
Suicide Mortality Risk among Patients with Lung Cancer—A Systematic Review and Meta-Analysis
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria, Systematic Literature Search, and Data Extraction
2.2. Statistical Analyses
3. Results
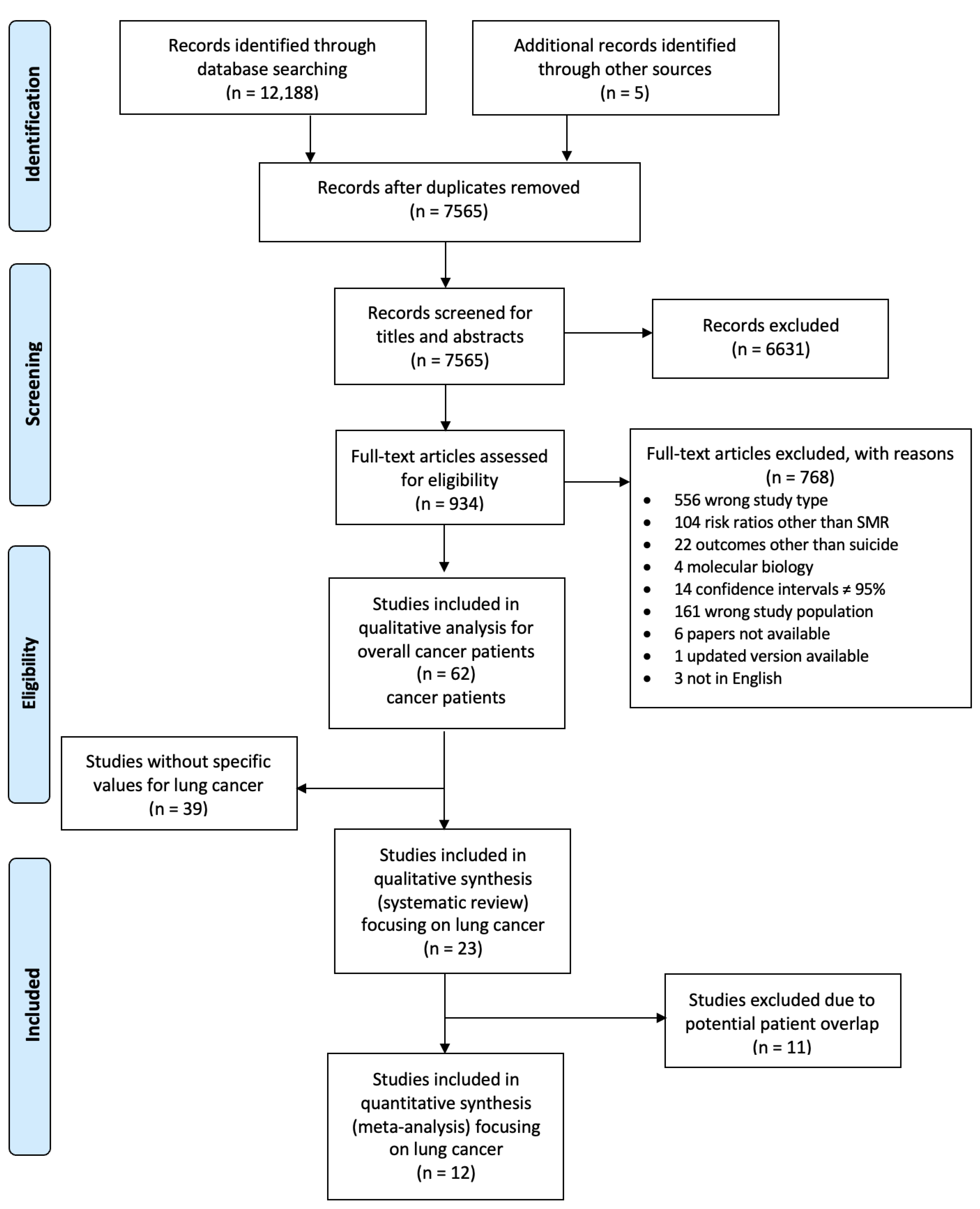
3.1. Study Selection and Characteristics
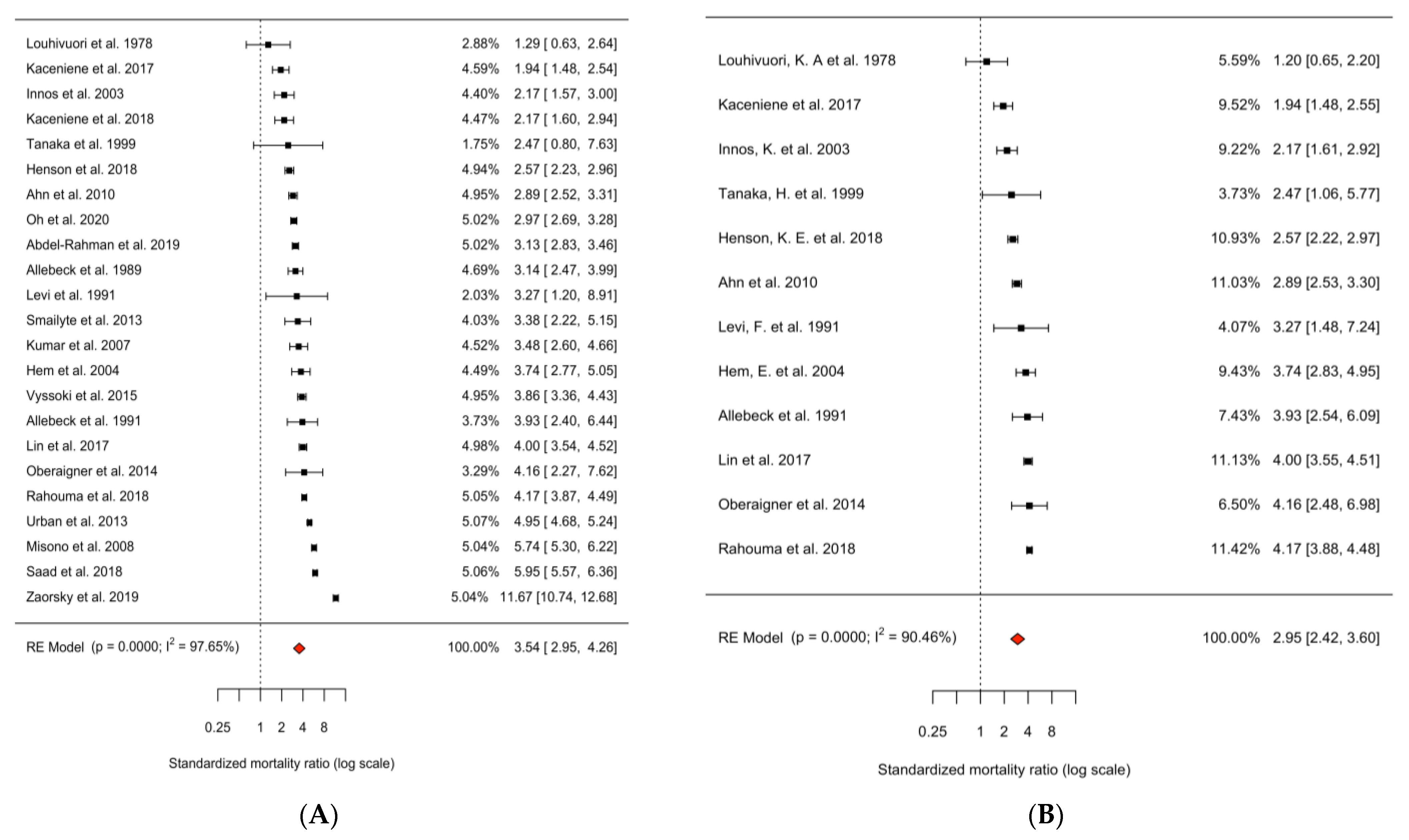
3.2. Main Analysis
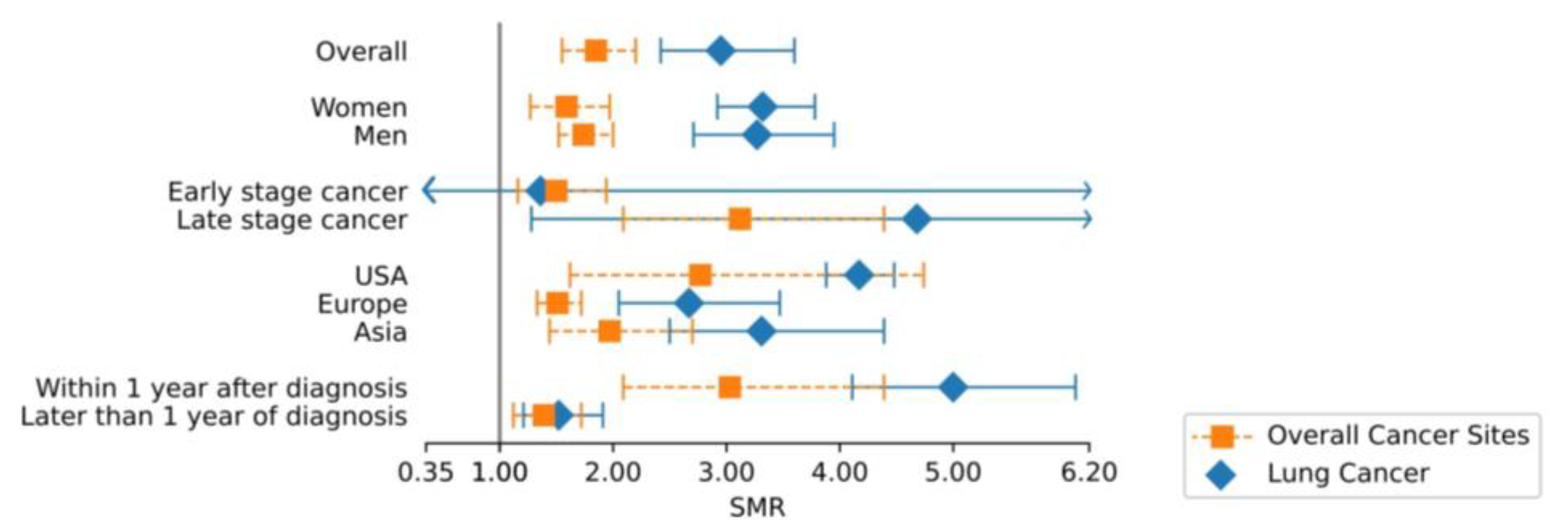
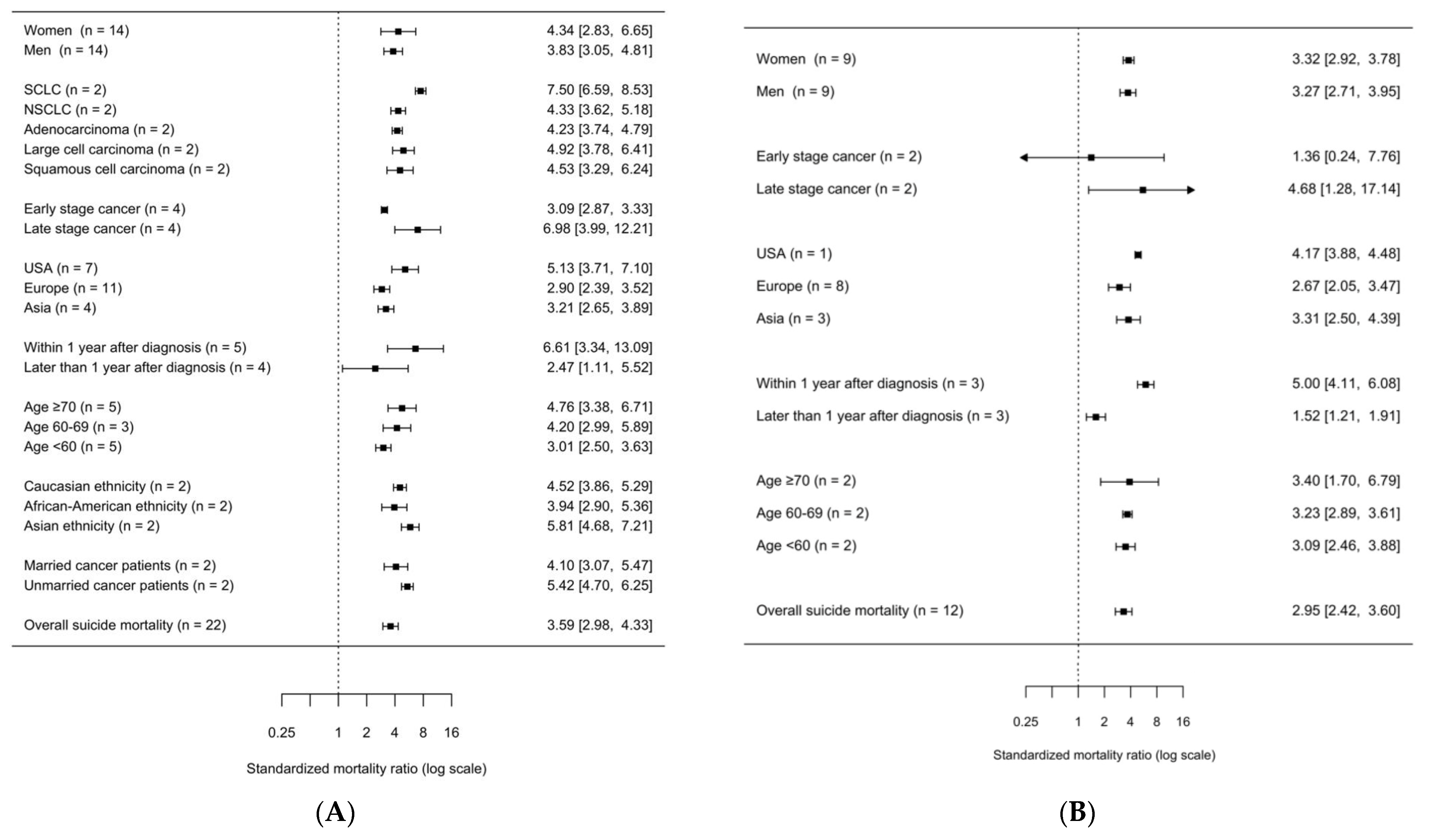
3.3. Subgroup Analyses
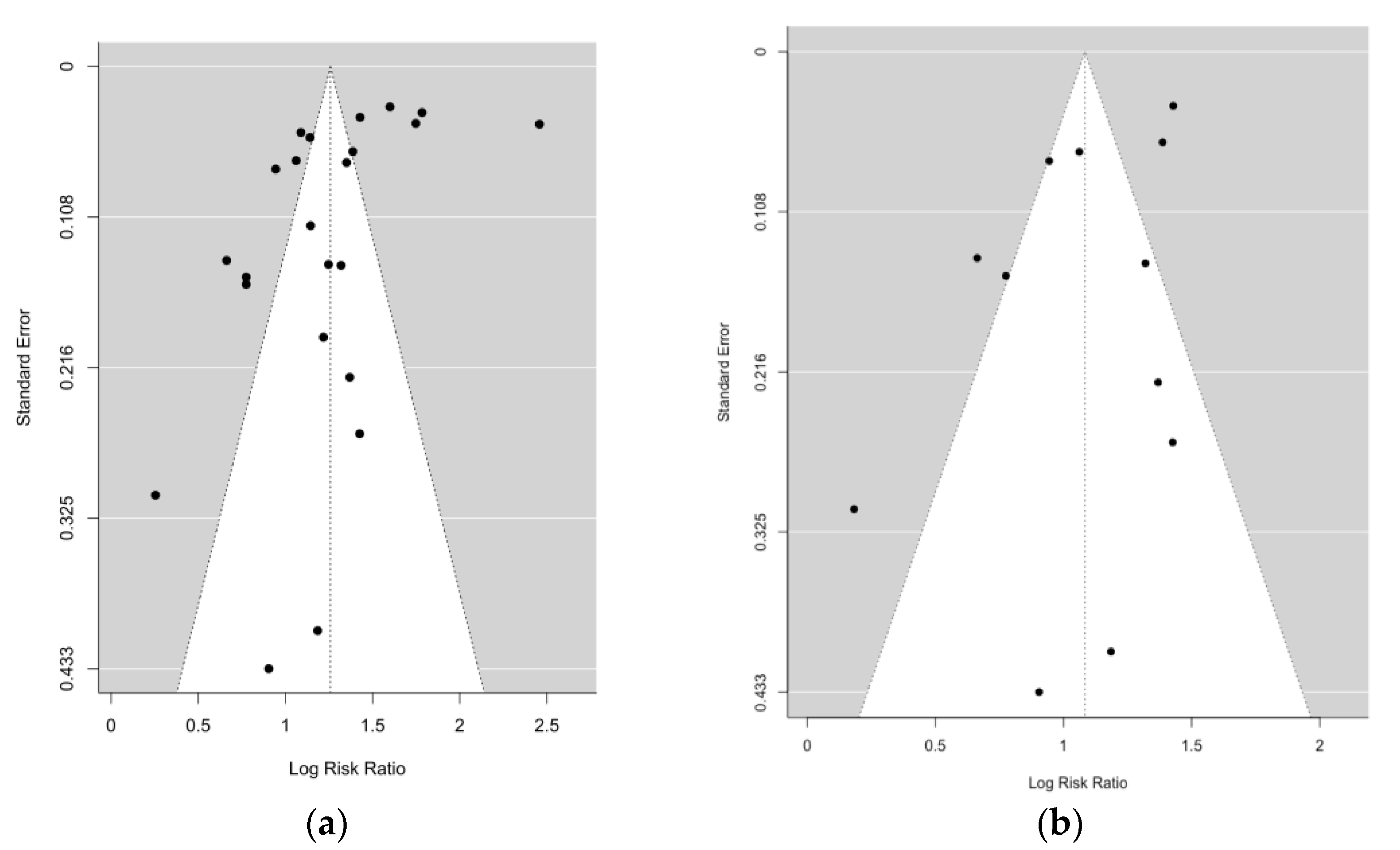
3.4. Assessment of Publication Bias and Study Quality
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

Appendix B

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Co-Variable | SMR | 95% CI | p-Value | q-Value | |
|---|---|---|---|---|---|
| Sex | 0.03 | 0.38 | |||
| women | 3.32 | 2.92–3.78 | 0.61 | ||
| men | 3.27 | 2.71–3.95 | - | ||
| Stage | 0.027 | 0.38 | |||
| early stage cancer | 1.36 | 0.24–7.76 | 0.67 | ||
| late stage cancer | 4.68 | 1.28–17.14 | 0.27 | ||
| Region | 0.03 | 0.38 | |||
| USA | 4.17 | 3.88–4.48 | 0.15 | ||
| Europe | 2.67 | 2.05–3.47 | - | ||
| Asia | 3.31 | 2.50–4.39 | 0.38 | ||
