
Reporting Liver Cancer Trends in the Island of Crete, Greece: Results from a Geo-Epidemiological Study

 ,
, 
Abstract
:1. Introduction
2. Methods
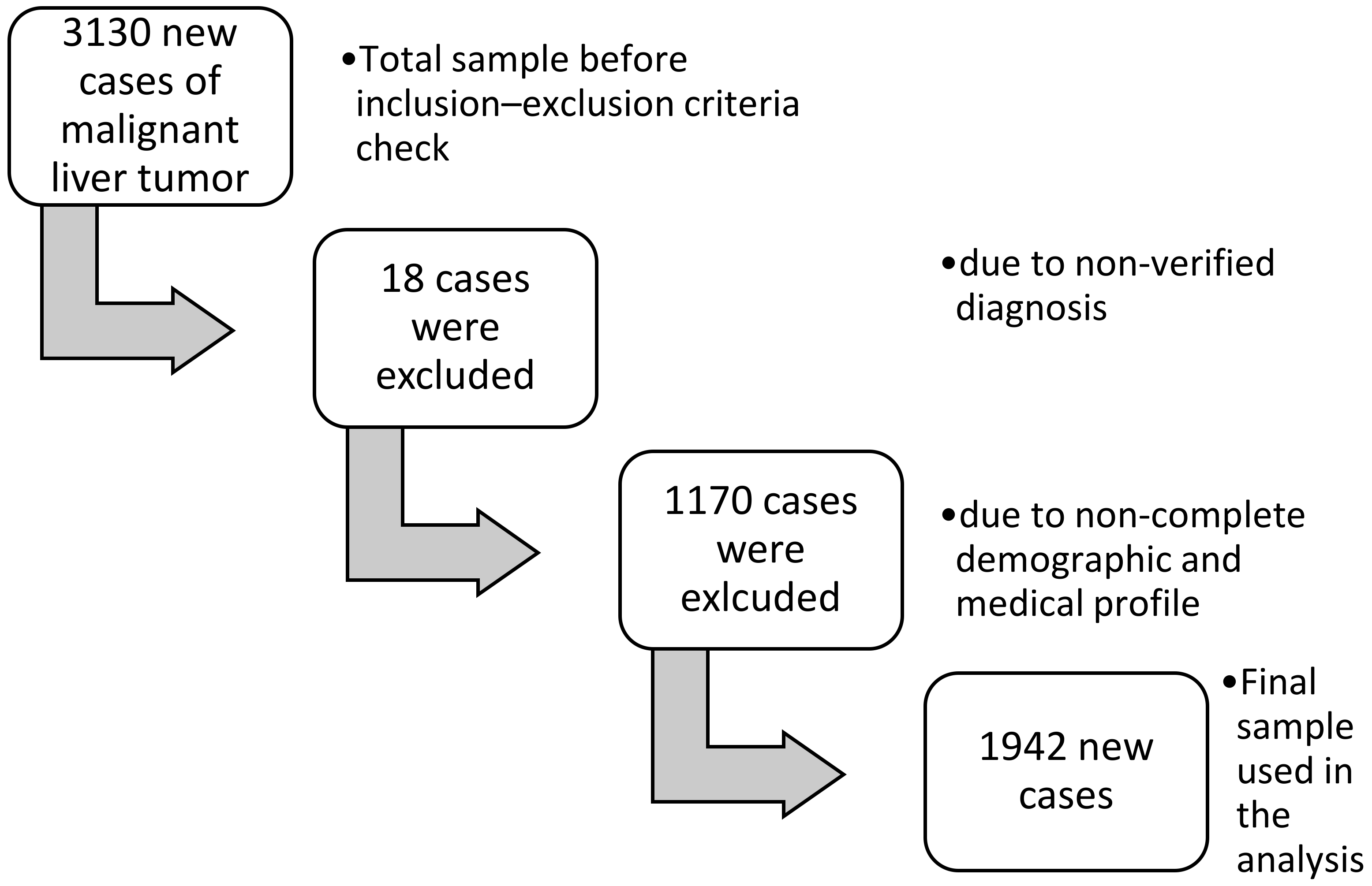
2.1. Setting and Study Population
2.2. Criteria for Inclusion in the Study
2.3. Variables Recorded in the Study
2.4. Measures
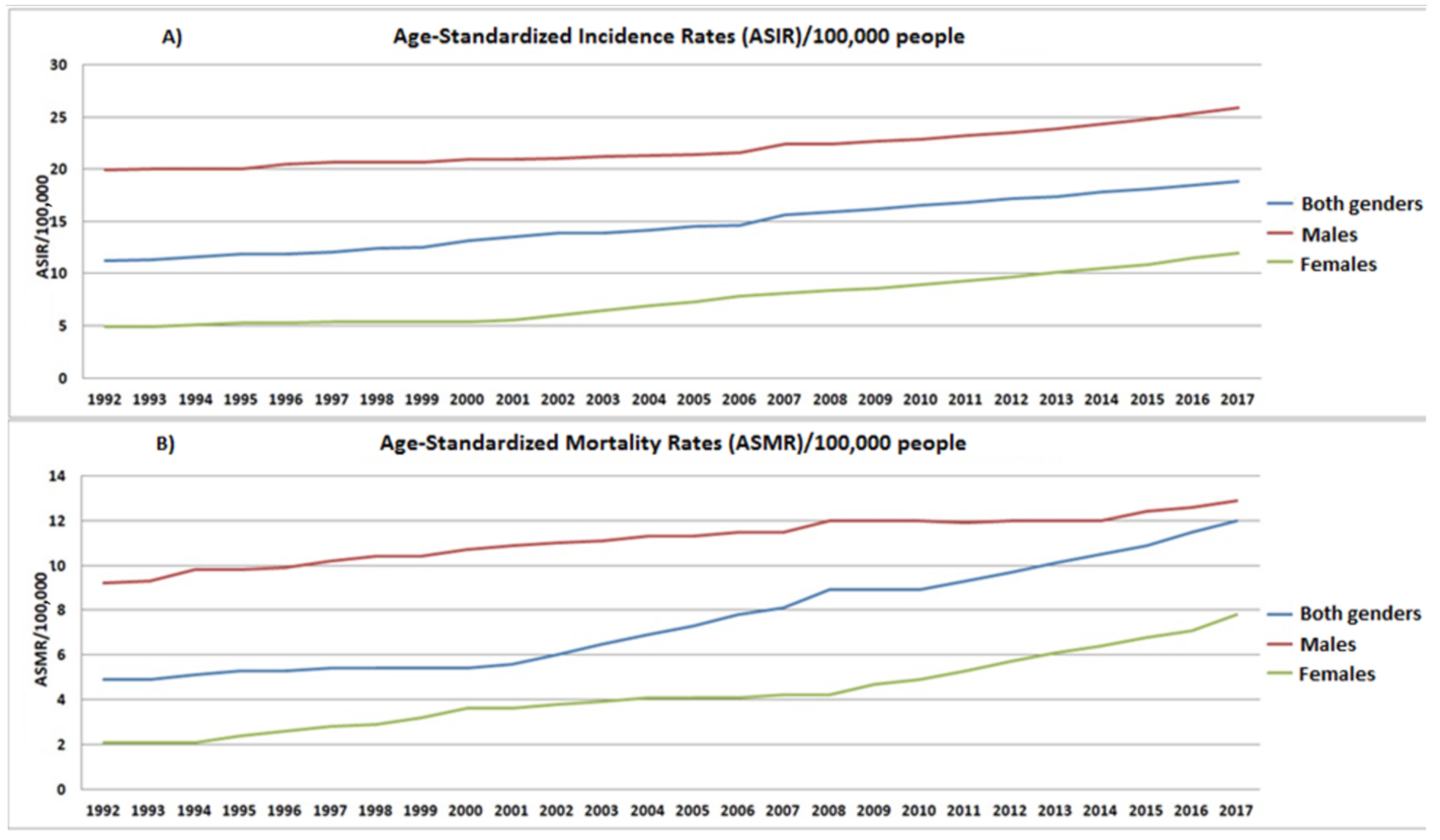
- Age-standardized incidence rates (ASIR)
- Age-standardized mortality rates (ASMR)
2.5. Statistical Analysis
2.6. Ethical Approval
3. Results
3.1. Morbidity and Mortality from Malignant Liver Tumor
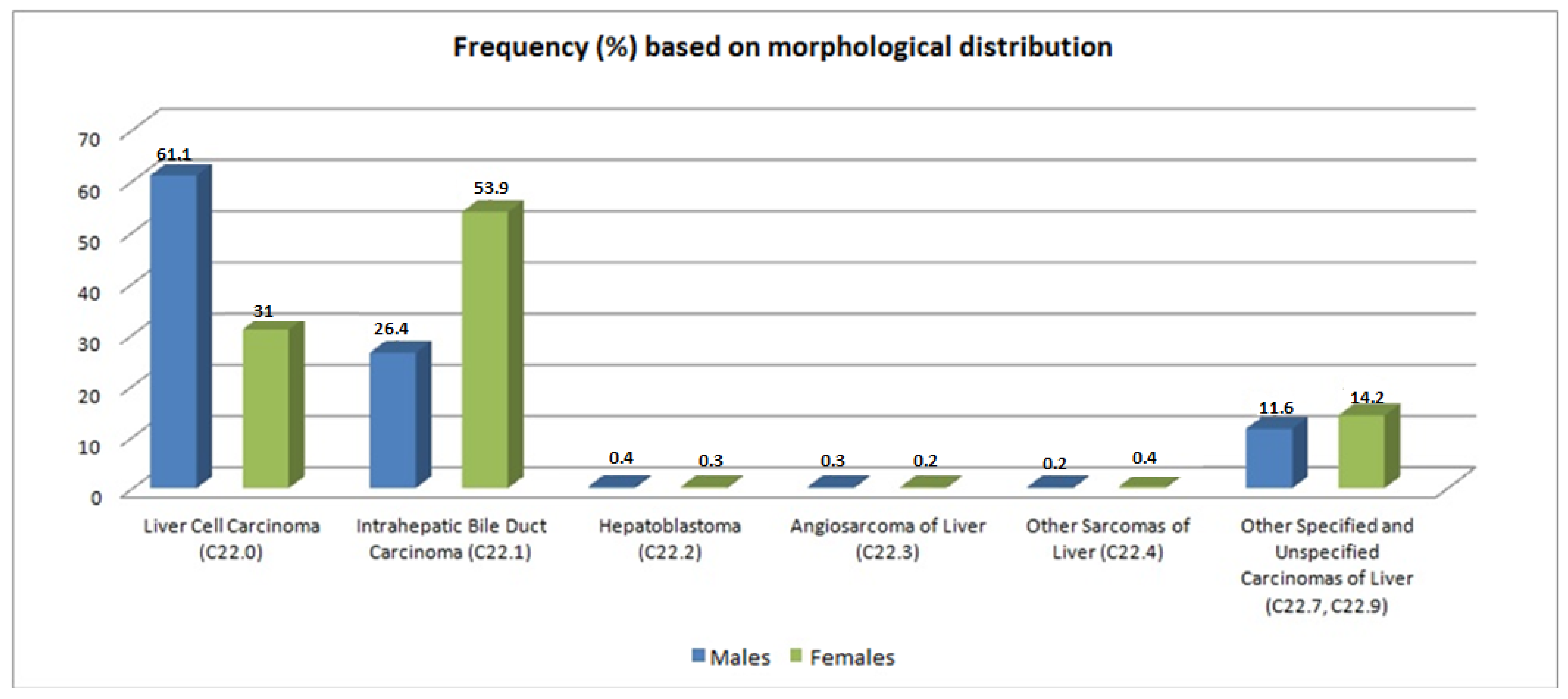
3.2. Types of Malignant Liver Tumors
3.3. Therapy
3.4. Survival Rate
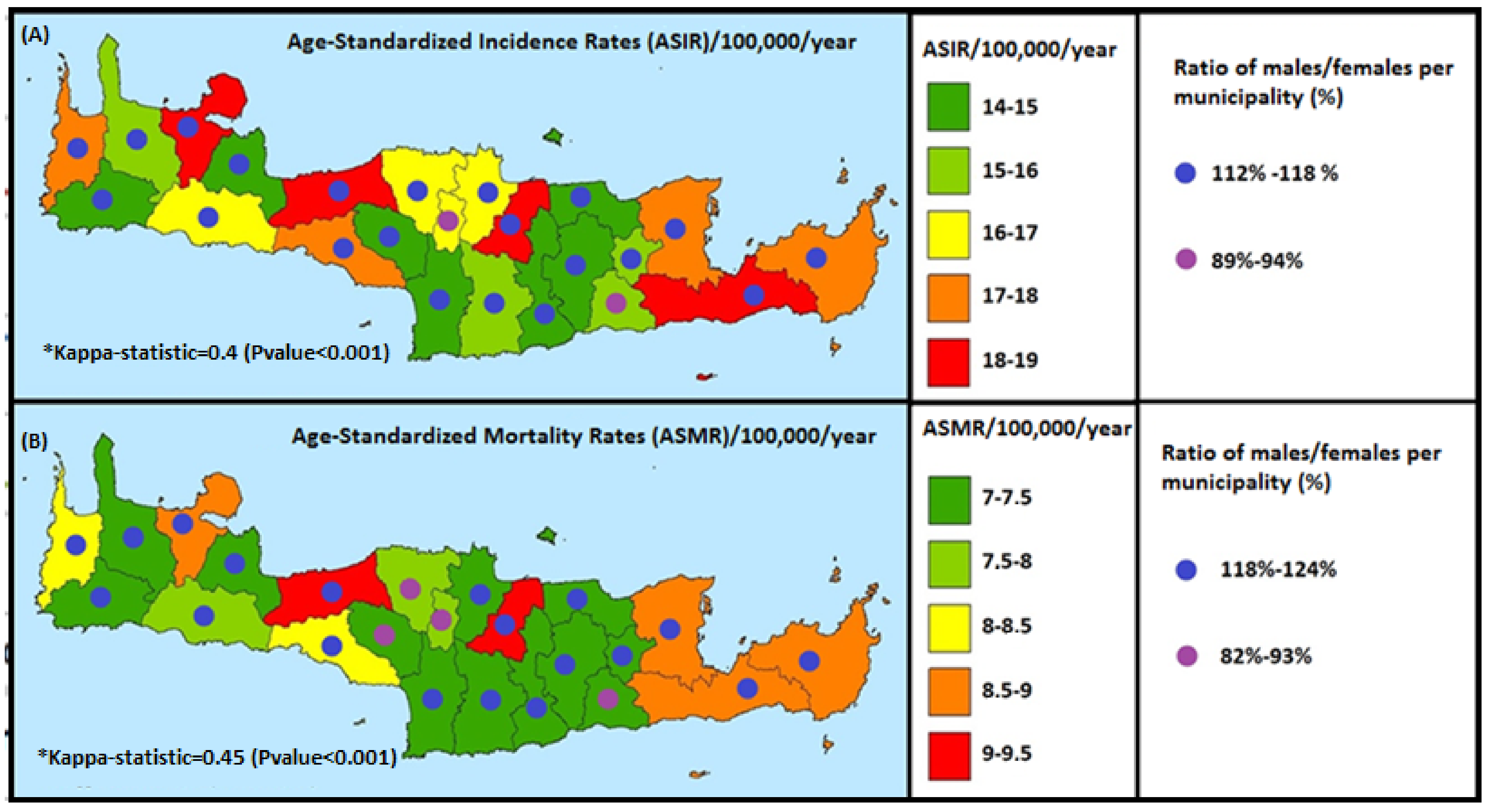
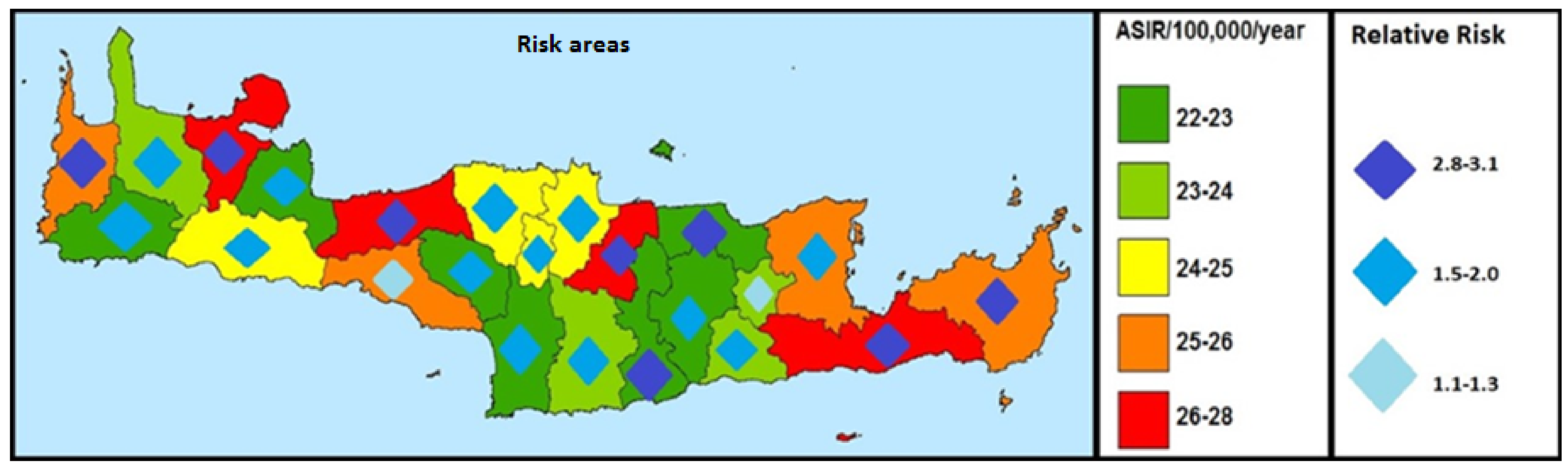
3.5. Geographical Distribution
3.6. Relative Risk (RR)
4. Discussion
4.1. Main Findings
4.2. Reading Local Data with the Existing Literature
4.3. Strengths and Limitations
4.4. Impact of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Li, L.; Wang, H. Mini-review Heterogeneity of liver cancer and personalized therapy. Cancer Lett. 2015, 379, 191–197. [Google Scholar] [CrossRef] [PubMed]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Banales, J.M.; Cardinale, V.; Carpino, G.; Marzioni, M.; Andersen, J.B.; Invernizzi, P.; Lind, G.E.; Folseraas, T.; Forbes, S.J.; Fouassier, L.; et al. Expert consensus document: Cholangiocarcinoma: Current knowledge and future perspectives consensus statement from the European Network for the Study of Cholangiocarcinoma (ENS-CCA). Nat. Rev. Gastroenterol. Hepatol. 