
Safety of Combined Targeted and Helixor® Viscum album L. Therapy in Breast and Gynecological Cancer Patients, a Real-World Data Study

Abstract
:1. Introduction
2. Materials and Methods
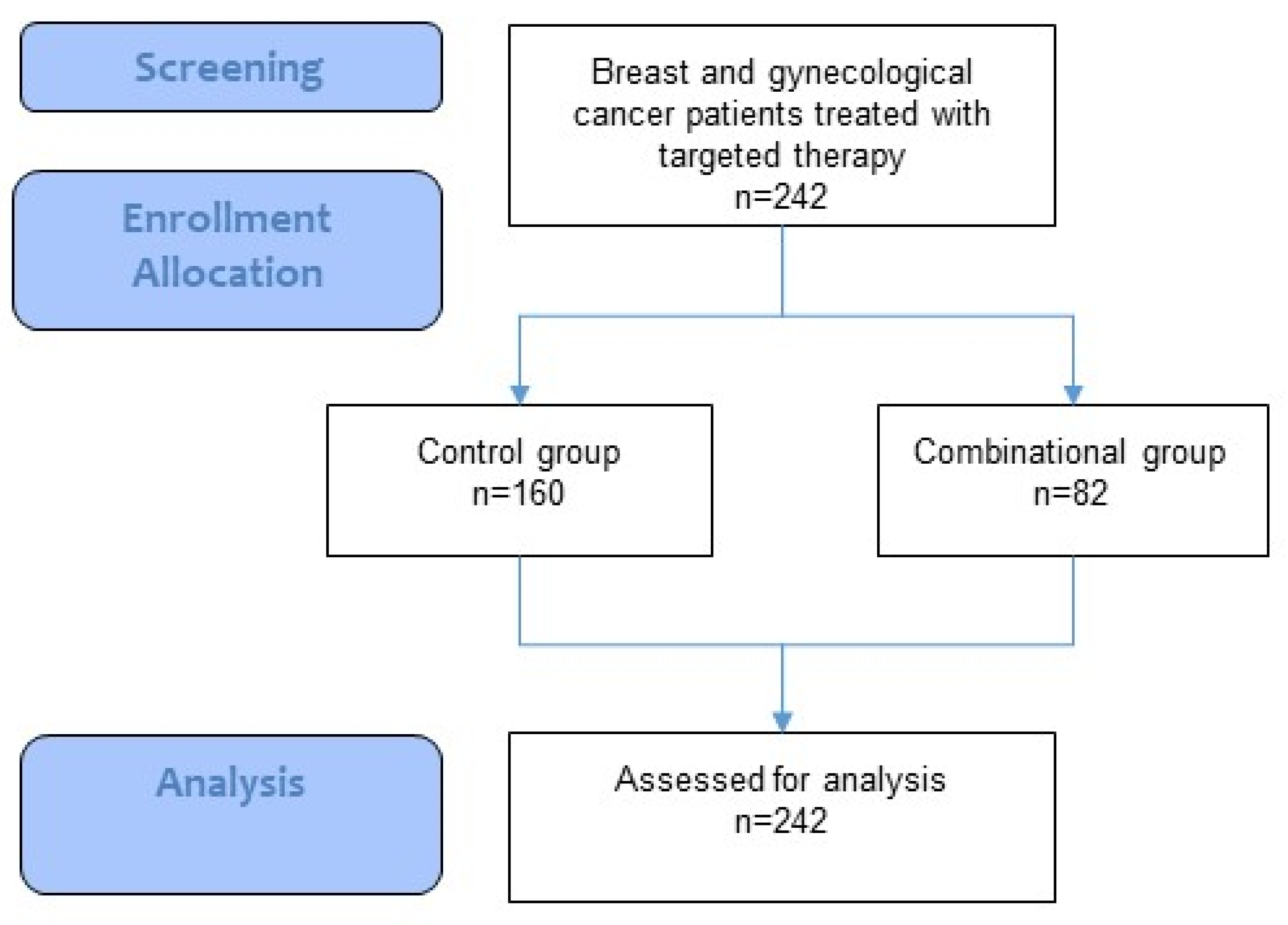
2.1. Study Design
