
Effect of Menstrual Cycle Phase on the Recovery Process of High-Intensity Interval Exercise—A Cross-Sectional Observational Study
 , , , ,
, , , ,  and
on behalf of the IronFEMME Study Group
and
on behalf of the IronFEMME Study Group
Abstract
:1. Introduction
2. Methods
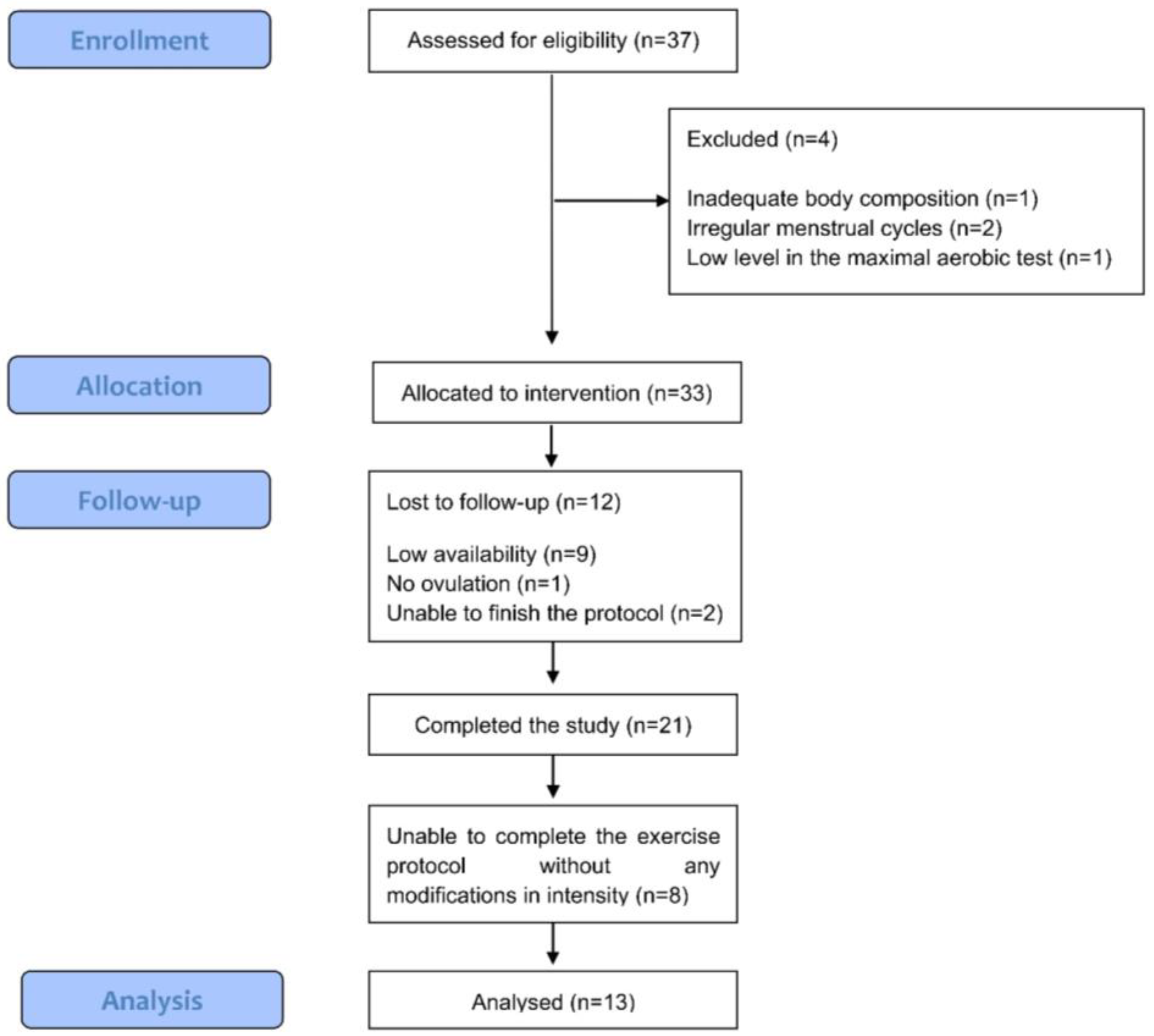
2.1. Participants
2.2. Menstrual Cycle Monitoring
2.3. Study Design
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- McNulty, K.L.; Elliott-Sale, K.J.; Dolan, E.; Swinton, P.A.; Ansdell, P.; Goodall, S.; Thomas, K.; Hicks, K.M. The effects of menstrual cycle phase on exercise performance in eumenorrheic women: A systematic review and meta-analysis. Sports Med. 2020, 50, 1813–1827. [Google Scholar] [CrossRef]
- Rael, B.; Alfaro-Magallanes, V.M.; Romero-Parra, N.; Castro, E.A.; Janse de Jonge, X.; Wehrwein, E.A.; Peinado, A.B. Menstrual Cycle Phases Influence on Cardiorespiratory Response to Exercise in Endurance-Trained Females. Int. J. Environ. Res. Public Health 2021, 18, 860. [Google Scholar] [CrossRef]
- Sims, S.T.; Heather, A.K. Myths and Methodologies: Reducing scientific design ambiguity in studies comparing sexes and/or menstrual cycle phases. Exp. Physiol. 2018, 103, 1309–1317. [Google Scholar] [CrossRef]
- Goldsmith, E.; Glaister, M. The effect of the menstrual cycle on running economy. J. Sports Med. Phys. Fitness 2020, 60, 610–617. [Google Scholar] [CrossRef]
- Barba-Moreno, L.; Cupeiro, R.; Romero-Parra, N.; Janse de Jonge, X.A.K.; Peinado, A.B. Cardiorespiratory Responses to Endurance Exercise Over the Menstrual Cycle and With Oral Contraceptive Use. J. Strength Cond Res. 2022, 36, 392–399. [Google Scholar] [CrossRef]
- Arena, R.; Guazzi, M.; Myers, J.; Peberdy, M.A. Prognostic value of heart rate recovery in patients with heart failure. Am. Heart J. 2006, 151, e7–e13. [Google Scholar] [CrossRef]
- Bilsel, T.; Terzi, S.; Akbulut, T.; Sayar, N.; Hobikoglu, G.; Yesilcimen, K. Abnormal heart rate recovery immediately after cardiopulmonary exercise testing in heart failure patients. Int. Heart J. 2006, 47, 431–440. [Google Scholar] [CrossRef]
- Legramante, J.M.; Iellamo, F.; Massaro, M.; Sacco, S.; Galante, A. Effects of residential exercise training on heart rate recovery in coronary artery patients. Am. J. Physiol. Heart Circ. Physiol. 2007, 292, H510–H515. [Google Scholar] [CrossRef] [PubMed]
- Smith, L.L.; Kukielka, M.; Billman, G.E. Heart rate recovery after exercise: A predictor of ventricular fibrillation susceptibility after myocardial infarction. Am. J. Physiol. Heart Circ. Physiol. 2005, 288, H1763–H1769. [Google Scholar] [CrossRef] [PubMed]
- Streuber, S.D.; Amsterdam, E.A.; Stebbins, C.L. Heart rate recovery in heart failure patients after a 12-week cardiac rehabilitation program. Am. J. Cardiol. 2006, 97, 694–698. [Google Scholar] [CrossRef] [PubMed]
