
Gender and Context Matter: Behavioral and Structural Interventions for People Who Use Alcohol and Other Drugs in Africa

 , , ,
, , ,
Abstract
:1. Introduction
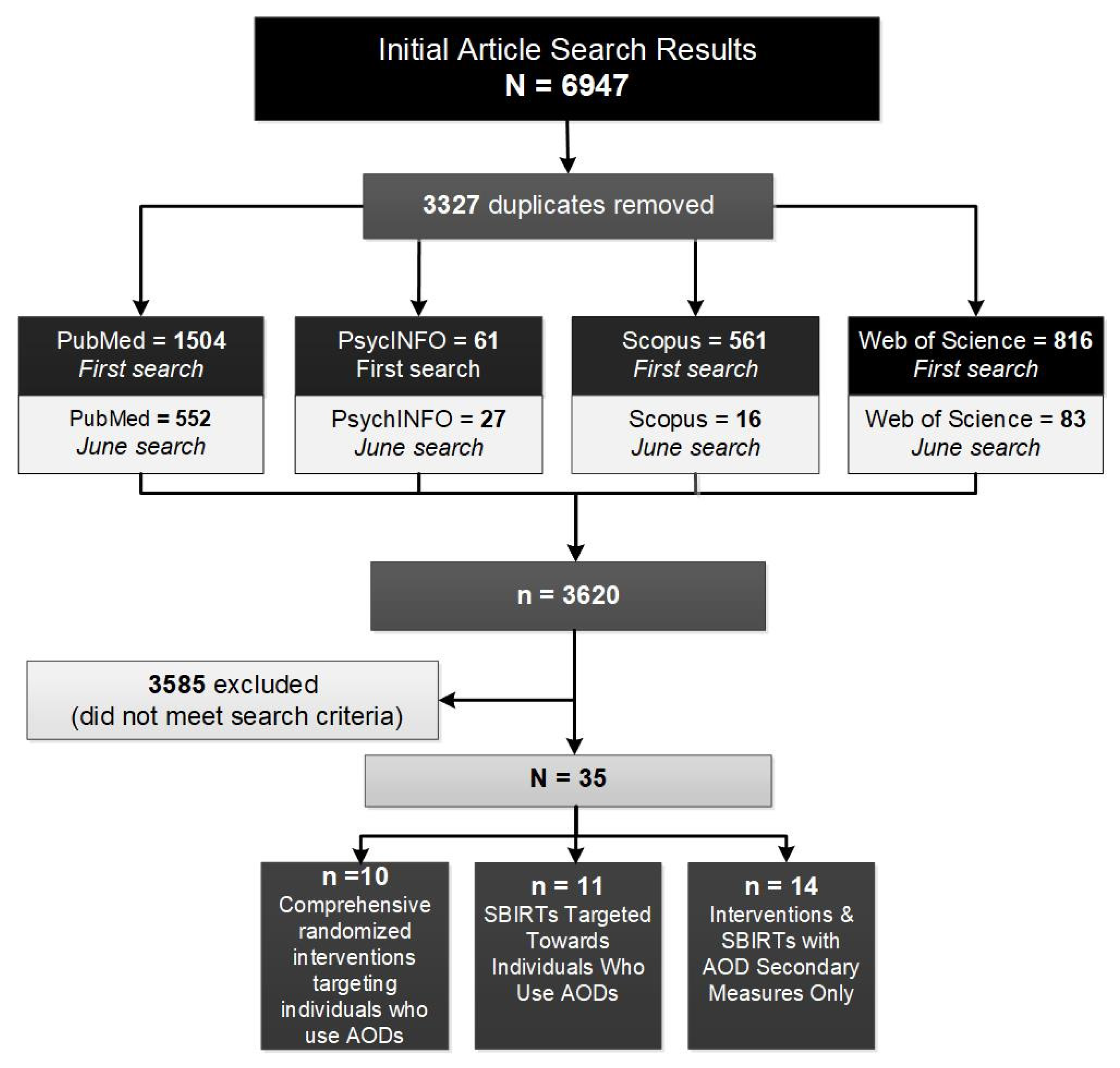
2. Methods
- −
- Comprehensive interventions targeting individuals who use AODs, including randomized trials with at least two arms (including a control arm), a sample size of at least 100 participants, and study eligibility criterion of AOD use. These interventions address AODs and other issues—such as HIV or GBV—to distinguish them from brief intervention studies that focus on AOD only.
- −
- Single-session or screening brief intervention and referral to treatment (SBIRTs) targeting individuals who use AODs, including studies with single or brief intervention (up to four) sessions, with a study eligibility criterion of AOD use.
- −
- SBIRTs with AOD use as secondary measures; that is, AOD use was not an eligibility requirement for participants.
3. Results
3.1. Comprehensive Interventions Targeting Individuals Who Use Alcohol and Other Drugs
3.1.1. Delivery Setting
3.1.2. Gender
3.1.3. Context and Culture
3.1.4. Other Intersectional Issues
3.2. Single-Session or Screening Brief Intervention and Referral to Treatment Targeting Individuals Who Use Alcohol and Other Drugs
3.2.1. Delivery Setting
3.2.2. Gender
3.2.3. Other Intersectional Issues

{kind=link}
| Citation | Region/Sample | Setting/Topics | Intervention | Outcomes |
|---|---|---|---|---|
| Behavioral | ||||
| Harder et al. (2020) [80] | Kenya: 300 adults with alcohol use problems | Health center staff administered the in-person intervention (one session, 30 min) or spoke with health center staff by telephone for those in the mHealth condition EtOH | Arm 1: mHealth MI delivered via telephone Arm 2: MI delivered in person | No differences between mHealth or in-person MI, but participants in the waiting list control group had higher AUDIT-C scores than participants in intervention arms |
| Huis in’t Veld et al. (2019) [81] | South Africa: 560 adults living with HIV | Four nurses not associated with the clinics delivered the interventions to patients and completed the follow-ups at clinic sites EtOH, HIV | WHO brief intervention package for harmful drinking: advice on AUDIT scores, health education leaflet, and brief counseling | * AUDIT scores decreased in both groups compared with baseline, but no significant impact over time No between-group differences |
| Marais et al. (2011) [86] | South Africa: 194 women who were less than 20 weeks pregnant and more than 15 years of age (rationale for sampling was to destigmatize FASD) | Brief interventions varying in length and objective delivered individually by trained staff EtOH | A series of four brief interventions and a comprehensive assessment addressing alcohol use among pregnant women | * Decrease in AUDIT between arms |
| Mertens et al. (2014) [85] | South Africa: 403 young people aged 18 to 24 who use AOD seeking primary care at a clinic | Individual session in a large public-sector primary health clinic in Delft, Cape Town, delivered by a trained nurse to address alcohol and substance use among young people EtOH, THC, METH, Methaqualone, Sedatives | A brief motivational intervention and a referral resource list for drinking and drug use | * Reductions in ASSIST alcohol involvement scores larger for the intervention condition |
| Peltzer et al. (2013) [88] | South Africa: 1196 participants from selected clinics with active tuberculosis who scored less than 7 or 8 on the AUDIT (women/men) | Lay counselor delivered individual two-session intervention TB, EtOH | Brief counseling sessions on alcohol risk reduction | Reductions in AUDIT score, hazardous or harmful drinking, alcohol dependence, heavy episodic drinking, and hazardous drinking in treatment groups |
| Pengpid et al. (2013) [89] | South Africa: 392 outpatients who were screened for alcohol problems | Intervention delivered by the intervention assistant nurse counselor in groups at a hospital in Tshwane EtOH | Brief intervention on substance use strategies for reduction, including sensible limits, diaries, problem solving, and goal setting | No significant intervention effects on alcohol use, including AUDIT score |
| Pengpid et al. (2013) [84] | South Africa: 152 university students who scored as risk drinkers through the AUDIT | One 20-min intervention session delivered by counselors EtOH, THC, MH | Brief intervention addressing AUDIT score results and providing education and strategies for reducing risky drinking | No significant between-group changes in AUDIT score, but reductions in all treatment groups over time |
| Rendall-Mkosi et al. (2013) [82] | South Africa: 196 women engaging in risky drinking with ineffective or no contraceptive use | Five-session MI delivered individually by locally recruited and trained lay counselors at study sites EtOH, THC, SRH | MI focused on supporting behavior change based on the Project CHOICES study along with an information pamphlet about FASD and a women’s health handbook | * 50% reduction in the proportion of women at risk for an alcohol-exposed pregnancy in the MI group * Greater reduction in the proportion of women not using birth control in the MI group Reduction in women who met the criteria for risky drinking in both groups |
| Sorsdahl et al. (2015) [79] | South Africa: 335 patients at emergency departments in health clinics at moderate to high risk for substance use problems based on the ASSIST | MI arm: 20-min intervention delivered individually by a counselor at a community health center MI + PST arm: Five 45- to 60-min sessions delivered individually by a counselor at a community health center EtOH, THC, COC, METH, Methaqualone, MH | MI: adapted from the ASSIST-Linked Brief Intervention MI + PST: multiple interventions building goals for substance use reduction and learning techniques of PST | * ASSIST scores lower in MI + PST group than MI and control No significant difference between the MI and control groups * Lower CES-D score in MI + PST group compared with the MI and control groups No differences in AOD-related injury, violence, or police interaction between groups |
| Wandera et al. (2017) [83] | Uganda: 337 adults living with HIV that use alcohol (scored less than or equal to 3 on AUDIT-C) | Standardized positive prevention counseling and MI counseling delivered by trained counselors alone at the study site EtOH, HIV | Standardized positive prevention counseling plus MI counseling | * Reduction in mean AUDIT-C score at 6-month follow-up in both arms * Women had a greater AUDIT-C reduction in the MI group than in the control group No between-group differences |
| Ward et al. (2015) [87] | South Africa: 403 young adults aged 18 to 24 who use AODs | Trained nurse practitioners delivered the intervention individually EtOH, THC, Methaqualone, COC, METH, Sedatives | Brief motivational intervention and a referral resource list | No significant between-group differences * Observed that those who reduced alcohol consumption also reported reduced aggressive behaviors |
3.3. Interventions and SBIRTs with AOD Use as Secondary Measures
3.3.1. Delivery Settings
3.3.2. Gender and Culture
3.3.3. Other Intersectional Issues
| Citation | Region/Sample | Setting/Topics | Intervention | Outcomes |
|---|---|---|---|---|
| Behavioral | ||||
| Burnhams et al. (2015) [101] | South Africa: 325 safety and security division employees of a municipality | Six training modules presented to employees in groups over an 8-h session delivered in the workplace by interventionists EtOH | TA: evidence-based workplace training program that addresses behavioral risks and stigma and promotes help-seeking and proactive behaviors | * TA had the greatest impact on days having 5 or more drinks at one sitting in the past 30 days * TA showed modest reductions in binge drinking from baseline to 3-month follow-up and going to work or calling in sick because of a hangover |
| Eze et al. (2020) [99] | Nigeria: 376 adults who were registered members of the market traders’ association | Public health physician, dietician, and physical fitness counselor facilitated group intervention over two sessions of 5-h each EtOH, Nutrition | A lifestyle and behavioral modification intervention to control hypertension by promoting increased physical activity and dietary adjustments | * At post-test, intervention participants reduced excessive alcohol consumption and increased physical activity and fruit and vegetable servings, resulting in overall lower risk for hypertension |
