
Non-Specific Low Back Pain, Dietary Salt Intake, and Posterior Lumbar Subcutaneous Edema


School of Public Health Sciences, University of Waterloo, Waterloo, ON N2L 3G1, Canada
Int. J. Environ. Res. Public Health 2022, 19(15), 9158; https://doi.org/10.3390/ijerph19159158
Submission received: 5 July 2022
/
Revised: 16 July 2022
/
Accepted: 25 July 2022
/
Published: 27 July 2022
(This article belongs to the Special Issue Second Edition: Low Back Pain (LBP))
{kind=link}
{kind=link}
{kind=link}
Abstract
:Low back pain is the world’s leading disability, but the etiology of the majority of low back pain is non-specific with no known cause. Moreover, overuse of opioids to treat low back pain is a widespread problem. This paper proposes that non-specific low back pain may be associated with excessive intake of dietary salt, potentially mediated by posterior lumbar subcutaneous edema. In addition to pain, symptoms of edema include swelling, tightness, and stiff joints, which are common complaints of people with low back pain, along with restricted lumbar range of motion and impaired mobility. Many global populations consume excess sodium chloride, which can lead to fluid overload in hypervolemia, and cause swelling and temporary weight gain associated with low back pain. Numerous conditions comorbid with low back pain are also potentially mediated by excessive salt intake, including migraine headache, hypertension, cardiovascular disease, venous thromboembolism, liver disease, respiratory disorders, chronic kidney disease, pregnancy complications, and multiple sclerosis. Novel approaches to identify and prevent the cause of non-specific low back pain have potential to reduce disability worldwide by reducing low back pain prevalence. More research is needed to confirm the involvement of dietary salt and posterior lumbar subcutaneous edema in non-specific low back pain.
1. Introduction
For the past three decades, low back pain (LBP) has been the world-leading non-fatal cause of disability [1], burdening the U.S. healthcare system with costs exceeded only by diabetes and ischemic heart disease [2]. However, with the exception of LPB arising from pathological mechanisms, specific causes of most LPB (~85%) are unknown [3,4]. Discussing management of non-specific low back pain, the Lancet noted that overuse of opioids, diagnostic imaging, and surgery “remains a widespread problem” [5]. Back pain (in general) is the second most common diagnosis for opioid prescriptions in emergency departments, next to non-fracture injuries, and 45.2% of patients with back pain receive opioids [6]. Other researchers pointed out that although opioids have short-term analgesic effects in chronic back pain, “benefits for function are less clear” [7]. Furthermore, “complications of opioid use include addiction and overdose related mortality, which have risen in parallel with prescription rates.” On the other hand, from a primary prevention perspective, the Lancet predicted that novel approaches to identify and mitigate the cause of non-specific LBP have “potential to help the many people with disabling low back pain worldwide” [5].
Excess body weight has been associated with overall back pain [8], but not all overweight people have back pain, nor are all people with back pain overweight, implying that other etiological factors are involved. Even highly conditioned athletes commonly have low back pain from a “benign” source [9]. Additionally, low-quality dietary patterns with high intake of sodium, saturated fat, and added sugars have been associated with spinal pain [10]. Excessive sodium in the body can cause increased water retention in edema, which could affect tissues involved in LBP of young and old individuals, regardless of body weight and health status.
This perspective article proposes a biological mechanism in which non-specific LBP is associated with excessive dietary salt intake, potentially mediated by posterior lumbar subcutaneous edema. Using a grounded theory approach to review the research literature [11], evidence based on research findings was retrieved from a keyword search for “low back pain”, “dietary sodium”, “sodium chloride”, “salt”, and “posterior lumbar subcutaneous edema”. Additional keywords were used to search for various conditions comorbid with low back pain. Studies cited in retrieved literature were used to expand the literature search. Research findings were examined by comparative analysis for similarities and differences in concepts, and concepts were combined into interrelated themes. Through an iterative process of retrieving additional information from the literature (theoretical sampling), an evidence-based explanatory theory linking salt with LBP was gradually induced until no more new knowledge was obtained (theoretical saturation). Evidence from the grounded theory presented in this paper provides novel insights and new directions for further research and hypothesis testing in the etiology of non-specific LBP potentially related to salt intake.