2.2. Description of Study Participants
2.3. Data Source and Assessment
2.4. Statistical Methods
3. Results
3.1. Baseline Characteristics
3.2. Oncological Treatment
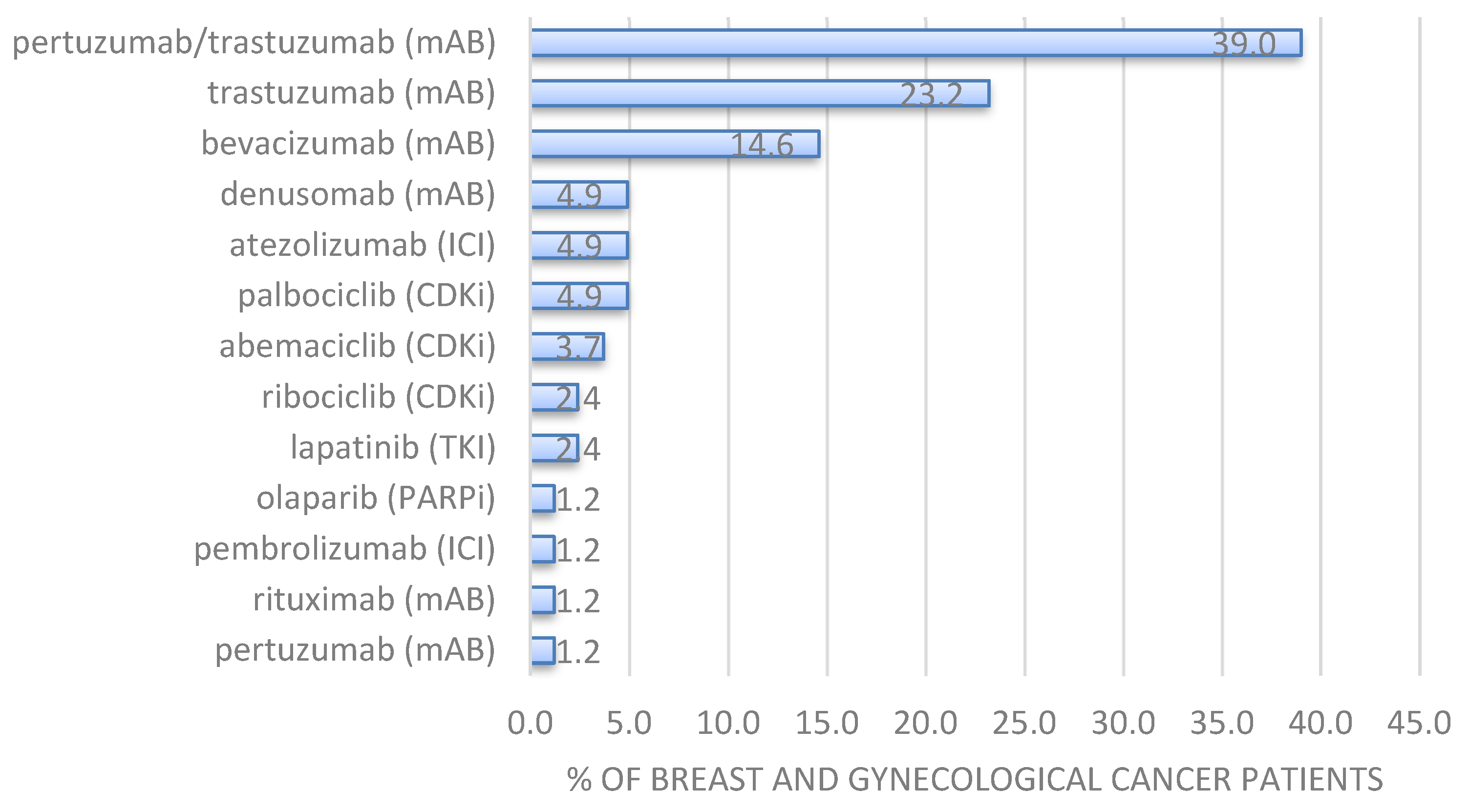
3.3. Characterization of Targeted Therapy