| Jemmott et al. (2014) [94] | South Africa: 1181 men from 22 geographical neighborhood clusters | Six 75-min group intervention modules facilitated by men from the community at the University of Fort Hare in East London HIV, EtOH | HIV risk-reduction intervention to improve condom use and increase HIV/STI knowledge | * Intervention effects were increases in consistent condom use, talking to partners about condom use, and frequency of condom use |
| Manyaapelo et al. (2019) [96] | South Africa: 575 young men aged 18 to 35 | Four 3-h group sessions delivered by peer educators over 4 weeks AOD, SRH | Ubudoda Abukhulelwa Responsible Manhood: program developed for soon-to-be-released justice-involved men addressing masculinity, sexual relationships, communication, and AOD use | * Increases in intentions to reduce AOD use and changes in attitudes toward avoiding sex when one is intoxicated among men in the intervention |
| Massarwi et al. (2021) [98] | South Africa: 525 parents and caregivers of adolescents | Fourteen-session parenting program lasting 1 to 1.5-h per week AOD, MH | Parenting for Lifelong Health/Sinovuyo Teen: program to promote family cohesion and nonviolent discipline, improve parent-child relationships, and improve communication in low-resource settings | * Parental substance use reduction was associated with a reduction in parental depression at 5- and 9-month follow-ups |
| Moscoe et al. (2019) [97] | Kenya: 300 men aged 21 or older engaged in fishing or transportation work | Provided financial incentives based on the amount of savings in a registered bank account EtOH, Gambling | Participants received weekly financial rewards if they saved money by not spending on alcohol or gambling | The intervention group had higher growth in bank saving balance but no differences in spending on alcohol or gambling between groups |
| Rotheram-Borus et al.(2015) [90] | South Africa: 1238 pregnant women residing in urban, low-income neighborhoods in Cape Town, South Africa | Home visits by community health workers EtOH, IPV, MH | Home visits promoting educational knowledge and behavior change on HIV/TB, alcohol, mental health, breastfeeding, and malnutrition | * Mothers in the intervention arm were less likely to report depressive symptoms and more likely to report positive quality of life at 36-month follow-up * Drinking increased over the 5 years post-birth, but participants in the intervention arm had smaller increases |
| Tibbits et al. (2011) [95] | South Africa: 4040 youth attending nine schools in Mitchell’s Plain, Cape Town | Teacher-delivered intervention over two to three class periods in groups EtOH, THC, SRH | HW is a school-based intervention promoting social-emotional skills, substance use and sexual behavior knowledge and refusal skills, and healthy free-time activities | * Greater reduction in rate of polydrug use in women and frequent polydrug use among participants in HW Reduction in lifetime sexual activity and refusal to have condomless sex in the HW arm |
| Combination Behavioral and Structural | ||||
| Bachanas et al. (2016) [100] | Namibia, Kenya, and Tanzania: 3522 patients living with HIV attending clinical care | Clinic-based package of HIV prevention interventions delivered in 9 of 18 clinics by health care providers in groups EtOH, SRH | HIV prevention intervention provided by trained clinicians and lay counselors | * Sexual barrier use outcomes achieved by the community health care staff were comparable to or better than those achieved by the Partner Project research staff, and both were superior to the control group * A reduction in IPV was observed for the entire sample, although no change in alcohol use was observed |
| Cubbins et al. (2012) [102] | Zimbabwe: 185 individuals aged 18 to 30 living within 30 selected sample sites | CPOLs shared intervention messages in social and community settings EtOH, HIV | 60 CPOLs trained to deliver HIV risk- reduction messages, with not drinking alcohol being a secondary message | Community-level analyses found no differences between groups * Declines in alcohol use, frequency of use, and quantity of drinks were found in intervention and control sites at relatively equal levels |
| SBIRTs, Motivational Interviewing | ||||
| Louwagie et al.(2022) [93] | South Africa: 574 adults beginning treatment for drug-sensitive pulmonary TB | Lay health workers delivering three MI sessions along with SMS messages to bolster intervention content EtOH, TB | ProLife Intervention: Participants created plans to address alcohol and tobacco use and TB adherence followed by 10 SMS messages supporting TB treatment adherence | Reductions in AUDIT scores at follow-up but no significant intervention effect |
| Peltzer et al. (2010) [91] | South Africa: 488 adults living with HIV receiving services at HCT clinics | Three sessions (20 to 30 min each) delivered by lay counselors individually EtOH, HIV | Motivational skills-building risk reduction counseling intervention assisting individuals living with HIV to reduce sexual risk behaviors and alcohol consumption | * Reductions in drinking and various sexual risk behavior following intervention |
| Pitpitan et al. (2015) [92] | South Africa: 617 participants from an STI clinic in Cape Town, South Africa | Group counseling and intervention providing education EtOH, SRH | Brief risk-reduction intervention about HIV transmission and risk behaviors, including alcohol use as a risk factor | * IMB model-based intervention reduced alcohol risk behaviors and expectancies |
| Wagman et al. (2015) [103] | Uganda: 11,448 individuals aged 15 to 49 from preexisting clusters who agreed to provide blood samples for HIV testing | Surveys conducted by same-sex interviewers in private; intervention conducted in groups by RHSP counselors at project site EtOH, IPV, HIV | S.H.A.R.E. violence reduction intervention: consisted of screening and a brief intervention to reduce IPV related to HIV disclosure and address risk behaviors | * Proportion of women experiencing IPV lower among intervention participants * Women’s rates of HIV disclosure were higher in the intervention group * Lower HIV incidence among men in the intervention group |
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AOD | alcohol and other drugs |
| ART | antiretroviral therapy |
| AUD | Alcohol Use Disorder |
| AUDIT | Alcohol Use Disorders Identification Test |
| CBT | cognitive behavioral therapy |
| CES-D | Center for Epidemiologic Studies Depression Scale |
| CETA | Common Elements Treatment Approach |
| CHC | Couples Health CoOp |
| FASD | Fetal Alcohol Spectrum Disorder |
| GBV | gender-based violence |
| IMB | Information–Motivation–Behavioral Skills Model |
| IPV | intimate partner violence |
| MH | mental health |
| MI | Motivational Interviewing |
| MI + PST | Motivational Interviewing and Problem Solving Therapy |
| PLWH | people living with HIV |
| PrEP | pre-exposure prophylaxis |
| RCT | randomized control trial |
| REHT | Rational emotive health therapy treatment |
| SBIRTs | screening brief intervention and referral to treatments |
| SRH | sexual and reproductive health |
| STI | sexually transmitted infection |
| TB | tuberculosis |
| WHC | Women’s Health CoOp |
| WHC+ | Women’s Health CoOp Plus |
| WHO | World Health Organization |
Appendix A. Search Terms
- Search 1
- (((behavioral) OR (structural)) AND ((intervention) OR (program) OR (project)) AND (Africa) AND ((“substance use disorder”) OR (“substance use”) OR (alcohol) OR (alcoholism) OR (“drug use”) OR (“drug abuse”)) NOT ((“cross-sectional”) OR (review) OR (systematic))) Filters: from January 2010–October 2021
- Search 2
- (((behavioral) OR (structural)) AND ((intervention) OR (program) OR (project) OR (treatment)) AND (Africa) AND ((“substance use disorder”) OR (“substance use”) OR (alcohol) OR (alcoholism) OR (“drug use”) OR (“drug abuse”) OR (methadone) OR (buprenorphine)) NOT ((“cross-sectional”) OR (review) OR (systematic))) Filters: from November 2021–May 2022
References
- Sudhinaraset, M.; Wigglesworth, C.; Takeuchi, D.T. Social and cultural contexts of alcohol use. Alcohol Res. Curr. Rev. 2015, 38, E1–E11. [Google Scholar]
- National Institute on Drug Abuse. Alcohol. 2020. Available online: https://www.drugabuse.gov/drug-topics/alcohol#Ref (accessed on 5 September 2021).