2. Posterior Lumbar Subcutaneous Edema
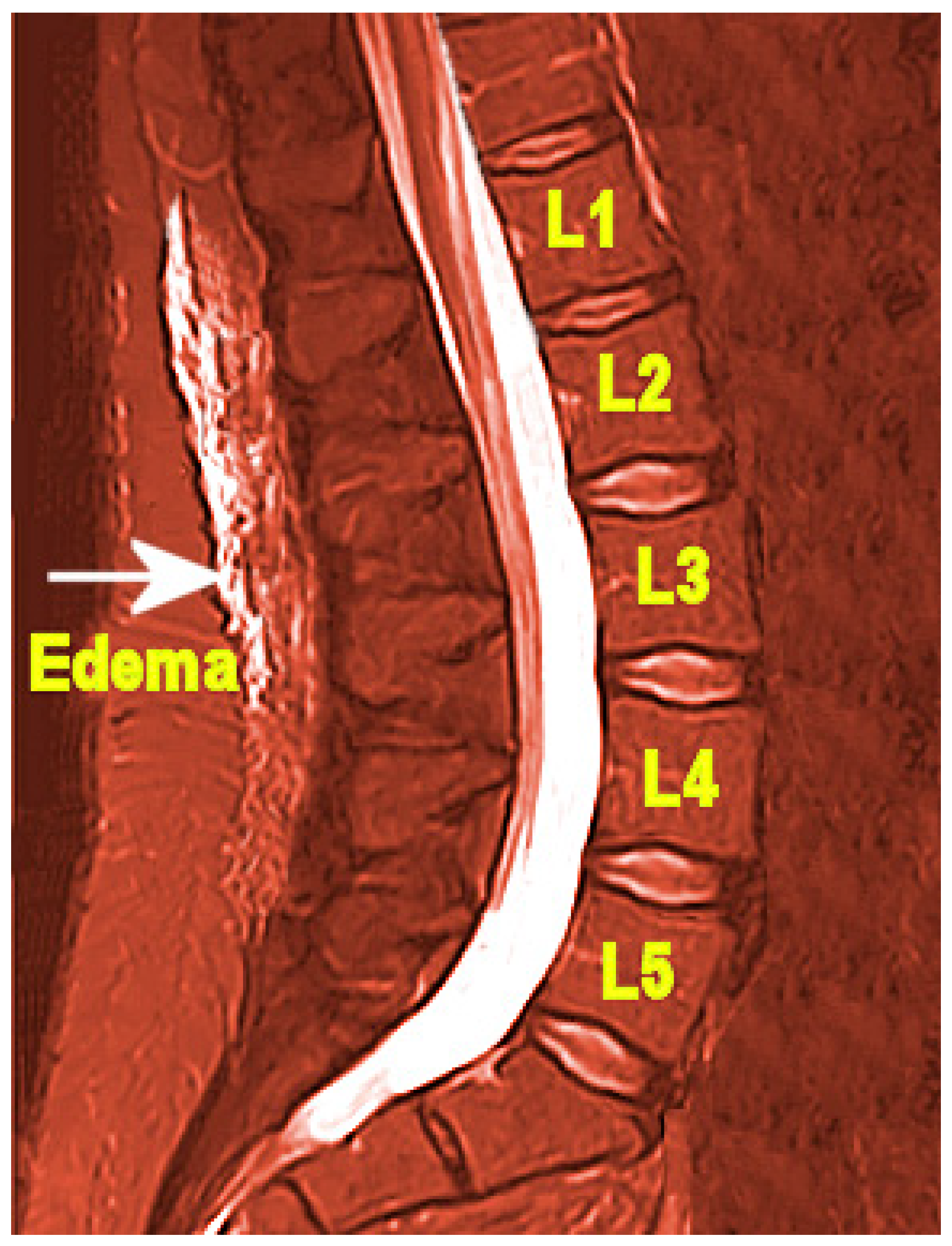
Posterior lumbar subcutaneous edema (PLSE) affects deep perifascial soft tissue in the lumbar spine (lumbar vertebrae L1–L5), which is commonly ignored as an incidental finding on spinal magnetic resonance images (MRI), shown in Figure 1 [12]. Importantly, PLSE should not be confused with edema caused by serious trauma and injury. In addition to subcutaneous edema, a case control study found that structures within the lumbar spine may also be affected by edema associated with LBP, such as interspinous ligament edema, facet joint effusion, paraspinal muscle edema, as well as neocyst formation [13]. An important study limitation is that “there was no correlation between the lesions and the intensity of symptoms (degree of pain)”.
Symptoms of edema include swelling, tightness, pain, and stiff joints [14], and cases with PLSE may be accompanied by these edema symptoms. Similar to pain and limited mobility with restricted range of motion associated with edema of peripheral limbs [15], LBP is associated with restricted lumbar range of motion and mobility impairment, sometimes in combination with lower extremity pain [16]. Additionally, qualitative studies of patients with LBP report symptoms of stiffness, which is consistent with tightness and stiff joints from edema [17], although the authors noted that “feeling stiff” is not a reliable biomarker of biomechanical impairment. Importantly, the Mayo Foundation for Medical Education and Research, associated with the Mayo Clinic—the top ranked U.S. hospital in 2021–2022 [18], listed adverse effects from medical administration of sodium chloride. Listed symptoms include joint pain, stiffness and swelling when given orally [19] and pain of the low back when injected [20].
3. Salt and Hypervolemia
Swelling and temporary weight gain in edema is often associated with fluid overload in hypervolemia due to sodium and water retention; as the body’s total sodium content increases, serum levels of sodium in hypervolemia can be high, normal, or low [21], (hypernatremia, eunatremia, and hyponatremia, respectively). Serum sodium becomes dysregulated when renal function is burdened, especially in combination with high dietary sodium intake [22]. The body’s requirement for sodium is low, 500 mg per day [23]. Yet, salt (sodium chloride) contributes excessive amounts of sodium in the diet of many global populations, with an average salt intake of 9−12 g per day [24]. Importantly, the taste for salt decreases as people are exposed to lower dietary intake levels [25]. Potassium also aids renal elimination of sodium to maintain sodium and fluid balance, but dietary potassium intake is often inadequate as consumption of processed foods increases in many populations.