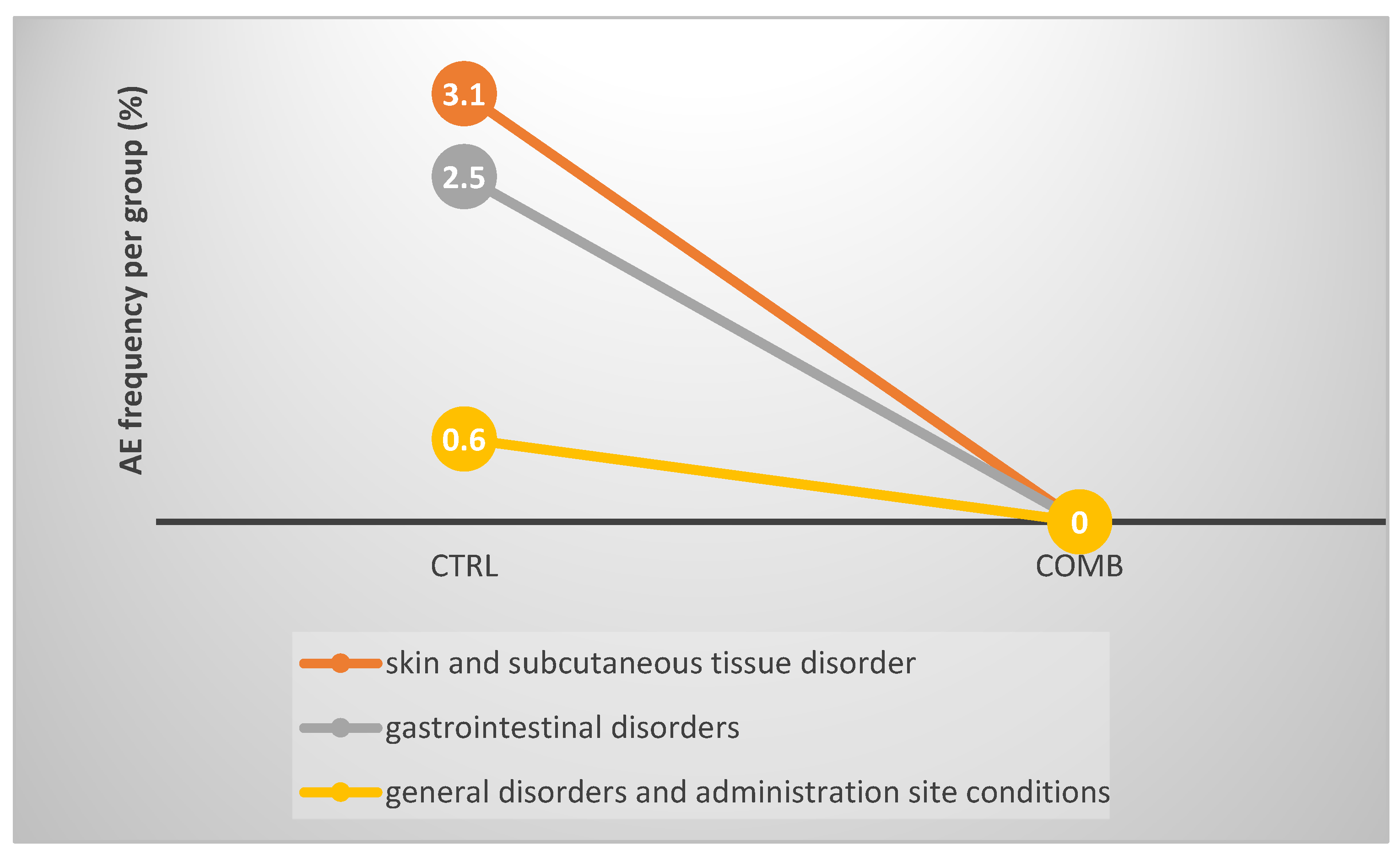
3.4. AEs Related to Targeted and Combinational Treatment
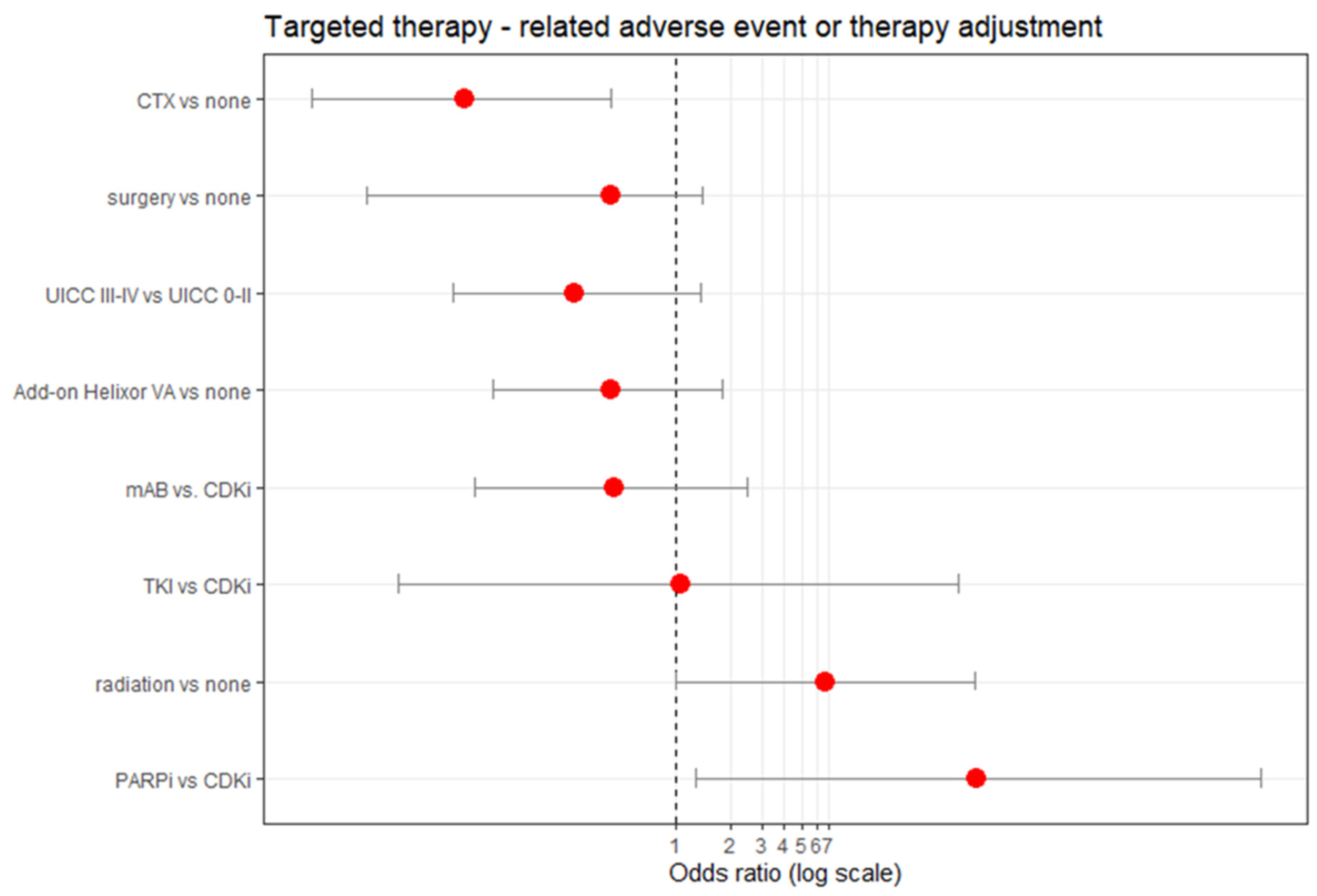
3.5. Factors Associated with Occurrence of AE, Treatment Discontinuation or Dose Disruption in Targeted Therapy
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- National Cancer Institute. Targeted Therapy to Treat Cancer. Available online: https://www.cancer.gov/about-cancer/treatment/types/targeted-therapies (accessed on 11 November 2022).