- United Nations Office on Drugs and Crime. Press Release: UNODC World Drug Report 2020: Global Drug Use Rising; While COVID-19 Has Far Reaching Impact on Global Drug Markets. 2020. Available online: https://www.unodc.org/unodc/press/releases/2020/June/media-advisory---global-launch-of-the-2020-world-drug-report.html (accessed on 24 September 2021).
- Johnson, B. Illicit Drug Markets in South Africa: A Review. 2007. Available online: https://www.drugabuse.gov/international/abstracts/illicit-drug-markets-in-south-africa-review (accessed on 7 September 2021).
- Ferreira-Borges, C.; Parry, C.D.H.; Babor, T.F. Harmful use of alcohol: A shadow over Sub-Saharan Africa in need of workable solutions. Int. J. Environ. Res. Public Health 2017, 14, 346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eligh, J. A Synthetic Age: The Evolution of Methamphetamine Markets in Eastern and Southern Africa. 2021. Available online: https://globalinitiative.net/wp-content/uploads/2021/03/GITOC-A-Synthetic-Age-The-Evolution-of-Methamphetamine-Markets-in-Eastern-and-Southern-Africa.pdf (accessed on 15 September 2021).
- Statista. Percentage of Illicit Drug Use in Global Population by Drug Type 2019. 2019. Available online: https://www.statista.com/statistics/443460/percentage-of-population-that-has-used-illicit-drugs-by-drug/ (accessed on 28 September 2021).
- Donnenfeld, Z.; Bellow-Schünemann, J.; Welborn, L. Drug Demand and Use in Africa: Modelling Trends to 2050. 2019. Available online: https://enact-africa.s3.amazonaws.com/site/uploads/2019-08-28-drug-demand-and-use-in-africa-reaseach-paper-cb.pdf (accessed on 5 September 2021).
- South African Community Epidemiology Network on Drug Use. January–June 2020 Phase 48: Monitoring Alcohol, Tobacco, and Other Drug Abuse Treatment Admissions in South Africa. Available online: https://www.samrc.ac.za/sites/default/files/attachments/2021-07-29/SACENDU%20Full%20Report_Phase%2048_July%202020.pdf (accessed on 5 September 2021).
- Wechsberg, W.M.; Jones, H.E.; Zule, W.A.; Myers, B.J.; Browne, F.A.; Kaufman, M.R.; Luseno, W.; Flisher, A.J.; Parry, C.D. Methamphetamine (“tik”) use and its association with condom use among out-of-school females in Cape Town, South Africa. Am. J. Drug Alcohol Abuse 2010, 36, 208–213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- UNAIDS. UNAIDS Fact Sheet 2021: Global HIV Statistics. 2021. Available online: https://www.unaids.org/en/resources/fact-sheet (accessed on 12 September 2021).
- UNAIDS. AIDSinfo: Global Data on HIV Epidemiology and Response. 2020. Available online: http://aidsinfo.unaids.org/ (accessed on 12 September 2021).
- United Nations Office on Drugs and Crime. World Drug Report: Women and Drugs. 2018. Available online: https://www.unodc.org/wdr2018/prelaunch/WDR18_Booklet_5_WOMEN.pdf (accessed on 8 September 2021).
- United Nations Office on Drugs and Crime. World Drug Report. 2021. Available online: https://www.unodc.org/unodc/data-and-analysis/wdr2021.html (accessed on 28 September 2021).
- World Health Organization. Fact Sheet: Alcohol. 2018. Available online: https://www.who.int/news-room/fact-sheets/detail/alcohol (accessed on 5 September 2021).
- Tapert, S.F.; Caldwell, L.; Burke, C. Alcohol and the adolescent brain: Human studies. Alcohol Res Health 2004, 28, 205. [Google Scholar]
- Salmanzadeh, H.; Ahmadi-Soleimani, S.M.; Pachenari, N.; Azadi, M.; Halliwell, R.F.; Rubino, T.; Azizi, H. Adolescent drug exposure: A review of evidence for the development of persistent changes in brain function. Brain Res. Bull 2020, 156, 105–117. [Google Scholar] [CrossRef] [PubMed]
- Raiford, J.L.; Herbst, J.H.; Carry, M.; Browne, F.A.; Doherty, I.; Wechsberg, W.M. Low prospects and high risk: Structural determinants of health associated with sexual risk among young African American women residing in resource-poor communities in the south. Am. J. Community Psychol 2014, 54, 243–250. [Google Scholar] [CrossRef]
- Myers, B.; Carney, T.; Johnson, K.; Browne, F.A.; Wechsberg, W.M. Service providers’ perceptions of barriers to the implementation of trauma-focused substance use services for women in Cape Town, South Africa. Int. J. Drug Policy 2020, 75, 102628. [Google Scholar] [CrossRef]
- Meyer, J.P.; Springer, S.A.; Altice, F.L. Substance abuse, violence, and HIV in women: A literature review of the syndemic. J. Womens Health 2011, 20, 991–1006. [Google Scholar] [CrossRef] [Green Version]
- Bonner, C.P.; Browne, F.A.; Ndirangu, J.W.; Howard, B.; Zule, W.A.; Speizer, I.S.; Kline, T.; Wechsberg, W.M. Exploring the associations between physical and sexual gender-based violence and HIV among women who use substances in South Africa: The role of agency and alcohol. AIDS Care 2019, 31, 1369–1375. [Google Scholar] [CrossRef]
- Adebiyi, B.O.; Mukumbang, F.C.; Beytell, A.-M. To what extent is Fetal Alcohol Spectrum Disorder considered in policy-related documents in South Africa? A document review. Health Res. Policy Syst 2019, 17, 46. [Google Scholar] [CrossRef]
- Ritchie, H.R.M. Our World in Data: Alcohol Consumption. 2019. Available online: https://ourworldindata.org/alcohol-consumption (accessed on 24 September 2021).
- Kaiser Family Foundation. The Global HIV/AIDS Epidemic Fact Sheet. 2021. Available online: https://www.kff.org/global-health-policy/fact-sheet/the-global-hivaids-epidemic/ (accessed on 22 September 2021).
- El-Bassel, N.; Gilbert, L.; Witte, S.; Wu, E.; Gaeta, T.; Schilling, R.; Wada, T. Intimate partner violence and substance abuse among minority women receiving care from an inner-city emergency department. Womens Health 2003, 13, 16–22. [Google Scholar] [CrossRef]
- El-Bassel, N.; Gilbert, L.; Witte, S.; Wu, E.; Chang, M. Intimate partner violence and HIV among drug-involved women: Contexts linking these two epidemics--challenges and implications for prevention and treatment. Subst. Use Misuse 2011, 46, 295–306. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Facts on Alcohol and Violence: Intimate Partner Violence and Alcohol. 2006. Available online: https://www.who.int/violence_injury_prevention/violence/world_report/factsheets/fs_intimate.pdf (accessed on 22 September 2021).
