
Pedometers and Accelerometers in Multiple Sclerosis: Current and New Applications
 , ,
, , {kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
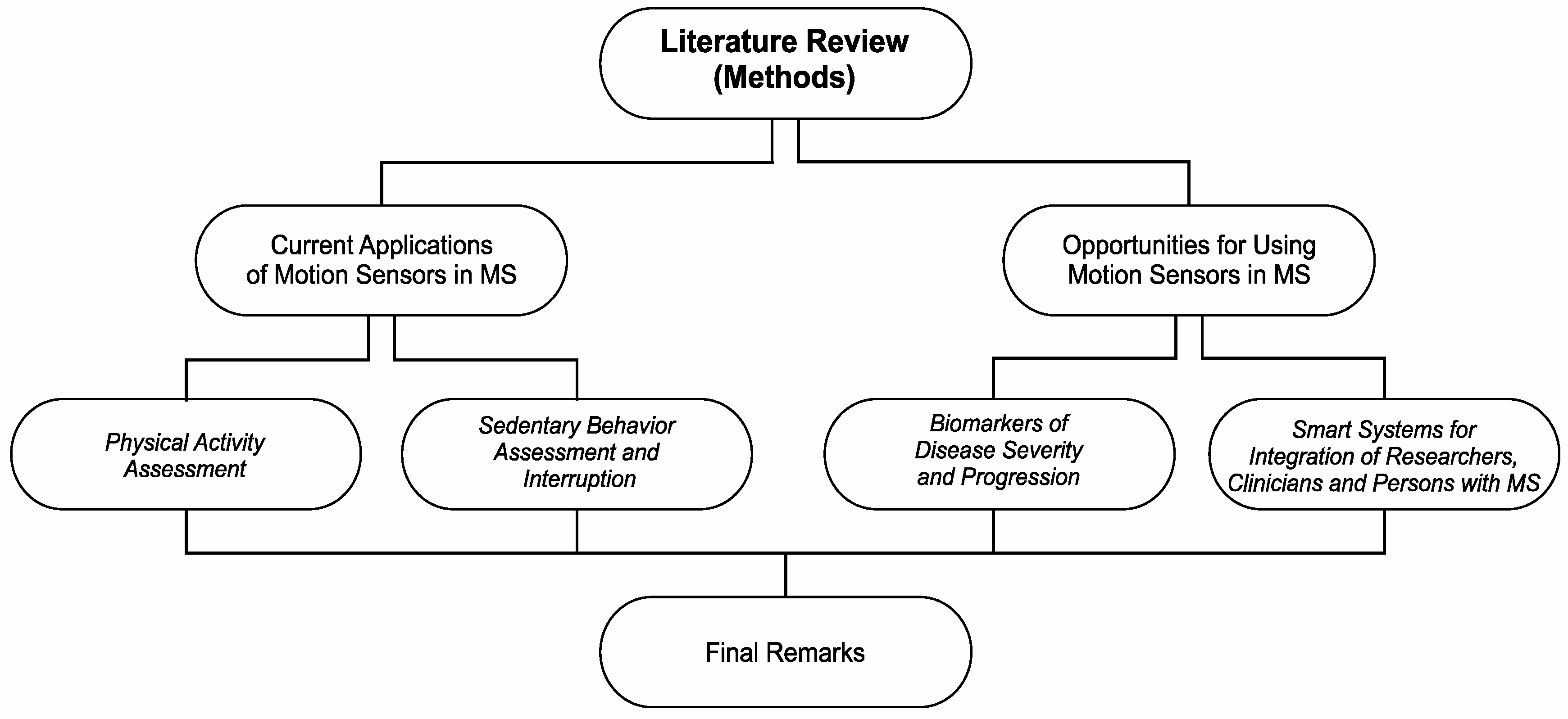
2. Methods
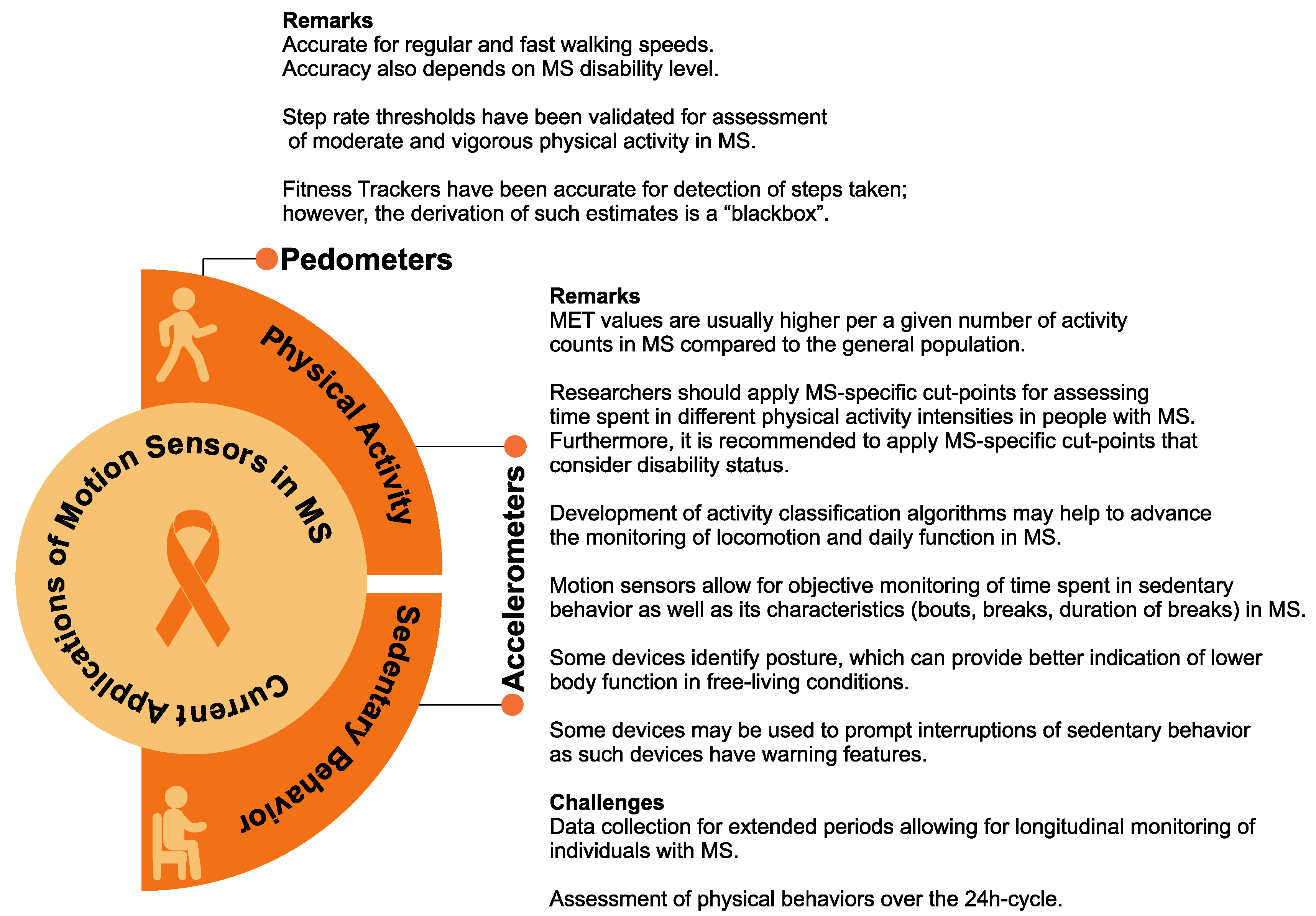
3. Current Applications of Motion Sensors in MS
3.1. Physical Activity Assessment
3.2. Sedentary Behavior Assessment and Interruption
4. Opportunities for Using Motion Sensors in MS
4.1. Biomarkers of Disease Severity and Progression
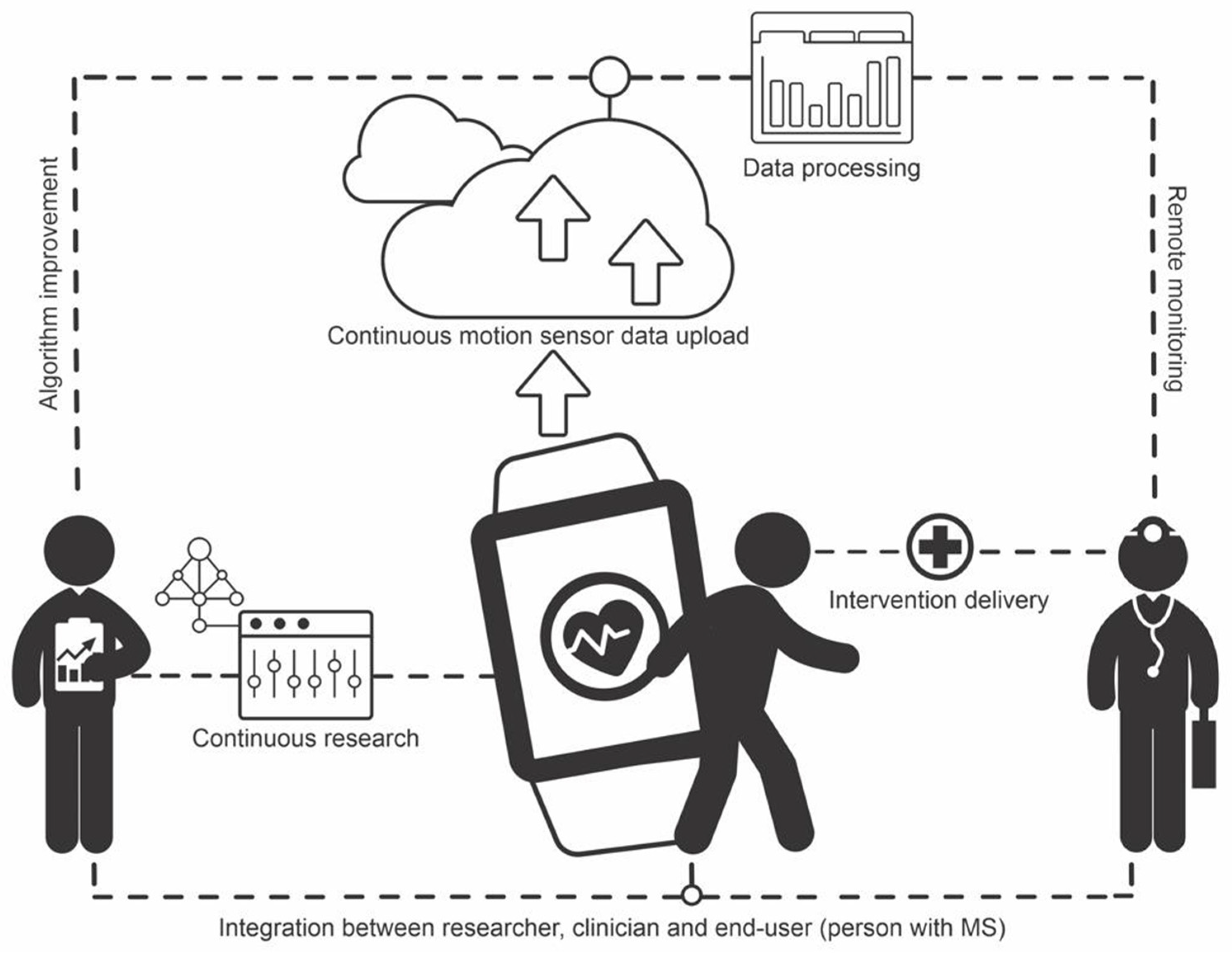
4.2. Smart Systems for the Integration of Researchers, Clinicians, and Persons with MS
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sasaki, J.E.; Da Silva, K.S.; Da Costa, B.G.G.; John, D. Measurement of Physical Activity Using Accelerometers. In Computer-Assisted and Web-Based Innovations in Psychology, Special Education, and Health; Academic Press: Cambrige, MA, USA, 2016; pp. 33–60. [Google Scholar]
- Block, V.A.J.; Pitsch, E.; Tahir, P.; Cree, B.A.C.; Allen, D.D.; Gelfand, J.M. Remote Physical Activity Monitoring in Neurological Disease: A Systematic Review. PLoS ONE 2016, 11, e0154335. [Google Scholar] [CrossRef] [PubMed]
- Kalb, R.; Brown, T.R.; Coote, S.; Costello, K.; Dalgas, U.; Garmon, E.; Giesser, B.; Halper, J.; Karpatkin, H.; Keller, J.; et al. Exercise and Lifestyle Physical Activity Recommendations for People with Multiple Sclerosis throughout the Disease Course. Mult. Scler. Houndmills Basingstoke Engl. 2020, 26, 1459–1469. [Google Scholar] [CrossRef] [PubMed]
- Murray, T.J. Multiple Sclerosis: The History of a Disease; Demos Medical Publishing: New York, NY, USA, 2005. [Google Scholar]
- Bradshaw, M.J.; Farrow, S.; Motl, R.W.; Chitnis, T. Wearable Biosensors to Monitor Disability in Multiple Sclerosis. Neurol. Clin. Pract. 2017, 7, 354–362. [Google Scholar] [CrossRef] [PubMed]
- Caspersen, C.J.; Powell, K.E.; Christenson, G.M. Physical Activity, Exercise, and Physical Fitness: Definitions and Distinctions for Health-Related Research. Public Health Rep. 1985, 100, 126–131. [Google Scholar]
