occupied properties, while the percentage of functional smoke alarms increased by 183% and the residential fires confined to the object of origin after the visit decreased by 33% (
Table 5).
3.2. City-Wide Outcomes
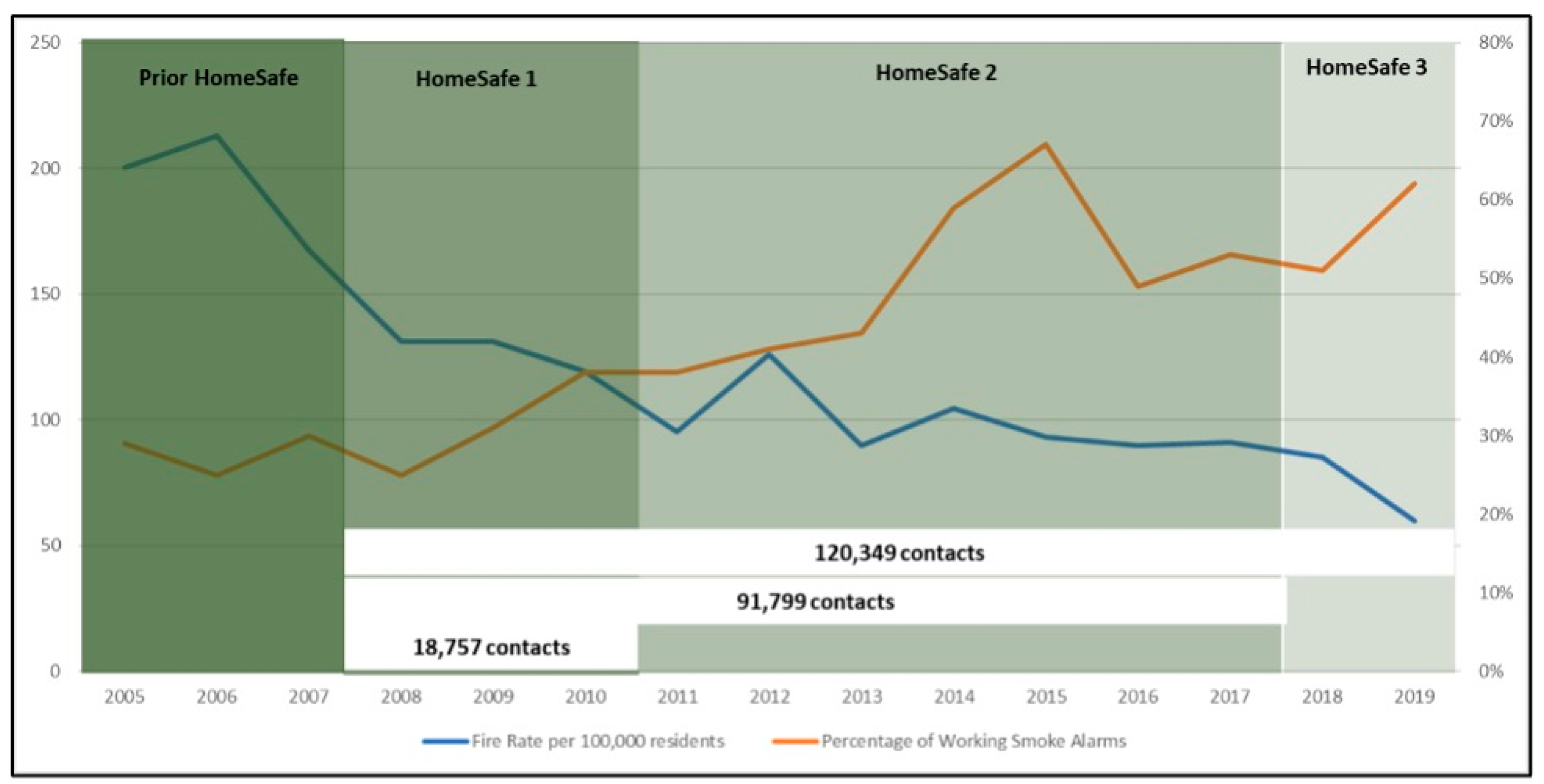
During the initial three years of the HomeSafe1 program, successful city-wide outcomes were illustrated by a 34% reduction in residential fires and a 58% reduction in the fire casualty rate, while the number of residential properties with functional smoke alarms increased by 11% and the number of residential fires contained to the object of origin increased by nearly 54% (
Figure 5).
