
Influence of Provider and Leader Perspectives about Concurrent Tobacco-Use Care during Substance-Use Treatment on Their Tobacco Intervention Provision with Clients: A Mixed-Methods Study
 , , , ,
, , , , 
Abstract
:1. Introduction
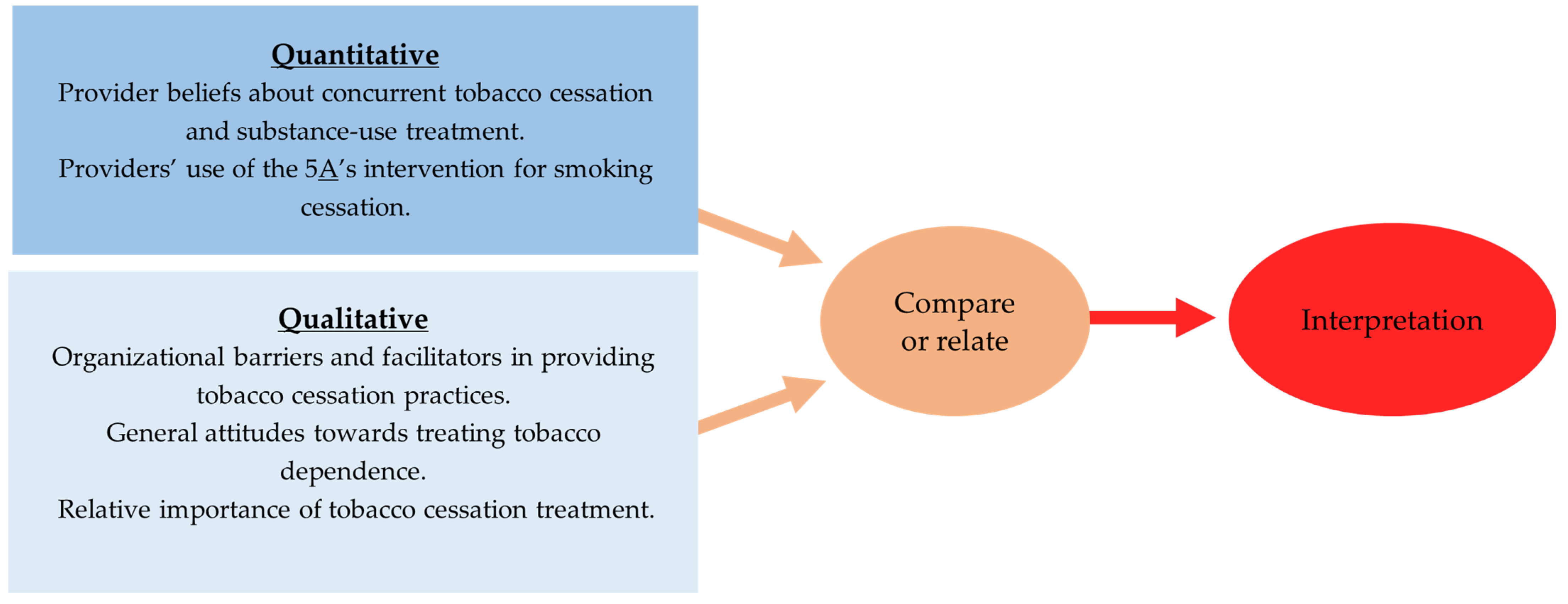
2. Materials and Methods
2.1. Study Design
2.2. Procedures and Participants
2.3. Quantitative Measures
2.3.1. Healthcare Center Characteristics
2.3.2. Providers’ Beliefs about Concurrent Tobacco Cessation and Substance-Use Treatment
2.3.3. Providers’ Use of the 5A’s Intervention for Smoking Cessation
2.4. Qualitative Procedures
2.5. Data Analysis
3. Results
3.1. Quantitative Results
3.1.1. Healthcare Center Characteristics and Provider Information
3.1.2. Logistic Regression Analyses
3.2. Qualitative Findings
3.2.1. Misconceptions about the Concurrent Treatment of Smoking/Tobacco and Substance Use: Smoking Reduces Stress and Is a Valuable Coping Mechanism
I think a lot of our staff though, especially the ones who are tobacco users, they tend to approach tobacco use in conjunction with substance use as an issue of harm reduction. So, if somebody is trying to quit using one substance, they try to make the argument that you shouldn’t be trying to quit using tobacco at the same time because it’s stressful. We’ve tried to train our staff to understand that’s a misconception and the research does not back that up.(Lisa, direct service provider, Director of Operations)
The clients, they’re dealing with enough as it is. They’re dealing with a lot as far as addiction. You know, they’re trying to get off of drugs and alcohol. That’s hard enough as it is, let alone trying to quit smoking. That’s their vice. I mean, I understand that. If we had a smoke-free environment, I probably wouldn’t have a job. [Laughter] You know, I teach the smoking cessation programs.(Martha, direct service provider, Quality Mental Health Professional, Tobacco Treatment Specialist)
I think more training is needed. I also think there’s a stigma there where mental health clients, they’re smoking and it calms them down and it’s just happened a lot, especially with the higher levels of care where our staff—I’ve heard some staff say, “They need to smoke. They need to smoke because if not, they get anxious. Keep on giving them cigarettes.”… There’s that connection with addiction and also just giving in to that behavior and not working with the client. I think that’s something that’s a part of our culture—at least in the area that could change, not really just being okay with it—I think it’s something that we can improve on. I’m talking about the community in general.(Robert, direct service provider, Licensed Professional Counselor/Chemical Dependency Counselor)
3.2.2. “Blame the Victim” Mentality: Clients Are Not Interested in Quitting Smoking Tobacco
They [clients] really don’t want to quit, and there’s really nothing to tie the action to in terms of a reward for a lot of them. So, they don’t see the benefits, or they don’t care about improving their health. That’s not what they’re focused on. So, if there’s no reward like in terms of an incentive or a financial reward, they don’t follow through.(Edith, Director of Behavioral Health Care Services)
The barrier [to providing tobacco cessation] would be the clients not really being interested in stopping the use of tobacco, being more focused on their other substances or the clinicians and the case managers and peer coaches making sure that they find time to include that as part of somebody’s recovery plan or treatment plan.(Lisa, direct service provider, Director of Operations)
[Tobacco cessation] is client-directed, client-driven, client-volunteered…The counselors, the education process, the group processing, we talk about it, but we leave it totally up to the client to ask direction as to whether or not they want to try that…. Probably effort on my part and making it less of a client-driven opportunity; more of a staff-driven opportunity [would facilitate tobacco cessation treatment provision]. We can do better in terms of more than just “Here it is if you want it.” It’s more of a “Here’s an opportunity. Let’s show you how this would work.”(Frank, direct service provider, Executive Director)
3.2.3. Attitudes towards Smoking/Tobacco Cessation
- i.