2016, 13, 261–280. [Google Scholar] [CrossRef] [PubMed]
- Spolverato, G.; Kim, Y.; Ejaz, A.; Alexandrescu, S.; Marques, H.; Aldrighetti, L.; Gamblin, T.C.; Pulitano, C.; Bauer, T.W.; Shen, F.; et al. Conditional probability of longterm survival after liver resection for intrahepatic cholangiocarcinoma: A multi-institutional analysis of 535 patients. JAMA Surg. 2015, 150, 538–545. [Google Scholar] [CrossRef]
- Ferlay, J.; Steliarova-Foucher, E.; Lortet-Tieulent, J.; Rosso, S.; Coebergh, J.W.W.; Comber, H.; Forman, D.; Bray, F. Cancer incidence and mortality patterns in Europe: Estimates for 40 countries in 2012. Eur. J. Cancer. 2013, 49, 1374–1403. [Google Scholar] [CrossRef]
- Kouroumalis, E.A.; Skordilis, P.G.; Moschandrea, J.; Alexandrakis, G.; Charoulakis, N.; Tzardi, M.; Manousos, O.N. Natural history of advanced hepatocellular carcinoma in Crete. Association with hepatitis C virus. Eur. J. Gastroenterol. Hepatol. 1997, 9, 981–988. [Google Scholar] [CrossRef]
- Karageorgos, S.A.; Stratakou, S.; Koulentaki, M.; Voumvouraki, A.; Mantaka, A.; Samonakis, D.; Notas, G.; Kouroumalis, E.A. Long-term change in incidence and risk factors of cirrhosis and hepatocellular carcinoma in Crete, Greece: A 25-year study. Ann. Gastroenterol. 2017, 30, 357. [Google Scholar] [CrossRef]