During HomeSafe2, Surrey City sustained a 22% decrease in residential fires, a 39% increase in functioning smoke alarms (66.75 increase in 2015 alone), a 20% decrease in fires contained within the room of origin, and a 24% increase in the casualty rate (
Table 6).
In the HomeSafe3 period, residential fire rates in the city of Surrey continued to decrease to reach a 26% reduction since HS2 and a 43% reduction since the onset of the HomeSafe1 initiative in 2008. The proportion of functional smoke alarms increased by 130% to reach 56%, with 43% of residential fires contained within the object of origin (
Table 6). The casualty rate increased by 9% on average since the end of HS2. However, by the end of 2019, there was a drop of 0.4 in the number of casualties per 100,000 population (
Table 6).
4. Discussion
This study presents the outcomes of the HomeSafe Program over a period of 12 years and demonstrates the effectiveness of implemented fire interventions in decreasing the occurrence and the impact of residential fires, enhancing fire safety measures, and reducing fire-related injuries and deaths.
Throughout the implementation period, HomeSafe achieved considerable success in decreasing fire rates within the city of Surrey by 80%, increasing the presence of operational smoke alarms in residential homes by 60%, improving fire confinement to the initial source by 94%, and, more importantly, decreasing fire casualties by more than 40%. The study findings confirm that the three most effective HomeSafe initiatives were the household visits conducted by on-duty firefighters, smoke alarm inspections and installations upon request, and the validation of smoke alarms by fire crews during fire incidents.
Despite the overall success of the HomeSafe program, data showed that some initiatives were more effective than others for the measured outcomes. For instance, outreach initiatives, such as information package drop-offs and door hangers, which lack direct personal contact and informational transactions with household residents, have proven to be less effective at ameliorating fire-related outcomes. As for telemarketing outreach, the data set of contact numbers available was somewhat random and not necessarily aligned with the targeted risk criteria. The post-outreach analysis demonstrated the absence of fire incidents reported in the contacted properties pre- or post-implementation of the initiative. Aligning with existing studies, the evidence from this study further demonstrates that door-to-door visits by firefighters or public safety volunteers served to enhance residents’ safety knowledge through interactive and engaging educational information and to ensure functioning fire alarms were installed in targeted households [
24,
25]. This approach was particularly effective in significantly protecting communities against residential fires. Several studies have underscored the importance of engaging with household members through direct face-to-face personal contact and hands-on training for enhancing individuals’ acquisition of safety knowledge and the adoption of fire safety behaviors and practices [
26,
27,
28].
Aligning with the international literature, this study confirms that households with functioning fire alarms reported remarkably low rates of fire-related injuries and deaths [
29]. Installing and maintaining functional smoke alarms at residential properties is one of the prominent residential fire prevention strategies and key to sustainably securing fire safety over time [
28,
30,
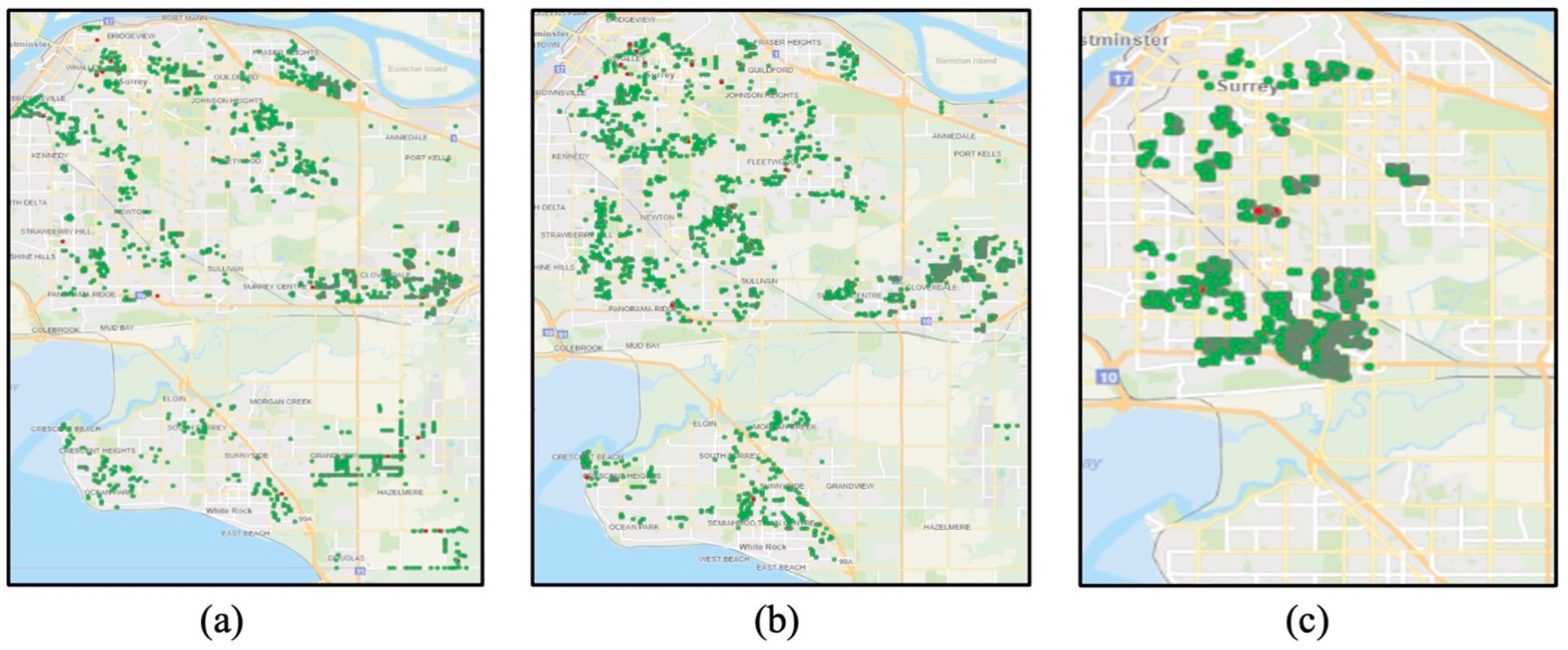