Figure 2 is a directed acyclic graph illustrating the proposed causative pathways (solid lines) in which posterior lumbar subcutaneous edema potentially mediates the association (dotted line) between increased sodium chloride intake and non-specific low back pain. Note that a mediator, or an intermediate variable, is a causative factor that “lies on the causal pathway” [26].
4. Salt Transitively Links Low Back Pain and Comorbid Conditions
Additional evidence that excessive sodium chloride intake is a potential mediator or causative factor in nonspecific LBP is implied in numerous associations of LBP with comorbid conditions mediated by salt, including migraine headache, hypertension, cardiovascular disease, venous thromboembolism, liver disease, respiratory disorders, chronic kidney disease, pregnancy complications, and multiple sclerosis.
Analysis of research findings in this section uses a transitive inference method, inferring that salt is a common causative factor related to both non-specific LBP and comorbid conditions that are also associated with salt intake. Transitive inference is a technique used in literature-based discovery (LBD) to synthesize new knowledge from disjointed knowledge domains [27]. If concepts A and C from separate knowledge domains are each associated with concept B, a novel association is inferred between A and C through B. This technique is useful for exploring new insights and directions for future research in a new area.
As shown in Figure 3, the following subsections describe evidence transitively linking non-specific LBP (A) with specific comorbid conditions (C), through the common mediating factor of increased salt intake (B). For evidence linking non-specific LBP with increased sodium chloride intake and PLSE, the reader is referred to Section 2 and Section 3 and Figure 2 of this paper. Future studies should investigate prevalence of PLSE in conditions comorbid with non-specific LBP.
4.1. Migraine Headache and Low Back Pain
Earlier research found that patients had a high prevalence of migraine headache following back pain [28,29]. More recently, a positive association of primary chronic headaches with persistent LBP was found in a systematic review of 14 studies [30], with odds ratios across a variety of populations ranging from 1.55 (95% CI 1.13–2.11) to 8.00 (95% CI 5.3–12.1). The researchers noted that “there might be a particular association between migraine and persistent back pain mediated through a specific biological mechanism.” Of relevance, clinical trials show lower salt intake is associated with reduced headaches [31,32], and migraine headache pain has been linked to withdrawal symptoms of salt intake [33], suggesting that salt mediates the association of headache with LBP. Importantly, increased water retention, similar to edema linked to salt intake, has been observed before the onset of migraine [34].
4.2. Hypertension and Low Back Pain
People with hypertension have a greater reduction in blood pressure from reduced sodium intake compared to people with normal blood pressure, and populations with lower sodium intake have overall lower blood pressure compared to other populations [35]. Low sodium intake in combination with the Dietary Approaches to Stop Hypertension (DASH) diet has been shown to reduce prehypertension or stage 1 hypertension [36].
Nevertheless, some studies found an inverse association of hypertension with LBP [37], which contradicts a potential relationship between high salt intake and non-specific LBP. However, the relationship between LBP and hypertension is complicated by the fact that chronic pain increases blood pressure through sympathetic nervous system responses [38]. This relationship between chronic pain and hypertension is reversed in acute pain in which sensitivity to pain is lowered through hypertension-associated hypoalgesia, which could account for inverse associations of acute LBP with hypertension in some studies. Furthermore, pain relief through use of nonsteroidal anti-inflammatory drugs and acetaminophen increases blood pressure by decreasing sodium excretion and increasing vascular volume, prompting a reminder to patients taking these drugs to “limit their sodium intake” [39]. Relieving LBP with such medications that increase hypertension could also account for inverse associations of LBP with hypertension.
4.3. Cardiovascular Disease and Chronic Low Back Pain
A study of Spanish twins found that chronic LBP was associated with a 2.69 odds ratio of lifetime myocardial infarction (95% CI 1.35–5.36), and a 2.58 odds ratio of other heart diseases over a lifetime (95% CI 1.69–3.93) [40]. Although a dose–response relationship between cardiovascular disease (CVD) and salt intake is unclear, a recent systematic review and dose–response meta-analysis found that each gram of sodium intake was associated with a 6% increased risk of CVD [41]. Moreover, a high-salt diet fed to rats was shown to increase damage to cardiomyocytes of the heart, independently of blood pressure [42]. This evidence infers that salt may transitively link chronic LBP with CVD.
4.4. Venous Thromboembolism and Severe Low Back Pain
Venous thromboembolism (VTE) is associated with severe LBP [43]. Researchers reviewed multiple case histories of patients with VTE and found that patients with inferior vena cava thrombosis frequently presented with initial symptoms of inexplicable lower back pain [44]. VTE is also related to sodium imbalance in hyponatremia and hypernatremia [45]. A high-salt diet increased plasma fibrinogen, platelet counts, and neutrophils in a mouse model [46]. Elevated serum sodium levels in a mouse model also increased secretion of von Willebrand factor (vWF) which initiates blood clots, and plasma vWF and stroke risk are positively associated with elevated serum sodium in the Atherosclerosis Risk in Communities Study [47].