| Time after diagnosis | <0.001 | <0.001 | |||
| Within 1 year after diagnosis | 5.00 | 4.11–6.08 | <0.001 | ||
| Later than 1 year after diagnosis | 1.52 | 1.21–1.91 | - | ||
| Age | 0.09 | 0.91 | |||
| >70 | 3.40 | 1.70–6.79 | 0.68 | ||
| 60–69 | 3.23 | 2.89–3.61 | 0.89 | ||
| <60 | 3.09 | 2.46–3.88 | - |
References
- Carlson, L.E.; Zelinski, E.L.; Toivonen, K.I.; Sundstrom, L.; Jobin, C.T.; Damaskos, P.; Zebrack, B. Prevalence of psychosocial distress in cancer patients across 55 North American cancer centers. J. Psychosoc. Oncol. 2019, 37, 5–21. [Google Scholar] [CrossRef] [PubMed]
- Krebber, A.M.; Buffart, L.M.; Kleijn, G.; Riepma, I.C.; de Bree, R.; Leemans, C.R.; Becker, A.; Brug, J.; van Straten, A.; Cuijpers, P.; et al. Prevalence of depression in cancer patients: A meta-analysis of diagnostic interviews and self-report instruments. Psychooncology 2014, 23, 121–130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mitchell, A.J.; Chan, M.; Bhatti, H.; Halton, M.; Grassi, L.; Johansen, C.; Meader, N. Prevalence of depression, anxiety, and adjustment disorder in oncological, haematological, and palliative-care settings: A meta-analysis of 94 interview-based studies. Lancet Oncol. 2011, 12, 160–174. [Google Scholar] [CrossRef] [PubMed]