- Devaluing smoking tobacco as a serious addiction
There is sort of this mentality here, “Let’s take care of the most serious addiction first and let’s talk about the other pieces of your addiction as you go along.” We try to deal with one addiction at a time.(Frank, direct service provider, Executive Director)
It’s [tobacco screening] just included in the substance use history. It’s really just asking “What type of tobacco product or nicotine product do you use, what was your age of first use, how much you currently use and do you have any abstinence history?” That’s about it… I certainly have already thought about talking to our vice president, our clinical person about adding a piece there. Now, it would have to be very, very brief but at least we could just ask if they are interested in stopping [tobacco use].(Jane, direct service provider, Director of Step One Services)
- ii.
- Clients were overwhelmed by multiple social disadvanatges and did not have the capacity to quit smoking tobacco
I think that the biggest barrier is that folks that we serve have so many other major issues. When you don’t have a job or you don’t have appropriate housing or you don’t have food to feed your family or any of those things….Yes, you can argue, “Well, if you quit smoking, that would be money that you could use for food,” but when there’s so many overwhelming barriers in one individual’s life, that’s the last of the things that they’re going to focus on. So that, I think, is a huge barrier. We’re serving the indigent, low-income, uninsured population with lots of big issues, and so if you can …. help them resolve some of those other issues, what my staff tell me, then you can approach them about stopping smoking.(Edith, Director of Behavioral Health Care Services)
3.2.4. Limited Resources for Addressing Tobacco Dependence
Well, first of all, I think there has to be a lot of education on the link between continuing smoking and risk of relapse. There would have to be that buy-in for that piece of it because if there’s not—and again, it’s very old school and I know it’s antiquated but I think it’s very—I don’t think I’ll employ the only person in the treatment realm or in recovery realm that feels like you shouldn’t quit all at once. That’s kind of has always been the thought process. “Okay. Well, you’re quitting. Your three or four drugs of choice were—or we definitely don’t want you to quit smoking.” I mean that’s definitely been an old-school mentality. I think that education would be a key.(Jane, direct service provider, Director of Step One Services)
[…] that [tobacco education training] would probably be an area of improvement for us to provide better clinical training for tobacco use and cessation for our clinical staff. That might help bring them onboard more actively to encourage people to try to quit using tobacco if they had a better understanding of that […] I think that the clinicians probably need more training and to create better buy-in on the importance of not using tobacco products. Also encouraging their clients and participants to pursue tobacco cessation as well as recovery from other substances.(Lisa, direct service provider, Director of Operations)
I think it all comes down, I guess, in the bottom line, it all comes down to funding. Like I said, funding in the form of being able to dedicate specific staff to just this issue, to run smoking cessation groups, to do the trainings. I think what we’re doing is pretty much—well, maybe it’s not the bare minimum […] but there’s so much potential for this to grow but it all comes down to lack of staff, which comes down to lack of resources to be able to hire and train staff and have them specifically devoted to that.(Susan, Director of Special Programs)
[Providers’] case load is high and they have limited time with people and that not an environment that is conducive to prioritizing smoking cessation, let me just put it like that. It’s like, I’m supposed to see now my time cut down. Now my time is cut down by this many minutes to see this many clients, and now we have two vacant positions and so it’s just nonstop, nonstop, nonstop. My groups are growing bigger. The timeframe that I have to meet with people is growing smaller and it’s just—you tend to get on that slimmed down version of service provision.(Susan, Director of Special Programs)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Drope, J.; Liber, A.C.; Cahn, Z.; Stoklosa, M.; Kennedy, R.; Douglas, C.E.; Henson, R.; Drope, J. Who’s still smoking? Disparities in adult cigarette smoking prevalence in the United States. CA Cancer J. Clin. 2018, 68, 106–115. [Google Scholar] [CrossRef] [PubMed]
- Schroeder, S.A.; Morris, C.D. Confronting a neglected epidemic: Tobacco cessation for persons with mental illnesses and substance abuse problems. Annu. Rev. Public Health 2010, 31, 297–314. [Google Scholar] [CrossRef]
- Tidey, J.W. Advancing Our Understanding of Tobacco Use in Vulnerable Populations. Nicotine Tob. Res. 2020, 22, 865–866. [Google Scholar] [CrossRef] [PubMed]
- Williams, J.M.; Steinberg, M.L.; Griffiths, K.G.; Cooperman, N. Smokers with behavioral health comorbidity should be designated a tobacco use disparity group. Am. J. Public Health 2013, 103, 1549–1555. [Google Scholar] [CrossRef] [PubMed]
- Burden of Tobacco Use in the U.S. Available online: https://www.cdc.gov/tobacco/campaign/tips/resources/data/cigarette-smoking-in-united-states.html (accessed on 2 December 2022).