- Sifaki-Pistolla, D.; Karageorgos, S.A.; Koulentaki, M.; Samonakis, D.; Stratakou, S.; Digenakis, E.; Kouroumalis, E. Geoepidemiology of hepatocellular carcinoma in the island of Crete, Greece. A possible role of pesticides. Liver Int. 2016, 36, 588–594. [Google Scholar] [CrossRef]
- Hadziyannis, S.; Tabor, E.; Kaklamani, E.; Tzonou, A.; Stuver, S.; Tassopoulos, N.; Mueller, N.; Trichopoulos, D. A case-control study of hepatitis B and C virus infections in the etiology of hepatocellular carcinoma. Int. J. Cancer 1995, 60, 627–631. [Google Scholar] [CrossRef]
- Kamposioras, K.; Mauri, D.; Alevizaki, P.; Ferentinos, G.; Karampoiki, V.; Kouiroukidou, P.; Zorba, E.; Proiskos, A.; Chasioti, D.; Panou, C.; et al. Cancer screening in Greece. Guideline awareness and prescription behavior among Hellenic physicians. Eur. J. Intern. Med. 2008, 19, 452–460. [Google Scholar] [CrossRef]
- Symvoulakis, E.K.; Zaravinos, A.; Panutsopulos, D.; Zoras, O.; Papalambros, E.; Sigala, F.; Spandidos, D.A. Highly conserved sequence of exon 15 BRAF gene and KRAS codon 12 mutation among Greek patients with colorectal cancer. Int. J. Biol. Markers 2007, 22, 12–18. [Google Scholar] [CrossRef]
- Bosetti, C.; Turati, F.; La Vecchia, C. Hepatocellular carcinoma epidemiology. Best Pract. Res. Clin. Gastroenterol. 2014, 28, 753–770. [Google Scholar] [CrossRef]
