1. Introduction
The novel coronavirus disease 2019 (COVID-19) pandemic has exposed people to significant and prolonged stress [
1,
2]. The myriad of primary stressors includes personal and familial health consequences of infection, together with social and financial impacts of the ongoing public health restrictions, e.g., lockdowns, social distancing requirements, travel bans, and vaccination mandates. These psychosocial impacts were amplified by uncertainty relating to new variants of COVID-19, the limited effectiveness of public health restrictions, and political responses. What was happening amid increased societal divisions and polarisation around vaccination and mask mandates, and associated additional stresses (e.g., people losing jobs, verbal abuse of vaccinators, and staff checking vaccination passports) [
3]. Those restrictions have largely been removed, although uncertainty about future variants remains.
No one is exempt from exposure to pandemic-related stressors but some segments of society (e.g., health workers, law enforcement, providers of essential goods/services, and at-risk populations) are more vulnerable to these stressors than others [
4]. Some of the psychosocial impacts of COVID-19 were anticipated from the start of the pandemic [
5]; however, the fluid nature of the pandemic globally, both within and across contexts and the varied responses, has made the assessment and cross-cultural comparison of the psychosocial impacts of COVID-19 extremely challenging.
Different approaches have been utilized to examine the psychological and social impacts of the COVID-19 pandemic. These include employing cross-sectional [
6,
7,
8,
9,
10,
11,
12] and longitudinal [
13] study designs with a representative [
6,
7,
8] and convenience samples [
9] of the general population, those in specific work roles (especially healthcare) [
10,
11], or those having a previous history of mental disorders [
12,
13]. Most studies have employed standardized self-report measures of wellbeing, psychological distress, depression, anxiety, and post-traumatic stress disorder (PTSD). These studies have generally reported negative psychosocial impacts, for example, psychological distress [
8,
14], alcohol abuse [
14], family harm [
8], and suicidality [
8,
14,
15]. Some studies have used standardised instruments across countries to obtain comparable data sets [
6,
7,
10]. Although the use of pre-existing standardised measures also allows for pre-pandemic comparisons, these measures do not specifically examine the impacts of COVID-related stressors.
As a result, there have been recommendations for novel self-report measures to be used alongside established psychometric measures [
16,
17]. Several scales have been developed to this end, which vary in focus and length. These include those assessing the impacts of the COVID-19 pandemic and public health restrictions on physical health, employment and finances, family and social disruption; and measures of psychological distress, loneliness, anxiety, depression, and PTSD (see [
17] for a summary of these measures). While few scales attempt to capture the psychosocial impacts of the COVID-19 pandemic (for example, CRISIS assesses COVID stress on key domains namely COVID exposure, COVID worries, life changes, mood states, daily behaviors) [
18], they frequently reflect the context and country in which they were developed, limiting their more general applicability. Other scales have a more specific focus rather than assessing the wider impacts of the pandemic (for example, the Fear of COVID-19 scale [
19], the Coronavirus Anxiety Scale [
20], and the COVID-19 Anxiety Scale [
21]). With the exception of the Fear of COVID-19 scale, most of these novel scales lack detailed validation studies.
Importantly, the potential positive impacts of the pandemic were also recognised [
22] but very few empirical studies have been undertaken to examine the positive psychosocial impacts of the pandemic. Jenkins et al. [
23] and Beaglehole et al. [
24] reported data from a demographically representative sample of New Zealanders. Jenkins et al. described the experience of the silver linings (positive impacts) resulting from the COVID-19 pandemic and reported positive impacts in two-thirds of their sample. They also reported two overarching themes of positive psychosocial impacts, including surviving (coping well, meeting basic needs, and maintaining health) and thriving (self-development, reflection, and growth) [
23]. Beaglehole et al. examined lockdown experiences, wellbeing, and key sociodemographic determinants; and reported excellent wellbeing in 9% of their sample during the lockdown. They emphasised the need to assess a positive wellbeing to gain a comprehensive understanding of the psychosocial impacts of the COVID-19 pandemic [
24].