- Wechsberg, W.M.; Browne, F.A.; Ndirangu, J.; Bonner, C.P.; Kline, T.L.; Gichane, M.; Zule, W.A. Outcomes of implementing in the real world the Women’s Health CoOp intervention in Cape Town, South Africa. AIDS Behav. 2021, 25, 276–289. [Google Scholar] [CrossRef] [PubMed]
- El-Krab, R.; Kalichman, S.C. Alcohol-antiretroviral therapy interactive toxicity beliefs and intentional medication nonadherence: Review of research with implications for interventions. AIDS Behav. 2021, 25, 251–264. [Google Scholar] [CrossRef] [PubMed]
- Rose, A.L.; Belus, J.M.; Ma, T.; Lee, J.S.; Wan, C.; De Los Reyes, A.; Joska, J.A.; Andersen, L.S.; Myers, B.; Magidson, J.F. The relationship between harmful alcohol use and antiretroviral non-adherence in people accessing HIV treatment in Cape Town, South Africa: An event-level analysis. AIDS Behav. 2022, 26, 2055–2066. [Google Scholar] [CrossRef] [PubMed]
- UNAIDS. Global AIDS Update 2019—Communities at the Centre: Defending Rights Breaking Barriers, Reaching People with HIV Services. 2019. Available online: https://www.unaids.org/sites/default/files/media_asset/2019-global-AIDS-update_en.pdf (accessed on 22 September 2021).
- Sileo, K.M.; Miller, A.P.; Huynh, T.A.; Kiene, S.M. A systematic review of interventions for reducing heavy episodic drinking in sub-Saharan African settings. PLoS ONE 2020, 15, e0242678. [Google Scholar] [CrossRef] [PubMed]
- Biggane, A.M.; Briegal, E.; Obasi, A. Interventions for adolescent alcohol consumption in Africa: Protocol for a scoping review including an overview of reviews. Syst. Rev 2021, 10, 1–7. [Google Scholar] [CrossRef]
- Wechsberg, W.M.; Browne, F.A.; Bonner, C.P.; Washio, Y.; Howard, B.N.; van der Drift, I. Current interventions for people living with HIV who use alcohol: Why gender matters. Curr. HIV/AIDS Rep. 2021, 18, 351–364. [Google Scholar] [CrossRef]
- Kalichman, S.C.; Simbayi, L.C.; Kaufman, M.; Cain, D.; Jooste, S. Alcohol use and sexual risks for HIV/AIDS in sub-Saharan Africa: Systematic review of empirical findings. Prev. Sci. 2007, 8, 141–151. [Google Scholar] [CrossRef]
- Tomokawa, S.; Miyake, K.; Akiyama, T.; Makino, Y.; Nishio, A.; Kobayashi, J.; Jimba, M.; Ayi, I.; Njenga, S.M.; Asakura, T. Effective school-based preventive interventions for alcohol use in Africa: A systematic review. Afr. Health Sci. 2020, 20, 1397–1406. [Google Scholar] [CrossRef]
- Wechsberg, W.M.; Browne, F.A.; Ndirangu, J.; Bonner, C.P.; Minnis, A.M.; Nyblade, L.; Speizer, I.S.; Howard, B.N.; Myers, B.; Ahmed, K. The PrEPARE Pretoria Project: Protocol for a cluster-randomized factorial-design trial to prevent HIV with PrEP among adolescent girls and young women in Tshwane, South Africa. BMC Public Health 2020, 20, 1403. [Google Scholar] [CrossRef]
- Staton, C.A.; Zadey, S.; O’Leary, P.; Phillips, A.; Minja, L.; Swahn, M.H.; Hirshon, J.M.; Boshe, J.; Sakita, F.; Vissoci, J.R.N.; et al. PRACT: A pragmatic randomized adaptive clinical trial protocol to investigate a culturally adapted brief negotiational intervention for alcohol use in the emergency department in Tanzania. Trials 2022, 23, 120. [Google Scholar] [CrossRef] [PubMed]
- Huis In ‘t Veld, D.; Skaal, L.; Peltzer, K.; Colebunders, R.; Ndimande, J.V.; Pengpid, S. The efficacy of a brief intervention to reduce alcohol misuse in patients with HIV in South Africa: Study protocol for a randomized controlled trial. Trials 2012, 13, 190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kane, J.C.; Skavenski Van Wyk, S.; Murray, S.M.; Bolton, P.; Melendez, F.; Danielson, C.K.; Chimponda, P.; Munthali, S.; Murray, L.K. Testing the effectiveness of a transdiagnostic treatment approach in reducing violence and alcohol abuse among families in Zambia: Study protocol of the Violence and Alcohol Treatment (VATU) trial. Glob. Ment. Health 2017, 4, e18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuo, C.C.; Sibeko, G.; Akande, M.; Allie, S.; Tisaker, N.; Stein, D.J.; Becker, S.J. Advancing a cascading train-the-trainer model of frontline HIV service providers in South Africa: Protocol of an implementation trial. Addict. Sci. Clin. Pract. 2021, 16, 27. [Google Scholar] [CrossRef] [PubMed]
- Leddy, A.M.; Hahn, J.A.; Getahun, M.; Emenyonu, N.I.; Woolf-King, S.E.; Sanyu, N.; Katusiime, A.; Fatch, R.; Chander, G.; Hutton, H.E.; et al. Cultural adaptation of an intervention to reduce hazardous alcohol use among people living with HIV in Southwestern Uganda. AIDS Behav. 2021, 25, 237–250. [Google Scholar] [CrossRef]
- Madhombiro, M.; Dube-Marimbe, B.; Dube, M.; Chibanda, D.; Zunza, M.; Rusakaniko, S.; Stewart, D.; Seedat, S. A cluster randomised controlled trial protocol of an adapted intervention for alcohol use disorders in people living with HIV and AIDS: Impact on alcohol use, general functional ability, quality of life and adherence to HAART. BMC Psychiatry 2017, 17, 44. [Google Scholar] [CrossRef] [Green Version]
- Musyoka, C.M.; Mbwayo, A.; Donovan, D.M.; Mathai, M. mHealth-based peer mentoring for prevention of alcohol and substance abuse among first year university students: Protocol for quasi-experimental intervention. J. Subst. Use 2021, 26, 53–59. [Google Scholar] [CrossRef]
- Parry, C.D.; Morojele, N.K.; Myers, B.J.; Kekwaletswe, C.T.; Manda, S.O.; Sorsdahl, K.; Ramjee, G.; Hahn, J.A.; Rehm, J.; Shuper, P.A. Efficacy of an alcohol-focused intervention for improving adherence to antiretroviral therapy (ART) and HIV treatment outcomes—A randomised controlled trial protocol. BMC Infect. Dis. 2014, 14, 500. [Google Scholar] [CrossRef] [Green Version]
- Rotheram-Borus, M.J.; Tomlinson, M.; Mayekiso, A.; Bantjes, J.; Harris, D.M.; Stewart, J.; Weiss, R.E. Gender-specific HIV and substance abuse prevention strategies for South African men: Study protocol for a randomized controlled trial. Trials 2018, 19, 1–13. [Google Scholar] [CrossRef]
- Tzilos Wernette, G.; Plegue, M.; Mmeje, O.; Sen, A.; Countryman, K.; Ngo, Q.; Prosser, L.; Zlotnick, C. Reducing sexual health risks and substance use in the prenatal setting: A study protocol for a randomized controlled trial. Contemp. Clin. Trials 2019, 84, 105827. [Google Scholar] [CrossRef] [PubMed]
- Jewkes, R.; Gibbs, A.; Jama-Shai, N.; Willan, S.; Misselhorn, A.; Mushinga, M.; Washington, L.; Mbatha, N.; Skiweyiya, Y. Stepping Stones and Creating Futures intervention: Shortened interrupted time series evaluation of a behavioural and structural health promotion and violence prevention intervention for young people in informal settlements in Durban, South Africa. BMC Public Health 2014, 14, 1325. [Google Scholar] [CrossRef] [PubMed]
- Sorsdahl, K.; Myers, B.; Ward, C.; Matzopoulos, R.; Mtukushe, B.; Nicol, A.; Stein, D.J. Screening and brief interventions for substance use in emergency departments in the Western Cape province of South Africa: Views of health care professionals. Int. J. Inj. Control Saf. Promot. 2014, 21, 236–243. [Google Scholar] [CrossRef]
- Beres, L.K.; Mbabali, I.; Anok, A.; Katabalwa, C.; Mulamba, J.; Thomas, A.G.; Bugos, E.; Nakigozi, G.; Grabowski, M.K.; Chang, L.W. Mobile ecological momentary assessment and intervention and health behavior change among adults in Rakai, Uganda: Pilot randomized controlled trial. JMIR Form Res. 2021, 5, e22693. [Google Scholar] [CrossRef]