- Markakis, G.E.; Koulouris, A.; Tampaki, M.; Cholongitas, E.; Deutsch, M.; Papatheodoridis, G.V.; Koskinas, J. The changing epidemiology of hepatocellular carcinoma in Greece. Ann. Gastroenterol. 2022, 35, 88. [Google Scholar] [CrossRef]
- Anwar, W.A.; Khaled, H.M.; Amra, H.A.E.S.; El-Nezami, H.; Loffredo, C.A. Changing pattern of hepatocellular carcinoma (HCC) and its risk factors in Egypt: Possibilities for prevention. Mutat. Res. Rev. Mutat. Res. 2008, 659, 176–184. [Google Scholar] [CrossRef]
- Couri, T.; Pillai, A. Goals and targets for personalized therapy for HCC. Hepatol. Int. 2019, 13, 125–137. [Google Scholar] [CrossRef]
- Tang, A.; Hallouch, O.; Chernyak, V.; Kamaya, A.; Sirlin, C.B. Epidemiology of hepatocellular carcinoma: Target population for surveillance and diagnosis. Abdom. Radiol. 2018, 43, 13–25. [Google Scholar] [CrossRef]
- Li, L.; Lan, X. Association between hepatitis B virus/hepatitis C virus infection and primary hepatocellular carcinoma risk: A meta-Analysis based on Chinese population. J. Cancer Res. Ther. 2016, 12, C284–C287. [Google Scholar]
- Volk, M.L.; Lok, A.S.F. Is family history of liver cancer a risk factor for hepatocellular carcinoma? J. Hepatol. 2009, 50, 247–248. [Google Scholar] [CrossRef]
- Park, C.-H.; Jeong, S.-H.; Yim, H.-W.; Kim, J.D.; Bae, S.H.; Choi, J.Y.; Yoon, S.K. Family history influences the early onset of hepatocellular carcinoma. World J. Gastroenterol. 2012, 18, 2661–2667. [Google Scholar] [CrossRef]