4.5. Liver Disease and Back Pain
An early study found that back pain was the most common complaint among 54% of 239 patients with chronic hepatitis C [48]. Patients with liver cirrhosis had an increased incidence of spondylodiscitis of the spine with non-specific back pain [49]. Liver function in mice is harmed by excessive salt intake, which can induce fibrosis through excessive production of reactive oxygen species [50], and transcriptome sequencing technology demonstrated that a high-salt diet caused liver abnormalities in the metabolism of numerous substances and at least 15 enzymatic activities in mice [51].
4.6. Respiratory Disorders and Low Back Pain
A systematic review of 16 studies found a significant association between LBP and respiratory disorders, including respiratory infections, asthma, certain allergies, and dyspnea, but not chronic obstructive pulmonary disease [52]. The researchers suggested that biomechanical and immunological factors were among potential causes of the relationship of respiratory disorders with LBP, and further studies were recommended. A later prospective study that followed individuals from the Stockholm Public Health Cohort found that having asthma or chronic obstructive pulmonary disease at baseline was associated with a greater risk of LBP after four years follow up [53].
Of relevance, salt is a nutritional immunological factor associated with COVID-19 [54], a respiratory illness with SARS-CoV-2 infection that includes symptoms of shortness of breath, fever, congestion, headache, and body aches [55]. Changes in immune response from sodium chloride promote inflammation with increased inflammatory cytokines [56], which are prevalent in severe cases of COVID-19. The gummy yellow fluid observed to fill the air sacs of lungs in seriously ill COVID-19 patients appears similar to the yellow fluid in pulmonary edema [57,58], which could be related to excessive sodium intake.
A meta-analysis of 51 studies investigated prevalence of musculoskeletal and neurological manifestations in COVID-19. Next to cases with myalgia and headache, with prevalence of 19% and 12%, respectively, general back pain was prevalent in 10% of COVID-19 cases [59]. Another study found that hospitalized COVID-19 patients complained of pain an average of 2.2 days before admission, and among 133 COVID-19 patients admitted with pain, LBP accounted for 43.6% of complaints [60].
4.7. Chronic Kidney Disease and Low Back Pain
Excessive salt intake harms kidneys by activating inflammatory responses and inducing fibrosis in renal tissue, which reduces kidney blood vessel density [22]. A low-sodium diet is useful in all stages of chronic kidney disease to reduce fluid overload, hypertension, and proteinuria in non-dialysis patients [61]. Moreover, a cross sectional study found that hemodialysis is associated with non-specific LBP in a majority of patients receiving hemodialysis, and LBP is associated with lower health-related quality of life among hemodialysis patients [62].
4.8. Pregnancy Complications and Low Back Pain
LBP affects 86% of pregnant women during the third trimester, and may persist for many months after delivery [63]. It is not clear if lordosis that normally occurs in the curvature of the lumbar spine during pregnancy is a causative factor of low back pain. Pregnant women with low back pain have worse quality of life and higher levels of sick leave than other pregnant women. Whether LBP in pregnancy and non-specific LBP “share similar underlying physiological mechanisms is still up for debate.” Furthermore, a previous history of LBP before pregnancy is one of the strongest predictors of LBP during pregnancy. Although earlier studies showed no benefit from sodium restriction in preventing pregnancy complications, a more recent study of Danish pregnant women found that lower dietary sodium intake to reduce risk of cardiovascular disease was associated with decreased risk of hypertensive disorders of pregnancy, including gestational hypertension and preeclampsia [64].
4.9. Multiple Sclerosis and Low Back Pain
A recent systematic review found that the prevalence of LBP in the French multiple sclerosis (MS) population ranged between 41.6% to 52.4%, which is two to three times as high as in the general population [65]. The study found that LBP in MS is the leading cause of limitation in daily activities, but the pathophysiology of LBP in MS remains unknown. Another study found that medium and high levels of dietary sodium compared to low levels consumed by MS patients were associated with 2.75 to 3.95 times worse clinical and MRI outcomes, respectively [66]. Excess dietary sodium chloride is proposed to induce pro-inflammatory mechanisms in the pathophysiology of MS [67], and high salt concentrations in experimental animal models produced pathological changes in the structure of myelin sheaths that protect neurons, which researchers suggested could explain demyelination in MS [68].
5. Conclusions
Novel primary prevention approaches to identify and mitigate the cause of non-specific LBP have potential to reduce disability worldwide. This paper presented evidence that posterior lumbar subcutaneous edema potentially mediates the association of increased dietary salt intake with non-specific low back pain. Salt is also a mediating factor in the transitive relationship between LBP and many comorbid conditions. More research is needed to confirm the mediating role of posterior lumbar subcutaneous edema in the proposed association of increased sodium chloride intake with non-specific low back pain and comorbid conditions. Additionally, future clinical research should explore the feasibility of using a salt-reduced diet for the reduction and prevention of non-specific LBP.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Conflicts of Interest
The author declares no conflict of interest.