- Bhana, A.; Mellins, C.A.; Petersen, I.; Alicea, S.; Myeza, N.; Holst, H.; Abrams, E.; John, S.; Chhagan, M.; Nestadt, D.F.; et al. The VUKA family program: Piloting a family-based psychosocial intervention to promote health and mental health among HIV infected early adolescents in South Africa. AIDS Care 2014, 26, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Calligaro, G.L.; de Wit, Z.; Cirota, J.; Orrell, C.; Myers, B.; Decker, S.; Stein, D.J.; Sorsdahl, K.; Dawson, R. Brief psychotherapy administered by non-specialised health workers to address risky substance use in patients with multidrug-resistant tuberculosis: A feasibility and acceptability study. Pilot Feasibility Stud. 2021, 7, 28. [Google Scholar] [CrossRef] [PubMed]
- Carney, T.; Browne, F.A.; Myers, B.; Kline, T.L.; Howard, B.; Wechsberg, W.M. Adolescent female school dropouts who use drugs and engage in risky sex: Effects of a brief pilot intervention in Cape Town, South Africa. AIDS Care 2019, 31, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Papas, R.K.; Sidle, J.E.; Gakinya, B.N.; Baliddawa, J.B.; Martino, S.; Mwaniki, M.M.; Songole, R.; Omolo, O.E.; Kamanda, A.M.; Ayuku, D.O.; et al. Treatment outcomes of a stage 1 cognitive-behavioral trial to reduce alcohol use among human immunodeficiency virus-infected out-patients in western Kenya. Addiction 2011, 106, 2156–2166. [Google Scholar] [CrossRef] [Green Version]
- Sorsdahl, K.; Stein, D.J.; Weich, L.; Fourie, D.; Myers, B. The effectiveness of a hospital-based intervention for patients with substance-use problems in the Western Cape. S. Afr. Med. J. 2012, 102, 634–635. [Google Scholar] [CrossRef] [Green Version]
- Carney, T.; Johnson, K.; Carrico, A.; Myers, B. Acceptability and feasibility of a brief substance use intervention for adolescents in Cape Town, South Africa: A pilot study. Int. J. Psychol. 2020, 55, 1016–1025. [Google Scholar] [CrossRef]
- Madhombiro, M.; Dube, B.; Dube, M.; Zunza, M.; Chibanda, D.; Rusakaniko, S.; Seedat, S. Intervention for alcohol use disorders at an HIV care clinic in Harare: A pilot and feasibility study. Addict. Sci. Clin. Pract. 2019, 14, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Magidson, J.F.; Joska, J.A.; Belus, J.M.; Andersen, L.S.; Regenauer, K.S.; Rose, A.L.; Myers, B.; Majokweni, S.; O’Cleirigh, C.; Safren, S.A. Project Khanya: Results from a pilot randomized type 1 hybrid effectiveness-implementation trial of a peer-delivered behavioural intervention for ART adherence and substance use in HIV care in South Africa. J. Int. AIDS Soc. 2021, 24, e25720. [Google Scholar] [CrossRef] [PubMed]
- Rotheram-Borus, M.J.; Lightfoot, M.; Kasirye, R.; Desmond, K. Vocational training with HIV prevention for Ugandan youth. AIDS Behav. 2012, 16, 1133–1137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tang, A.M.; Hamunime, N.; Adams, R.A.; Kanyinga, G.; Fischer-Walker, C.; Agolory, S.; Prybylski, D.; Mutenda, N.; Sughrue, S.; Walker, D.D.; et al. Introduction of an alcohol-related electronic screening and brief intervention (eSBI) program to reduce hazardous alcohol consumption in Namibia’s antiretroviral treatment (ART) program. AIDS Behav. 2019, 23, 3078–3092. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conroy, A.A.; Ruark, A.; McKenna, S.A.; Tan, J.Y.; Darbes, L.A.; Hahn, J.A.; Mkandawire, J. The unaddressed needs of alcohol-using couples on antiretroviral therapy in Malawi: Formative research on multilevel interventions. AIDS Behav. 2020, 24, 1599–1611. [Google Scholar] [CrossRef]
- Kerrigan, D.; Mbwambo, J.; Likindikoki, S.; Beckham, S.; Mwampashi, A.; Shembilu, C.; Mantsios, A.; Leddy, A.; Davis, W.; Galai, N. Project Shikamana: Baseline findings from a community empowerment-based combination HIV prevention trial among female sex workers in Iringa, Tanzania. J. Acquir. Immune Defic. Syndr. 2017, 74 (Suppl. 1), S60–S68. [Google Scholar] [CrossRef] [Green Version]
- Kane, J.C.; Sharma, A.; Murray, L.K.; Chander, G.; Kanguya, T.; Skavenski, S.; Chitambi, C.; Lasater, M.E.; Paul, R.; Cropsey, K.; et al. Efficacy of the Common Elements Treatment Approach (CETA) for unhealthy alcohol use among adults with HIV in Zambia: Results from a pilot randomized controlled trial. AIDS Behav. 2022, 26, 523–536. [Google Scholar] [CrossRef]
- Magidson, J.F.; Andersen, L.S.; Satinsky, E.N.; Myers, B.; Kagee, A.; Anvari, M.; Joska, J.A. “Too much boredom isn’t a good thing”: Adapting behavioral activation for substance use in a resource-limited South African HIV care setting. Psychotherapy 2020, 57, 107–118. [Google Scholar] [CrossRef]
- Morojele, N.K.; Kitleli, N.; Ngako, K.; Kekwaletswe, C.T.; Nkosi, S.; Fritz, K.; Parry, C.D. Feasibility and acceptability of a bar-based sexual risk reduction intervention for bar patrons in Tshwane, South Africa. Sahara J. 2014, 11, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Myers, B.; Carney, T.; Browne, F.A.; Wechsberg, W.M. A trauma-informed substance use and sexual risk reduction intervention for young South African women: A mixed-methods feasibility study. BMJ Open 2019, 9, e024776. [Google Scholar] [CrossRef] [Green Version]
- Myers, B.; Parry, C.D.H.; Morojele, N.K.; Nkosi, S.; Shuper, P.A.; Kekwaletswe, C.T.; Sorsdahl, K.R. “Moving forward with life”: Acceptability of a brief alcohol reduction intervention for people receiving antiretroviral therapy in South Africa. Int. J. Environ. Res. Public Health. 2020, 17, 5706. [Google Scholar] [CrossRef] [PubMed]
- Myers, B.; Sorsdahl, K.; Morojele, N.K.; Kekwaletswe, C.; Shuper, P.A.; Parry, C.D. “In this thing I have everything I need”: Perceived acceptability of a brief alcohol-focused intervention for people living with HIV. AIDS Care 2017, 29, 209–213. [Google Scholar] [CrossRef] [PubMed]
- Sorsdahl, K.; Stein, D.J.; Pasche, S.; Jacobs, Y.; Kader, R.; Odlaug, B.; Richter, S.; Myers, B.; Grant, J.E. A novel brief treatment for methamphetamine use disorders in South Africa: A randomised feasibility trial. Addict. Sci. Clin. Pract. 2021, 16, 3. [Google Scholar] [CrossRef] [PubMed]
- LʼEngle, K.L.; Mwarogo, P.; Kingola, N.; Sinkele, W.; Weiner, D.H. A randomized controlled trial of a brief intervention to reduce alcohol use among female sex workers in Mombasa, Kenya. J. Acquir. Immune Defic. Syndr. 2014, 67, 446–453. [Google Scholar] [CrossRef] [PubMed]
- Madhombiro, M.; Kidd, M.; Dube, B.; Dube, M.; Mutsvuke, W.; Muronzie, T.; Zhou, D.T.; Derveeuw, S.; Chibanda, D.; Chingono, A.; et al. Effectiveness of a psychological intervention delivered by general nurses for alcohol use disorders in people living with HIV in Zimbabwe: A cluster randomized controlled trial. J. Int. AIDS Soc. 2020, 23, e25641. [Google Scholar] [CrossRef] [PubMed]
- Murray, L.K.; Kane, J.C.; Glass, N.; Skavenski van Wyk, S.; Melendez, F.; Paul, R.; Kmett Danielson, C.; Murray, S.M.; Mayeya, J.; Simenda, F.; et al. Effectiveness of the Common Elements Treatment Approach (CETA) in reducing intimate partner violence and hazardous alcohol use in Zambia (VATU): A randomized controlled trial. PLoS Med. 2020, 17, e1003056. [Google Scholar] [CrossRef] [PubMed]
- Omeje, J.C.; Otu, M.S.; Aneke, A.O.; Adikwu, V.O.; Nwaubani, O.O.; Chigbu, E.F.; Onuigbo, L.N.; Udom, I.E.; Aye, E.N.; Akaneme, I.N.; et al. Effect of rational emotive health therapy on alcohol use among community-dwelling, HIV-positive patients. Medicine 2018, 97, e11688. [Google Scholar] [CrossRef]
- Papas, R.K.; Gakinya, B.N.; Mwaniki, M.M.; Lee, H.; Keter, A.K.; Martino, S.; Klein, D.A.; Liu, T.; Loxley, M.P.; Sidle, J.E.; et al. A randomized clinical trial of a group cognitive-behavioral therapy to reduce alcohol use among human immunodeficiency virus-infected outpatients in western Kenya. Addiction 2021, 116, 305–318. [Google Scholar] [CrossRef]