- Heinrich, M.; Hofmann, L.; Baurecht, H.; Kreuzer, P.M.; Knüttel, H.; Leitzmann, M.F.; Seliger, C. Suicide risk and mortality among patients with cancer. Nat. Med. 2022, 28, 852–859. [Google Scholar] [CrossRef]
- Zabora, J.; Brintzenhofeszoc, K.; Curbow, B.; Hooker, C.; Piantadosi, S. The Prevalence of Psychological Distress by Cancer Site. Psycho-Oncol. 2001, 10, 19–28. [Google Scholar] [CrossRef]
- Ahn, E.; Shin, D.W.; Cho, S.I.; Park, S.; Won, Y.J.; Yun, Y.H. Suicide rates and risk factors among Korean cancer patients, 1993-2005. Cancer Epidemiol. Biomark. Prev. 2010, 19, 2097–2105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Innos, K.; Rahu, K.; Rahu, M.; Baburin, A. Suicides among cancer patients in Estonia: A population-based study. Eur. J. Cancer 2003, 39, 2223–2228. [Google Scholar] [CrossRef]
- Oberaigner, W.; Sperner-Unterweger, B.; Fiegl, M.; Geiger-Gritsch, S.; Haring, C. Increased suicide risk in cancer patients in Tyrol/Austria. Gen. Hosp. Psychiatry 2014, 36, 483–487. [Google Scholar] [CrossRef]