References
- James, S.L.; Abate, D.; Abate, K.H.; Abay, S.M.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdela, J.; Abdelalim, A. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar] [CrossRef] [Green Version]
- Kim, L.H.; Vail, D.; Azad, T.D.; Bentley, J.P.; Zhang, Y.; Ho, A.L.; Fatemi, P.; Feng, A.; Varshneya, K.; Desai, M.; et al. Expenditures and Health Care Utilization Among Adults With Newly Diagnosed Low Back and Lower Extremity Pain. JAMA Netw. Open 2019, 2, e193676. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hartvigsen, J.; Hancock, M.J.; Kongsted, A.; Louw, Q.; Ferreira, M.L.; Genevay, S.; Hoy, D.; Karppinen, J.; Pransky, G.; Sieper, J. What low back pain is and why we need to pay attention. Lancet 2018, 391, 2356–2367. [Google Scholar] [CrossRef] [Green Version]
- Koch, C.; Hänsel, F. Non-specific Low Back Pain and Postural Control During Quiet Standing—A Systematic Review. Front. Psychol. 2019, 10, 586. [Google Scholar] [CrossRef] [PubMed]
- Maher, C.; Underwood, M.; Buchbinder, R. Non-specific low back pain. Lancet 2017, 389, 736–747. [Google Scholar] [CrossRef] [Green Version]
- Kea, B.; Fu, R.; Lowe, R.A.; Sun, B.C. Interpreting the National Hospital Ambulatory Medical Care Survey: United States Emergency Department Opioid Prescribing, 2006–2010. Acad. Emerg. Med. 2016, 23, 159–165. [Google Scholar] [CrossRef] [Green Version]
- Deyo, R.A.; Von Korff, M.; Duhrkoop, D. Opioids for low back pain. BMJ 2015, 350, g6380. [Google Scholar] [CrossRef] [PubMed]
- Perera, R.S.; Chen, L.; Hart, D.J.; Spector, T.D.; Arden, N.K.; Ferreira, M.L.; Radojčić, M.R. Effects of body weight and fat mass on back pain—direct mechanical or indirect through inflammatory and metabolic parameters? Semin. Arthritis Rheum. 2022, 52, 151935. [Google Scholar] [CrossRef]
- Mortazavi, J.; Zebardast, J.; Mirzashahi, B. Low Back Pain in Athletes. Asian J. Sports Med. 2015, 6, e24718. [Google Scholar] [CrossRef] [Green Version]
- Zick, S.M.; Murphy, S.L.; Colacino, J. Association of chronic spinal pain with diet quality. Pain Rep. 2020, 5, e837. [Google Scholar] [CrossRef]
- Wolfswinkel, J.F.; Furtmueller, E.; Wilderom, C.P.M. Using grounded theory as a method for rigorously reviewing literature. Eur. J. Inf. Syst. 2013, 22, 45–55. [Google Scholar] [CrossRef]
- Schwarz-Nemec, U.; Friedrich, K.M.; Arnoldner, M.A.; Schwarz, F.K.; Weber, M.; Trattnig, S.; Grohs, J.G.; Nemec, S.F. When an incidental MRI finding becomes a clinical issue: Posterior lumbar subcutaneous edema in degenerative, inflammatory, and infectious conditions of the lumbar spine. Wien. Klin. Wochenschr. 2020, 132, 27–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lakadamyali, H.; Tarhan, N.C.; Ergun, T.; Cakir, B.; Agildere, A.M. STIR sequence for depiction of degenerative changes in posterior stabilizing elements in patients with lower back pain. Am. J. Roentgenol. 2008, 191, 973–979. [Google Scholar] [CrossRef] [PubMed]
- Brazier, Y. Everything You Need to Know about Edema. Available online: https://www.medicalnewstoday.com/articles/159111#_noHeaderPrefixedContent (accessed on 21 April 2022).
- Besharat, S.; Grol-Prokopczyk, H.; Gao, S.; Feng, C.; Akwaa, F.; Gewandter, J.S. Peripheral edema: A common and persistent health problem for older Americans. PLoS ONE 2021, 16, e0260742. [Google Scholar] [CrossRef]
- Delitto, A.; George, S.Z.; Van Dillen, L.; Whitman, J.M.; Sowa, G.; Shekelle, P.; Denninger, T.R.; Godges, J.J. Low back pain: Clinical practice guidelines linked to the International Classification of Functioning, Disability, and Health from the Orthopaedic Section of the American Physical Therapy Association. J. Orthop. Sports Phys. Ther. 2012, 42, A1–A57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stanton, T.R.; Moseley, G.L.; Wong, A.Y.L.; Kawchuk, G.N. Feeling stiffness in the back: A protective perceptual inference in chronic back pain. Sci. Rep. 2017, 7, 9681. [Google Scholar] [CrossRef] [Green Version]
- U.S. News Best Hospitals. Available online: https://health.usnews.com/best-hospitals (accessed on 22 June 2022).
- MFMER. Sodium Chloride (Oral Route) Side Effects. Mayo Foundation for Medical Education and Research. Available online: https://www.mayoclinic.org/drugs-supplements/sodium-chloride-oral-route/side-effects/drg-20122545 (accessed on 23 June 2022).
- Sodium Chloride (Injection Route) Side Effects. Available online: https://www.mayoclinic.org/drugs-supplements/sodium-chloride-injection-route/side-effects/drg-20068846 (accessed on 2 May 2022).
- Cirino, E. Hypervolemia (Fluid Overload). Available online: https://www.healthline.com/health/hypervolemia (accessed on 22 April 2022).