- Guydish, J.; Passalacqua, E.; Tajima, B.; Chan, M.; Chun, J.; Bostrom, A. Smoking Prevalence in Addiction Treatment: A Review. Nicotine Tob. Res. 2011, 13, 401–411. [Google Scholar] [CrossRef] [PubMed]
- Guydish, J.; Yip, D.; Le, T.; Gubner, N.R.; Delucchi, K.; Roman, P. Smoking-related outcomes and associations with tobacco-free policy in addiction treatment, 2015–2016. Drug Alcohol Depend. 2017, 179, 355–361. [Google Scholar] [CrossRef]
- Guydish, J.; Yip, D.; Le, T.; Gubner, N.R.; Williams, D.D.; Delucchi, K.L. Tobacco Cessation Services in Addiction Treatment: What Do Clients Say? Psychiatr. Serv. 2019, 70, 229–232. [Google Scholar] [CrossRef]
- Guydish, J.; Le, T.; Hosakote, S.; Straus, E.; Wong, J.; Martínez, C.; Delucchi, K. Tobacco use among substance use disorder (SUD) treatment staff is associated with tobacco-related services received by clients. J. Subst. Abuse Treat. 2022, 132, 108496. [Google Scholar] [CrossRef]
- Richter, K.P.; Gibson, C.A.; Ahluwalia, J.S.; Schmelzle, K.H. Tobacco use and quit attempts among methadone maintenance clients. Am. J. Public Health 2001, 91, 296–299. [Google Scholar]
- Callaghan, R.C.; Gatley, J.M.; Sykes, J.; Taylor, L. The prominence of smoking-related mortality among individuals with alcohol- or drug-use disorders. Drug Alcohol Rev. 2018, 37, 97–105. [Google Scholar] [CrossRef]
- Glei, D.A.; Lee, C.; Weinstein, M. Socioeconomic disparities in U.S. mortality: The role of smoking and alcohol/drug abuse. SSM Popul. Health 2020, 12, 100699. [Google Scholar] [CrossRef] [PubMed]
- Bandiera, F.C.; Anteneh, B.; Le, T.; Delucchi, K.; Guydish, J. Tobacco-Related Mortality among Persons with Mental Health and Substance Abuse Problems. PLoS ONE 2015, 10, e0120581. [Google Scholar] [CrossRef] [PubMed]
- Hall, S.M.; Prochaska, J.J. Treatment of smokers with co-occurring disorders: Emphasis on integration in mental health and addiction treatment settings. Annu. Rev. Clin. Psychol. 2009, 5, 409–431. [Google Scholar] [CrossRef] [PubMed]
- Fiore, M.C.; Bailey, W.C.; Cohen, S.J. Treating Tobacco Use and Dependence: Clinical Practice Guideline; U.S. Department of Health and Human Services: Rockville, MD, USA, 2000. [Google Scholar]
- Marynak, K.; VanFrank, B.; Tetlow, S.; Mahoney, M.; Phillips, E.; Jamal Mbbs, A.; Schecter, A.; Tipperman, D.; Babb, S. Tobacco Cessation Interventions and Smoke-Free Policies in Mental Health and Substance Abuse Treatment Facilities—United States, 2016. Morb. Mortal. Wkly. Rep. 2018, 67, 519–523. [Google Scholar] [CrossRef]
- Reitzel, L.R.; Britton, M.K.; Martinez Leal, I.; Chen, T.A.; Kyburz, B.; Williams, T.; Rogova, A.; Jafry, M.Z. Evidence-Based Tobacco Control Policies and Practices in Substance Use Treatment Settings across Texas: A Statewide Needs Assessment; Report 2 for HHS000961900001; Taking Texas Tobacco Free: Austin, TX, USA, 2022; Unpublished report. [Google Scholar]
- Wilson, A.J.; Bonevski, B.; Dunlop, A.; Shakeshaft, A.; Tzelepis, F.; Walsberger, S.; Farrell, M.; Kelly, P.J.; Guillaumier, A. ‘The lesser of two evils’: A qualitative study of staff and client experiences and beliefs about addressing tobacco in addiction treatment settings. Drug Alcohol Rev. 2016, 35, 92–101. [Google Scholar] [CrossRef]
- Gill, B.S.; Bennett, D.L.; Abu-Salha, M.; Fore-Arcand, L. Addiction professionals’ attitudes regarding treatment of nicotine dependence. J. Subst. Abuse Treat. 2000, 19, 317–318. [Google Scholar] [CrossRef]
- Cookson, C.; Strang, J.; Ratschen, E.; Sutherland, G.; Finch, E.; McNeill, A. Smoking and its treatment in addiction services: Clients’ and staff behaviour and attitudes. BMC Health Serv. Res. 2014, 14, 304. [Google Scholar] [CrossRef]
- Clarke, J.G.; Stein, M.D.; McGarry, K.A.; Gogineni, A. Interest in smoking cessation among injection drug users. Am. J. Addict. 2001, 10, 159–166. [Google Scholar]
- Baca, C.T.; Yahne, C.E. Smoking cessation during substance abuse treatment: What you need to know. J. Subst. Abuse Treat. 2009, 36, 205–219. [Google Scholar] [CrossRef]
- Prochaska, J.J.; Delucchi, K.; Hall, S.M. A meta-analysis of smoking cessation interventions with individuals in substance abuse treatment or recovery. J. Consult. Clin. Psychol. 2004, 72, 1144–1156. [Google Scholar] [CrossRef]
- Rohsenow, D.J.; Monti, P.M.; Colby, S.M.; Gulliver, S.B.; Swift, R.M.; Abrams, D.B. Naltrexone treatment for alcoholics: Effect on cigarette smoking rates. Nicotine Tob. Res. 2003, 5, 231–236. [Google Scholar] [CrossRef] [PubMed]
- Weinberger, A.H.; Platt, J.; Esan, H.; Galea, S.; Erlich, D.; Goodwin, R.D. Cigarette Smoking Is Associated With Increased Risk of Substance Use Disorder Relapse: A Nationally Representative, Prospective Longitudinal Investigation. J. Clin. Psychiatry 2017, 78, e152–e160. [Google Scholar] [CrossRef] [PubMed]
- Reitzel, L.R.; Nguyen, N.; Eischen, S.; Thomas, J.; Okuyemi, K.S. Is smoking cessation associated with worse comorbid substance use outcomes among homeless adults? Addiction 2014, 109, 2098–2104. [Google Scholar] [CrossRef] [PubMed]
- Ziedonis, D.M.; Guydish, J.; Williams, J.; Steinberg, M.; Foulds, J. Barriers and solutions to addressing tobacco dependence in addiction treatment programs. Alcohol Res. Health 2006, 29, 228–235. [Google Scholar]
- Fuller, B.E.; Guydish, J.; Tsoh, J.; Reid, M.S.; Resnick, M.; Zammarelli, L.; Ziedonis, D.M.; Sears, C.; McCarty, D. Attitudes toward the integration of smoking cessation treatment into drug abuse clinics. J. Subst. Abuse Treat. 2007, 32, 53–60. [Google Scholar] [CrossRef] [PubMed]
- Ajzen, I. The theory of planned behavior. Organ. Behav. Hum. Decis. Process. 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Francis, J.; Eccles, M.; Johnston, M.; Walker, A.E.; Grimshaw, J.M.; Foy, R.; Kaner, E.F.S.; Smith, L.; Bonetti, D. Constructing Questionnaires Based on the Theory of Planned Behaviour: A Manual for Health Services Researchers. 2004. Available online: https://openaccess.city.ac.uk/id/eprint/1735/1/ (accessed on 14 March 2023).