- Owen, N.; Healy, G.N.; Matthews, C.E.; Dunstan, D.W. Too Much Sitting: The Population Health Science of Sedentary Behavior. Exerc. Sport Sci. Rev. 2010, 38, 105–113. [Google Scholar] [CrossRef]
- Sasaki, J.E.; Sandroff, B.; Bamman, M.; Motl, R.W. Motion Sensors in Multiple Sclerosis: Narrative Review and Update of Applications. Expert Rev. Med. Devices 2017, 14, 891–900. [Google Scholar] [CrossRef]
- Frechette, M.L.; Meyer, B.M.; Tulipani, L.J.; Gurchiek, R.D.; McGinnis, R.S.; Sosnoff, J.J. Next Steps in Wearable Technology and Community Ambulation in Multiple Sclerosis. Curr. Neurol. Neurosci. Rep. 2019, 19, 80. [Google Scholar] [CrossRef]
- Rother, E.T. Systematic Literature Review X Narrative Review. Acta Paul. Enferm. 2007, 20, 5–6. [Google Scholar] [CrossRef]
- Motl, R.W.; McAuley, E.; Snook, E.M.; Scott, J.A. Accuracy of Two Electronic Pedometers for Measuring Steps Taken under Controlled Conditions among Ambulatory Individuals with Multiple Sclerosis. Mult. Scler. J. 2005, 11, 343–345. [Google Scholar] [CrossRef]
- Elsworth, C.; Dawes, H.; Winward, C.; Howells, K.; Collett, J.; Dennis, A.; Sackley, C.; Wade, D. Pedometer Step Counts in Individuals with Neurological Conditions. Clin. Rehabil. 2009, 23, 171–175. [Google Scholar] [CrossRef]
- Motl, R.W.; Snook, E.M.; Agiovlasitis, S. Does an Accelerometer Accurately Measure Steps Taken under Controlled Conditions in Adults with Mild Multiple Sclerosis? Disabil. Health J. 2011, 4, 52–57. [Google Scholar] [CrossRef] [PubMed]
- Sandroff, B.M.; Motl, R.W.; Pilutti, L.A.; Learmonth, Y.C.; Ensari, I.; Dlugonski, D.; Klaren, R.E.; Balantrapu, S.; Riskin, B.J. Accuracy of StepWatchTM and ActiGraph Accelerometers for Measuring Steps Taken among Persons with Multiple Sclerosis. PLoS ONE 2014, 9, e93511. [Google Scholar] [CrossRef] [PubMed]