- Dimopoulos, S.; Anastasiou-Nana, M.; Sakellariou, D.; Drakos, S.; Kapsimalakou, S.; Maroulidis, G.; Roditis, P.; Papazachou, O.; Vogiatzis, I.; Roussos, C.; et al. Effects of exercise rehabilitation program on heart rate recovery in patients with chronic heart failure. Eur. J. Cardiovasc. Prev. Rehabil. 2006, 13, 67–73. [Google Scholar] [CrossRef] [PubMed]
- Hirsh, D.S.; Vittorio, T.J.; Barbarash, S.L.; Hudaihed, A.; Tseng, C.H.; Arwady, A.; Goldsmith, R.L.; Jorde, U.P. Association of heart rate recovery and maximum oxygen consumption in patients with chronic congestive heart failure. J. Heart Lung Transplant 2006, 25, 942–945. [Google Scholar] [CrossRef]
- Huang, P.H.; Leu, H.B.; Chen, J.W.; Lin, S.J. Heart rate recovery after exercise and endothelial function—Two important factors to predict cardiovascular events. Prev. Cardiol. 2005, 8, 167–170. [Google Scholar] [CrossRef]
- Myers, J.; Tan, S.Y.; Abella, J.; Aleti, V.; Froelicher, V.F. Comparison of the chronotropic response to exercise and heart rate recovery in predicting cardiovascular mortality. Eur. J. Cardiovasc. Prev. Rehabil. 2007, 14, 215–221. [Google Scholar] [CrossRef] [PubMed]
- Gmada, N.; Bouhlel, E.; Mrizak, I.; Debabi, H.; Ben Jabrallah, M.; Tabka, Z.; Feki, Y.; Amri, M. Effect of combined active recovery from supramaximal exercise on blood lactate disappearance in trained and untrained man. Int. J. Sports Med. 2005, 26, 874–879. [Google Scholar] [CrossRef] [PubMed]
- Monedero, J.; Donne, B. Effect of recovery interventions on lactate removal and subsequent performance. Int. J. Sports Med. 2000, 21, 593–597. [Google Scholar] [CrossRef]
- Kemi, O.J.; Fowler, E.; McGlynn, K.; Primrose, D.; Smirthwaite, R.; Wilson, J. Intensity-dependence of exercise and active recovery in high-intensity interval training. J. Sports Med. Phys. Fit. 2019, 59, 1937–1943. [Google Scholar] [CrossRef]
- Calderón, F.J.; Brita, J.L.; Gonzalez, C.; Machota, V. Estudio de la recuperación en tres formas de esfuerzo intermitente: Aeróbico, umbral y anaeróbico. Apunts 1997, 55, 14–19. [Google Scholar]
- Calderón, F.J.; Brita, J.L.; Gonzalez, C.; Machota, V. Estudio de la recuperación de la frecuencia cardíaca en deportistas de élite. Selección 1997, 6, 101–105. [Google Scholar]
- Hausswirth, C.; Le Meur, Y. Physiological and nutritional aspects of post-exercise recovery: Specific recommendations for female athletes. Sports Med. 2011, 41, 861–882. [Google Scholar] [CrossRef]
- Cornelissen, V.A.; Verheyden, B.; Aubert, A.E.; Fagard, R.H. Effects of aerobic training intensity on resting, exercise and post-exercise blood pressure, heart rate and heart-rate variability. J. Human Hypertens. 2010, 24, 175–182. [Google Scholar] [CrossRef]