31]. Moreover, this study shows that targeting high-risk households through an initial assessment and mapping using geographic information systems (GIS) [
14,
15,
30,
32] was critical to substantially reducing fire casualties among vulnerable populations. Selected household characteristics tend to increase individuals’ vulnerability to and risk of fires, including households with children aged less than 6 or older adults aged more than 64, single parents, residents who are frequent movers, residents with low income or unemployment status, those residing in older buildings, individuals with disabilities, and immigrants [
33,
34]. Moreover, tailored and culturally sensitive fire safety interventions were shown to effectively reduce fire-related morbidity and mortality, particularly among populations with unique demographic characteristics [
35,
36,
37,
38].
The HomeSafe program offers opportunities for lessons learned and presents a series of recommendations for future fire prevention programs, including:
4.1. Engaging Community and Government
Community engagement and government support are key to enhancing safety and reducing residential fires [
14,
15]. Active commitment from the municipal government to fund and implement fire awareness programs, promote smoke alarm installation, and enforce fire safety measures coupled with fire service support and community engagement with fire prevention programs represent a vital step toward a safer community.
4.2. Focusing on Successful Initiatives
As demonstrated in this study, variation in the success of the HomeSafe initiatives was clearly highlighted. Door visits conducted by firefighters, smoke alarm inspection and installation upon request, as well as fire crew validation of smoke alarms at fire incidents were proven effective in raising awareness about fire safety, advising on potential hazards at home, and, consequently, reducing the occurrence and severity of fires. However, initiatives that lacked social interaction opportunities, such as personal contact and dialogue with recipients, were less successful. It is critical to identify which initiative has the potential to succeed and to invest efforts into its proper implementation.
4.3. Targeting High-Risk Populations
To ensure an effective fire safety program, the intervention should target high-risk populations and should regularly update and map the higher-risk neighborhoods (
Figures S1 and S2). This approach will increase the likelihood that the program is directed toward the targeted population. Hence, it is critical that the intervention program is supported by a comprehensive data repository of updated population demographics and information related to city planning and development to ensure constant monitoring. As the fire safety program evolves, it is important to continuously assess population characteristics within cities and identify high-risk residents to ensure successful and sustainable interventions.
4.4. Conducting Longitudinal Assessment of Implemented Initiative
Ongoing monitoring and evaluation of the fire interventions are crucial to ensure the long-term success of the initiative [
14]. To maintain the sustainability of the fire intervention, a longitudinal and evidence-based assessment, followed by re-assessment, is needed to ensure the detection of any changes in the progression of the implemented initiatives and measures and adapt accordingly.
4.5. Ensuring Sustainability and Long-Term Programs
Implementing a large-scale program that aims to reach a sizeable proportion of the targeted population can lead to a sustainable decrease in fire-related injury and death rates over decades.