- Block, V.J.; Lizée, A.; Crabtree-Hartman, E.; Bevan, C.J.; Graves, J.S.; Bove, R.; Green, A.J.; Nourbakhsh, B.; Tremblay, M.; Gourraud, P.-A.; et al. Continuous Daily Assessment of Multiple Sclerosis Disability Using Remote Step Count Monitoring. J. Neurol. 2017, 264, 316–326. [Google Scholar] [CrossRef] [PubMed]
- Balto, J.M.; Kinnett-Hopkins, D.L.; Motl, R.W. Accuracy and Precision of Smartphone Applications and Commercially Available Motion Sensors in Multiple Sclerosis. Mult. Scler. J. Exp. Transl. Clin. 2016, 2, 2055217316634754. [Google Scholar] [CrossRef] [PubMed]
- Sandroff, B.M.; Riskin, B.J.; Agiovlasitis, S.; Motl, R.W. Accelerometer Cut-Points Derived during over-Ground Walking in Persons with Mild, Moderate, and Severe Multiple Sclerosis. J. Neurol. Sci. 2014, 340, 50–57. [Google Scholar] [CrossRef] [PubMed]
- Motl, R.W.; Snook, E.M.; Agiovlasitis, S.; Suh, Y. Calibration of Accelerometer Output for Ambulatory Adults with Multiple Sclerosis. Arch. Phys. Med. Rehabil. 2009, 90, 1778–1784. [Google Scholar] [CrossRef] [PubMed]
- Sandroff, B.M.; Motl, R.W.; Suh, Y. Accelerometer Output and Its Association with Energy Expenditure in Persons with Multiple Sclerosis. J. Rehabil. Res. Dev. 2012, 49, 467–475. [Google Scholar] [CrossRef]
- Agiovlasitis, S.; Motl, R.W. Step-Rate Thresholds for Physical Activity Intensity in Persons with Multiple Sclerosis. Adapt. Phys. Act. Q. APAQ 2014, 31, 4–18. [Google Scholar] [CrossRef]
- Agiovlasitis, S.; Sandroff, B.M.; Motl, R.W. Step-Rate Cut-Points for Physical Activity Intensity in Patients with Multiple Sclerosis: The Effect of Disability Status. J. Neurol. Sci. 2016, 361, 95–100. [Google Scholar] [CrossRef]
- Coulter, E.H.; Miller, L.; McCorkell, S.; McGuire, C.; Algie, K.; Freeman, J.; Weller, B.; Mattison, P.G.; McConnachie, A.; Wu, O.; et al. Validity of the ActivPAL3 Activity Monitor in People Moderately Affected by Multiple Sclerosis. Med. Eng. Phys. 2017, 45, 78–82. [Google Scholar] [CrossRef]