- Wong, C.R.; Nguyen, M.H.; Lim, J.K. Hepatocellular carcinoma in patients with non-alcoholic fatty liver disease. World J. Gastroenterol. 2016, 22, 8294–8303. [Google Scholar] [CrossRef]
- Anastasaki, M.; Papadakis, S.; Linardakis, M.; Anyfantakis, D.; Symvoulakis, E.K.; Lionis, C.; on behalf of the Cretan Primary Care Research Group. Burden of metabolic syndrome among primary care patients in Crete, Greece: A descriptive study. Eur. J. General. Pract. 2020, 26, 166–174. [Google Scholar] [CrossRef]
- Arlsen, T.H.; Sheron, N.; Zelber-Sagi, S.; Carrieri, P.; Dusheiko, G.; Bugianesi, E.; Pryke, R.; Hutchinson, S.J.; Sangro, B.; Martin, N.K.; et al. The EASL–Lancet Liver Commission: Protecting the next generation of Europeans against liver disease complications and premature mortality. Lancet 2022, 399, 61–116. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | With Malignant Liver Tumor | p-Value | |
|---|---|---|---|
| n = 2022 | % | ||
| Sex | 0.03 | ||
| Male | 1490 | 73.7 | |
| Female | 532 | 26.3 | |
| Age at diagnosis | 64 | 3.4 | <0.001 |
| Stage at diagnosis | 0.04 | ||
| I | 495 | 24.5 | |
| II | 907 | 44.8 | |
| III | 396 | 19.6 | |
| IV | 126 | 6.2 | |
| Unknown | 98 | 4.8 | |
| Obesity (based on BMI) | 495 | 24.5 | 0.04 |
| Individual medical history of cancer | 0.03 | ||
| No | 719 | 35.5 | |