- Oppelaar, J.J.; Vogt, L. Body Fluid-Independent Effects of Dietary Salt Consumption in Chronic Kidney Disease. Nutrients 2019, 11, 2779. [Google Scholar] [CrossRef] [Green Version]
- NHLBI. Implementing Recommendat Ions for Dietary Salt Reduction: Where Are We? Where Are We Going? How Do We Get There?: A Summary of an NHLBI Workshop; National Institutes of Health, National Heart, Lung, and Blood Institute: Bethesda, MA, USA, 1996.
- Salt Reduction. Available online: https://www.who.int/news-room/fact-sheets/detail/salt-reduction (accessed on 22 April 2022).
- Bertino, M.; Beauchamp, G.K.; Engelman, K. Long-term reduction in dietary sodium alters the taste of salt. Am. J. Clin. Nutr. 1982, 36, 1134–1144. [Google Scholar] [CrossRef] [Green Version]
- Imai, K.; Keele, L.; Tingley, D.; Yamamoto, T. Unpacking the Black Box of Causality: Learning about Causal Mechanisms from Experimental and Observational Studies. Am. Political Sci. Rev. 2011, 105, 765–789. [Google Scholar] [CrossRef]
- Thilakaratne, M.; Falkner, K.; Atapattu, T. A systematic review on literature-based discovery workflow. PeerJ Comput. Sci. 2019, 5, e235. [Google Scholar] [CrossRef] [Green Version]
- Duckro, P.N.; Schultz, K.T.; Chibnall, J.T. Migraine as a sequela to chronic low back pain. Headache 1994, 34, 279–281. [Google Scholar] [CrossRef] [PubMed]
- Yoon, M.S.; Manack, A.; Schramm, S.; Fritsche, G.; Obermann, M.; Diener, H.C.; Moebus, S.; Katsarava, Z. Chronic migraine and chronic tension-type headache are associated with concomitant low back pain: Results of the German Headache Consortium study. Pain 2013, 154, 484–492. [Google Scholar] [CrossRef]
- Vivekanantham, A.; Edwin, C.; Pincus, T.; Matharu, M.; Parsons, H.; Underwood, M. The association between headache and low back pain: A systematic review. J. Headache Pain 2019, 20, 82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amer, M.; Woodward, M.; Appel, L.J. Effects of dietary sodium and the DASH diet on the occurrence of headaches: Results from randomised multicentre DASH-Sodium clinical trial. BMJ Open 2014, 4, e006671. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Zhang, Z.; Chen, W.; Whelton, P.K.; Appel, L.J. Lower Sodium Intake and Risk of Headaches: Results From the Trial of Nonpharmacologic Interventions in the Elderly. Am. J. Public Health 2016, 106, 1270–1275. [Google Scholar] [CrossRef]
- Brown, R.B. Sodium Chloride, Migraine and Salt Withdrawal: Controversy and Insights. Med. Sci. 2021, 9, 67. [Google Scholar] [CrossRef]
- Robbins, L. Migraine Treatment: What’s Old, What’s New. Available online: https://www.practicalpainmanagement.com/pain/headache/migraine/migraine-treatment-what-old-what-new (accessed on 30 July 2021).
- Appel, L.J. Salt Intake, Salt Restriction and Primary (Essential) Hypertension. Available online: https://www.medilib.ir/uptodate/show/3877#rid17 (accessed on 30 April 2022).
- Lim, G.B. Low sodium and DASH diet to lower blood pressure. Nat. Rev. Cardiol. 2018, 15, 68. [Google Scholar] [CrossRef]
- Bae, Y.H.; Shin, J.S.; Lee, J.; Kim, M.R.; Park, K.B.; Cho, J.H.; Ha, I.H. Association between Hypertension and the Prevalence of Low Back Pain and Osteoarthritis in Koreans: A Cross-Sectional Study. PLoS ONE 2015, 10, e0138790. [Google Scholar] [CrossRef]
- Saccò, M.; Meschi, M.; Regolisti, G.; Detrenis, S.; Bianchi, L.; Bertorelli, M.; Pioli, S.; Magnano, A.; Spagnoli, F.; Giuri, P.G.; et al. The relationship between blood pressure and pain. J. Clin. Hypertens. 2013, 15, 600–605. [Google Scholar] [CrossRef]
- Townsend, R.R. NSAIDs and Acetaminophen: Effects on Blood Pressure and Hypertension. Available online: https://www.medilib.ir/uptodate/show/2385 (accessed on 30 April 2022).