The COVID Psychosocial Impacts Scale (CPIS) was therefore developed to address some of the issues identified above. The CPIS was developed by academics and practitioners in the field of psychology, psychiatry, epidemiology, and public health in the very early stages of the pandemic in New Zealand when we had a strict lockdown and very few cases. This situation did not change substantively until early 2022 when the Omicron variants arrived with higher infection rates, despite a high vaccination rate. We aimed to develop a measure for use in adults (18 years and above) that comprehensively assessed the impacts of the COVID-19 pandemic, including the adverse personal, social, and economic consequences that followed and recognised the positive outcomes which may have occurred. Ideally, the items must be derived based on prior research. However, it was the first historical occurrence of a widespread novel virus during a period in history where we have in place the tools to try to understand the stress caused by it. Notably, at the time of designing the CPIS, there were no established measures for assessing COVID-related stresses. As a consequence, we used an empirically driven approach to item and scale construction informed by our experience of developing a nuanced model for measuring exposure to the Canterbury earthquakes [
25,
26], in which the domains were modelled on a modified version of the Social Readjustment Scale [
27]. In this approach, participants are asked to indicate the life event they have experienced and subsequently report the resultant level of stress owing to that life event. This approach allows us to work out the relative “weights” of different types of stresses and also shows combined stress load. Importantly, the relevant literature [
4,
5,
6,
8,
10,
11,
12,
13,
16,
17] and existing pandemic scales [
18,
19,
20,
21] were consulted in the process of scale construction. The CPIS applicability for use in a range of countries and cultures was also considered in the scale development.
There were three steps to scale construction, namely item development (identification of domain, item generation, content validity); scale development (pre-testing of items, survey administration, item reduction, extraction of factors); and scale evaluation (reliability, construct validity) [
28]. The items were empirically derived from clinical experience in which participants were asked to indicate the resultant level of stress to a pandemic-related life event. Notably, the existing pandemic-related scale that examined the psychosocial impacts [
18] was consulted in the process of item generation and identification of domains. Questions examining the positive consequences of the COVID-19 pandemic were also included. The CPIS was refined using the ‘group mind’ process [
29], which asks colleagues including researchers based on personal contacts from a range of countries and cultures (Bangladesh, Ghana, and Pakistan) to review and rigorously critique a draft of the questionnaire, with iterative improvements made based on their comments. These specific low- and middle-income countries faced the substantial burden of COVID-19 (unlike New Zealand) and also vary in socio-economic context to New Zealand where the CPIS was developed. Collectively, this provided sufficient context to design a widely applicable measure. This was done to ensure content validity and applicability of newly developed CPIS in varying contexts.
In the scale development phase, we pre-tested the revised questionnaire on a small sample of the general public and further modified it to address respondents’ feedback. The CPIS was then administered to a non-representative New Zealand population at two distinct time points (2020, 2022) using an online survey to examine the psychometric properties of the newly developed scale. This paper reports on the item reduction, reliability analysis, factor extraction, and construct validity of the newly developed CPIS and its comparison with standardized self-report measures of psychological distress (Kessler Psychological Distress Scale, K10) [
30] and wellbeing (World Health Organization Well-Being Index, WHO-5) [
31]. Importantly, the psychometric study was carried out in New Zealand at two distinct time points to capture different exposures to the pandemic in the New Zealand population: (1) in 2020 (survey 1) when the pandemic was well-controlled and there was no reported community transmission of COVID-19; and (2) in 2022 (survey 2) when approximately 35% of the population had had a reported confirmed case of COVID-19 and nearly 2800 deaths had resulted [
32]. At the time of both surveys, there was no lockdown in place across New Zealand, but the conditions on the ground changed considerably from successfully suppressing COVID-19 for two years to a reduced restriction due to a high vaccination rate, followed by an infection increase in 2022. The same set of items has been used in both surveys, except three items that were modified owing to psychometric and pragmatic considerations reflecting the process of constant improvement (for details see
Table 1 and
Section 3.1). This is the first part of the program of work and further work will examine its psychometric properties for cross-cultural use after the data acquisition is complete.