| Yes (apart from malignant liver tumor) | 1280 | 63.3 | |
| Unknown | 23 | 1.1 | |
| Individual history of Hepatitis B and C | 632 | 34.2 | 0.04 |
| Family medical history | 0.02 | ||
| No | 211 | 10.4 | |
| Malignant liver tumor | 787 | 38.9 | |
| Other malignant tumor (apart from malignant liver tumor) | 979 | 48.4 | |
| Unknown | 45 | 2.2 | |
| Degree of relationship (family history of malignant liver tumor, n = 787) | <0.001 | ||
| 1st | 557 | 70.7 | |
| 2nd | 208 | 26.4 | |
| Unknown | 22 | 2.8 | |
| Smoking | 0.01 | ||
| Non-smokers | 582 | 28.7 | |
| Smokers | 1338 | 66.1 | |
| Unknown | 102 | 5.0 | |
| Alcohol | |||
| Non-consumption | 671 | 33.2 | 0.01 |
| Consumption | 1275 | 63.1 | |
| Unknown | 76 | 3.7 | |
| Routes of diagnosis | 0.03 | ||
| Emergency clinic | 992 | 49.1 | |
| Other hospital clinics | 113 | 5.6 | |
| Referral from a general practitioner | 516 | 25.5 | |
| Another outpatient clinic/diagnostic | 208 | 10.3 | |
| Unknown | 193 | 9.5 | |
| Characteristics | Relative Risk (95%CI) | p-Value |
|---|---|---|
| Individual medical history of cancer | <0.001 | |
| No | 1 | |
| Yes (apart from malignant liver tumor) | 2.4 (2.2–2.6) | |
| Individual history of Hepatitis B and C | 2.8 (2.1–3.5) | 0.03 |
| Family medical history | 0.02 | |
| No | 1 | |
| Malignant liver tumor | 2.3 (2.0–2.6) | |
| Other type of cancer (apart from malignant liver tumor) | 1.8 (1.4–2.2) | |