- Fernandez, M.; Ordoñana, J.R.; Hartvigsen, J.; Ferreira, M.L.; Refshauge, K.M.; Sánchez-Romera, J.F.; Pinheiro, M.B.; Simpson, S.J.; Hopper, J.L.; Ferreira, P.H. Is Chronic Low Back Pain Associated with the Prevalence of Coronary Heart Disease when Genetic Susceptibility Is Considered? A Co-Twin Control Study of Spanish Twins. PLoS ONE 2016, 11, e0155194. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.J.; Yeh, T.L.; Shih, M.C.; Tu, Y.K.; Chien, K.L. Dietary Sodium Intake and Risk of Cardiovascular Disease: A Systematic Review and Dose-Response Meta-Analysis. Nutrients 2020, 12, 2934. [Google Scholar] [CrossRef]
- Li, Y.; Wu, X.; Mao, Y.; Liu, C.; Wu, Y.; Tang, J.; Zhao, K.; Li, P. Nitric Oxide Alleviated High Salt–Induced Cardiomyocyte Apoptosis and Autophagy Independent of Blood Pressure in Rats. Front. Cell Dev. Biol. 2021, 9, 646575. [Google Scholar] [CrossRef]
- Tabatabai, M.A.; Butros, V.M.; Mahdi, S.A.; Ahmad, M.J. Severe low back pain as the initial symptom of venous thrombosis of the inferior vena cava. BMJ Case Rep. 2014, 2014, bcr2014205259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kraft, C.; Hecking, C.; Schwonberg, J.; Schindewolf, M.; Lindhoff-Last, E.; Linnemann, B. Patients with inferior vena cava thrombosis frequently present with lower back pain and bilateral lower-extremity deep vein thrombosis. Vasa 2013, 42, 275–283. [Google Scholar] [CrossRef] [PubMed]
- Temraz, S.; Tamim, H.; Mailhac, A.; Taher, A. Could sodium imbalances predispose to postoperative venous thromboembolism? An analysis of the NSQIP database. Thromb. J. 2018, 16, 11. [Google Scholar] [CrossRef]
- Wild, J.; Knopp, T.; Molitor, M.; Hobohm, L.; Munzel, T.; Wenzel, P.; Karbach, S. High Salt Intake Increases Platelet Counts and Plasma Fibrinogen Levels but Has No Effect on Thrombus Formation or Resolution in a Murine Model of Venous Thrombosis [abstract]. Res. Pract. Thromb. Haemost. 2020, 4 (Suppl. 1). [Google Scholar]
- Dmitrieva, N.I.; Burg, M.B. Secretion of von Willebrand factor by endothelial cells links sodium to hypercoagulability and thrombosis. Proc. Natl. Acad. Sci. USA 2014, 111, 6485–6490. [Google Scholar] [CrossRef] [Green Version]
- Barkhuizen, A.; Rosen, H.R.; Wolf, S.; Flora, K.; Benner, K.; Bennett, R.M. Musculoskeletal pain and fatigue are associated with chronic hepatitis C: A report of 239 hepatology clinic patients. Am. J. Gastroenterol. 1999, 94, 1355–1360. [Google Scholar] [CrossRef]
- Arora, A.; Rajesh, S.; Bansal, K.; Sureka, B.; Patidar, Y.; Thapar, S.; Mukund, A. Cirrhosis-related musculoskeletal disease: Radiological review. Br. J. Radiol. 2016, 89, 20150450. [Google Scholar] [CrossRef] [Green Version]
- Wang, G.; Yeung, C.-k.; Wong, W.-Y.; Zhang, N.; Wei, Y.-f.; Zhang, J.-l.; Yan, Y.; Wong, C.-y.; Tang, J.-j.; Chuai, M. Liver fibrosis can be induced by high salt intake through excess reactive oxygen species (ROS) production. J. Agric. Food Chem. 2016, 64, 1610–1617. [Google Scholar] [CrossRef]
- Li, Y.; Lyu, Y.; Huang, J.; Huang, K.; Yu, J. Transcriptome sequencing reveals high-salt diet-induced abnormal liver metabolic pathways in mice. BMC Gastroenterol. 2021, 21, 335. [Google Scholar] [CrossRef]
- Beeckmans, N.; Vermeersch, A.; Lysens, R.; Van Wambeke, P.; Goossens, N.; Thys, T.; Brumagne, S.; Janssens, L. The presence of respiratory disorders in individuals with low back pain: A systematic review. Man. Ther. 2016, 26, 77–86. [Google Scholar] [CrossRef] [Green Version]
- Rasmussen-Barr, E.; Magnusson, C.; Nordin, M.; Skillgate, E. Are respiratory disorders risk factors for troublesome low-back pain? A study of a general population cohort in Sweden. Eur. Spine J. 2019, 28, 2502–2509. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, R.B. Sodium Toxicity in the Nutritional Epidemiology and Nutritional Immunology of COVID-19. Medicina 2021, 57, 739. [Google Scholar] [CrossRef] [PubMed]
- Symptoms of COVID-19. Available online: https://www.cdc.gov/coronavirus/2019-ncov/symptoms-testing/symptoms.html (accessed on 30 April 2022).
