
Explorative Assessment of the Temperature–Mortality Association to Support Health-Based Heat-Warning Thresholds: A National Case-Crossover Study in Switzerland
 , , , , ,
, , , , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Mortality Data
2.3. Temperature Data
2.4. Statistical Analyses
2.4.1. Temperature–Mortality Associations
2.4.2. Threshold Temperatures
2.4.3. Evaluation of Regional Variability
2.4.4. Stratified Analyses by Age Group, Season, and Time Period
2.4.5. Effect of Heatwave Duration
3. Results
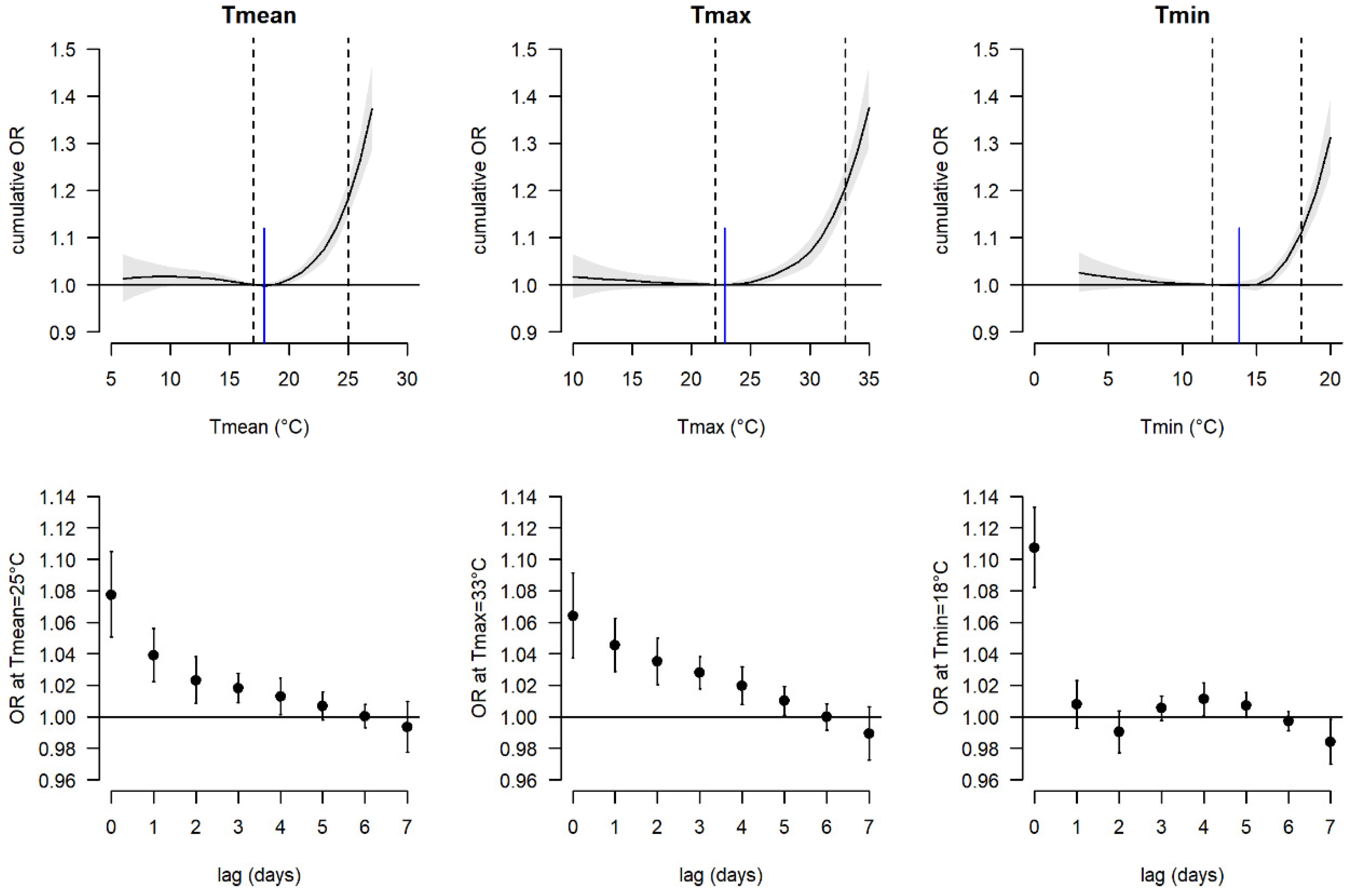
3.1. Exploration of Threshold Temperatures
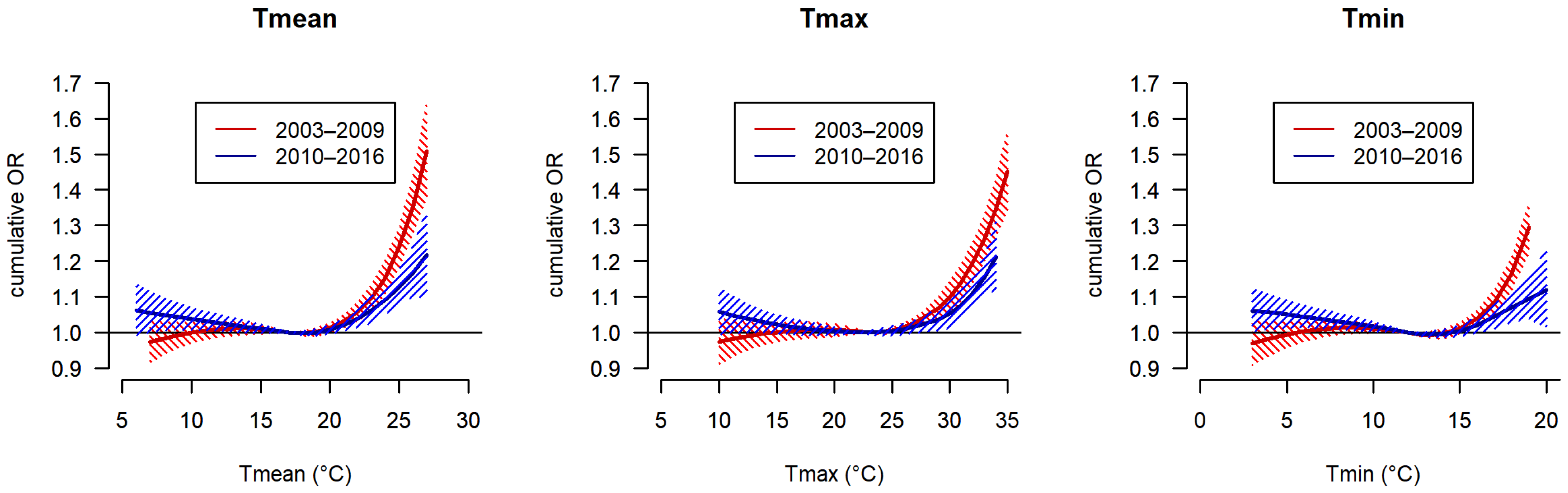
3.2. Analyses by Age Group, Season, and Time Period
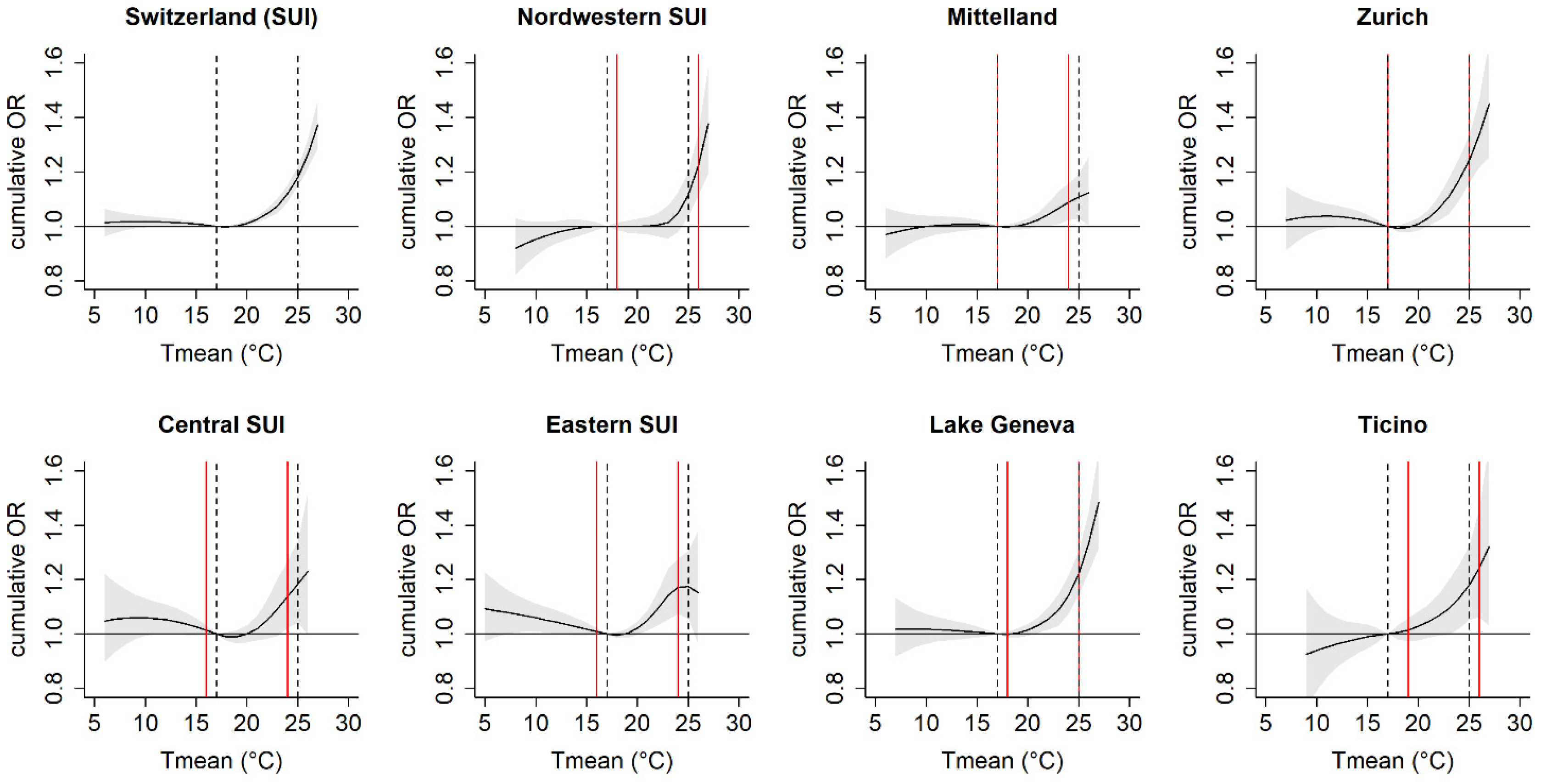
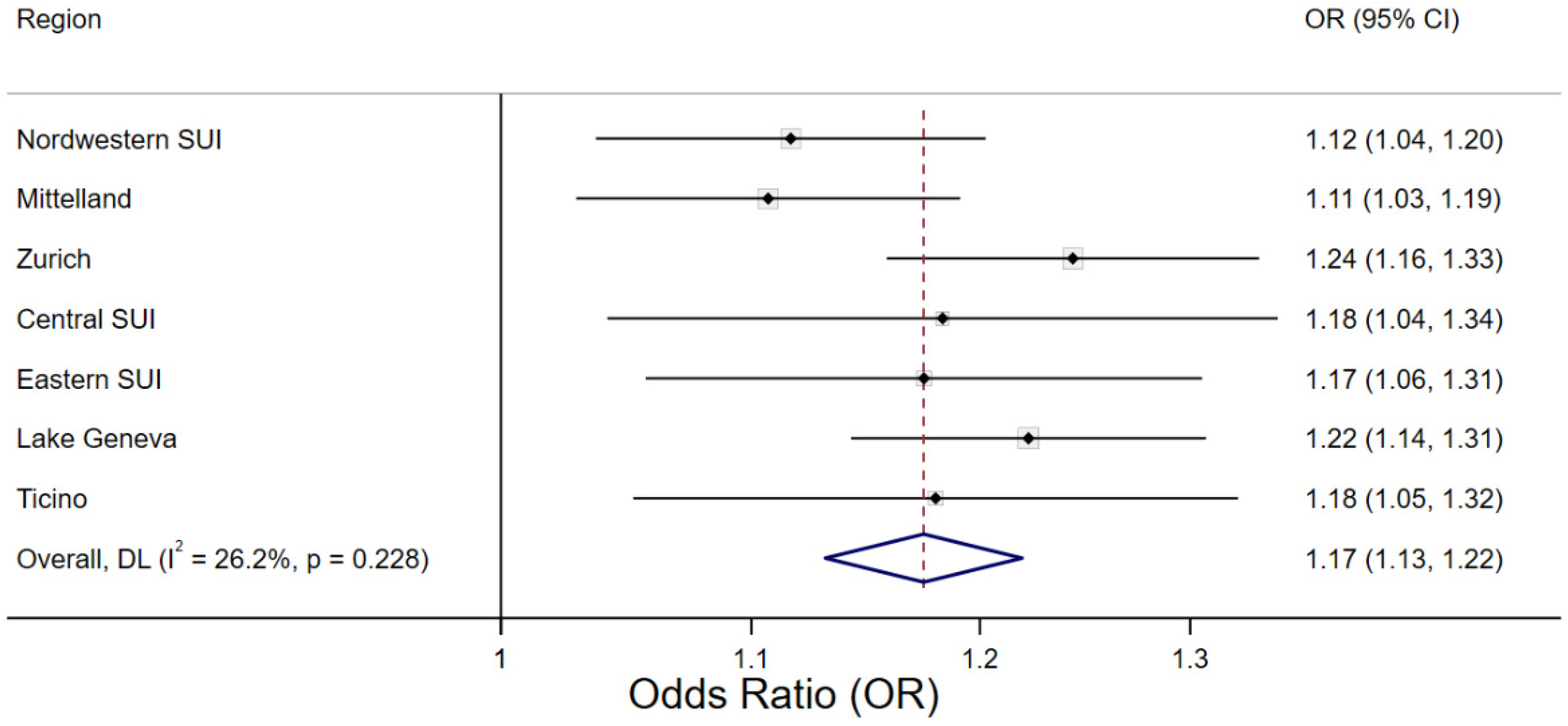
3.3. Regional Variability
3.4. Effect of Heatwave Duration
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Romanello, M.; McGushin, A.; Di Napoli, C.; Drummond, P.; Hughes, N.; Jamart, L.; Kennard, H.; Lampard, P.; Solano Rodriguez, B.; Arnell, N.; et al. The 2021 report of the Lancet Countdown on health and climate change: Code red for a healthy future. Lancet 2021, 398, 1619–1662. [Google Scholar] [CrossRef]
- IPCC. Climate Change 2022: Impacts, Adaptation and Vulnerability. Contribution of Working Group II to the Sixth Assessment Report of the Intergovernmental Panel on Climate Change; Cambridge University Press: Cambridge, UK; New York, NY, USA, 2022; p. 3056. [Google Scholar]
- Song, X.; Wang, S.; Hu, Y.; Yue, M.; Zhang, T.; Liu, Y.; Tian, J.; Shang, K. Impact of ambient temperature on morbidity and mortality: An overview of reviews. Sci. Total Environ. 2017, 586, 241–254. [Google Scholar] [CrossRef] [PubMed]