- Wechsberg, W.M.; Bonner, C.P.; Zule, W.A.; van der Horst, C.; Ndirangu, J.; Browne, F.A.; Kline, T.L.; Howard, B.N.; Rodman, N.F. Addressing the nexus of risk: Biobehavioral outcomes from a cluster randomized trial of the Women’s Health CoOp Plus in Pretoria, South Africa. Drug Alcohol. Depend. 2019, 195, 16–26. [Google Scholar] [CrossRef]
- Wechsberg, W.M.; Zule, W.A.; El-Bassel, N.; Doherty, I.A.; Minnis, A.M.; Novak, S.D.; Myers, B.; Carney, T. The male factor: Outcomes from a cluster randomized field experiment with a couples-based HIV prevention intervention in a South African township. Drug Alcohol Depend. 2016, 161, 307–315. [Google Scholar] [CrossRef] [Green Version]
- Wechsberg, W.M.; Jewkes, R.; Novak, S.P.; Kline, T.; Myers, B.; Browne, F.A.; Carney, T.; Morgan Lopez, A.A.; Parry, C. A brief intervention for drug use, sexual risk behaviours and violence prevention with vulnerable women in South Africa: A randomised trial of the Women’s Health CoOp. BMJ Open 2013, 3, e002622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wechsberg, W.M.; Zule, W.A.; Luseno, W.K.; Kline, T.L.; Browne, F.A.; Novak, S.P.; Ellerson, R.M. Effectiveness of an adapted evidence-based woman-focused intervention for sex workers and non-sex workers: The Women’s Health CoOp in South Africa. J. Drug Issues 2011, 41, 233–252. [Google Scholar] [CrossRef]
- Sorsdahl, K.; Stein, D.J.; Corrigall, J.; Cuijpers, P.; Smits, N.; Naledi, T.; Myers, B. The efficacy of a blended motivational interviewing and problem solving therapy intervention to reduce substance use among patients presenting for emergency services in South Africa: A randomized controlled trial. Subst. Abuse Treat. Prev. Policy 2015, 10, 46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harder, V.S.; Musau, A.M.; Musyimi, C.W.; Ndetei, D.M.; Mutiso, V.N. A randomized clinical trial of mobile phone motivational interviewing for alcohol use problems in Kenya. Addiction 2020, 115, 1050–1060. [Google Scholar] [CrossRef]
- Huis In ‘t Veld, D.; Ensoy-Musoro, C.; Pengpid, S.; Peltzer, K.; Colebunders, R. The efficacy of a brief intervention to reduce alcohol use in persons with HIV in South Africa, a randomized clinical trial. PLoS ONE 2019, 14, e0220799. [Google Scholar] [CrossRef]
- Rendall-Mkosi, K.; Morojele, N.; London, L.; Moodley, S.; Singh, C.; Girdler-Brown, B. A randomized controlled trial of motivational interviewing to prevent risk for an alcohol-exposed pregnancy in the Western Cape, South Africa. Addiction 2013, 108, 725–732. [Google Scholar] [CrossRef] [Green Version]
- Wandera, B.; Tumwesigye, N.M.; Nankabirwa, J.I.; Mafigiri, D.K.; Parkes-Ratanshi, R.M.; Kapiga, S.; Hahn, J.; Sethi, A.K. Efficacy of a single, brief alcohol reduction intervention among men and women living with HIV/AIDS and using alcohol in Kampala, Uganda: A randomized trial. J. Int. Assoc. Provid. AIDS Care 2017, 16, 276–285. [Google Scholar] [CrossRef] [Green Version]
- Pengpid, S.; Peltzer, K.; Van der Heever, H.; Skaal, L. Screening and Brief Interventions for Hazardous and Harmful Alcohol Use among University Students in South Africa: Results from a Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2013, 10, 2043–2057. [Google Scholar] [CrossRef] [Green Version]
- Mertens, J.R.; Ward, C.L.; Bresick, G.F.; Broder, T.; Weisner, C.M. Effectiveness of nurse-practitioner-delivered brief motivational intervention for young adult alcohol and drug use in primary care in South Africa: A randomized clinical trial. Alcohol Alcohol. 2014, 49, 430–438. [Google Scholar] [CrossRef] [Green Version]
- Marais, S.; Jordaan, E.; Viljoen, D.; Olivier, L.; de Waal, J.; Poole, C. The effect of brief interventions on the drinking behaviour of pregnant women in a high-risk rural South African community: A cluster randomised trial. Early Child Dev. Care 2011, 181, 463–474. [Google Scholar] [CrossRef]
- Ward, C.L.; Mertens, J.R.; Bresick, G.F.; Little, F.; Weisner, C.M. Screening and brief intervention for substance misuse: Does it reduce aggression and HIV-related risk behaviours? Alcohol Alcohol. 2015, 50, 302–309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peltzer, K.; Naidoo, P.; Louw, J.; Matseke, G.; Zuma, K.; McHunu, G.; Tutshana, B.; Mabaso, M. Screening and brief interventions for hazardous and harmful alcohol use among patients with active tuberculosis attending primary public care clinics in South Africa: Results from a cluster randomized controlled trial. BMC Public Health 2013, 13, 699. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pengpid, S.; Peltzer, K.; Skaal, L.; Van der Heever, H. Screening and brief interventions for hazardous and harmful alcohol use among hospital outpatients in South Africa: Results from a randomized controlled trial. BMC Public Health 2013, 13, 644. [Google Scholar] [CrossRef] [Green Version]
- Rotheram-Borus, M.J.; Tomlinson, M.; Le Roux, I.; Stein, J.A. Alcohol Use, Partner Violence, and Depression A Cluster Randomized Controlled Trial Among Urban South African Mothers Over 3 Years. Am. J. Prev. Med. 2015, 49, 715–725. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peltzer, K.; Tabane, C.; Matseke, G.; Simbayi, L. Lay counsellor-based risk reduction intervention with HIV positive diagnosed patients at public HIV counselling and testing sites in Mpumalanga, South Africa. Eval. Program Plan. 2010, 33, 379–385. [Google Scholar] [CrossRef]
- Pitpitan, E.V.; Kalichman, S.C.; Garcia, R.L.; Cain, D.; Eaton, L.A.; Simbayi, L.C. Mediators of behavior change resulting from a sexual risk reduction intervention for STI patients, Cape Town, South Africa. J. Behav. Med. 2015, 38, 194–203. [Google Scholar] [CrossRef] [Green Version]
- Louwagie, G.; Kanaan, M.; Morojele, N.K.; Van Zyl, A.; Moriarty, A.S.; Li, J.; Siddiqi, K.; Turner, A.; Mdege, N.D.; Omole, O.B.; et al. Effect of a brief motivational interview and text message intervention targeting tobacco smoking, alcohol use and medication adherence to improve tuberculosis treatment outcomes in adult patients with tuberculosis: A multicentre, randomised controlled trial of the ProLife programme in South Africa. BMJ Open 2022, 12, e056496. [Google Scholar] [CrossRef] [PubMed]
- Jemmott III, J.B.; Jemmott, L.S.; O’Leary, A.; Ngwane, Z.; Icard, L.D.; Heeren, G.A.; Mtose, X.; Carty, C. Cluster-randomized controlled trial of an HIV/sexually transmitted infection risk-reduction intervention for South African men. Am. J. Public Health 2014, 104, 467–473. [Google Scholar] [CrossRef]
- Tibbits, M.K.; Smith, E.A.; Caldwell, L.L.; Flisher, A.J. Impact of HealthWise South Africa on polydrug use and high-risk sexual behavior. Health Educ. Res 2011, 26, 653–663. [Google Scholar] [CrossRef]
- Manyaapelo, T.; Van den Borne, B.; Ruiter, R.A.C.; Sifunda, S.; Reddy, P. Effectiveness of a health behavioural intervention aimed at reduction of risky sexual behaviours among young men in the KwaZulu-Natal province, South Africa. Int. J. Environ. Res. Public Health 2019, 16, 1938. [Google Scholar] [CrossRef] [Green Version]
- Moscoe, E.; Agot, K.; Thirumurthy, H. Effect of a prize-linked savings intervention on savings and healthy behaviors among Mmen in Kenya: A randomized clinical trial. JAMA Netw. Open 2019, 2, e1911162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Massarwi, A.A.; Cluver, L.; Meinck, F.; Doubt, J.; Lachman, J.M.; Shenderovich, Y.; Green, O. Mediation pathways for reduced substance use among parents in South Africa: A randomized controlled trial. BMC Public Health 2021, 21, 1656. [Google Scholar] [CrossRef] [PubMed]