- Holt, A.C.; Plews, D.J.; Oberlin-Brown, K.T.; Merien, F.; Kilding, A.E. Cardiac Parasympathetic and Anaerobic Performance Recovery After High-Intensity Exercise in Rowers. Int. J. Sports Physiol. Perform. 2019, 14, 331–338. [Google Scholar] [CrossRef]
- Elliott-Sale, K.J.; Minahan, C.L.; de Jonge, X.; Ackerman, K.E.; Sipila, S.; Constantini, N.W.; Lebrun, C.M.; Hackney, A.C. Methodological Considerations for Studies in Sport and Exercise Science with Women as Participants: A Working Guide for Standards of Practice for Research on Women. Sports Med. 2021, 51, 843–861. [Google Scholar] [CrossRef] [PubMed]
- Peinado, A.B.; Alfaro-Magallanes, V.M.; Romero-Parra, N.; Barba-Moreno, L.; Rael, B.; Maestre-Cascales, C.; Rojo-Tirado, M.A.; Castro, E.A.; Benito, P.J.; Ortega-Santos, C.P.; et al. Methodological Approach of the Iron and Muscular Damage: Female Metabolism and Menstrual Cycle during Exercise Project (IronFEMME Study). Int. J. Environ. Res. Public Health 2021, 18, 735. [Google Scholar] [CrossRef] [PubMed]
- Janse de Jonge, X.; Thompson, B.; Han, A. Methodological Recommendations for Menstrual Cycle Research in Sports and Exercise. Med. Sci. Sport Exerc. 2019, 51, 2610–2617. [Google Scholar] [CrossRef] [PubMed]
- Lainé, F.; Angeli, A.; Ropert, M.; Jezequel, C.; Bardou-Jacquet, E.; Deugnier, Y.; Gissot, V.; Lacut, K.; Sacher-Huvelin, S.; Lavenu, A.; et al. Variations of hepcidin and iron-status parameters during the menstrual cycle in healthy women. Br. J. Haematol. 2016, 175, 980–982. [Google Scholar] [CrossRef] [PubMed]
- Wasserman, K.; Hansen, J.E.; Sue, D.V.; Whipp, B.J. Principles of Exercise Testing and Interpretation; Lea & Febiger: Philadelphia, PA, USA, 1987. [Google Scholar]
- Carter, J.; Jeukendrup, A.E. Validity and reliability of three commercially available breath-by-breath respiratory systems. Eur. J. Appl. Physiol. 2002, 86, 435–441. [Google Scholar] [CrossRef]
- Foss, Ø.; Hallén, J. Validity and stability of a computerized metabolic system with mixing chamber. Int. J. Sports Med. 2005, 26, 569–575. [Google Scholar] [CrossRef]
- Nakagawa, S.; Cuthill, I.C. Effect size, confidence interval and statistical significance: A practical guide for biologists. Biol. Rev. 2007, 82, 591–605. [Google Scholar] [CrossRef]
- Opina, M.T.D.; Brinkley, T.E.; Gordon, M.; Lyles, M.F.; Nicklas, B.J. Association of Breathing Reserve at Peak Exercise with Body Composition and Physical Function in Older Adults With Obesity. J. Gerontol. A Biol. Sci. Med. Sci. 2019, 74, 1973–1979. [Google Scholar] [CrossRef]
- Urquhart, D.S.; Vendrusculo, F.M. Clinical interpretation of cardiopulmonary exercise testing in cystic fibrosis and implications for exercise counselling. Paediatr. Respir. Rev. 2017, 24, 72–78. [Google Scholar] [CrossRef] [PubMed]