- Saad, A.M.; Gad, M.M.; Al-Husseini, M.J.; AlKhayat, M.A.; Rachid, A.; Alfaar, A.S.; Hamoda, H.M. Suicidal death within a year of a cancer diagnosis: A population-based study. Cancer 2019, 125, 972–979. [Google Scholar] [CrossRef]
- Levi, F.; Bulliard, J.L.; La Vecchia, C. Suicide risk among incident cases of cancer in the Swiss Canton of Vaud. Oncology 1991, 48, 44–47. [Google Scholar] [CrossRef]
- Allebeck, P.; Bolund, C.; Ringback, G. Increased suicide rate in cancer patients. A cohort study based on the Swedish Cancer-Environment Register. J. Clin. Epidemiol. 1989, 42, 611–616. [Google Scholar] [CrossRef] [PubMed]
- Misono, S.; Weiss, N.S.; Fann, J.R.; Redman, M.; Yueh, B. Incidence of suicide in persons with cancer. J. Clin. Oncol. 2008, 26, 4731–4738. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Torre, L.A.; Bray, F.; Siegel, R.L.; Ferlay, J.; Lortet-Tieulent, J.; Jemal, A. Global cancer statistics, 2012. CA Cancer J. Clin. 2015, 65, 87–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Noone, A.M.H.N.; Krapcho, M.; Miller, D.; Brest, A.; Yu, M.; Ruhl, J.; Tatalovich, Z.; Mariotto, A.; Lewis, D.R.; Chen, H.S.; et al. SEER Cancer Statistics Review, 1975–2015; National Cancer Institute: Bethesda, MD, USA, 2017.