- Benmarhnia, T.; Deguen, S.; Kaufman, J.S.; Smargiassi, A. Review article: Vulnerability to heat-related mortality: A systematic review, meta-analysis, and meta-regression analysis. Epidemiology 2015, 26, 781–793. [Google Scholar] [CrossRef] [PubMed]
- Åström, D.O.; Bertil, F.; Joacim, R. Heat wave impact on morbidity and mortality in the elderly population: A review of recent studies. Maturitas 2011, 69, 99–105. [Google Scholar] [CrossRef]
- Ebi, K.L.; Capon, A.; Berry, P.; Broderick, C.; de Dear, R.; Havenith, G.; Honda, Y.; Kovats, R.S.; Ma, W.; Malik, A.; et al. Hot weather and heat extremes: Health risks. Lancet 2021, 398, 698–708. [Google Scholar] [CrossRef]
- Vicedo-Cabrera, A.M.; Scovronick, N.; Sera, F.; Royé, D.; Schneider, R.; Tobias, A.; Astrom, C.; Guo, Y.; Honda, Y.; Hondula, D.; et al. The burden of heat-related mortality attributable to recent human-induced climate change. Nat. Clim. Change 2021, 11, 492–500. [Google Scholar] [CrossRef]
- Zhao, Q.; Guo, Y.; Ye, T.; Gasparrini, A.; Tong, S.; Overcenco, A.; Urban, A.; Schneider, A.; Entezari, A.; Vicedo-Cabrera, A.M.; et al. Global, regional, and national burden of mortality associated with non-optimal ambient temperatures from 2000 to 2019: A three-stage modelling study. Lancet Planet. Health 2021, 5, e415–e425. [Google Scholar] [CrossRef] [PubMed]
- Saucy, A.; Ragettli, M.S.; Vienneau, D.; de Hoogh, K.; Tangermann, L.; Schäffer, B.; Wunderli, J.-M.; Probst-Hensch, N.; Röösli, M. The role of extreme temperature in cause-specific acute cardiovascular mortality in Switzerland: A case-crossover study. Sci. Total Environ. 2021, 790, 147958. [Google Scholar] [CrossRef]
- Gasparrini, A.; Guo, Y.; Hashizume, M.; Lavigne, E.; Zanobetti, A.; Schwartz, J.; Tobias, A.; Tong, S.; Rocklöv, J.; Forsberg, B.; et al. Mortality risk attributable to high and low ambient temperature: A multicountry observational study. Lancet 2015, 386, 369–375. [Google Scholar] [CrossRef]