- Ezeugwu, V.; Klaren, R.E.; Hubbard, A.E.; Manns, P.T.; Motl, R.W. Mobility Disability and the Pattern of Accelerometer-Derived Sedentary and Physical Activity Behaviors in People with Multiple Sclerosis. Prev. Med. Rep. 2015, 2, 241–246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vienne-Jumeau, A.; Quijoux, F.; Vidal, P.-P.; Ricard, D. Wearable Inertial Sensors Provide Reliable Biomarkers of Disease Severity in Multiple Sclerosis: A Systematic Review and Meta-Analysis. Ann. Phys. Rehabil. Med. 2020, 63, 138–147. [Google Scholar] [CrossRef]
- Motl, R.W.; Sosnoff, J.J.; Dlugonski, D.; Suh, Y.; Goldman, M. Does a Waist-Worn Accelerometer Capture Intra- and Inter-Person Variation in Walking Behavior among Persons with Multiple Sclerosis? Med. Eng. Phys. 2010, 32, 1224–1228. [Google Scholar] [CrossRef] [PubMed]
- Weikert, M.; Suh, Y.; Lane, A.; Sandroff, B.; Dlugonski, D.; Fernhall, B.; Motl, R.W. Accelerometry Is Associated with Walking Mobility, Not Physical Activity, in Persons with Multiple Sclerosis. Med. Eng. Phys. 2012, 34, 590–597. [Google Scholar] [CrossRef] [PubMed]
- Cavanaugh, J.T.; Gappmaier, V.O.; Dibble, L.E.; Gappmaier, E. Ambulatory Activity in Individuals with Multiple Sclerosis. J. Neurol. Phys. Ther. JNPT 2011, 35, 26–33. [Google Scholar] [CrossRef] [PubMed]
- Storm, F.A.; Nair, K.P.S.; Clarke, A.J.; der Meulen, J.M.V.; Mazzà, C. Free-Living and Laboratory Gait Characteristics in Patients with Multiple Sclerosis. PLoS ONE 2018, 13, e0196463. [Google Scholar] [CrossRef]
- Motl, R.W.; Pilutti, L.A.; Learmonth, Y.C.; Goldman, M.D.; Brown, T. Clinical Importance of Steps Taken per Day among Persons with Multiple Sclerosis. PLoS ONE 2013, 8, e73247. [Google Scholar] [CrossRef]
- Crouter, S.E.; Schneider, P.L.; Bassett, D.R. Spring-Levered versus Piezo-Electric Pedometer Accuracy in Overweight and Obese Adults. Med. Sci. Sports Exerc. 2005, 37, 1673–1679. [Google Scholar] [CrossRef]