- Welch, H.G.; Faulkner, J.A.; Barclay, J.K.; Brooks, G.A. Ventilatory response during recovery from muscular work and its relation with O2 debt. Med. Sci. Sports 1970, 2, 15–19. [Google Scholar] [PubMed]
- Williams, T.J.; Krahenbuhl, G.S. Menstrual cycle phase and running economy. Med. Sci. Sports Exerc. 1997, 29, 1609–1618. [Google Scholar] [CrossRef]
- Constantini, N.W.; Dubnov, G.; Lebrun, C.M. The menstrual cycle and sport performance. Clin. Sports Med. 2005, 24, e51–e82. [Google Scholar] [CrossRef]
- Samsudeen, N.; Rajagopalan, A. Effect of different phases of menstrual cycle on cardio-respiratory efficiency in normal, overweight and obese female undergraduate students. J. Clin. Diagn. Res. 2016, 10, CC01. [Google Scholar] [CrossRef]
- Luthi, M.; Roach, D.E.; Beaudin, A.E.; Debert, C.T.; Sheldon, R.S.; Poulin, M.J. Effects of ovarian hormones and aging on respiratory sinus arrhythmia and breathing patterns in women. Clin. Auton. Res. 2008, 18, 134–144. [Google Scholar] [CrossRef]
- Behan, M.; Zabka, A.G.; Thomas, C.F.; Mitchell, G.S. Sex steroid hormones and the neural control of breathing. Respir. Physiol. Neurobiol. 2003, 136, 249–263. [Google Scholar] [CrossRef]
- Da Silva, S.B.; de Sousa Ramalho Viana, E.; de Sousa, M.B. Changes in peak expiratory flow and respiratory strength during the menstrual cycle. Respir. Physiol. Neurobiol. 2006, 150, 211–219. [Google Scholar] [CrossRef] [PubMed]
- Blagrove, R.C.; Bruinvels, G.; Pedlar, C.R. Variations in strength-related measures during the menstrual cycle in eumenorrheic women: A systematic review and meta-analysis. J. Sci. Med. Sport 2020, 23, 1220–1227. [Google Scholar] [CrossRef]
- Collins, S.; Phillips, D.B.; Brotto, A.R.; Rampuri, Z.H.; Stickland, M.K. Ventilatory efficiency in athletes, asthma and obesity. Eur. Respir. Rev. 2021, 30, 200206. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Mean | SD | 95% CI | |
|---|---|---|---|
| Age (y) | 30.8 | 5.9 | 27.6 to 34.0 |
| Height (m) | 1.65 | 0.06 | 1.62 to 1.68 |
| Weight (kg) | 61.0 | 8.4 | 56.4 to 65.6 |
| BMI (kg/m2) | 21.7 | 2.1 | 20.6 to 22.8 |
| BMD (g/cm2) | 1.205 | 0.087 | 1.157 to 1.252 |
| Fat mass (kg) | 16.1 | 6.2 | 12.7 to 19.4 |
| Fat mass (%) | 26.6 | 7.8 | 22.4 to 30.8 |
| Lean mass (kg) | 42.2 | 3.6 | 40.3 to 44.2 |
| Lean mass (%) | 71.9 | 8.9 | 67.1 to 76.8 |
| VO2 max (mL/kg/min) | 48.2 | 5.1 | 45.4 to 51.0 |
| Early Follicular Phase (EFP) | Late Follicular Phase (LFP) | Mid-Luteal Phase (MLP) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | 95% CI | Mean | SD | 95% CI | Mean | SD | 95% CI | |
| Estrogen (pg/mL) | 40.94 | 28.67 | 28.68 to 53.21 | 214.69 | 185.06 | 135.53 to 293.84 | 142.20 | 89.14 | 104.07 to 180.32 |
| Progesterone (ng/mL) | 0.34 | 0.19 | 0.27 to 0.42 | 0.38 | 0.31 | 0.25 to 0.52 | 11.46 | 5.08 | 9.29 to 13.63 |
| LH (mIU/mL) | 6.66 | 1.61 | 5.97 to 7.34 | 13.60 | 8.01 | 10.18 to 17.03 | 6.03 | 2.77 | 4.84 to 7.21 |