- Guo, Y.; Gasparrini, A.; Armstrong, B.G.; Tawatsupa, B.; Tobias, A.; Lavigne, E.; de Sousa Zanotti Stagliorio Coelho, M.; Pan, X.; Kim, H.; Hashizume, M.; et al. Heat wave and mortality: A multicountry, multicommunity study. Environ. Health Perspect. 2017, 125, 087006. [Google Scholar] [CrossRef] [Green Version]
- Cheng, J.; Xu, Z.; Bambrick, H.; Su, H.; Tong, S.; Hu, W. Heatwave and elderly mortality: An evaluation of death burden and health costs considering short-term mortality displacement. Environ. Int. 2018, 115, 334–342. [Google Scholar] [CrossRef]
- Åström, D.O.; Åström, C.; Forsberg, B.; Vicedo-Cabrera, A.M.; Gasparrini, A.; Oudin, A.; Sundquist, K. Heat wave–related mortality in Sweden: A case-crossover study investigating effect modification by neighbourhood deprivation. Scand. J. Public Health 2020, 48, 428–435. [Google Scholar] [CrossRef] [PubMed]
- Vicedo-Cabrera, A.M.; Ragettli, M.S.; Schindler, C.; Röösli, M. Excess mortality during the warm summer of 2015 in Switzerland. Swiss Med. Wkly. 2016, 146, w14379. [Google Scholar] [CrossRef] [Green Version]
- Lowe, D.; Ebi, K.L.; Forsberg, B. Heatwave early warning systems and adaptation advice to reduce human health consequences of heatwaves. Int. J. Environ. Res. Public Health 2011, 8, 4623–4648. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO Regional Office for Europe. Heat and Health in the WHO European Region: Updated Evidence for Effective Prevention; WHO Regional Office for Europe: Copenhagen, Denmark, 2021; pp. 1–176. [Google Scholar]
- Casanueva, A.; Burgstall, A.; Kotlarski, S.; Messeri, A.; Morabito, M.; Flouris, A.D.; Nybo, L.; Spirig, C.; Schwierz, C. Overview of Existing Heat-Health Warning Systems in Europe. Int J Env. Res Public Health 2019, 16, 2657. [Google Scholar] [CrossRef] [Green Version]