| Degree of relationship | <0.001 | |
| 2nd | 1 | |
| 1st | 2.9 (2.8–3.1) | |
| Obesity (based on BMI) | 0.04 | |
| No | 1 | |
| Yes | 1.7 (1.1–2.3) | |
| Alcohol consumption | 0.01 | |
| Non-consumption | 1 | |
| Consumption | 3.1 (2.4–3.8) | 0.03 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kalpadakis, S.; Sifaki-Pistolla, D.; Symvoulakis, E.K.; Kelefiotis-Stratidakis, P.; Vamvakas, L.; Mavroudis, D.; Lionis, C. Reporting Liver Cancer Trends in the Island of Crete, Greece: Results from a Geo-Epidemiological Study. Int. J. Environ. Res. Public Health 2022, 19, 10166. https://doi.org/10.3390/ijerph191610166
Kalpadakis S, Sifaki-Pistolla D, Symvoulakis EK, Kelefiotis-Stratidakis P, Vamvakas L, Mavroudis D, Lionis C. Reporting Liver Cancer Trends in the Island of Crete, Greece: Results from a Geo-Epidemiological Study. International Journal of Environmental Research and Public Health. 2022; 19(16):10166. https://doi.org/10.3390/ijerph191610166
Chicago/Turabian StyleKalpadakis, Stavros, Dimitra Sifaki-Pistolla, Emmanouil K. Symvoulakis, Panagiotis Kelefiotis-Stratidakis, Lambros Vamvakas, Dimitrios Mavroudis, and Christos Lionis. 2022. "Reporting Liver Cancer Trends in the Island of Crete, Greece: Results from a Geo-Epidemiological Study" International Journal of Environmental Research and Public Health 19, no. 16: 10166. https://doi.org/10.3390/ijerph191610166