- Latimer, K.; Mott, T. Lung cancer: Diagnosis, treatment principles, and screening. Am. Fam. Phys. 2015, 91, 250–256. [Google Scholar]
- Rahouma, M.; Kamel, M.; Abouarab, A.; Eldessouki, I.; Nasar, A.; Harrison, S.; Lee, B.; Shostak, E.; Morris, J.; Stiles, B.; et al. Lung cancer patients have the highest malignancy-associated suicide rate in USA: A population-based analysis. Ecancermedicalscience 2018, 12, 859. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McGowan, J.; Sampson, M.; Salzwedel, D.M.; Cogo, E.; Foerster, V.; Lefebvre, C. PRESS Peer Review of Electronic Search Strategies: 2015 Guideline Statement. J. Clin. Epidemiol. 2016, 75, 40–46. [Google Scholar] [CrossRef] [Green Version]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B. Meta-analysis of observational studies in epidemiology: A proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. Jama 2000, 283, 2008–2012. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Rethlefsen, M.L.; Kirtley, S.; Waffenschmidt, S.; Ayala, A.P.; Moher, D.; Page, M.J.; Koffel, J.B. PRISMA-S: An extension to the PRISMA statement for reporting literature searches in systematic reviews. Syst. Rev. 2021, 10, 1–19. [Google Scholar] [CrossRef]
- Bramer, W.M.; Giustini, D.; de Jonge, G.B.; Holland, L.; Bekhuis, T. De-duplication of database search results for systematic reviews in EndNote. J. Med. Libr. Assoc. JMLA 2016, 104, 240–243. [Google Scholar] [CrossRef]
- Wells, G.; Shea, B.; OConnell, D.L.; Peterson, J.; Welch Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. 2014. Available online: https://www.semanticscholar.org/paper/The-Newcastle-Ottawa-Scale-(NOS)-for-Assessing-the-Wells-Wells/c293fb316b6176154c3fdbb8340a107d9c8c82bf (accessed on 1 August 2022).
- Lunny, C.; Pieper, D.; Thabet, P.; Kanji, S. Managing overlap of primary study results across systematic reviews: Practical considerations for authors of overviews of reviews. BMC Med. Res. Methodol. 2021, 21, 140. [Google Scholar] [CrossRef]
- Cohen, G.R.; Yang, S.Y. Mid-P confidence intervals for the Poisson expectation. Stat. Med. 1994, 13, 2189–2203. [Google Scholar] [CrossRef] [PubMed]
- Viechtbauer, W. Conducting Meta-Analyses in R with the metafor Package. J. Stat. Softw. 2010, 36, 1–48. [Google Scholar] [CrossRef] [Green Version]
- Benjamini, Y.; Hochberg, Y. Controlling the False Discovery Rate: A Practical and Powerful Approach to Multiple Testing. J. R. Stat. Soc. Ser. B (Methodol.) 1995, 57, 289–300. [Google Scholar] [CrossRef]
- Begg, C.B.; Mazumdar, M. Operating characteristics of a rank correlation test for publication bias. Biometrics 1994, 50, 1088–1101. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. Bmj 1997, 315, 629–634. [Google Scholar] [CrossRef] [Green Version]
- R Development Core Team, R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2018.
- Allebeck, P.; Bolund, C. Suicides and suicide attempts in cancer patients. Psychol. Med. 1991, 21, 979–984. [Google Scholar] [CrossRef]
- Hem, E.; Loge, J.H.; Haldorsen, T.; Ekeberg, O. Suicide risk in cancer patients from 1960 to 1999. J. Clin. Oncol. 2004, 22, 4209–4216. [Google Scholar] [CrossRef]
- Kaceniene, A.; Krilaviciute, A.; Kazlauskiene, J.; Bulotiene, G.; Smailyte, G. Increasing suicide risk among cancer patients in Lithuania from 1993 to 2012, a cancer registry-based study. Eur. J. Cancer Prev. 2017, 26, S197–S203. [Google Scholar] [CrossRef]
- Lin, P.H.; Liao, S.C.; Chen, I.M.; Kuo, P.H.; Shan, J.C.; Lee, M.B.; Chen, W.J. Impact of universal health coverage on suicide risk in newly diagnosed cancer patients: Population-based cohort study from 1985 to 2007 in Taiwan. Psycho-Oncol. 2017, 26, 1852–1859. [Google Scholar] [CrossRef]
- Louhivuori, K.A.; Hakama, M. Risk of suicide among cancer patients. Am. J. Epidemiol. 1979, 109, 59–65. [Google Scholar] [CrossRef]
- Smailyte, G.; Jasilionis, D.; Kaceniene, A.; Krilaviciute, A.; Ambrozaitiene, D.; Stankuniene, V. Suicides among cancer patients in Lithuania: A population-based census-linked study. Cancer Epidemiol. 2013, 37, 714–718. [Google Scholar] [CrossRef]
- Urban, D.; Rao, A.; Bressel, M.; Neiger, D.; Solomon, B.; Mileshkin, L. Suicide in lung cancer: Who is at risk? Chest 2013, 144, 1245–1252. [Google Scholar] [CrossRef]
- Vyssoki, B.; Gleiss, A.; Rockett, I.R.; Hackl, M.; Leitner, B.; Sonneck, G.; Kapusta, N.D. Suicide among 915,303 Austrian cancer patients: Who is at risk? J. Affect. Disord. 2015, 175, 287–291. [Google Scholar] [CrossRef] [PubMed]
- Zaorsky, N.G.; Zhang, Y.; Tuanquin, L.; Bluethmann, S.M.; Park, H.S.; Chinchilli, V.M. Suicide among cancer patients. Nat. Commun. 2019, 10, 207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdel-Rahman, O. Socioeconomic predictors of suicide risk among cancer patients in the United States: A population-based study. Cancer Epidemiol. 2019, 63, 101601. [Google Scholar] [CrossRef] [PubMed]