- Chan, C.Y.; Tan, K.V.; Cornelissen, B. PARP Inhibitors in Cancer Diagnosis and Therapy. Clin. Cancer Res. 2021, 27, 1585–1594. [Google Scholar] [CrossRef] [PubMed]
- Braal, C.L.; Jongbloed, E.M.; Wilting, S.M.; Mathijssen, R.H.J.; Koolen, S.L.W.; Jager, A. Inhibiting CDK4/6 in Breast Cancer with Palbociclib, Ribociclib, and Abemaciclib: Similarities and Differences. Drugs 2021, 81, 317–331. [Google Scholar] [CrossRef] [PubMed]
- Davis, C.; Naci, H.; Gurpinar, E.; Poplavska, E.; Pinto, A.; Aggarwal, A. Availability of evidence of benefits on overall survival and quality of life of cancer drugs approved by European Medicines Agency: Retrospective cohort study of drug approvals 2009-13. BMJ 2017, 359, j4530. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, C.; Prasad, V. Cancer Drugs Approved on the Basis of a Surrogate End Point and Subsequent Overall Survival: An Analysis of 5 Years of US Food and Drug Administration Approvals. JAMA Intern Med. 2015, 175, 1992–1994. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arciero, V.; Delos Santos, S.; Koshy, L.; Rahmadian, A.; Saluja, R.; Everest, L.; Parmar, A.; Chan, K.K.W. Assessment of Food and Drug Administration- and European Medicines Agency-Approved Systemic Oncology Therapies and Clinically Meaningful Improvements in Quality of Life: A Systematic Review. JAMA Netw. Open 2021, 4, e2033004. [Google Scholar] [CrossRef] [PubMed]
- Bock, P.R.; Friedel, W.E.; Hanisch, J.; Karasmann, M.; Schneider, B. Efficacy and safety of long-term complementary treatment with standardized European mistletoe extract (Viscum album L.) in addition to the conventional adjuvant oncologic therapy in patients with primary non-metastasized mammary carcinoma. Results of a multi-center, comparative, epidemiological cohort study in Germany and Switzerland. Arzneimittelforschung 2004, 54, 456–466. [Google Scholar] [PubMed]
- Bar-Sela, G.; Wollner, M.; Hammer, L.; Agbarya, A.; Dudnik, E.; Haim, N. Mistletoe as complementary treatment in patients with advanced non-small-cell lung cancer treated with carboplatin-based combinations: A randomised phase II study. Eur. J. Cancer 2013, 49, 1058–1064. [Google Scholar] [CrossRef] [PubMed]
- Büssing, A. Immune Modulation Using Mistletoe (Viscum album L.) Extracts Iscador. Arzneimittelforschung 2006, 56, 508–515. [Google Scholar] [CrossRef] [PubMed]
- Schad, F.; Axtner, J.; Kröz, M.; Matthes, H.; Steele, M.L. Safety of Combined Treatment With Monoclonal Antibodies and Viscum album L Preparations. Integr. Cancer Ther. 2016, 17, 41–51. [Google Scholar] [CrossRef] [PubMed]
- Thronicke, A.; Steele, M.L.; Grah, C.; Matthes, B.; Schad, F. Clinical safety of combined therapy of immune checkpoint inhibitors and Viscum album L. therapy in patients with advanced or metastatic cancer. BMC Complement. Altern. Med. 2017, 17, 534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thronicke, A.; Oei, S.L.; Grah, C.; Matthes, B.; Schad, F. Nivolumab-induced toxicity profile in patients with advanced or metastasized lung cancer treated with Viscum album L. extracts. Abstract. In Proceedings of the German Cancer Congress, Berlin, Germany, 21–24 February 2018. [Google Scholar]