- Afsar, B.; Kuwabara, M.; Ortiz, A.; Yerlikaya, A.; Siriopol, D.; Covic, A.; Rodriguez-Iturbe, B.; Johnson, R.J.; Kanbay, M. Salt intake and immunity. Hypertension 2018, 72, 19–23. [Google Scholar] [CrossRef] [PubMed]
- Carlson, R.W.; Schaeffer Jr, R.C.; Michaels, S.G.; Weil, M. Pulmonary edema fluid. Spectrum of features in 37 patients. Circulation 1979, 60, 1161–1169. [Google Scholar] [CrossRef] [Green Version]
- Cui, X.; Chen, W.; Zhou, H.; Gong, Y.; Zhu, B.; Lv, X.; Guo, H.; Duan, J.; Zhou, J.; Marcon, E.; et al. Pulmonary Edema in COVID-19 Patients: Mechanisms and Treatment Potential. Front. Pharmacol. 2021, 12, 664349. [Google Scholar] [CrossRef] [PubMed]
- Abdullahi, A.; Candan, S.A.; Abba, M.A.; Bello, A.H.; Alshehri, M.A.; Afamefuna Victor, E.; Umar, N.A.; Kundakci, B. Neurological and Musculoskeletal Features of COVID-19: A Systematic Review and Meta-Analysis. Front. Neurol. 2020, 11, 687. [Google Scholar] [CrossRef]
- Murat, S.; Dogruoz Karatekin, B.; Icagasioglu, A.; Ulasoglu, C.; İçten, S.; Incealtin, O. Clinical presentations of pain in patients with COVID-19 infection. Ir. J. Med. Sci. 2021, 190, 913–917. [Google Scholar] [CrossRef]
- Borrelli, S.; Provenzano, M.; Gagliardi, I.; Michael, A.; Liberti, M.E.; De Nicola, L.; Conte, G.; Garofalo, C.; Andreucci, M. Sodium Intake and Chronic Kidney Disease. Int. J. Mol. Sci. 2020, 21, 4744. [Google Scholar] [CrossRef] [PubMed]
- Kesikburun, B.; Ekşioğlu, E.; Akdağ, İ.; Çakçı, A. Low back pain in hemodialysis patients: Risk factors and its impact on health-related quality of life. Turk. J. Phys. Med. Rehabil. 2018, 64, 66–71. [Google Scholar] [CrossRef] [PubMed]
- Daneau, C.; Abboud, J.; Marchand, A.-A.; Houle, M.; Pasquier, M.; Ruchat, S.-M.; Descarreaux, M. Mechanisms Underlying Lumbopelvic Pain During Pregnancy: A Proposed Model. Front. Pain Res. 2021, 2, 773988. [Google Scholar] [CrossRef] [PubMed]
- Arvizu, M.; Bjerregaard, A.A.; Madsen, M.T.B.; Granström, C.; Halldorsson, T.I.; Olsen, S.F.; Gaskins, A.J.; Rich-Edwards, J.W.; Rosner, B.A.; Chavarro, J.E. Sodium Intake during Pregnancy, but Not Other Diet Recommendations Aimed at Preventing Cardiovascular Disease, Is Positively Related to Risk of Hypertensive Disorders of Pregnancy. J. Nutr. 2020, 150, 159–166. [Google Scholar] [CrossRef] [PubMed]
- Massot, C.; Donze, C.; Guyot, M.A.; Leteneur, S. Low back pain in patients with multiple sclerosis: A systematic review and the prevalence in a French multiple sclerosis population. Rev. Neurol. 2021, 177, 349–358. [Google Scholar] [CrossRef] [PubMed]
- Farez, M.F.; Fiol, M.P.; Gaitán, M.I.; Quintana, F.J.; Correale, J. Sodium intake is associated with increased disease activity in multiple sclerosis. J. Neurol. Neurosurg. Psychiatry 2015, 86, 26–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zostawa, J.; Adamczyk, J.; Sowa, P.; Adamczyk-Sowa, M. The influence of sodium on pathophysiology of multiple sclerosis. Neurol. Sci. 2017, 38, 389–398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shaharabani, R.; Ram-On, M.; Talmon, Y.; Beck, R. Pathological transitions in myelin membranes driven by environmental and multiple sclerosis conditions. Proc. Natl. Acad. Sci. USA 2018, 115, 11156–11161. [Google Scholar] [CrossRef] [Green Version]
Figure 1.
Posterior lumbar subcutaneous edema. Adapted with permission from Schwarz-Nemec et al., 2020 [12].
Figure 1.
Posterior lumbar subcutaneous edema. Adapted with permission from Schwarz-Nemec et al., 2020 [12].

Figure 2.
Posterior lumbar subcutaneous edema potentially mediates the association of increased sodium chloride intake with non-specific low back pain.
Figure 2.
Posterior lumbar subcutaneous edema potentially mediates the association of increased sodium chloride intake with non-specific low back pain.

Figure 3.
Non-specific low back pain (A) is transitively linked to comorbid conditions (C) through the common mediating factor of increased sodium chloride intake (B). Future studies should investigate prevalence of posterior lumbar subcutaneous edema in conditions comorbid with non-specific low back pain.
Figure 3.
Non-specific low back pain (A) is transitively linked to comorbid conditions (C) through the common mediating factor of increased sodium chloride intake (B). Future studies should investigate prevalence of posterior lumbar subcutaneous edema in conditions comorbid with non-specific low back pain.

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Brown, R.B. Non-Specific Low Back Pain, Dietary Salt Intake, and Posterior Lumbar Subcutaneous Edema. Int. J. Environ. Res. Public Health 2022, 19, 9158. https://doi.org/10.3390/ijerph19159158
AMA Style
Brown RB. Non-Specific Low Back Pain, Dietary Salt Intake, and Posterior Lumbar Subcutaneous Edema. International Journal of Environmental Research and Public Health. 2022; 19(15):9158. https://doi.org/10.3390/ijerph19159158
Chicago/Turabian StyleBrown, Ronald B. 2022. "Non-Specific Low Back Pain, Dietary Salt Intake, and Posterior Lumbar Subcutaneous Edema" International Journal of Environmental Research and Public Health 19, no. 15: 9158. https://doi.org/10.3390/ijerph19159158
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.