- Kumar, V.; Chaudhary, N.; Soni, P.; Jha, P. Suicide rates in cancer patients in the current era in United States. Am. J. Psychiatry Resid. J. 2017, 12, 11–14. [Google Scholar] [CrossRef] [Green Version]
- Oh, C.M.; Lee, D.; Kong, H.J.; Lee, S.; Won, Y.J.; Jung, K.W.; Cho, H. Causes of death among cancer patients in the era of cancer survivorship in Korea: Attention to the suicide and cardiovascular mortality. Cancer Med. 2020, 9, 1741–1752. [Google Scholar] [CrossRef] [Green Version]
- Henson, K.E.; Brock, R.; Charnock, J.; Wickramasinghe, B.; Will, O.; Pitman, A. Risk of Suicide After Cancer Diagnosis in England. JAMA Psychiatry 2019, 76, 51–60. [Google Scholar] [CrossRef] [Green Version]
- Tanaka, H.; Tsukuma, H.; Masaoka, T.; Ajiki, W.; Koyama, Y.; Kinoshita, N.; Hasuo, S.; Oshima, A. Suicide risk among cancer patients: Experience at one medical center in Japan, 1978–1994. Jpn. J. Cancer Res. 1999, 90, 812–817. [Google Scholar] [CrossRef]
- Kaceniene, A.; Danila, E.; Cicenas, S.; Smailyte, G. Suicide risk among lung cancer patients in Lithuania. Clin. Respir. J. 2018, 12, 2455–2456. [Google Scholar] [CrossRef]
- De Angelis, R.; Sant, M.; Coleman, M.P.; Francisci, S.; Baili, P.; Pierannunzio, D.; Trama, A.; Visser, O.; Brenner, H.; Ardanaz, E.; et al. Cancer survival in Europe 1999–2007 by country and age: Results of EUROCARE--5-a population-based study. Lancet Oncol. 2014, 15, 23–34. [Google Scholar] [CrossRef] [PubMed]
- Haas, M. Contemporary Issues in Lung Cancer; Jones & Bartlett Learning: Burlington, MA, USA, 2010. [Google Scholar]
- Beckles, M.A.; Spiro, S.G.; Colice, G.L.; Rudd, R.M. Initial evaluation of the patient with lung cancer: Symptoms, signs, laboratory tests, and paraneoplastic syndromes. Chest 2003, 123, 97s–104s. [Google Scholar] [CrossRef] [Green Version]
- Schag, C.A.C.; Ganz, P.A.; Wing, D.S.; Sim, M.S.; Lee, J.J. Quality of life in adult survivors of lung, colon and prostate cancer. Qual. Life Res. 1994, 3, 127–141. [Google Scholar] [CrossRef] [PubMed]
- Hewitt, M.; Rowland, J.H.; Yancik, R. Cancer survivors in the United States: Age, health, and disability. J. Gerontol. A Biol. Sci. Med. Sci. 2003, 58, 82–91. [Google Scholar] [CrossRef] [PubMed]
- Spoletini, I.; Gianni, W.; Caltagirone, C.; Madaio, R.; Repetto, L.; Spalletta, G. Suicide and cancer: Where do we go from here? Crit. Rev. Oncol. Hematol. 2011, 78, 206–219. [Google Scholar] [CrossRef] [PubMed]
- LoConte, N.K.; Else-Quest, N.M.; Eickhoff, J.; Hyde, J.; Schiller, J.H. Assessment of guilt and shame in patients with non-small-cell lung cancer compared with patients with breast and prostate cancer. Clin. Lung Cancer 2008, 9, 171–178. [Google Scholar] [CrossRef] [Green Version]
- West, E.; Barron, D.N.; Reeves, R. Overcoming the barriers to patient-centred care: Time, tools and training. J. Clin. Nurs. 2005, 14, 435–443. [Google Scholar] [CrossRef]
- Valente, S.M. Oncology nurses’ knowledge of suicide evaluation and prevention. Cancer Nurs. 2010, 33, 290–295. [Google Scholar] [CrossRef] [PubMed]
- Chapple, A.; Ziebland, S.; McPherson, A. Stigma, shame, and blame experienced by patients with lung cancer: Qualitative study. Bmj 2004, 328, 1470. [Google Scholar] [CrossRef] [Green Version]
- Weiss, J.; Yang, H.; Weiss, S.; Rigney, M.; Copeland, A.; King, J.C.; Deal, A. Stigma, self-blame, and satisfaction with care among patients with lung cancer. J. Psychosoc. Oncol. 2017, 35, 166–179. [Google Scholar] [CrossRef]
- Glynn, R.W.; Kelly, J.C.; Coffey, N.; Sweeney, K.J.; Kerin, M.J. The effect of breast cancer awareness month on internet search activity--a comparison with awareness campaigns for lung and prostate cancer. BMC Cancer 2011, 11, 442. [Google Scholar] [CrossRef] [Green Version]
- Cataldo, J.K.; Brodsky, J.L. Lung cancer stigma, anxiety, depression and symptom severity. Oncology 2013, 85, 33–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kapusta, N.; Sonneck, G. Suicides in Austria: Update on present state and recent trends. Neuropsychiatrie 2012, 26, 103–105. [Google Scholar] [CrossRef]
- Liu, N.S.; Spitz, M.R.; Kemp, B.L.; Cooksley, C.; Fossella, F.V.; Lee, J.S.; Hong, W.K.; Khuri, F.R. Adenocarcinoma of the lung in young patients: The MD Anderson experience. Cancer Interdiscip. Int. J. Am. Cancer Soc. 2000, 88, 1837–1841. [Google Scholar] [CrossRef]
- Akechi, T.; Okuyama, T.; Akizuki, N.; Azuma, H.; Sagawa, R.; Furukawa, T.A.; Uchitomi, Y. Course of psychological distress and its predictors in advanced non-small cell lung cancer patients. Psycho-Oncol. 2006, 15, 463–473. [Google Scholar] [CrossRef] [PubMed]
- Kantarjian, H.; Steensma, D.; Rius Sanjuan, J.; Elshaug, A.; Light, D. High cancer drug prices in the United States: Reasons and proposed solutions. J. Oncol. Pract. 2014, 10, e208–e211. [Google Scholar] [CrossRef]
- Kantarjian, H. Does the United States have the best health-care system in the world? ASCO Post 2014, 5, 1. [Google Scholar]