- Silveira, S.L.; Baird, J.F.; Motl, R.W. Rates, Patterns, and Correlates of Fitness Tracker Use among Older Adults with Multiple Sclerosis. Disabil. Health J. 2021, 14, 100966. [Google Scholar] [CrossRef]
- Sasaki, J.E.; Motl, R.W. Motion Sensors for Physical Activity Assessment: Review of Applications. In Reference Module in Biomedical Sciences; Elsevier: Amsterdam, The Netherlands, 2021. [Google Scholar]
- Sasaki, J.E.; John, D.; Freedson, P.S. Validation and Comparison of ActiGraph Activity Monitors. J. Sci. Med. Sport Sports Med. Aust. 2011, 14, 411–416. [Google Scholar] [CrossRef]
- Sandroff, B.M.; Klaren, R.E.; Pilutti, L.A.; Motl, R.W. Oxygen Cost of Walking in Persons with Multiple Sclerosis: Disability Matters, but Why? Mult. Scler. Int. 2014, 2014, 162765. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Motl, R.W.; Learmonth, Y.C.; Pilutti, L.A.; Gappmaier, E.; Coote, S. Top 10 Research Questions Related to Physical Activity and Multiple Sclerosis. Res. Q. Exerc. Sport 2015, 86, 117–129. [Google Scholar] [CrossRef] [PubMed]
- Suh, Y.; Weikert, M.; Dlugonski, D.; Sandroff, B.; Motl, R.W. Social Cognitive Correlates of Physical Activity: Findings from a Cross-Sectional Study of Adults with Relapsing-Remitting Multiple Sclerosis. J. Phys. Act. Health 2011, 8, 626–635. [Google Scholar] [CrossRef]
- Sandroff, B.M.; Dlugonski, D.; Weikert, M.; Suh, Y.; Balantrapu, S.; Motl, R.W. Physical Activity and Multiple Sclerosis: New Insights Regarding Inactivity. Acta Neurol. Scand. 2012, 126, 256–262. [Google Scholar] [CrossRef] [PubMed]
- Klaren, R.E.; Sasaki, J.E.; McAuley, E.; Motl, R.W. Patterns and Predictors of Change in Moderate-to-Vigorous Physical Activity Over Time in Multiple Sclerosis. J. Phys. Act. Health 2017, 14, 183–188. [Google Scholar] [CrossRef] [PubMed]