- Kotharkar, R.; Ghosh, A. Progress in extreme heat management and warning systems: A systematic review of heat-health action plans (1995–2020). Sustain. Cities Soc. 2022, 76, 103487. [Google Scholar] [CrossRef]
- Sanchez Martinez, G.; Kendrovski, V.; Salazar, M.A.; de’Donato, F.; Boeckmann, M. Heat-health action planning in the WHO European Region: Status and policy implications. Environ. Res. 2022, 214, 113709. [Google Scholar] [CrossRef]
- Benmarhnia, T.; Bailey, Z.; Kaiser, D.; Auger, N.; King, N.; Kaufman, J. A difference-in-differences approach to assess the effect of a heat action plan on heat-related mortality, and differences in effectiveness according to sex, age, and socioeconomic status (Montreal, Quebec). Environ. Health Perspect. 2016, 124, 1694. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weinberger, K.R.; Zanobetti, A.; Schwartz, J.; Wellenius, G.A. Effectiveness of National Weather Service heat alerts in preventing mortality in 20 US cities. Environ. Int. 2018, 116, 30–38. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Solanas, È.; Basagaña, X. Temporal changes in temperature-related mortality in Spain and effect of the implementation of a Heat Health Prevention Plan. Environ. Res. 2019, 169, 102–113. [Google Scholar] [CrossRef]
- Pascal, M.; Lagarrigue, R.; Tabai, A.; Bonmarin, I.; Camail, S.; Laaidi, K.; Le Tertre, A.; Denys, S. Evolving heat waves characteristics challenge heat warning systems and prevention plans. Int. J. Biometeorol. 2021, 65, 1683–1694. [Google Scholar] [CrossRef] [PubMed]
- Xu, Z.; FitzGerald, G.; Guo, Y.; Jalaludin, B.; Tong, S. Impact of heatwave on mortality under different heatwave definitions: A systematic review and meta-analysis. Environ. Int. 2016, 89, 193–203. [Google Scholar] [CrossRef] [PubMed]