- Eze, I.I.; Mbachu, C.O.; Azuogu, B.N.; Ossai, E.; Unah, A.I.; Akamike, I.C.; Onwasigwe, C.N. Effect of on-site behavioural modification intervention on lifestyle risk factors of hypertension among adult market traders in Abakaliki, Nigeria. Int. J. Health Promot. Educ. 2021, 59, 35–49. [Google Scholar] [CrossRef]
- Bachanas, P.; Kidder, D.; Medley, A.; Pals, S.L.; Carpenter, D.; Howard, A.; Antelman, G.; DeLuca, N.; Muhenje, O.; Sheriff, M.; et al. Delivering prevention interventions to people living with HIV in clinical care settings: Results of a cluster randomized trial in Kenya, Namibia, and Tanzania. AIDS Behav. 2016, 20, 2110–2118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burnhams, N.H.; London, L.; Laubscher, R.; Nel, E.; Parry, C. Results of a cluster randomised controlled trial to reduce risky use of alcohol, alcohol-related HIV risks and improve help-seeking behaviour among safety and security employees in the Western Cape, South Africa. Subst. Abuse Treat. Prev. Policy 2015, 10, 18. [Google Scholar] [CrossRef] [Green Version]
- Cubbins, L.A.; Kasprzyk, D.; Montano, D.; Jordan, L.P.; Woelk, G. Alcohol use and abuse among rural Zimbabwean adults: A test of a community-level intervention. Drug Alcohol Depend. 2012, 124, 333–339. [Google Scholar] [CrossRef] [Green Version]
- Wagman, J.A.; Gray, R.H.; Campbell, J.C.; Thoma, M.; Ndyanabo, A.; Ssekasanvu, J.; Nalugoda, F.; Kagaayi, J.; Nakigozi, G.; Serwadda, D.; et al. Effectiveness of an integrated intimate partner violence and HIV prevention intervention in Rakai, Uganda: Analysis of an intervention in an existing cluster randomised cohort. Lancet Glob. Health 2015, 3, e23–e33. [Google Scholar] [CrossRef] [Green Version]
- London, L. The dop’system, alcohol abuse and social control amongst farm workers in South Africa: A public health challenge. Soc. Sci. Med 1999, 48, 1407–1414. [Google Scholar] [CrossRef]
- Martinez, P.; Røislien, J.; Naidoo, N.; Clausen, T. Alcohol abstinence and drinking among African women: Data from the World Health Surveys. BMC Public Health 2011, 11, 160. [Google Scholar] [CrossRef] [Green Version]
- Lange, S.; Probst, C.; Gmel, G.; Rehm, J.; Burd, L.; Popova, S. Global prevalence of Fetal Alcohol Spectrum Disorder among children and youth: A systematic review and meta-analysis. JAMA Pediatr. 2017, 171, 948–956. [Google Scholar] [CrossRef]
- Adnams, C.M. Fetal alcohol spectrum disorder in Africa. Curr. Opin. Psychiatry 2017, 30, 108–112. [Google Scholar] [CrossRef] [PubMed]
- Myers, B.; Joska, J.A.; Lund, C.; Levitt, N.S.; Butler, C.C.; Naledi, T.; Milligan, P.; Stein, D.J.; Sorsdahl, K. Patient preferences for the integration of mental health counseling and chronic disease care in South Africa. Patient Prefer. Adherence 2018, 12, 1797. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abrahams, N.; Mhlongo, S.; Chirwa, E.; Lombard, C.; Dunkle, K.; Seedat, S.; Kengne, A.P.; Myers, B.; Peer, N.; García-Moreno, C.M.; et al. Rape survivors in South Africa: Analysis of the baseline socio-demographic and health characteristics of a rape cohort. Glob. Health Action 2020, 13, 1834769. [Google Scholar] [CrossRef] [PubMed]
- Myers, B.; Bantjes, J.; Lochner, C.; Mortier, P.; Kessler, R.C.; Stein, D.J. Maltreatment during childhood and risk for common mental disorders among first year university students in South Africa. Soc. Psychiatry Psychiatr. Epidemiol 2021, 56, 1175–1187. [Google Scholar] [CrossRef] [PubMed]
- Statistics South Africa. Mid-Year Population Estimates. 2021. Available online: https://www.statssa.gov.za/publications/P0302/P03022021.pdf (accessed on 13 April 2022).
- Wechsberg, W.M.; van der Horst, C.; Ndirangu, J.; Doherty, I.A.; Kline, T.; Browne, F.A.; Belus, J.M.; Nance, R.; Zule, W.A. Seek, test, treat: Substance-using women in the HIV treatment cascade in South Africa. Addict. Sci. Clin. Pract. 2017, 12, 12. [Google Scholar] [CrossRef] [Green Version]
- Myers, B.; Lund, C.; Lombard, C.; Joska, J.; Levitt, N.; Butler, C.; Cleary, S.; Naledi, T.; Milligan, P.; Stein, D.J.; et al. Comparing dedicated and designated models of integrating mental health into chronic disease care: Study protocol for a cluster randomized controlled trial. Trials 2018, 19, 185. [Google Scholar] [CrossRef]
- Howard, B.N.; Van Dorn, R.; Myers, B.J.; Zule, W.A.; Browne, F.A.; Carney, T.; Wechsberg, W.M. Barriers and facilitators to implementing an evidence-based woman-focused intervention in South African health services. BMC Health Serv. Res 2017, 17, 746. [Google Scholar] [CrossRef] [Green Version]
- Myers, B.; Kline, T.L.; Doherty, I.A.; Carney, T.; Wechsberg, W.M. Perceived need for substance use treatment among young women from disadvantaged communities in Cape Town, South Africa. BMC Psychiatry 2014, 14, 100. [Google Scholar] [CrossRef] [Green Version]
- Morris, Z.S.; Wooding, S.; Grant, J. The answer is 17 years, what is the question: Understanding time lags in translational research. J. R. Soc. Med 2011, 104, 510–520. [Google Scholar] [CrossRef]
- Jacobs, Y.; Myers, B.; van der Westhuizen, C.; Brooke-Sumner, C.; Sorsdahl, K. Task sharing or task dumping: Counsellors experiences of delivering a psychosocial intervention for mental health problems in South Africa. Community Ment. Health J. 2021, 57, 1082–1093. [Google Scholar] [CrossRef]
- Myers, B.; Louw, J.; Pasche, S. Gender differences in barriers to alcohol and other drug treatment in Cape Town South Africa. Afr. J. Psychiatry 2011, 14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Myers, B.; Carney, T.; Wechsberg, W.M. “Not on the agenda”: A qualitative study of influences on health services use among poor young women who use drugs in Cape Town, South Africa. Int. J. Drug Policy 2016, 30, 52–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cooper, D.K. Christiaan Barnard—The surgeon who dared: The story of the first human-to-human heart transplant. Glob. Cardiol. Sci. Pract. 2018, 2018. [Google Scholar] [CrossRef] [PubMed]
- Ertl, V.; Groß, M.; Mwaka, S.O.; Neuner, F. Treating alcohol use disorder in the absence of specialized services—Evaluation of the moving inpatient Treatment Camp approach in Uganda. BMC Psychiatry 2021, 21, 601. [Google Scholar] [CrossRef]
- Kurth, A.E.; Cherutich, P.; Conover, R.; Chhun, N.; Bruce, R.D.; Lambdin, B.H. The opioid epidemic in Africa and its impact. Curr. Addict. Rep. 2018, 5, 428–453. [Google Scholar] [CrossRef]
- Gouse, H. Implementation of the Matrix Model in Cape Town, South Africa: Evaluating treatment engagement and relapse outcomes. In Proceedings of the 2015 College on Problems of Drug Dependence, Phoenix, AZ, USA, 13–18 June 2015. [Google Scholar]
- Huber, A.; Ling, W.; Shoptaw, S.; Gulati, V.; Brethen, P.; Rawson, R. Integrating treatments for methamphetamine abuse: A psychosocial perspective. J. Addict. Dis. 1997, 16, 41–50. [Google Scholar] [CrossRef]
- Gichane, M.W.; Wechsberg, W.M.; Ndirangu, J.; Browne, F.A.; Bonner, C.P.; Grimwood, A.; Shaikh, N.; Howard, B.; Zule, W.A. Implementation science outcomes of a gender-focused HIV and alcohol risk-reduction intervention in usual-care settings in South Africa. Drug Alcohol Depend. 2020, 215, 108206. [Google Scholar] [CrossRef]