- Five Major Steps to Intervention (The “5 A’s”). Available online: https://www.ahrq.gov/prevention/guidelines/tobacco/5steps.html (accessed on 2 December 2022).
- Creswell, J.W.; Clark, V.L.P. Designing and Conducting Mixed Methods Research; Sage Publications: Thousand Oaks, CA, USA, 2017. [Google Scholar]
- Greene, J.C.; Caracelli, V.J.; Graham, W.F. Toward a Conceptual Framework for Mixed-Method Evaluation Designs. Educ. Eval. Policy Anal. 1989, 11, 255–274. [Google Scholar] [CrossRef]
- Public Health Regions. Available online: https://www.dshs.texas.gov/regions/default.shtm (accessed on 10 July 2022).
- Cornelius, M.E.; Loretan, C.G.; Wang, T.W.; Jamal, A.; Homa, D.M. Tobacco Product Use Among Adults—United States, 2020. Morb. Mortal. Wkly. Rep. 2022, 71, 397–405. [Google Scholar] [CrossRef]
- Kalman, D.; Hayes, K.; Colby, S.M.; Eaton, C.A.; Rohsenow, D.J.; Monti, P.M. Concurrent versus delayed smoking cessation treatment for persons in early alcohol recovery: A pilot study. J. Subst. Abuse Treat. 2001, 20, 233–238. [Google Scholar] [CrossRef]
- Key Substance Use and Mental Health Indicators in the United States: Results from the 2020 National Survey on Drug Use and Health (HHS Publication No. PEP21-07-01-003, NSDUH Series H-56). Available online: https://www.samhsa.gov/data/report/2019-nsduh-annual-national-report (accessed on 21 December 2022).
- Jafry, M.Z.; Reuven, S.M.; Britton, M.; Chen, T.A.; Martinez Leal, I.; Rogova, A.; Kyburz, B.; Williams, T.; Patel, M.; Reitzel, L.R. Providers’ Non-Cigarette Tobacco Use Intervention Practices in Relation to Beliefs about Patients, Prioritization of and Skills for Intervention, and Referral Knowledge in Texas Healthcare Centers Providing Care to Persons with Behavioral Health Needs. Int. J. Environ. Res. Public Health 2022, 19, 14269. [Google Scholar] [CrossRef]
- Taing, M.; Le, K.; Britton, M.; Chen, T.A.; Parent, M.; Tami-Maury, I.; Martinez Leal, I.; Rogova, A.; Kyburz, B.; Williams, T.; et al. Smoking Intervention Practices in Texas Healthcare Centers with Sexual and Gender Minority Patients. Health Behav. Policy Rev. 2022, 9, 1074–1088. [Google Scholar] [CrossRef] [PubMed]
- Loparco, C.R.; Chen, T.A.; Martinez Leal, I.; Britton, M.; Carter, B.J.; Correa-Fernández, V.; Kyburz, B.; Williams, T.; Casey, K.; Rogova, A.; et al. Organization-Level Factors Associated with Changes in the Delivery of the Five A’s for Smoking Cessation following the Implementation of a Comprehensive Tobacco-Free Workplace Program within Substance Use Treatment Centers. Int. J. Environ. Res. Public Health 2022, 19, 11850. [Google Scholar] [CrossRef] [PubMed]
- Correa-Fernández, V.; Wilson, W.T.; Kyburz, B.; O’Connor, D.P.; Stacey, T.; Williams, T.; Lam, C.Y.; Reitzel, L.R. Evaluation of the Taking Texas Tobacco Free Workplace Program within behavioral health centers. Transl. Behav. Med. 2018, 9, 319–327. [Google Scholar] [CrossRef] [PubMed]
- Le, K.; Chen, T.A.; Martinez Leal, I.; Correa-Fernández, V.; Obasi, E.M.; Kyburz, B.; Williams, T.; Casey, K.; Taing, M.; O’Connor, D.P.; et al. Organizational Factors Moderating Changes in Tobacco Use Dependence Care Delivery Following a Comprehensive Tobacco-Free Workplace Intervention in Non-Profit Substance Use Treatment Centers. Int. J. Environ. Res. Public Health 2021, 18, 10485. [Google Scholar] [CrossRef]
- Taing, M.; Nitturi, V.; Chen, T.A.; Kyburz, B.; Martinez Leal, I.; Correa-Fernández, V.; Obasi, E.M.; Williams, T.; Casey, K.; O’Connor, D.P.; et al. Implementation and Outcomes of a Comprehensive Tobacco Free Workplace Program in Opioid Treatment Centers. Int. J. Environ. Res. Public Health 2022, 19, 239. [Google Scholar] [CrossRef]
- Nitturi, V.; Chen, T.-A.; Kyburz, B.; Martinez Leal, I.; Correa-Fernandez, V.; O’Connor, D.P.; Williams, T.; Garey, L.; Stacey, T.; Wilson, W.T.; et al. Organizational Characteristics and Readiness for Tobacco-Free Workplace Program Implementation Moderates Changes in Clinician’s Delivery of Smoking Interventions within Behavioral Health Treatment Clinics. Nicotine Tob. Res. 2020, 23, 310–319. [Google Scholar] [CrossRef]
- Taing, M.; Kyburz, B.; Martinez Leal, I.; Le, K.; Chen, T.-A.; Correa-Fernandez, V.; Williams, T.; O’Connor, D.P.; Obasi, E.M.; Casey, K.; et al. Clinician Training in the Adaptation of a Comprehensive Tobacco-Free Workplace Program in Agencies Serving the Homeless and Vulnerably Housed. Int. J. Environ. Res. Public Health 2020, 17, 6154. [Google Scholar] [CrossRef]
- Shi, Y.; Cummins, S.E. Smoking Cessation Services and Smoke-Free Policies at Substance Abuse Treatment Facilities: National Survey Results. Psychiatr. Serv. 2015, 66, 610–616. [Google Scholar] [CrossRef]