- Wójcicki, T.R.; Roberts, S.A.; Learmonth, Y.C.; Hubbard, E.A.; Kinnett-Hopkins, D.; Motl, R.W.; McAuley, E. Improving Physical Functional and Quality of Life in Older Adults with Multiple Sclerosis via a DVD-Delivered Exercise Intervention: A Study Protocol. BMJ Open 2014, 4, e006250. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Murray, P.; Zillmer, R.; Eston, R.G.; Catt, M.; Rowlands, A.V. Activity Classification Using the GENEA: Optimum Sampling Frequency and Number of Axes. Med. Sci. Sports Exerc. 2012, 44, 2228–2234. [Google Scholar] [CrossRef]
- Zhang, S.; Rowlands, A.V.; Murray, P.; Hurst, T.L. Physical Activity Classification Using the GENEA Wrist-Worn Accelerometer. Med. Sci. Sports Exerc. 2012, 44, 742–748. [Google Scholar] [CrossRef]
- Healy, G.N.; Dunstan, D.W.; Salmon, J.; Cerin, E.; Shaw, J.E.; Zimmet, P.Z.; Owen, N. Breaks in Sedentary Time: Beneficial Associations with Metabolic Risk. Diabetes Care 2008, 31, 661–666. [Google Scholar] [CrossRef]
- Klaren, R.E.; Sebastiao, E.; Chiu, C.-Y.; Kinnett-Hopkins, D.; McAuley, E.; Motl, R.W. Levels and Rates of Physical Activity in Older Adults with Multiple Sclerosis. Aging Dis. 2016, 7, 278–284. [Google Scholar] [CrossRef]
- Bollaert, R.E.; Motl, R.W. Physical and Cognitive Functions, Physical Activity, and Sedentary Behavior in Older Adults With Multiple Sclerosis. J. Geriatr. Phys. Ther. 2019, 42, 304–312. [Google Scholar] [CrossRef]
- Brocklebank, L.A.; Falconer, C.L.; Page, A.S.; Perry, R.; Cooper, A.R. Accelerometer-Measured Sedentary Time and Cardiometabolic Biomarkers: A Systematic Review. Prev. Med. 2015, 76, 92–102. [Google Scholar] [CrossRef]
- Healy, G.N.; Matthews, C.E.; Dunstan, D.W.; Winkler, E.A.H.; Owen, N. Sedentary Time and Cardio-Metabolic Biomarkers in US Adults: NHANES 2003–06. Eur. Heart J. 2011, 32, 590–597. [Google Scholar] [CrossRef]
- Karle, V.; Hartung, V.; Ivanovska, K.; Mäurer, M.; Flachenecker, P.; Pfeifer, K.; Tallner, A. The Two-Minute Walk Test in Persons with Multiple Sclerosis: Correlations of Cadence with Free-Living Walking Do Not Support Ecological Validity. Int. J. Environ. Res. Public. Health 2020, 17, 9044. [Google Scholar] [CrossRef]