- Tobías, A.; Hashizume, M.; Honda, Y.; Sera, F.; Ng, C.F.S.; Kim, Y.; Roye, D.; Chung, Y.; Dang, T.N.; Kim, H.; et al. Geographical variations of the minimum mortality temperature at a global scale: A multicountry study. Environ. Epidemiol. 2021, 5, e169. [Google Scholar] [CrossRef] [PubMed]
- Issa, M.A.; Chebana, F.; Masselot, P.; Campagna, C.; Lavigne, É.; Gosselin, P.; Ouarda, T.B.M.J. A heat-health watch and warning system with extended season and evolving thresholds. BMC Public Health 2021, 21, 1479. [Google Scholar] [CrossRef] [PubMed]
- Ragettli, M.S.; Vicedo-Cabrera, A.M.; Schindler, C.; Röösli, M. Exploring the association between heat and mortality in Switzerland between 1995 and 2013. Environ. Res. 2017, 158C, 703–709. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.Y.; Röösli, M.; Ragettli, M.S. Estimation of Heat-Attributable Mortality Using the Cross-Validated Best Temperature Metric in Switzerland and South Korea. Int. J. Environ. Res. Public Health 2021, 18, 6413. [Google Scholar] [CrossRef]
- Kovats, R.S.; Hajat, S. Heat stress and public health: A critical review. Annu. Rev. Public Health 2008, 29, 41–55. [Google Scholar] [CrossRef] [PubMed]
- Gubler, M.; Christen, A.; Remund, J.; Brönnimann, S. Evaluation and application of a low-cost measurement network to study intra-urban temperature differences during summer 2018 in Bern, Switzerland. Urban Clim. 2021, 37, 100817. [Google Scholar] [CrossRef]
- Gehrig, R.; König, N.; Scherrer, S. Städtische Wärmeinseln in der Schweiz: Klimatologische Studie mit Messdaten in fünf Städten (EN: “Urban heat islands in Switzerland—Climatological study with measurement data in five cities”). MeteoSwiss Tech. Rep. 2018, 273, 1–63. [Google Scholar]