4. Discussion
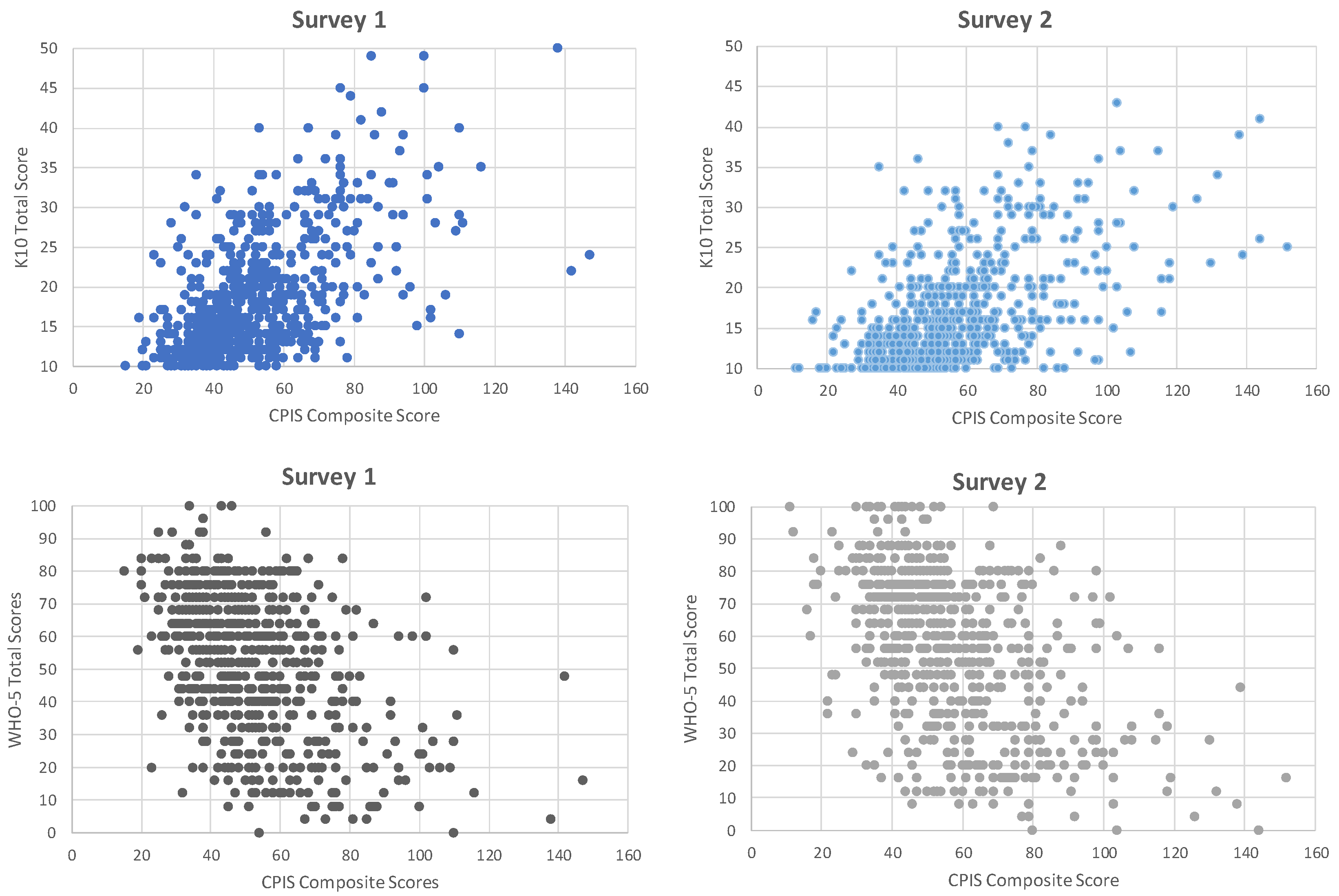
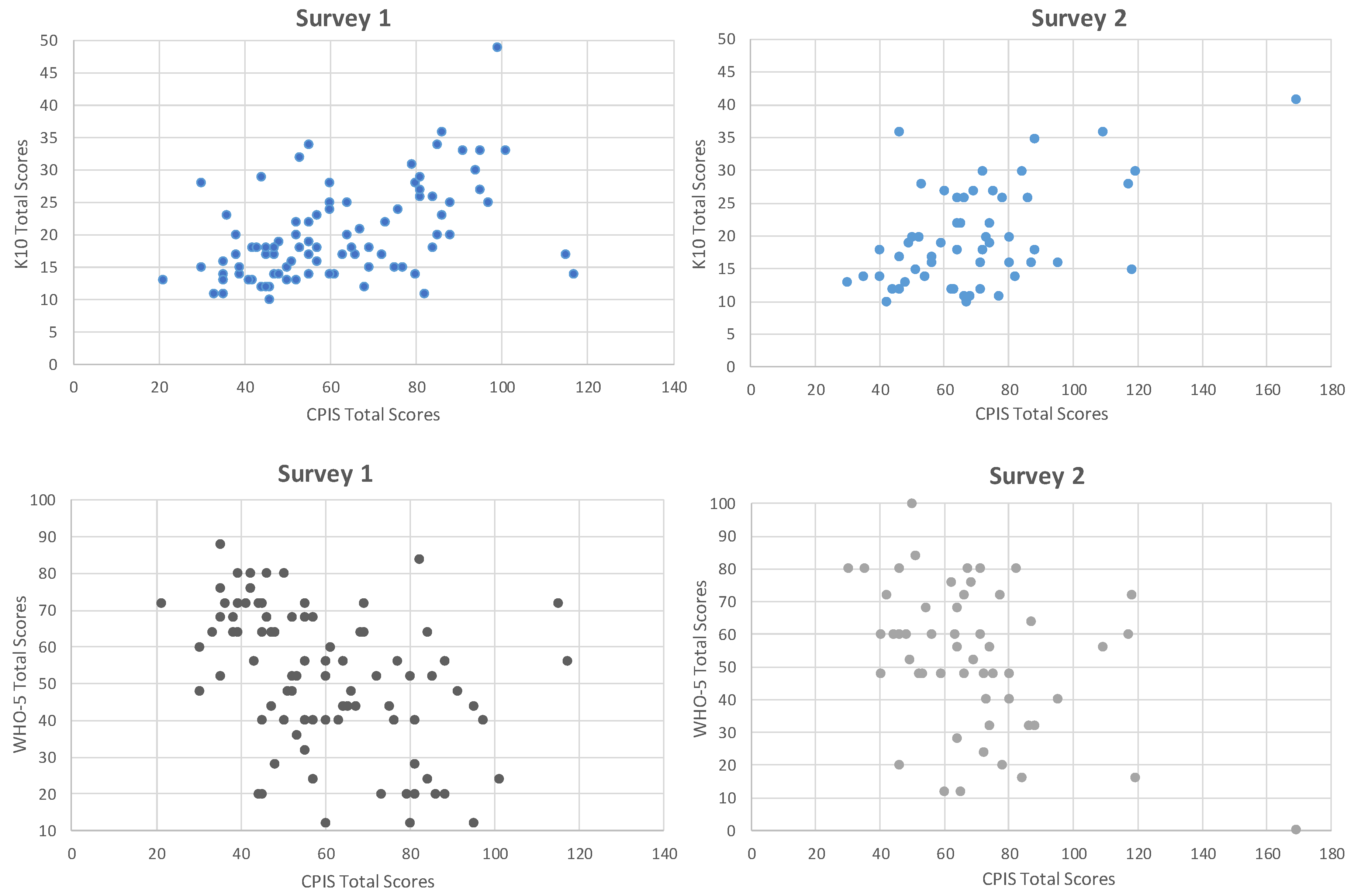
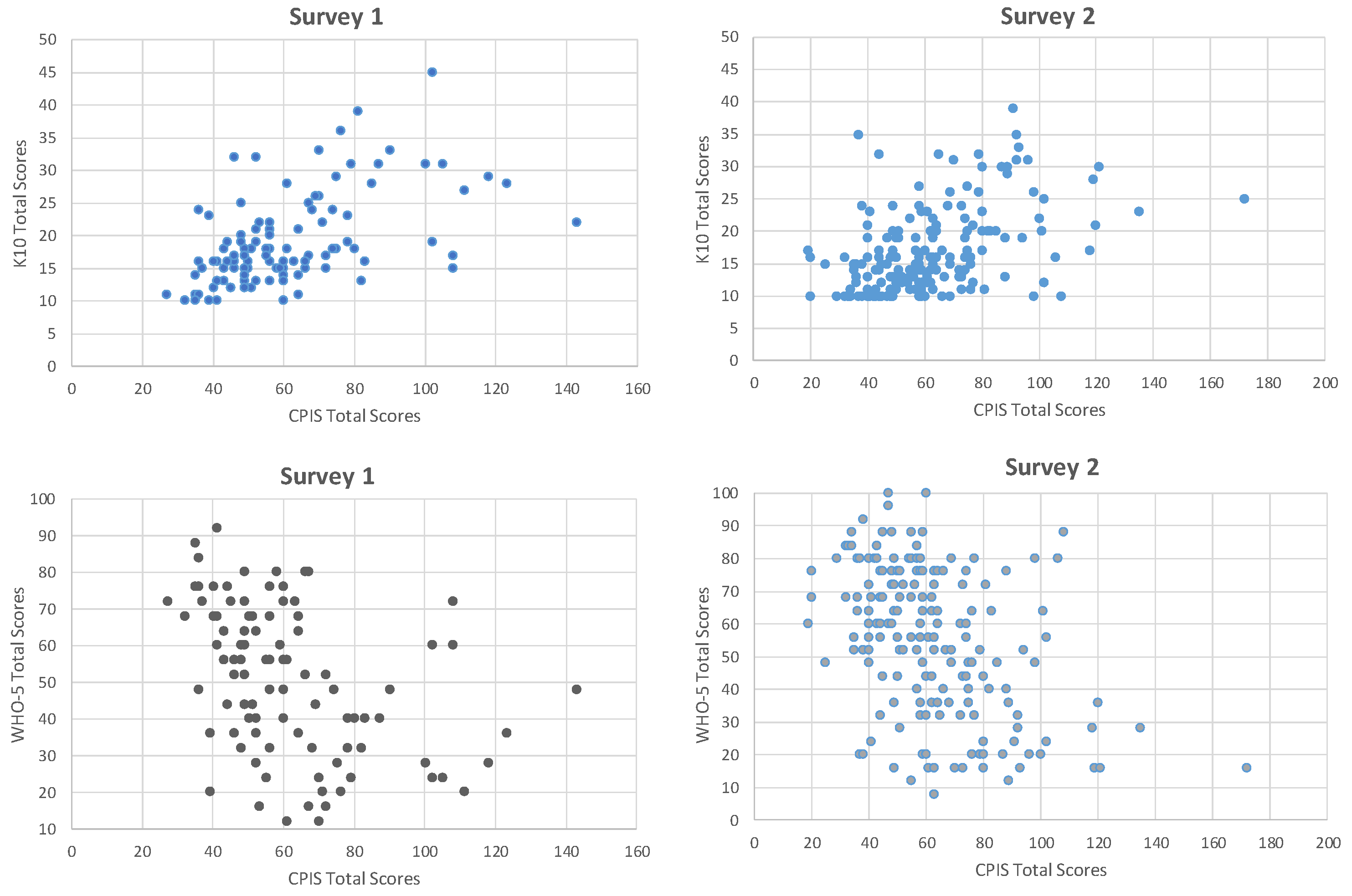
This study reports the findings of the psychometric study carried out to validate the newly developed CPIS that comprehensively assessed the impacts of the COVID-19 pandemic including the adverse personal, social, and economic consequences that followed along with the positive outcomes which may have occurred. Data were obtained in 2020 and 2022 to capture different exposures to the COVID-19 pandemic from a non-representative New Zealand sample. The main findings of this psychometric study were of a unidimensional structure within the CPIS subscales and inter-relatedness among CPIS stress-related subscales. Results showed CPIS to have a moderate negative correlation with K10 and a moderate positive correlation with WHO-5, reflecting construct validity.
Previously, Every-Palmer and colleagues examined psychological distress and wellbeing using the K10 and WHO-5 during New Zealand’s first lockdown in April 2020 in a demographically representative sample and reported moderate stress in thirty percent and low levels of wellbeing in forty percent of their participants [
8]. Although the findings of Every-Palmer and colleagues are not directly comparable, due to different sampling strategies, but collectively both studies indicate a significant increase in the level of distress compared to previous population surveys [
39,
40], reflecting the overall impacts of the COVID-19 pandemic. Similar findings of increased psychological distress have been reported by researchers in the US [
41], Europe [
42,
43], and Asia [
44] (see also [
7]). Although the use of pre-existing standardised measures allows pre-pandemic comparisons, these measures do not specifically examine the impacts of COVID-related stressors. Hence, we recommend using pandemic-related measures in conjunction with established psychometric measures to provide further depth to the interpretation of the findings.