- Ando, H.; Cousins, R.; Young, C. Achieving Saturation in Thematic Analysis: Development and Refinement of a Codebook. Compr. Psychol. 2014, 3, 03.CP.3.4. [Google Scholar] [CrossRef]
- Patton, M.Q. Enhancing the quality and credibility of qualitative analysis. Health Serv. Res. 1999, 34, 1189–1208. [Google Scholar]
- Dougherty, C.J. Bad faith and victimblaming: The limits of health promotion. Health Care Anal. 1993, 1, 111–119. [Google Scholar] [CrossRef] [PubMed]
- Chaiton, M.; Diemert, L.; Cohen, J.E.; Bondy, S.J.; Selby, P.; Philipneri, A.; Schwartz, R. Estimating the number of quit attempts it takes to quit smoking successfully in a longitudinal cohort of smokers. BMJ Open 2016, 6, e011045. [Google Scholar] [CrossRef] [PubMed]
- Prochaska, J.J. Failure to treat tobacco use in mental health and addiction treatment settings: A form of harm reduction? Drug Alcohol Depend. 2010, 110, 177–182. [Google Scholar] [CrossRef] [PubMed]
- Gatley, J.M.; Callaghan, R.C. Tobacco-Related Mortality among Individuals with Alcohol or Drug Use Disorders. In Neuropathology of Drug Addictions and Substance Misuse; Academic Press: Cambridge, MA, USA, 2016; ISBN 9780128002131. [Google Scholar]
- Taylor, G.; McNeill, A.; Girling, A.; Farley, A.; Lindson-Hawley, N.; Aveyard, P. Change in mental health after smoking cessation: Systematic review and meta-analysis. Br. Med. J. 2014, 348, g1151. [Google Scholar] [CrossRef]
- Our World in Data, Deaths from Tobacco, Alcohol and Drugs. Available online: https://ourworldindata.org/grapher/substances-risk-factor-vs-direct-deaths?country=~USA (accessed on 21 December 2022).
- National Center for Chronic Disease Prevention and Health Promotion (NCCDPHP). Reports of the Surgeon General. In The Health Consequences of Smoking-50 Years of Progress: A Report of the Surgeon General; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2014. [Google Scholar]
- Baggett, T.P.; Tobey, M.L.; Rigotti, N.A. Tobacco use among homeless people--addressing the neglected addiction. N. Engl. J. Med. 2013, 369, 201–204. [Google Scholar] [CrossRef]
- Businelle, M.S.; Kendzor, D.E.; Reitzel, L.R.; Costello, T.J.; Cofta-Woerpel, L.; Li, Y.; Mazas, C.A.; Vidrine, J.I.; Cinciripini, P.M.; Greisinger, A.J.; et al. Mechanisms linking socioeconomic status to smoking cessation: A structural equation modeling approach. Health Psychol. 2010, 29, 262–273. [Google Scholar] [CrossRef]
- Voigt, K. Smoking and Social Justice. Public Health Ethics 2010, 3, 91–106. [Google Scholar] [CrossRef]
- Marmot, M. Smoking and inequalities. Lancet 2006, 368, 341–342. [Google Scholar] [CrossRef]
- Graham, H. Women’s smoking and family health. Soc. Sci. Med. 1987, 25, 47–56. [Google Scholar] [CrossRef]
- Graham, H.; Inskip, H.M.; Francis, B.; Harman, J. Pathways of disadvantage and smoking careers: Evidence and policy implications. J. Epidemiol. Community Health 2006, 60 (Suppl. S2), ii7–ii12. [Google Scholar] [CrossRef]
- Correa-Fernández, V.; Díaz-Toro, E.C.; Reitzel, L.R.; Guo, L.; Chen, M.; Li, Y.; Calo, W.A.; Shih, Y.T.; Wetter, D.W. Combined treatment for at-risk drinking and smoking cessation among Puerto Ricans: A randomized clinical trial. Addict. Behav. 2017, 65, 185–192. [Google Scholar] [CrossRef] [PubMed]
- Hill, S.; Amos, A.; Clifford, D.; Platt, S. Impact of tobacco control interventions on socioeconomic inequalities in smoking: Review of the evidence. Tob. Control 2014, 23, e89–e97. [Google Scholar] [CrossRef] [PubMed]
- Smith, C.E.; Hill, S.E.; Amos, A. Impact of population tobacco control interventions on socioeconomic inequalities in smoking: A systematic review and appraisal of future research directions. Tob. Control 2020, 30, e87–e95. [Google Scholar] [CrossRef] [PubMed]
- Wright, A.; Smith, K.E.; Hellowell, M. Policy lessons from health taxes: A systematic review of empirical studies. BMC Public Health 2017, 17, 583. [Google Scholar] [CrossRef]
- Feliu, A.; Filippidis, F.T.; Joossens, L.; Fong, G.T.; Vardavas, C.I.; Baena, A.; Castellano, Y.; Martínez, C.; Fernández, E. Impact of tobacco control policies on smoking prevalence and quit ratios in 27 European Union countries from 2006 to 2014. Tob. Control 2019, 28, 101–109. [Google Scholar]
- Patients Not Ready to Make a Quit Attempt Now (The “5 R’s”). Available online: https://www.ahrq.gov/prevention/guidelines/tobacco/5rs.html#:~:text=The%20clinician%20can%20motivate%20clients,Rewards%2C%20Roadblocks%2C%20and%20Repetition (accessed on 2 December 2022).