- Thronicke, A.; Oei, S.L.; Merkle, A.; Matthes, H.; Schad, F. Clinical Safety of Combined Targeted and Viscum album L. Therapy in Oncological Patients. Medicines 2018, 5, 100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schad, F.; Axtner, J.; Happe, A.; Breitkreuz, T.; Paxino, C.; Gutsch, J.; Matthes, B.; Debus, M.; Kröz, M.; Spahn, G.; et al. Network Oncology (NO)--a clinical cancer register for health services research and the evaluation of integrative therapeutic interventions in anthroposophic medicine. Forsch Komplementmed 2013, 20, 353–360. [Google Scholar] [CrossRef] [PubMed]
- ICH. Ich Harmonised Tripartite Guideline. Clinical Safety Data Management: Definitions and Standards for Expedited Reporting e2a. Available online: https://database.ich.org/sites/default/files/E2A_Guideline.pdf (accessed on 19 January 2023).
- University of Virginia Library. A Brief on Brier Score. Available online: https://data.library.virginia.edu/a-brief-on-brier-scores/ (accessed on 19 January 2023).
- Clarke, M.; Collins, R.; Darby, S.; Davies, C.; Elphinstone, P.; Evans, V.; Godwin, J.; Gray, R.; Hicks, C.; James, S.; et al. Effects of radiotherapy and of differences in the extent of surgery for early breast cancer on local recurrence and 15-year survival: An overview of the randomised trials. Lancet 2005, 366, 2087–2106. [Google Scholar] [CrossRef] [PubMed]
- Early Breast Cancer Trialists’ Collaborative Group. Effect of radiotherapy after breast-conserving surgery on 10-year recurrence and 15-year breast cancer death: Meta-analysis of individual patient data for 10,801 women in 17 randomised trials. Lancet 2011, 378, 1707–1716. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- EMA. Herceptin, Annex I, Summary of Product Characteristics. Available online: http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/000278/WC500074922.pdf (accessed on 11 November 2022).
- EMA. European Public Assessment Report. Ibrance. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/ibrance (accessed on 11 November 2022).
- EMA. European Public Assessment Report. Tecentriq. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/tecentriq (accessed on 11 November 2022).
- EMA. European Public Assessment Report. Tyverb. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/tyverb (accessed on 11 November 2022).
- Piao, B.K.; Wang, Y.X.; Xie, G.R.; Mannmann, U.; Matthes, H.; Beuth, J.; Lin, H.S. Impact of complementary mistletoe extract treatment on quality of life in breast, ovarian and non-small cell lung cancer patients. A prospective randomized controlled clinical trial. Anticancer. Res. 2004, 24, 303–310. [Google Scholar] [PubMed]
- Tröger, W.; Zdrale, Z.; Tisma, N.; Matijasevic, M. Additional therapy with a mistletoe product during adjuvant chemotherapy of breast cancer patients improves quality of life: An open randomized clinical pilot trial. ECAM 2014, 2014, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- EMA. Perjeta. Summary of Product Characteristics. Available online: https://www.ema.europa.eu/en/documents/product-information/perjeta-epar-product-information_en.pdf (accessed on 11 November 2022).
- EMA. Zejula. Summary of Product Characteristics. Available online: https://www.ema.europa.eu/en/documents/product-information/zejula-epar-product-information_en.pdf (accessed on 11 November 2022).