- Light, D.W.; Lexchin, J. Foreign free riders and the high price of US medicines. Bmj 2005, 331, 958–960. [Google Scholar] [CrossRef] [Green Version]
- Davis, K.; Stremikis, K.; Schoen, C.; Squires, D. Mirror, mirror on the wall, 2014 update: How the US health care system compares internationally. Commonw. Fund 2014, 16, 1–15. [Google Scholar] [CrossRef]
- Nolte, E.; McKee, M. Variations in amenable mortality—Trends in 16 high-income nations. Health Policy 2011, 103, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Hillner, B.E.; Smith, T.J. Efficacy does not necessarily translate to cost effectiveness: A case study in the challenges associated with 21st-century cancer drug pricing. J. Clin. Oncol. 2009, 27. [Google Scholar] [CrossRef] [PubMed]
- Riley, G.F.; Potosky, A.L.; Lubitz, J.D.; Kessler, L.G. Medicare Payments from Diagnosis to Death for Elderly Cancer Patients by Stage at Diagnosis. Med. Care 1995, 33, 828–841. [Google Scholar] [CrossRef] [PubMed]
- Lang, H.-C.; Wu, S.-L. Lifetime costs of the top five cancers in Taiwan. Eur. J. Health Econ. 2012, 13, 347–353. [Google Scholar] [CrossRef]
- Popper, H.H. Progression and metastasis of lung cancer. Cancer Metastasis Rev. 2016, 35, 75–91. [Google Scholar] [CrossRef] [Green Version]
- Akechi, T.; Okamura, H.; Nishiwaki, Y.; Uchitomi, Y. Predictive factors for suicidal ideation in patients with unresectable lung carcinoma. Cancer 2002, 95, 1085–1093. [Google Scholar] [CrossRef]
- Shen, K.; Xu, Y.; Guan, H.; Zhong, W.; Chen, M.; Zhao, J.; Li, L.; Wang, M. Paraneoplastic limbic encephalitis associated with lung cancer. Sci. Rep. 2018, 8, 6792. [Google Scholar] [CrossRef] [Green Version]
- Tüzün, E.; Dalmau, J. Limbic Encephalitis and Variants: Classification, Diagnosis and Treatment. Neurol. 2007, 13, 261–271. [Google Scholar] [CrossRef]
- Radzikowska, E.; Głaz, P.; Roszkowski, K. Lung cancer in women: Age, smoking, histology, performance status, stage, initial treatment and survival. Population-based study of 20 561 cases. Ann. Oncol. 2002, 13, 1087–1093. [Google Scholar] [CrossRef]
- Sobue, T.; Yamamoto, S.; Hara, M.; Sasazuki, S.; Sasaki, S.; Tsugane, S.; JPHC Study Group; Japanese Public Health Center. Cigarette smoking and subsequent risk of lung cancer by histologic type in middle-aged Japanese men and women: The JPHC study. Int. J. Cancer 2002, 99, 245–251. [Google Scholar] [CrossRef]
- Sun, S.; Schiller, J.H.; Gazdar, A.F. Lung cancer in never smokers—A different disease. Nat. Rev. Cancer 2007, 7, 778–790. [Google Scholar] [CrossRef] [PubMed]
- Toh, C.K.; Gao, F.; Lim, W.T.; Leong, S.S.; Fong, K.W.; Yap, S.P.; Hsu, A.A.; Eng, P.; Koong, H.N.; Thirugnanam, A.; et al. Never-smokers with lung cancer: Epidemiologic evidence of a distinct disease entity. J. Clin. Oncol. 2006, 24, 2245–2251. [Google Scholar] [CrossRef]
- Khuder, S.A. Effect of cigarette smoking on major histological types of lung cancer: A meta-analysis. Lung Cancer 2001, 31, 139–148. [Google Scholar] [CrossRef] [PubMed]
- Milic, M.; Gazibara, T.; Pekmezovic, T.; Kisic Tepavcevic, D.; Maric, G.; Popovic, A.; Stevanovic, J.; Patil, K.H.; Levine, H. Tobacco smoking and health-related quality of life among university students: Mediating effect of depression. PLoS ONE 2020, 15, e0227042. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farrell, M.; Howes, S.; Taylor, C.; Lewis, G.; Jenkins, R.; Bebbington, P.; Jarvis, M.; Brugha, T.; Gill, B.; Meltzer, H. Substance misuse and psychiatric comorbidity: An overview of the OPCS National Psychiatric Morbidity Survey. Addict. Behav. 1998, 23, 909–918. [Google Scholar] [CrossRef]
- McNeill, A. (Ed.) Symposium Report: Smoking and Mental Health Smoke-Fee London; 2001: Citeseer. Available online: https://citeseerx.ist.psu.edu/document?repid=rep1&type=pdf&doi=54e6f90d69b2e3dd768c40600bac0f526f3a2b01 (accessed on 1 August 2022).
- de Leon, J.; Diaz, F.J. A meta-analysis of worldwide studies demonstrates an association between schizophrenia and tobacco smoking behaviors. Schizophr. Res. 2005, 76, 135–157. [Google Scholar] [CrossRef]
- Caldwell, C.B.; Gottesman, I.I. Schizophrenics kill themselves too: A review of risk factors for suicide. Schizophr. Bull 1990, 16, 571–589. [Google Scholar] [CrossRef] [Green Version]
- Bronisch, T.; Höfler, M.; Lieb, R. Smoking predicts suicidality: Findings from a prospective community study. J. Affect. Disord. 2008, 108, 135–145. [Google Scholar] [CrossRef]
- Gandini, S.; Botteri, E.; Iodice, S.; Boniol, M.; Lowenfels, A.B.; Maisonneuve, P.; Boyle, P. Tobacco smoking and cancer: A meta-analysis. Int. J. Cancer 2008, 122, 155–164. [Google Scholar] [CrossRef]
- Carter, B.W.; Glisson, B.S.; Truong, M.T.; Erasmus, J.J. Small Cell Lung Carcinoma: Staging, Imaging, and Treatment Considerations. Radio Graph. 2014, 34, 1707–1721. [Google Scholar] [CrossRef]
- Hodkinson, P.S.; Mackinnon, A.C.; Sethi, T. Extracellular matrix regulation of drug resistance in small-cell lung cancer. Int. J. Radiat. Biol. 2007, 83, 733–741. [Google Scholar] [CrossRef]