- American Academy of Addiction Psychiatry, Nicotine Dependence. Available online: https://www.aaap.org/wp-content/uploads/2015/06/AAAP-nicotine-dependence-FINAL.pdf (accessed on 2 December 2022).
- Sheals, K.; Tombor, I.; McNeill, A.; Shahab, L. A mixed-method systematic review and meta-analysis of mental health professionals’ attitudes toward smoking and smoking cessation among people with mental illnesses. Addiction 2016, 111, 1536–1553. [Google Scholar] [CrossRef] [PubMed]
- Graydon, M.M.; Corno, C.M.; Schacht, R.L.; Knoblach, D.J.; Wiprovnick, A.E.; Thrash, S.T.; Petersen, A.A.; DiClemente, C.C. A statewide initiative to train behavioral health providers in smoking cessation. Transl. Behav. Med. 2018, 8, 855–866. [Google Scholar] [CrossRef]
- Li, I.C.; Lee, S.-Y.; Chen, C.-Y.; Jeng, Y.-Q.; Chen, Y.-C. Facilitators and Barriers to Effective Smoking Cessation: Counselling Services for Inpatients from Nurse-Counsellors’ Perspectives—A Qualitative Study. Int. J. Environ. Res. Public Health 2014, 11, 4782–4798. [Google Scholar] [CrossRef]
- Eby, L.T.; Burk, H.; Maher, C.P. How serious of a problem is staff turnover in substance abuse treatment? A longitudinal study of actual turnover. J. Subst. Abuse Treat. 2010, 39, 264–271. [Google Scholar] [CrossRef]
- Aveyard, P.; Begh, R.; Parsons, A.; West, R. Brief opportunistic smoking cessation interventions: A systematic review and meta-analysis to compare advice to quit and offer of assistance. Addiction 2012, 107, 1066–1073. [Google Scholar] [CrossRef]
- Papadakis, S.; Anastasaki, M.; Papadakaki, M.; Antonopoulou, Μ.; Chliveros, C.; Daskalaki, C.; Varthalis, D.; Triantafyllou, S.; Vasilaki, I.; McEwen, A.; et al. ‘Very brief advice’ (VBA) on smoking in family practice: A qualitative evaluation of the tobacco user’s perspective. BMC Fam. Pract. 2020, 21, 121. [Google Scholar] [CrossRef] [PubMed]
- McKelvey, K.; Thrul, J.; Ramo, D. Impact of quitting smoking and smoking cessation treatment on substance use outcomes: An updated and narrative review. Addict. Behav. 2017, 65, 161–170. [Google Scholar] [CrossRef]
- Vidrine, J.I.; Shete, S.; Cao, Y.; Greisinger, A.; Harmonson, P.; Sharp, B.; Miles, L.; Zbikowski, S.M.; Wetter, D.W. Ask-Advise-Connect. JAMA Intern. Med. 2013, 173, 458. [Google Scholar] [CrossRef] [PubMed]
- Vidrine, J.I.; Shete, S.; Li, Y.; Cao, Y.; Alford, M.H.; Michelle Galindo-Talton, R.; Rabius, V.; Sharp, B.; Harmonson, P.; Zbikowski, S.M.; et al. The Ask–Advise–Connect Approach for Smokers in a Safety Net Healthcare System. Am. Prev. Med. 2013, 45, 737–741. [Google Scholar] [CrossRef]
- Himelhoch, S.; Riddle, J.; Goldman, H.H. Barriers to implementing evidence-based smoking cessation practices in nine community mental health sites. Psychiatr. Serv. 2014, 65, 75–80. [Google Scholar] [CrossRef] [PubMed]
- Gifford, E.; Tavakoli, S.; Wisdom, J.; Hamlett-Berry, K. Implementation of smoking cessation treatment in VHA substance use disorder residential treatment programs. Psychiatr. Serv. 2015, 66, 295–302. [Google Scholar] [CrossRef]
- Hunt, J.J.; Cupertino, A.P.; Gajewski, B.J.; Jiang, Y.; Ronzani, T.M.; Richter, K.P. Staff commitment to providing tobacco dependence in drug treatment: Reliability, validity, and results of a national survey. Psychol. Addict. Behav. 2014, 28, 389–395. [Google Scholar] [CrossRef]
- O’Cathain, A.; Murphy, E.; Nicholl, J. The Quality of Mixed Methods Studies in Health Services Research. J. Health Serv. Res. Policy 2008, 13, 92–98. [Google Scholar] [CrossRef]


{kind=link}
| Variables of Interest | All Centers |
|---|---|
| % (n) | |
| Healthcare Center Characteristics | |
| Center type | |
| Federally Qualified Health Center | 10.84 (9) |
| Substance-use program within LMHA | 6.02 (5) |
| LMHA overall | 19.28 (16) |
| Stand-alone substance-use treatment center | 63.86 (53) |
| # of unique clients seen annually | |
| 50–200 | 32.10 (26) |
| 201–1000 | 44.44 (36) |
| >1000 | 23.46 (19) |
| # of full-time employees | |
| 1–50 | 61.45 (51) |
| >50 | 38.55 (32) |
| Comprehensive tobacco-free workplace policy | |
| Yes | 48.19 (40) |
| No | 51.81 (43) |
| Provider’s Perceptions on Concurrent Smoking/Tobacco Cessation and Non-Nicotine-Substance-Use Treatment * | |
| In your opinion, what is the best point to encourage clients to stop smoking or using other tobacco products? | |
| Never/It depends on the client/After 1 year of treatment | 60.24 (50) |