Importantly, this study offered a unique opportunity to conduct the survey at various exposures of the COVID-19 pandemic in New Zealand and highlighted the impacts of the fluid nature of the pandemic on the findings. For survey 1, we reported mild-to-moderate levels of pandemic-related stress on CPIS amongst our sample when there was a low prevalence and no community transmission of COVID-19 in New Zealand. In survey 2, an overall increase in scores on CPIS and its subscales (personal stress, social stress, perception of overall life stress pre/post COVID-19, positive impacts) suggests that CPIS was sensitive to change in pandemic exposure. Interestingly, the participants who took part in both surveys also showed a similar trend. This may be due to a gradual recovery from the economic problems related to lockdowns and the country being closed.
Our findings suggest that the reliability and validity scores varied across time points. We attributed this to the various pandemic exposures and situational factors. Some of the items that were not reliable at the time of survey 1 showed acceptable reliability scores at the time of survey 2. These included item 2 (“Have you had a COVID test?”) and item 6 (“Do you feel any family member is at risk of being exposed to someone with COVID-19 through their work?”). In contrast, some of the items were reliable at the time of survey 1 but did not show acceptable reliability scores at the time of survey 2. This includes item 28 (“Has your household needed to seek help from a food bank or other charitable organisation?”). We argue that this is an issue of a floor effect rather than a reliability effect. Floor and ceiling effects are likely to affect some items in periods of relatively low and relatively high prevalence, but importantly no sustained floor or ceiling effects were observed over the two periods. We, therefore, argue that the reliability and validity of the CPIS were reasonably stable even though there was a difference in the levels of COVID-related stresses and morbidity between the two administrations of the questionnaire.
We also acknowledge some key contextual factors surrounding CPIS development. The experience of the pandemic in New Zealand was different compared to many other jurisdictions due to the presence of strong temporary laws that were in place to prevent the transmission of the virus. For instance, the “essential worker” category was a legal entity that permitted working outside of the home for certain designated professions during the lockdown in New Zealand, under the strict restrictions and measures in place. This was a heterogenous group (e.g., those working in healthcare, law enforcement, emergency services, or providers of essential goods/services such as those working in supermarkets or transport) in regard to income levels and risk of exposure to possible COVID-19 infection. In both surveys, a substantial percentage of participants and their families were essential workers (see
Appendix A), but items 12 and 13 assessing stress owing to being an essential worker or having a family or friend as an essential worker showed poor item-total correlations by including as part of the financial stress subscale. These low-item-total correlations could be attributed to the timing of data collection as both surveys were administered when there was no lockdown in place in New Zealand. Hence, being an essential worker did not appear to contribute to stress as these items did not show much variability in the true scores, resulting in low-item-total correlations. Considering the current COVID-19 scenario, we argue that these items will be less important in future iterations of CPIS, and hence these items would likely be reconsidered as demographic items.
In addition, in 2020 (at the time of survey 1), the item “Have you had a COVID test?” had a ‘leaf’ question “If Yes, was the result positive?” At that time there was a low prevalence of COVID-19 in New Zealand and no evidence of community transfer. Although one-third of the participants had a COVID-19 test (only polymerase chain reaction tests were available), only one participant had been diagnosed with COVID-19. In 2022 (at the time of survey 2), there were reduced COVID restrictions owing to high vaccination rates; with Omicron, the infection rates have increased to 35% or more of the New Zealand population. Since now most people have had a COVID diagnosis, having a positive test will not be particularly discriminative. Therefore, we have modified those two items to “Have you ever been suspected of having COVID-19?” and “If yes, have you had a COVID test?” to capture stress owing to being a suspect of getting COVID-19 and stress of having a COVID test. In survey 1, other items also showed low-item-total correlations. These items were retained in the follow-up survey pragmatically and our findings from survey 2 affirm that those items showed acceptable reliability scores when the prevalence of COVID-19 changed considerably. In short, our team considered both psychometric and pragmatic considerations in designing the items of CPIS to reflect the fluid situation on the ground.