- Sculier, J.-P.; Chansky, K.; Crowley, J.J.; Van Meerbeeck, J.; Goldstraw, P. The Impact of Additional Prognostic Factors on Survival and their Relationship with the Anatomical Extent of Disease Expressed by the 6th Edition of the TNM Classification of Malignant Tumors and the Proposals for the 7th Edition. J. Thorac. Oncol. 2008, 3, 457–466. [Google Scholar] [CrossRef] [PubMed]
- Van der Sluis, J.; Van Praag, M.; Vijverberg, W. Entrepreneurship selection and performance: A meta-analysis of the impact of education in developing economies. World Bank Econ. Rev. 2005, 19, 225–261. [Google Scholar] [CrossRef] [Green Version]
- Havránek, T. Measuring intertemporal substitution: The importance of method choices and selective reporting. J. Eur. Econ. Assoc. 2015, 13, 1180–1204. [Google Scholar] [CrossRef]
- Stanley, T.D. New wine in old bottles: A meta-analysis of Ricardian equivalence. South. Econ. J. 1998, 64, 713–727. [Google Scholar] [CrossRef]
- Van den Noortgate, W.; López-López, J.A.; Marín-Martínez, F.; Sánchez-Meca, J. Meta-analysis of multiple outcomes: A multilevel approach. Behav. Res. Methods 2015, 47, 1274–1294. [Google Scholar] [CrossRef]




| N | Author, Year | Time of Recruitment | SMR (95% CI) | Country | Subgroups | n Lung Cancer Patients | n Suicides | Person- Years |
|---|---|---|---|---|---|---|---|---|
| 1 | Abdel-Rahman et al. 2019 [39] | 2000–2010 | 3.13 (2.83–3.46) | USA | n.a. | 348,831 | 387 | n.a. |
| 2 | Ahn et al. 2010 [6] | 1993–2005 | 2.89 (2.52–3.30) | Korea | gender, time after diagnosis | 72,898 | 181 | n.a. |
| 3 | Allebeck et al. 1989 [11] | 1962–1979 | 3.14 (2.47–3.93) | Sweden | gender | n.a. | 71 | n.a. |
| 4 | Allebeck et al. 1991 [30] | 1975–1985 | 3.93 (2.40–6.09) | Sweden | gender | n.a. | 17 | n.a. |
| 5 | Hem et al. 2004 [31] | 1960–1997 | 3.74 (2.77–4.95) | Norway | gender | 14,567 | 46 | 56,808 |
| 6 | Henson et al. 2018 [42] | 1995–2018 | 2.57 (2.23–2.97) | England | gender | 613,772 | 184 | |
| 7 | Innos et al. 2003 [7] | 1983–1998 | 2.17 (1.57–2.92) | Estonia | gender, time after diagnosis, age | n.a. | 25 | n.a. |
| 8 | Kaceniene et al. 2017 [32] | 1993–2012 | 1.94 (1.48–2.55) | Lithuania | gender | n.a. | 51 | n.a. |
| 9 | Kaceniene et al. 2018 [44] | 1998–2012 | 2.17 (1.60–2.95) | Lithuania | gender | 19,781 | 41 | 79,124 |
| 10 | Kumar et al. 2017 [40] | 2000–2013 | 3.48 (2.6–4.6) | USA | n.a. | n.a. | 137 | n.a. |
| 11 | Levi et al. 1991 [10] | 1976–1987 | 3.27 (1.20–7.24) | Switzerland | n.a. | n.a. | 5 | n.a. |
| 12 | Lin et al. 2017 [33] | 1985–2007 | 4.00 (3.54–4.51) | Taiwan | gender | n.a. | n.a. | n.a. |
| 13 | Louhivuori et al. 1979 [34] | 1955–1965 | 1.29 (0.63–2.36) | Finland | stage | n.a. | 9 | n.a. |
| 14 | Misono et al. 2008 [12] | 1973–2002 | 5.74 (5.30–6.22) | USA | gender | 362,163 | 610 | 54,131 |
| 15 | Oberaigner et al. 2014 [8] | 1991–2010 | 4.16 (2.27–6.98) | Austria | gender | 5724 | 14 | n.a. |
| 16 | Oh et al. 2020 [41] | 2000–2016 | 2.97 (2.69–3.26) | Korea | gender | n.a. | 424 | n.a. |
| 17 | Rahouma et al. 2018 [16] | 1973–2013 | 4.17 (3.87–4.48) | USA | gender, stage, grade, marital status, ethnicity, histology | n.a. | 739 | n.a. |
| 18 | Saad et al. 2018 [9] | 2000–2014 | 5.95 (5.57–6.35) | USA | time after diagnosis, age, stage | 798,609 | 553 | n.a. |
| 19 | Smailyte et al. 2013 [35] | 2001–2009 | 3.38 (2.22–4.95) | Lithuania | gender | 1237 | 24 | 9896 |
| 20 | Tanaka et al. 1999 [43] | 1978–1994 | 2.47 (0.8–5.77) | Japan | n.a. | 2976 | 5 | |
| 21 | Urban et al. 2013 [36] | 1973–2008 | 4.95 (4.68–5.24) | USA | gender, age, stage, grade, marital status, ethnicity, histology | 87,123 | 1184 | n.a. |
| 22 | Vyssoki et al. 2015 [37] | 1983–2000 | 3.86 (3.36–4.42) | Austria | n.a. | 76,118 | 208 | 1,294,014 |
| 23 | Zaorsky et al. 2019 [38] | 1973–2014 | 11.67 (10.74–12.66) | USA | gender, time after diagnosis | n.a. | 583 | n.a. |
| Total | 1,790,027 | 5498 | 1,493,973 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hofmann, L.; Heinrich, M.; Baurecht, H.; Langguth, B.; Kreuzer, P.M.; Knüttel, H.; Leitzmann, M.F.; Seliger, C. Suicide Mortality Risk among Patients with Lung Cancer—A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2023, 20, 4146. https://doi.org/10.3390/ijerph20054146
Hofmann L, Heinrich M, Baurecht H, Langguth B, Kreuzer PM, Knüttel H, Leitzmann MF, Seliger C. Suicide Mortality Risk among Patients with Lung Cancer—A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2023; 20(5):4146. https://doi.org/10.3390/ijerph20054146
Chicago/Turabian StyleHofmann, Luisa, Michael Heinrich, Hansjörg Baurecht, Berthold Langguth, Peter M. Kreuzer, Helge Knüttel, Michael F. Leitzmann, and Corinna Seliger. 2023. "Suicide Mortality Risk among Patients with Lung Cancer—A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 20, no. 5: 4146. https://doi.org/10.3390/ijerph20054146