- de Schrijver, E.; Folly, C.L.; Schneider, R.; Franco Duran, O.H.; Gasparrini, A.; Vicedo Cabrera, A.M. A comparative analysis of the temperature-mortality risks using different weather datasets across heterogeneous regions. GeoHealth 2020, 5, e2020GH000363. [Google Scholar] [CrossRef]
- Maclure, M. The case-crossover design: A method for studying transient effects on the risk of acute events. Am. J. Epidemiol. 1991, 133, 144–153. [Google Scholar] [CrossRef]
- NCCS. CH2018—Climate Scenarios for Switzerland; National Centre for Climate Services (NCCS): Zurich, Switzerland, 2018; p. 24. ISBN 978-3-9525031-3-3. [Google Scholar]
- Ragettli, M.S.; Röösli, M. Die Bedeutung von Präventionsmassnahmen. Hitzebedingte Sterblichkeit im Sommer 2019. Prim Hosp. Care Allg. Inn. Med. 2021, 21, 90–95. [Google Scholar]
- Janes, H.; Sheppard, L.; Lumley, T. Case-crossover analyses of air pollution exposure data: Referent selection strategies and their implications for bias. Epidemiology 2005, 16, 717–726. [Google Scholar] [CrossRef] [PubMed]
- Spoerri, A.; Zwahlen, M.; Egger, M.; Bopp, M. The Swiss National Cohort: A unique database for national and international researchers. Int. J. Public Health 2010, 55, 239–242. [Google Scholar] [CrossRef] [Green Version]
- Flückiger, B.; Kloog, I.; Ragettli, M.S.; Eeftens, M.; Röösli, M.; de Hoogh, K. Modelling daily air temperature at a fine spatial resolution dealing with challenging meteorological phenomena and topography in Switzerland. Int. J. Climatol. 2022, 42, 6413–6428. [Google Scholar] [CrossRef]
- MeteoSwiss. MeteoSwiss Spatial Climate Analyses: Documentation of Datasets for Users 2021. Available online: https://www.meteoschweiz.admin.ch/content/dam/meteoswiss/de/klima/klima-der-schweiz/doc/ProdDoc_Cover.pdf (accessed on 20 June 2022).