- Warmerdam, E.; Hausdorff, J.M.; Atrsaei, A.; Zhou, Y.; Mirelman, A.; Aminian, K.; Espay, A.J.; Hansen, C.; Evers, L.J.W.; Keller, A.; et al. Long-Term Unsupervised Mobility Assessment in Movement Disorders. Lancet Neurol. 2020, 19, 462–470. [Google Scholar] [CrossRef]
- Polhemus, A.M.; Bergquist, R.; Bosch de Basea, M.; Brittain, G.; Buttery, S.C.; Chynkiamis, N.; Dalla Costa, G.; Delgado Ortiz, L.; Demeyer, H.; Emmert, K.; et al. Walking-Related Digital Mobility Outcomes as Clinical Trial Endpoint Measures: Protocol for a Scoping Review. BMJ Open 2020, 10, e038704. [Google Scholar] [CrossRef]
- Porciuncula, F.; Roto, A.V.; Kumar, D.; Davis, I.; Roy, S.; Walsh, C.J.; Awad, L.N. Wearable Movement Sensors for Rehabilitation: A Focused Review of Technological and Clinical Advances. PM R 2018, 10, S220–S232. [Google Scholar] [CrossRef]
- Kluge, F.; Din, S.D.; Cereatti, A.; Gaßner, H.; Hansen, C.; Helbostad, J.L.; Klucken, J.; Küderle, A.; Müller, A.; Rochester, L.; et al. Consensus Based Framework for Digital Mobility Monitoring. PLoS ONE 2021, 16, e0256541. [Google Scholar] [CrossRef]
- Grčić, P.F.; Matijaca, M.; Lušić, I.; Čapkun, V. Responsiveness of Walking-Based Outcome Measures after Multiple Sclerosis Relapses Following Steroid Pulses. Med. Sci. Monit. 2011, 17, CR704–CR710. [Google Scholar] [CrossRef]
- Tulipani, L.J.; Meyer, B.; Larie, D.; Solomon, A.J.; McGinnis, R.S. Metrics Extracted from a Single Wearable Sensor during Sit-Stand Transitions Relate to Mobility Impairment and Fall Risk in People with Multiple Sclerosis. Gait Posture 2020, 80, 361–366. [Google Scholar] [CrossRef]
- Pau, M.; Mandaresu, S.; Pilloni, G.; Porta, M.; Coghe, G.; Marrosu, M.G.; Cocco, E. Smoothness of Gait Detects Early Alterations of Walking in Persons with Multiple Sclerosis without Disability. Gait Posture 2017, 58, 307–309. [Google Scholar] [CrossRef]
- Sasaki, J.E.; Hickey, A.M.; Staudenmayer, J.W.; John, D.; Kent, J.A.; Freedson, P.S. Performance of Activity Classification Algorithms in Free-Living Older Adults. Med. Sci. Sports Exerc. 2016, 48, 941–950. [Google Scholar] [CrossRef]