- EMA. Herceptin. Summary of Product Characteristics. Available online: https://www.ema.europa.eu/en/documents/product-information/herceptin-epar-product-information_en.pdf (accessed on 11 November 2022).
- EMA. Votrient. Summary of product characteristics. Available online: https://www.ema.europa.eu/en/documents/product-information/votrient-epar-product-information_en.pdf (accessed on 11 November 2022).
- Hazell, L.; Shakir, S.A. Under-reporting of adverse drug reactions: A systematic review. Drug Saf. 2006, 29, 385–396. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Characteristics | Total Cohort n = 242 | CTRL n = 160 | COMB n = 82 | Significance p-Value |
|---|---|---|---|---|
| Age at first diagnosis, years, mean (SD) | 54.5 (14.2) | 54.7 (14.4) | 54.3 (13.7) | 0.84 |
| Cancer entity, n (%) | 1.13 | |||
| Breast, n (%) | 212 (87.6) | 136 (85) | 75 (91.5) | |
| Ovarian, n (%) | 25 (10.3) | 19 (11.9) | 6 (7.3) | |
| Other 1), n (%) | 5 (2.1) | 5 (3.1) | 0 (0) | |
| UICC stage | 0.08 | |||
| 0 | 1 (0.4) | 1 (0.6) | 0 | |
| I | 49 (20.2) | 26 (16.3) | 23 (28.0) | |
| II | 86 (35.5) | 55 (34.4) | 31 (37.8) | |
| III | 49 (20.2) | 39 (24.4) | 10 (12.2) | |
| IV | 44 (18.2) | 29 (18.1) | 15 (18.3) | |
| NA | 13 (5.4) | 10 (6.3) | 82 (3.7) |
| Total Cohort, n = 242 | CTRL n = 160 | COMB n = 82 | Significance p-Value | |
|---|---|---|---|---|
| Surgery | 0.91 | |||
| yes | 208 (86.0) | 140 (87.5) | 68 (82.9) | |
| no | 27 (11.2) | 19 (11.9) | 8 (9.8) | |
| NA | 7 (2.9) | 1 (0.6) | 6 (7.3) | |
| Radiation | 0.08 | |||
| yes | 140 (57.9) | 88 (55.0) | 52 (63.4) | |
| no | 95 (39.3) | 71 (44.4) | 24 (29.3) | |
| NA | 7 (2.9) | 1 (0.6) | 6 (7.3) | |
| CTx | 0.51 | |||
| yes | 229 (94.6) | 153 (95.6) | 76 (92.7) | |
| no | 13 (5.4) | 7 (4.4) | 6 (7.3) |
| Patient Characteristics | Total Cohort n = 242 | CTRL n = 160 | COMB n = 82 | Significance p-Value |
|---|---|---|---|---|
| CDKi, n (%) | 26 (10.7) | 17 (10.6) | 9 (11.0) | 1.0 |
| abemaciclib, n (%) | 4 (1.7) | 1 (0.6) | 3 (3.7) | |
| palbociclib, n (%) | 18 (7.4) | 14 (8.8) | 4 (4.9) | |
| ribociclib, n (%) | 5 (2.1) | 3 (1.9) | 2 (2.4) | |
| mAB, n (%) | 206 (84.1) | 136 (85.0) | 70 (85.4) | 1.0 |
| bevacizumab, n (%) | 47 (19.4) | 35 (2.19) | 12 (14.6) | |
| denusomab, n (%) | 8 (3.3) | 4 (2.5) | 4 (4.9) | |
| glembatumumab, n (%) | 1 (0.4) | 1 (0.6) | 0 | |
| pertuzumab, n (%) | 2 (0.8) | 1 (0.6) | 1 (1.2) | |
| pertuzumab/trastuzumab, n (%) | 62 (25.6) | 30 (18.8) | 32 (39.0) | |
| rituximab, n (%) | 2 (0.8) | 1 (0.6) | 1 (1.2) | |
| trastuzumab, n (%) | 74 (30.6) | 55 (34.4) | 19 (23.2) | |
| trastuzumab-emtasin, n (%) | 3 (1.2) | 3 (1.9) | 0 | |
| ICI, n (%) | 13 (5.4) | 8 (5) | 5 (6.1) | 1.0 |