- Kloog, I.; Nordio, F.; Coull, B.A.; Schwartz, J. Predicting spatiotemporal mean air temperature using MODIS satellite surface temperature measurements across the Northeastern USA. Remote Sens. Environ. 2014, 150, 132–139. [Google Scholar] [CrossRef]
- Hough, I.; Just, A.C.; Zhou, B.; Dorman, M.; Lepeule, J.; Kloog, I. A multi-resolution air temperature model for France from MODIS and Landsat thermal data. Environ. Res. 2020, 183, 109244. [Google Scholar] [CrossRef] [PubMed]
- Gasparrini, A. Distributed lag linear and non-linear models in R: The package dlnm. J. Stat. Softw. 2011, 43, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murage, P.; Hajat, S.; Kovats, R.S. Effect of night-time temperatures on cause and age-specific mortality in London. Environ. Epidemiol. 2017, 1, e005. [Google Scholar] [CrossRef]
- Royé, D.; Sera, F.; Tobías, A.; Lowe, R.; Gasparrini, A.; Pascal, M.; de’Donato, F.; Nunes, B.; Teixeira, J.P. Effects of hot nights on mortality in Southern Europe. Epidemiology 2021, 32, 487–498. [Google Scholar] [CrossRef]
- Gasparrini, A.; Guo, Y.; Hashizume, M.; Kinney, P.L.; Petkova, E.P.; Lavigne, E.; Zanobetti, A.; Schwartz, J.D.; Tobias, A.; Leone, M.; et al. Temporal variation in heat–mortality associations: A multicountry study. Environ. Health Perspect. 2015, 123, 1200–1207. [Google Scholar] [CrossRef] [Green Version]
- Gasparrini, A.; Armstrong, B. The impact of heat waves on mortality. Epidemiology 2011, 22, 68–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, Z.; Cheng, J.; Hu, W.; Tong, S. Heatwave and health events: A systematic evaluation of different temperature indicators, heatwave intensities and durations. Sci. Total Environ. 2018, 630, 679–689. [Google Scholar] [CrossRef] [Green Version]
- Eilers, P.H.; Marx, B.D. Flexible smoothing with B-splines and penalties. Stat. Sci. 1996, 11, 89–121. [Google Scholar] [CrossRef]
- Harris, R.J.; Deeks, J.J.; Altman, D.G.; Bradburn, M.J.; Harbord, R.M.; Sterne, J.A.C. Metan: Fixed- and Random-Effects Meta-Analysis. Stata J. 2008, 8, 3–28. [Google Scholar] [CrossRef] [Green Version]
- Gasparrini, A. Extensions of the Dlnm Package. 2021. Available online: https://cran.r-project.org/web/packages/dlnm/vignettes/dlnmExtended.pdf (accessed on 20 June 2022).
- Ragettli, M.S.; Röösli, M. Hitzeaktionspläne zur Prävention von hitzebedingten Todesfällen–Erfahrungen aus der Schweiz (EN: Heat-health action plans to prevent heat-related deaths–experiences from Switzerland). Bundesgesundheitsblatt 2019, 62, 605–611. [Google Scholar] [CrossRef] [PubMed]
- Sanchez Martinez, G.; Linares, C.; Ayuso, A.; Kendrovski, V.; Boeckmann, M.; Diaz, J. Heat-health action plans in Europe: Challenges ahead and how to tackle them. Environ. Res. 2019, 176, 108548. [Google Scholar] [CrossRef]
- Swiss Union of Cities (SSV); Federal Statistical Office (FSO). Statistics on Swiss Cities 2020 (German Title: Statistik der Schweizer Städte 2020). 2020. Available online: https://www.bfs.admin.ch/bfs/de/home/statistiken/kataloge-datenbanken/publikationen.assetdetail.12767482.html (accessed on 11 April 2022).
- Hajat, S.; Armstrong, B.; Baccini, M.; Biggeri, A.; Bisanti, L.; Russo, A.; Paldy, A.; Menne, B.; Kosatsky, T. Impact of high temperatures on mortality: Is there an added heat wave effect? Epidemiology 2006, 17, 632–638. [Google Scholar] [CrossRef]
- Cheng, Y.-T.; Lung, S.-C.C.; Hwang, J.-S. New approach to identifying proper thresholds for a heat warning system using health risk increments. Environ. Res. 2019, 170, 282–292. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Gu, S.; Bi, P.; Yang, J.; Liu, Q. Heat Waves and Morbidity: Current Knowledge and Further Direction-A Comprehensive Literature Review. Int. J. Environ. Res. Public Health 2015, 12, 5256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, J.; Varghese, B.M.; Hansen, A.; Xiang, J.; Zhang, Y.; Dear, K.; Gourley, M.; Driscoll, T.; Morgan, G.; Capon, A.; et al. Is there an association between hot weather and poor mental health outcomes? A systematic review and meta-analysis. Environ. Int. 2021, 153, 106533. [Google Scholar] [CrossRef] [PubMed]