To enhance program sustainability, it is important to tailor the intervention based on new protocols associated with any surging pandemic and to address the challenge of maintaining effective program operation while prioritizing the health and safety of crews, volunteers, and residents. Future fire intervention programs should take into consideration the ‘knowing–doing gap’ and the ‘wear-off’ effect [
19] to ensure the long-term impact of the intervention program on enhancing individuals’ knowledge and practicing safety behavior over time. The sustainability and ongoing effectiveness of this work would also not have been possible without the commitment shown from city management, fire service management, the firefighter union, the firefighters, and a range of other service providers throughout the municipality. The program’s success was not an accident. It depended on participation from key stakeholders with a shared vision for safety. Continuing to implement evidence-based fire prevention across changes in leadership at the city level, fire service level, and union level is a success in its own right. The results of this success are clearly demonstrated in the longitudinal reductions in fire loss and casualty documented through this paper.
4.6. Highlighting the Importance of Management
One of the major contributing factors to the success of the HomeSafe program is the adoption of a systematic and coherent approach for conducting fire safety campaigns as well as validation and installation of smoke alarms. This approach has shown positive impacts on the visited properties and the entire city. The success of the program reinforces existing research and emphasizes the significance of evidence-based, systematic, and continuing dissemination of fire safety information to residences together with smoke alarm testing and installation services. The mutual benefits of reducing community residential fires and improving firefighters’ jobs with less exposure to fires, the produced smoke’s toxic chemicals, and the associated risk of contracting occupational-related cancers led to more sustainable and consistently monitored fire safety initiatives across the community over time.
4.7. Benchmarking and Informing Evidence-Based Policies
Synthesized findings from the HomeSafe program can be adopted by policy makers and key stakeholders to inform evidence-based safety regulations and data-driven decisions on resource allocation and fire safety program implementation. Further to supporting policy makers’ decisions, findings from the HomeSafe program can be adopted to benchmark the effectiveness of various fire prevention programs in other regions and to use HomeSafe as a model program to evaluate existing programs and refine and make changes to improve outcomes.
The long-term, sustained commitment to the program across the Surrey Fire Service is exceptional. The mutual understanding between fire management and firefighters has led to a cultural shift of incorporating the activities of HomeSafe into regular daily duties. By verifying a working smoke alarm at every residential opportunity, the program becomes sustainable on an ongoing basis. One of the distinguishing features of this program can be explained by the literature on government innovation. While the definition of innovation remains contested [
39], this program certainly qualifies as being innovative in any practical sense.
Using a framework of key factors for innovation, it is apparent that this success was due to several organizational, managerial, and cultural conditions. In
Table 7, we account for these factors and explain their importance to the efforts. This framework may offer some explanatory insights into the underlying components of this program’s success.
This study has some strengths and limitations. The systematic and consistent approach adopted to implement the fire intervention represents the major strength of this study. The longitudinal aspect of the HomeSafe initiative, with the fire safety campaigns and smoke alarm testing and installations, constitutes a key strength of the HomeSafe program. This study faces a few challenges and incurs some limitations. One of the main limitations of the HomeSafe initiative is the ability to map neighborhoods that align with the profile of the targeted population while taking into consideration the dynamic environment of the city based on its organization, development, and residents’ socio-economic status. The lack of recent and updated population demographic data hindered the precise identification of high-risk areas for HomeSafe targeting. However, a possible solution for properly identifying high-risk areas would be the implementation of a nearly real-time monitoring system for each initiative and merging it with an up-to-date database of population demographics, as well as city organization and development. Additionally, within each HomeSafe initiative, residents’ demographic data could be collected whenever social interaction with residents is possible. This would further enhance the overall data collection process. Another limitation refers to the spread of the coronavirus pandemic in 2019, which coincided with the implementation of HomeSafe3.
This posed a new challenge in maintaining the effective operation of the HomeSafe program without risking the health and safety of residents, fire crews, and community volunteers. Restricted social interaction among residents hindered the promotion of fire safety campaigns for at-risk residents. Existing fire initiatives should adapt to and accommodate the spreading of the pandemic while aligning with protocols and measures for the well-being of individuals. Nonetheless, these obstacles created opportunities for program enhancements that can be explored in future work. Finally, the effectiveness and outcomes of the tax lineup and Surrey Food Bank initiatives were impeded by the challenges encountered in collecting property information during these events.

 ,
, 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}