In recognition of the positive impacts of COVID-19 [
22,
23,
24], we added four items assessing the sense of the meaning to life. On reflection, these items appear limited in their assessment of this area. We are considering removing these items in future iterations of the CPIS to balance the question types and to reduce the response burden. This area can be assessed by a standardised scale such as the Post-traumatic Growth Inventory [
45] to examine whether a person has undergone a positive transformation after a traumatic event, such as COVID-19. In addition, there were twelve opposite items in three domains (relationships, changes to daily routines and behaviours, changes to faith-related activities) of CPIS assessing the same idea but one from a positive, and the other from a negative direction. These items were added to conceptualize any change in these domains as being a stressor, whether it is positive or negative. Either of these pairs of items could be considered ‘stressful’, however, it is unlikely that participants would endorse both items, rather they would be more likely to endorse one, but not the other. Although these items were not highly correlated warranting item-response bias [
46], we are considering removing them to reduce the response burden in future iterations of CPIS and to capture negative aspects of functioning in these domains alone by assessing conceptually similar items to shed light on the same underlying construct. The CPIS included two optional subscales assessing the stress owing to changes to education-related and faith-related activities in response to COVID-19. This paper demonstrates how to use CPIS with and without these subscales. Future researchers can consider taking out optional subscales depending on their research interests. Lastly, there can be other pandemic-related life events that can be stressful (such as stress owing to vaccination mandates, travel bans, etc.) or other positive life changes due to the pandemic (such as adopting a healthier lifestyle or improving financial status) which could be added in the future iterations of CPIS, if applicable to the pandemic context.
This study has the following strengths. The CPIS was developed using the same “participant researcher” approach applied to understanding the psychosocial impacts of the Canterbury earthquakes [
25,
26,
34,
35]. This approach assesses exposure to the immediate impacts of the disaster and the adverse personal, social, and economic consequences that follow. We believe that the use of pandemic-specific impact scales is required to identify specific impacts of COVID-related stressors, and this cannot be achieved by established measures alone. The CPIS offers some unique advantages over other available pandemic-related scales, including an assessment of both negative and positive impacts. The CPIS can also be used in the general population and targeted groups, such as healthcare workers, essential workers, and other at-risk groups. We have also demonstrated its use in different pandemic-related contexts.
This study has the following limitations. The main limitations include data collection from a non-representative New Zealand sample representing literate or high-income individuals. Since the psychological effects of COVID-19 were widely anticipated, it would be ideal to have a representative sample. The survey was delivered online, and evidence suggests that people living with disabilities (including mental illness) are less likely to participate in online surveys [
47]. It would be interesting to explore the association between socio-demographic and study variables using regression analysis to pool predictor variables. This was not done to keep the emphasis on reporting the scale’s psychometric characteristics. Future analyses of this or an expanded data set using a regression analysis would be useful.
Lastly, the COVID-19 mortality rate—even at its peak in New Zealand—was considerably lower than in many other countries. For instance, as of 3 March 2023, the USA’s total COVID-19 attributable death rate per 100,000 was estimated at 335.09, some 6.4 times higher than New Zealand’s rate of 52.71 [
48]. This may affect the external validity and/or psychometric properties—especially in countries with considerably higher morbitiy and mortality rates. Although the CPIS was developed to be cross-culturally applicable, it has not yet been trialed in different cultures/countries—but consultation and co-design were used to fit it for such use. Further studies are underway in which a brief 32-item CPIS will be used in combination with other standardised measures of wellbeing (WHO-5), distress (K10, PTSD Checklist for DSM-5 [
49]), and post-traumatic growth (PTGI) in several countries [
50]. To achieve this, the CPIS and other measures were translated using parallel back-to-back translations by a team of proficient bilingual academics and researchers who were familiar with the content and context [
51]. This follow-up study (Clinical Trials Registry (NCT05052333)) has the potential to contribute to an increased understanding of the psychosocial impacts of the COVID-19 pandemic and, importantly, to the development of psychosocial measures that allow cross-cultural comparisons.
The COVID-19 pandemic has had a profound impact on the world, causing widespread illness, death, and disruption to daily life. The fear and uncertainty surrounding the virus, coupled with social isolation and financial insecurity, have contributed to increased rates of depression, anxiety, and other mental health issues. With vaccines now widely available, and case numbers decreasing in many parts of the world, it may seem that the worst of the pandemic is over. However, measures taken to examine the psychosocial impacts of the pandemic should not be disregarded as new mutations of the virus could potentially lead to another global crisis. It is important to continue exploring and addressing the psychosocial impacts of the current pandemic as it evolves by adapting pandemic-related scales if necessary in future waves, as well as making efforts to improve preparedness for potential future pandemics.


 ,
, 
{kind=link}
{kind=link}
{kind=link}