| FSH (mIU/mL) | 8.52 | 4.50 | 6.59 to 10.44 | 6.70 | 3.15 | 5.35 to 8.05 | 3.62 | 1.41 | 3.02 to 4.23 |
| Prolactin (mIU/L) | 512.67 | 352.92 | 361.72 to 663.61 | 440.47 | 144.43 | 378.69 to 502.24 | 553.85 | 262.79 | 441.45 to 666.24 |
| Early Follicular Phase (EFP) | Late Follicular Phase (LFP) | Mid-Luteal Phase (MLP) | F-Value | p-Value | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | 95% CI | Mean | SD | 95% CI | Mean | SD | 95% CI | |||
| VT (L/min) | 1.27 | 0.35 | 1.16 to 1.38 | 1.19 a | 0.36 | 1.09 to 1.29 | 1.27 b | 0.37 | 1.16 to 1.38 | 7.592 | 0.003 |
| BF (1/min) | 35.14 | 7.14 | 32.71 to 37.57 | 36.32 | 7.11 | 33.70 to 38.94 | 37.62 c | 7.23 | 34.86 to 40.38 | 8.319 | 0.002 |
| VO2 (mL/min) | 1179.15 | 163.17 | 1075.48 to 1282.83 | 1123.09 | 169.62 | 1015.32 to 1230.86 | 1163.71 | 164.84 | 1058.97 to 1268.44 | 1.376 | 0.273 |
| VCO2 (mL/min) | 1120.46 | 137.62 | 1033.02 to 1207.89 | 1079.50 | 129.57 | 997.18 to 1161.82 | 1145.78 d | 107.91 | 1077.21 to 1214.34 | 4.701 | 0.02 |
| RER | 0.94 | 0.05 | 0.91 to 0.97 | 0.96 | 0.09 | 0.90 to 1.02 | 0.99 | 0.10 | 0.92 to 1.05 | 0.948 | 0.403 |
| EqO2 | 38.18 | 4.70 | 35.19 to 41.16 | 38.96 | 4.40 | 36.16 to 41.76 | 42.21 | 5.93 | 38.45 to 45.98 | 5.168 | 0.014 |
| EqCO2 | 40.49 | 3.85 | 38.04 to 42.93 | 40.78 | 3.50 | 38.55 to 43.00 | 42.77 ef | 3.58 | 40.50 to 45.05 | 8.377 | 0.002 |
| HR (bpm) | 139.42 | 14.11 | 130.54 to 148.30 | 139.69 | 14.41 | 130.62 to 148.75 | 138.48 | 12.27 | 130.77 to 146.20 | 0.194 | 0.743 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Benito, P.J.; Alfaro-Magallanes, V.M.; Rael, B.; Castro, E.A.; Romero-Parra, N.; Rojo-Tirado, M.A.; Peinado, A.B., on behalf of the IronFEMME Study Group. Effect of Menstrual Cycle Phase on the Recovery Process of High-Intensity Interval Exercise—A Cross-Sectional Observational Study. Int. J. Environ. Res. Public Health 2023, 20, 3266. https://doi.org/10.3390/ijerph20043266
Benito PJ, Alfaro-Magallanes VM, Rael B, Castro EA, Romero-Parra N, Rojo-Tirado MA, Peinado AB on behalf of the IronFEMME Study Group. Effect of Menstrual Cycle Phase on the Recovery Process of High-Intensity Interval Exercise—A Cross-Sectional Observational Study. International Journal of Environmental Research and Public Health. 2023; 20(4):3266. https://doi.org/10.3390/ijerph20043266
Chicago/Turabian StyleBenito, Pedro J., Víctor M. Alfaro-Magallanes, Beatriz Rael, Eliane A. Castro, Nuria Romero-Parra, Miguel A. Rojo-Tirado, and Ana B. Peinado on behalf of the IronFEMME Study Group. 2023. "Effect of Menstrual Cycle Phase on the Recovery Process of High-Intensity Interval Exercise—A Cross-Sectional Observational Study" International Journal of Environmental Research and Public Health 20, no. 4: 3266. https://doi.org/10.3390/ijerph20043266