| As soon as client begins treatment | 39.76 (33) |
| If a client has been in recovery from alcoholism for <6 months, quitting smoking would jeopardize their recovery. ⟡ | |
| Yes | 45.78 (38) |
| No | 54.22 (45) |
| Providers’ Provision of the 5A’s Smoking-cessation Intervention with Clients | |
| Asks clients about cigarette smoking ◊ | |
| Yes | 69.88 (58] |
| No | 30.12 (25) |
| Advises clients to quit smoking ◊ | |
| Yes | 68.67 (57) |
| No | 31.33 (26) |
| Assesses client interest in quitting smoking ◊ | |
| Yes | 62.65 (52) |
| No | 37.35 (31) |
| Assists a smoking quit attempt ◊ | |
| Yes | 57.83 (48) |
| No | 42.17 (35) |
| Arranges a follow-up ◊ | |
| Yes | 33.73 (28) |
| No | 66.27 (55) |
| Adjusted Model | |||||
|---|---|---|---|---|---|
| Estimate | SE | OR (95% CI) | p-Value | ||
| Ask | Intercept | 2.234 | 0.654 | 0.001 | |
| Perceived Best Point to Encourage Clients to Stop Smoking or Using Other Tobacco Products (ref: As soon as client begins treatment) | −1.634 | 0.620 | 0.195 (0.058, 0.657) | 0.008 | |
| Center Type FQHC (ref: SUTC) | 0.983 | 0.894 | 2.672 (0.463, 15.409) | 0.272 | |
| Center Type LMHA (ref: SUTC) | 1.565 | 1.752 | 4.781 (0.154, 148.271) | 0.372 | |
| Center Type Global LMHA (ref: SUTC) | −0.730 | 0.662 | 0.482 (0.132, 1.765) | 0.270 | |
| Comprehensive Tobacco-Free Workplace Policy (ref: No) | −0.766 | 0.558 | 0.465 (0.156, 1.389) | 0.170 | |
| Advise | Intercept | 2.607 | 0.701 | <0.001 | |
| Perceived Best Point to Encourage Clients to Stop Smoking or Using Other Tobacco Products (ref: As soon as client begins treatment) | −1.739 | 0.647 | 0.176 (0.049, 0.625) | 0.007 | |
| Center Type FQHC (ref: SUTC) | 1.319 | 0.927 | 3.741 (0.608, 23.013) | 0.155 | |
| Center Type LMHA (ref: SUTC) | 1.812 | 1.842 | 6.122 (0.166, 226.462) | 0.325 | |
| Center Type Global LMHA (ref: SUTC) | −0.847 | 0.671 | 0.429 (0.115, 1.599) | 0.207 | |
| Comprehensive Tobacco-Free Workplace Policy (ref: No) | −1.465 | 0.596 | 0.231 (0.072, 0.742) | 0.014 | |
| Assess | Intercept | 1.312 | 0.542 | 0.015 | |
| Perceived Best Point to Encourage Clients to Stop Smoking or Using Other Tobacco Products (ref: As soon as client begins treatment) | −1.134 | 0.539 | 0.322 (0.112, 0.925) | 0.035 | |
| Center Type FQHC (ref: SUTC) | −0.489 | 0.783 | 0.614 (0.132, 2.846) | 0.533 | |
| Center Type LMHA (ref: SUTC) | 1.676 | 1.665 | 5.346 (0.205, 139.606) | 0.314 | |
| Center Type Global LMHA (ref: SUTC) | −0.555 | 0.630 | 0.574 (0.167, 1.975) | 0.379 | |
| Comprehensive Tobacco-Free Workplace Policy (ref: No) | −0.017 | 0.514 | 0.983 (0.359, 2.691) | 0.974 | |
| Assist | Intercept | 0.725 | 0.488 | 0.137 | |
| Perceived Best Point to Encourage Clients to Stop Smoking or Using Other Tobacco Products (ref: As soon as client begins treatment) | −0.848 | 0.497 | 0.428 (0.162, 1.134) | 0.088 | |
| Center Type FQHC (ref: SUTC) | 0.670 | 0.799 | 1.955 (0.409, 9.350) | 0.401 | |
| Center Type LMHA (ref: SUTC) | 0.755 | 1.088 | 2.129 (0.252, 17.961) | 0.488 | |
| Center Type Global LMHA (ref: SUTC) | −0.097 | 0.609 | 0.908 (0.275, 2.995) | 0.874 | |
| Comprehensive Tobacco-Free Workplace Policy (ref: No) | −0.022 | 0.488 | 0.979 (0.376, 2.545) | 0.965 | |
| Arrange | Intercept | −0.667 | 0.490 | 0.174 | |
| Perceived Best Point to Encourage Clients to Stop Smoking or Using Other Tobacco Products (ref: As soon as client begins treatment) | −0.696 | 0.505 | 0.498 (0.185, 1.342) | 0.168 | |
| Center Type FQHC (ref: SUTC) | 0.136 | 0.818 | 1.145 (0.230, 5.695) | 0.868 | |
| Center Type LMHA (ref: SUTC) | 1.028 | 0.979 | 2.795 (0.410, 19.043) | 0.294 | |
| Center Type Global LMHA (ref: SUTC) | 0.016 | 0.632 | 1.016 (0.294, 3.507) | 0.980 | |
| Comprehensive Tobacco-Free Workplace Policy (ref: No) | 0.661 | 0.511 | 1.936 (0.711, 5.274) | 0.196 | |
| Ask | Intercept | 1.435 | 0.466 | 0.002 | |
| Perceives that Quitting Smoking Jeopardizes Recovery from Alcoholism (ref: No) | −0.975 | 0.518 | 0.377 (0.137, 1.040) | 0.060 | |
| Center Type FQHC (ref: SUTC) | 0.825 | 0.899 | 2.281 (0.392, 13.287) | 0.359 | |
| Center Type LMHA (ref: SUTC) | 1.874 | 1.666 | 6.512 (0.249, 170.382) | 0.261 | |
| Center Type Global LMHA (ref: SUTC) | −0.252 | 0.625 | 0.778 (0.228, 2.649) | 0.688 | |
| Comprehensive Tobacco-Free Workplace Policy (ref: No) | −0.571 | 0.531 | 0.565 (0.200, 1.599) | 0.282 | |
| Advise | Intercept | 1.555 | 0.480 | 0.001 | |