| atezolizumab, n (%) | 11 (4.5) | 7 (4.4) | 4 (4.9) | |
| pembrolizumab, n (%) | 2 (0.8) | 1 (0.6) | 1 (1.2) | |
| PARPi, n (%) | 4 (1.7) | 3 (1.9) | 1 (1.2) | 1.0 |
| niraparib, n (%) | 1 (0.4) | 1 (0.6) | 0 | |
| olaparib, n (%) | 3 (1.2) | 2 (1.3) | 1 (1.2) | |
| TKI, n (%) | 6 (2.5) | 4 (2.5) | 2 (2.4) | 1.0 |
| erlotinib, n (%) | 1 (0.4) | 1 (0.6) | 0 | |
| lapatinib, n (%) | 4 (1.7) | 2 (1.3) | 2 (2.4) | |
| nintedanib, n (%) | 1 (0.4) | 1 (0.6) | 0 | |
| pazopanib, n (%) | 1 (0.4) | 1 (0.6) | 0 |
| System Organ Class | Adverse Event (AE) | Total n = 242 | CTRL n = 160 | COMB n = 82 |
|---|---|---|---|---|
| gastrointestinal disorders | nausea | 2 | a 1), d 4) | - |
| appetite loss | 1 | d 4) | - | |
| vomiting | 1 | d 4) | - | |
| general disorders and administration site conditions | pain | 1 | c 3)* | - |
| temperature elevated | 1 | b 2)* | - | |
| fatigue | 1 | e 5) | - | |
| neck stiffness | 1 | e 5) | - | |
| impaired vision | 1 | e 5) | - | |
| skin and subcutaneous tissue disorder | erythema | 1 | e 5) | - |
| Total number of AEs | 10 | 10 | - | |
| Total number of patients experiencing AE | 5 | 5 | 0 | |
| AE per patient frequency (AE events divided by number of all patients, n (%) §) | 4.13% §) | 6.25% | 0 | |
| Patient with AE frequency (patient experiencing an AE divided by number of all patients) §§) | 2.07% §§) | 3.13% | 0 |
| Total Cohort n = 242 | CTRL n = 160 | COMB n = 82 | Significance p-Value | |
|---|---|---|---|---|
| AE due to targeted treatment, n (%) | 5 (2.1) | 5 (3.1) | 0 | 0.254 |
| Disruption of targeted treatment, n (%) | 6 (2.9) | 5 (3.1) | 1 (1.2) | 0.642 |
| Dose reduction of targeted treatment, n (%) | 8 (3.3) | 5 (3.1) | 3 (3.7) | 1.0 |
| Any event (AE or therapy adjustment §), n (%) | 14 (5.8) | 10 (6.3) | 3 (4.9) | 0.586 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schad, F.; Thronicke, A. Safety of Combined Targeted and Helixor® Viscum album L. Therapy in Breast and Gynecological Cancer Patients, a Real-World Data Study. Int. J. Environ. Res. Public Health 2023, 20, 2565. https://doi.org/10.3390/ijerph20032565
Schad F, Thronicke A. Safety of Combined Targeted and Helixor® Viscum album L. Therapy in Breast and Gynecological Cancer Patients, a Real-World Data Study. International Journal of Environmental Research and Public Health. 2023; 20(3):2565. https://doi.org/10.3390/ijerph20032565
Chicago/Turabian StyleSchad, Friedemann, and Anja Thronicke. 2023. "Safety of Combined Targeted and Helixor® Viscum album L. Therapy in Breast and Gynecological Cancer Patients, a Real-World Data Study" International Journal of Environmental Research and Public Health 20, no. 3: 2565. https://doi.org/10.3390/ijerph20032565