- Staudenmayer, J.; He, S.; Hickey, A.; Sasaki, J.; Freedson, P. Methods to Estimate Aspects of Physical Activity and Sedentary Behavior from High-Frequency Wrist Accelerometer Measurements. J. Appl. Physiol. 2015, 119, 396–403. [Google Scholar] [CrossRef]
- Stavropoulos, T.G.; Meditskos, G.; Papagiannopoulos, S.; Kompatsiaris, I. EHealth4MS: Problem Detection from Wearable Activity Trackers to Support the Care of Multiple Sclerosis. In Ambient Intelligence–Software and Applications; Novais, P., Vercelli, G., Larriba-Pey, J.L., Herrera, F., Chamoso, P., Eds.; Advances in Intelligent Systems and Computing; Springer International Publishing: Cham, Switzerland, 2021; Volume 1239, pp. 3–12. [Google Scholar]
- Lai, B.; Young, H.-J.; Bickel, C.S.; Motl, R.W.; Rimmer, J.H. Current Trends in Exercise Intervention Research, Technology, and Behavioral Change Strategies for People With Disabilities: A Scoping Review. Am. J. Phys. Med. Rehabil. 2017, 96, 748–761. [Google Scholar] [CrossRef]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sasaki, J.E.; Bertochi, G.F.A.; Meneguci, J.; Motl, R.W. Pedometers and Accelerometers in Multiple Sclerosis: Current and New Applications. Int. J. Environ. Res. Public Health 2022, 19, 11839. https://doi.org/10.3390/ijerph191811839
Sasaki JE, Bertochi GFA, Meneguci J, Motl RW. Pedometers and Accelerometers in Multiple Sclerosis: Current and New Applications. International Journal of Environmental Research and Public Health. 2022; 19(18):11839. https://doi.org/10.3390/ijerph191811839
Chicago/Turabian StyleSasaki, Jeffer Eidi, Gabriel Felipe Arantes Bertochi, Joilson Meneguci, and Robert W. Motl. 2022. "Pedometers and Accelerometers in Multiple Sclerosis: Current and New Applications" International Journal of Environmental Research and Public Health 19, no. 18: 11839. https://doi.org/10.3390/ijerph191811839