- Vicedo-Cabrera, A.M.; Sera, F.; Liu, C.; Armstrong, B.; Milojevic, A.; Guo, Y.; Tong, S.; Lavigne, E.; Kyselý, J.; Urban, A.; et al. Short term association between ozone and mortality: Global two stage time series study in 406 locations in 20 countries. BMJ 2020, 368, m108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buckley, J.P.; Samet, J.M.; Richardson, D.B. Commentary: Does air pollution confound studies of temperature? Epidemiology 2014, 25, 242–245. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, B.; Sera, F.; Vicedo-Cabrera, A.M.; Abrutzky, R.; Åström, D.O.; Bell, M.L.; Chen, B.-Y.; de Sousa Zanotti Stagliorio Coelho, M.; Correa, P.M.; Dang, T.N.; et al. The role of humidity in associations of high temperature with mortality: A multicountry, multicity study. Environ. Health Perspect. 2019, 127, 097007. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Deaths 1 | Tmean (°C) 2 | Tmax (°C) | Tmin (°C) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n (%) | p5 | p50 | p98 | p99 | p5 | p50 | p98 | p99 | p5 | p50 | p98 | p99 | ||
| Switzerland | 300,295 | (100) | 10.1 | 17.0 | 25.0 | 25.9 | 13.8 | 22.4 | 32.5 | 33.6 | 6.0 | 12.3 | 18.5 | 19.1 |
| Period 2003–2009 3 | 149,989 | (50) | 10.2 | 17.1 | 24.9 | 25.7 | 14.0 | 22.5 | 32.4 | 33.7 | 5.9 | 12.4 | 18.3 | 18.9 |
| Period 2010–2016 3 | 150,306 | (50) | 10.0 | 16.9 | 25.2 | 26.0 | 13.6 | 22.3 | 32.6 | 33.6 | 6.1 | 12.2 | 18.6 | 19.3 |
| Nordwestern Switzerland | 41,583 | (14) | 11.1 | 17.6 | 25.5 | 26.5 | 14.8 | 23.2 | 33.5 | 34.6 | 6.7 | 12.8 | 18.6 | 19.1 |
| Espace Mittelland | 72,619 | (24) | 9.8 | 16.5 | 24.4 | 25.3 | 13.6 | 22.0 | 32.1 | 33.3 | 5.6 | 11.8 | 17.8 | 18.4 |
| Zurich | 50,462 | (17) | 10.4 | 17.1 | 25.2 | 26.0 | 13.8 | 22.4 | 32.8 | 33.9 | 6.4 | 12.6 | 18.4 | 18.9 |
| Central Switzerland | 25,785 | (9) | 9.6 | 16.5 | 24.3 | 25.1 | 13.1 | 21.6 | 31.7 | 32.7 | 5.8 | 12.0 | 17.9 | 18.4 |
| Estern Switzerland | 42,582 | (14) | 8.8 | 16.0 | 24.1 | 24.9 | 12.5 | 21.1 | 31.5 | 32.6 | 5.0 | 11.6 | 17.6 | 18.1 |
| Lake Geneva region | 53,419 | (18) | 10.7 | 17.6 | 25.5 | 26.5 | 14.8 | 23.1 | 32.7 | 33.9 | 6.5 | 12.8 | 19.1 | 19.8 |
| Ticino | 13,845 | (5) | 12.8 | 19.1 | 25.9 | 26.6 | 17.0 | 24.9 | 32.7 | 33.5 | 8.5 | 14.3 | 19.9 | 20.6 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ragettli, M.S.; Saucy, A.; Flückiger, B.; Vienneau, D.; de Hoogh, K.; Vicedo-Cabrera, A.M.; Schindler, C.; Röösli, M. Explorative Assessment of the Temperature–Mortality Association to Support Health-Based Heat-Warning Thresholds: A National Case-Crossover Study in Switzerland. Int. J. Environ. Res. Public Health 2023, 20, 4958. https://doi.org/10.3390/ijerph20064958
Ragettli MS, Saucy A, Flückiger B, Vienneau D, de Hoogh K, Vicedo-Cabrera AM, Schindler C, Röösli M. Explorative Assessment of the Temperature–Mortality Association to Support Health-Based Heat-Warning Thresholds: A National Case-Crossover Study in Switzerland. International Journal of Environmental Research and Public Health. 2023; 20(6):4958. https://doi.org/10.3390/ijerph20064958
Chicago/Turabian StyleRagettli, Martina S., Apolline Saucy, Benjamin Flückiger, Danielle Vienneau, Kees de Hoogh, Ana M. Vicedo-Cabrera, Christian Schindler, and Martin Röösli. 2023. "Explorative Assessment of the Temperature–Mortality Association to Support Health-Based Heat-Warning Thresholds: A National Case-Crossover Study in Switzerland" International Journal of Environmental Research and Public Health 20, no. 6: 4958. https://doi.org/10.3390/ijerph20064958