| Perceives that Quitting Smoking Jeopardizes Recovery from Alcoholism (ref: No) | −0.703 | 0.524 | 0.495 (0.177, 1.381) | 0.179 | |
| Center Type FQHC (ref: SUTC) | 0.966 | 0.905 | 2.628 (0.446, 15.476) | 0.285 | |
| Center Type LMHA (ref: SUTC) | 1.868 | 1.686 | 6.475 (0.238, 176.478) | 0.268 | |
| Center Type Global LMHA (ref: SUTC) | −0.394 | 0.622 | 0.674 (0.199, 2.283) | 0.526 | |
| Comprehensive Tobacco-Free Workplace Policy (ref: No) | −1.115 | 0.538 | 0.328 (0.114, 0.942) | 0.038 | |
| Assess | Intercept | 0.723 | 0.405 | 0.074 | |
| Perceives that Quitting Smoking Jeopardizes Recovery from Alcoholism (ref: No) | −0.536 | 0.479 | 0.585 (0.229, 1.496) | 0.263 | |
| Center Type FQHC (ref: SUTC) | −0.662 | 0.776 | 0.516 (0.113, 2.360) | 0.394 | |
| Center Type LMHA (ref: SUTC) | 1.953 | 1.637 | 7.048 (0.285, 174.255) | 0.233 | |
| Center Type Global LMHA (ref: SUTC) | −0.269 | 0.613 | 0.764 (0.230, 2.543) | 0.661 | |
| Comprehensive Tobacco-Free Workplace Policy (ref: No) | 0.123 | 0.498 | 1.131 (0.426, 3.000) | 0.805 | |
| Assist | Intercept | 0.525 | 0.396 | 0.185 | |
| Perceives that Quitting Smoking Jeopardizes Recovery from Alcoholism (ref: No) | −0.895 | 0.479 | 0.409 (0.160, 1.044) | 0.061 | |
| Center Type FQHC (ref: SUTC) | 0.708 | 0.814 | 2.031 (0.412, 10.011) | 0.384 | |
| Center Type LMHA (ref: SUTC) | 1.151 | 1.096 | 3.163 (0.369, 27.107) | 0.294 | |
| Center Type Global LMHA (ref: SUTC) | 0.222 | 0.617 | 1.248 (0.372, 4.186) | 0.719 | |
| Comprehensive Tobacco-Free Workplace Policy (ref: No) | 0.004 | 0.486 | 1.004 (0.387, 2.604) | 0.994 | |
| Arrange | Intercept | −0.866 | 0.417 | 0.038 | |
| Perceives that Quitting Smoking Jeopardizes Recovery from Alcoholism (ref: No) | −0.635 | 0.506 | 0.53 (0.197, 1.430) | 0.210 | |
| Center Type FQHC (ref: SUTC) | 0.123 | 0.814 | 1.131 (0.229, 5.578) | 0.880 | |
| Center Type LMHA (ref: SUTC) | 1.326 | 0.995 | 3.768 (0.536, 26.465) | 0.182 | |
| Center Type Global LMHA (ref: SUTC) | 0.246 | 0.640 | 1.279 (0.365, 4.487) | 0.701 | |
| Comprehensive Tobacco-Free Workplace Policy (ref: No) | 0.689 | 0.508 | 1.992 (0.737, 5.388) | 0.174 | |
| Theme | Findings |
|---|---|
| Misconceptions about concurrent treatment of tobacco and substance use: smoking reduces stress and is a valuable coping mechanism. | Many participants espoused misconceptions that concurrent treatment of tobacco and substance use was detrimental to clients, in that it could jeopardize their substance-use recovery because:
|
| “Blame the victim” mentality: clients are not interested in quitting smoking. | Most participants stated clients’ lack of interest in quitting smoking kept them from pursuing tobacco cessation with them.
|
| Attitudes towards smoking cessation: (a) devaluing of tobacco dependence as a serious addiction; (b) clients were overwhelmed by multiple social inequities and did not have the wherewithal to quit smoking. | The key attitudes participants expressed regarding smoking cessation included:
|
| Limited resources for addressing tobacco dependence. | Participants have limited resources available to them to treat tobacco dependence, including a lack of:
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Britton, M.; Martinez Leal, I.; Jafry, M.Z.; Chen, T.A.; Rogova, A.; Kyburz, B.; Williams, T.; Reitzel, L.R. Influence of Provider and Leader Perspectives about Concurrent Tobacco-Use Care during Substance-Use Treatment on Their Tobacco Intervention Provision with Clients: A Mixed-Methods Study. Int. J. Environ. Res. Public Health 2023, 20, 5260. https://doi.org/10.3390/ijerph20075260
Britton M, Martinez Leal I, Jafry MZ, Chen TA, Rogova A, Kyburz B, Williams T, Reitzel LR. Influence of Provider and Leader Perspectives about Concurrent Tobacco-Use Care during Substance-Use Treatment on Their Tobacco Intervention Provision with Clients: A Mixed-Methods Study. International Journal of Environmental Research and Public Health. 2023; 20(7):5260. https://doi.org/10.3390/ijerph20075260
Chicago/Turabian StyleBritton, Maggie, Isabel Martinez Leal, Midhat Z. Jafry, Tzuan A. Chen, Anastasia Rogova, Bryce Kyburz, Teresa Williams, and Lorraine R. Reitzel. 2023. "Influence of Provider and Leader Perspectives about Concurrent Tobacco-Use Care during Substance-Use Treatment on Their Tobacco Intervention Provision with Clients: A Mixed-Methods Study" International Journal of Environmental Research and Public Health 20, no. 7: 5260. https://doi.org/10.3390/ijerph20075260