- Gichane, M.W.; Wechsberg, W.M.; Ndirangu, J.; Howard, B.; Bonner, C.P.; Browne, F.A.; Zule, W.A. Sustainability of a gender-focused HIV and alcohol risk-reduction intervention in usual care settings in South Africa: A mixed methods analysis. AIDS Care 2021, 33 (Suppl. 1), 11–17. [Google Scholar] [CrossRef]
- van der Westhuizen, C.; Myers, B.; Malan, M.; Naledi, T.; Roelofse, M.; Stein, D.J.; Lahri, S.a.; Sorsdahl, K. Implementation of a screening, brief intervention and referral to treatment programme for risky substance use in South African emergency centres: A mixed methods evaluation study. PLoS ONE 2019, 14, e0224951. [Google Scholar]
- Mutyambizi-Mafunda, V.; Myers, B.; Sorsdahl, K.; Chanakira, E.; Lund, C.; Cleary, S. Economic evaluations of psychological treatments for common mental disorders in low-and middle-income countries: Protocol for a systematic review. Glob. Health Action 2021, 14, 1972561. [Google Scholar] [CrossRef]

| Citation | Region/Sample | Setting/Topics | Intervention | Outcomes |
|---|---|---|---|---|
| Behavioral | ||||
| L’Engle et al. (2014) [70] | Kenya: 818 women who conduct sex work living with or at risk for contracting HIV who scored between 7 and 19 on the AUDIT | Six 20-min counseling sessions delivered one-on-one by trained nurses over 6 months at project site EtOH, GBV, SRH | Adapted WHO Brief Motivational Intervention for Alcohol Use and counseling sessions | * Significant reduction in binge drinking at 6- and 12-month follow-ups with intervention participants reporting less than one-third the odds of higher levels of drinking than the control group |
| Madhombiro et al. (2020) [71] | Zimbabwe: 529 adults living with HIV who also had an AUD and were on combination ART | Ten sessions lasting 45 to 60 min each with trained nurses at clinic locations EtOH, HIV | MI-CBT working with participants’ AUDIT scores, personalized information on addressing alcohol use and achieving HIV outcomes | * Difference in AUDIT scores between arms * Reduction in viral load between arms |
| Murray et al. (2020) [72] | Zambia: 123 heterosexual couples where the woman reported experiencing IPV by her male partner | Two-session sex-stratified groups with one additional spousal substance use support session delivered by lay counselors EtOH, IPV | CETA to teach CBT decision rules with elements of psychoeducation and substance use reduction | * Reduction in female reports of past-year IPV and in male reports of perpetrated violence * Significant treatment effects on male alcohol use and smaller effects on female alcohol use |
| Omeje et al. (2018) [73] | Nigeria: 124 community-dwelling adults living with HIV who experience AUD symptoms | 20 sessions (50 min each) twice a week, with 2 weeks of follow-up by trained researchers EtOH, HIV | REHT for AUD focused on beliefs related to AUD and techniques to reduce symptoms | * The REHT intervention led to a reduction in AUD symptoms in the treatment group compared with the waitlist control group * Difference in decrease in alcohol-related irrational beliefs between treatment and control groups |
| Papas et al. (2021) [74] | Kenya: 614 adults enrolled as an AMPATH HIV outpatient with hazardous drinking | Six weekly 90-min group sessions delivered by paraprofessional counselors EtOH, HIV | CBT intervention consisting of group sessions teaching coping skills for alcohol reduction | * Significantly lower percentage of drinking days and drinks per drinking day in CBT than healthy life-styles education overall and at all study phases |
| Wechsberg et al. (2021) [28] | South Africa: 480 women living with HIV who used AODs | Implementation science four-cycle stepped- wedge design of an evidence-based intervention delivered by trained clinic staff and researchers in groups at clinics and substance use rehabilitation and treatment centers EtOH, METH, OPI, HIV, IPV/GBV, SRH | Adapted WHC, an evidence-based gender-focused HIV intervention for women living with HIV, to reduce AOD use, GBV, and sexual risk and to increase linkage to HIV care among women who use AODs | * WHC increased ART adherence and reduced alcohol use * Compared with the first cycle, women in the fourth cycle were less likely to report AUD risk and were 4 times more likely to report ART adherence at 6-month follow-up |
| Wechsberg et al. (2019) [75] | South Africa: 641 Black women from 14 mapped AOD “hot spots” | Two intervention group sessions 1 week apart administered by experienced, multilingual female interventionists from the community EtOH, COC, OPI, THC, HIV, SRH, IPV | WHC+, an empowerment-based woman-focused HIV intervention to reduce sex risk, AOD use, and GBV and to increase linkage to HIV care among women who use AODs | * The WHC+ arm was less likely to report frequent heavy drinking and fewer heavy drinking days at 6-month follow-up but not at 12-month follow-up * The WHC+ arm was less likely to report being attacked with a weapon, beaten, or sexually abused by a boyfriend at 6-month follow-up * The WHC+ arm reported more frequent condom negotiation, using a condom while high, and refusing sex without a condom with a boyfriend in the past 3 months at 6-month follow-up |
| Wechsberg et al. (2016) [76] | South Africa: 300 couples: 300 men who used alcohol and their partners (300 women) | 3-h workshop delivered by peer educators in groups of couple dyads EtOH, METH, THC, COC, OPI, Methaqualone, GBV, HIV, SRH | CHC adapted from the WHC to provide couples with skill-building exercises around communication and sexual expectations | * Heavy drinking decreased among women in the CHC Heavy drinking decreased among men in all arms Condom use increased in all arms for women; men in the CHC were more likely to report consistent condom use |
| Wechsberg et al. (2013) [77] | South Africa: 720 women who use AODs | Two-session peer-facilitated group intervention with four modules each EtOH, METH, OPI, COC, THC, Methaqualone, GBV, HIV | Adapted WHC, an empowerment-based, woman-focused HIV intervention to reduce sex risk, AOD use, and GBV | At 6-month follow-up:
|
| Wechsberg et al. (2011) [78] | South Africa: 617 women who conduct sex work or engage in condomless sex and report alcohol use | Two-session (50 min each) cue card intervention delivered by trained interventionists in groups EtOH, COC, THC, OPI, AMP, METH, Ecstasy, HIV, GBV | WHC, an empowerment-based, woman-focused HIV intervention to reduce sex risk, AOD use, and GBV | Women who did not conduct sex work had a lower mean number of days drinking and were less likely to qualify for alcohol dependence compared with the control group * Greater reductions in drug use among WHC participants * Women who conducted sex work were less likely to report physical abuse by main partner at 6-month follow-up |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wechsberg, W.M.; van der Drift, I.; Howard, B.N.; Myers, B.; Browne, F.A.; Bonner, C.P.; Carney, T.; Ndirangu, J.; Washio, Y. Gender and Context Matter: Behavioral and Structural Interventions for People Who Use Alcohol and Other Drugs in Africa. Int. J. Environ. Res. Public Health 2022, 19, 8661. https://doi.org/10.3390/ijerph19148661
Wechsberg WM, van der Drift I, Howard BN, Myers B, Browne FA, Bonner CP, Carney T, Ndirangu J, Washio Y. Gender and Context Matter: Behavioral and Structural Interventions for People Who Use Alcohol and Other Drugs in Africa. International Journal of Environmental Research and Public Health. 2022; 19(14):8661. https://doi.org/10.3390/ijerph19148661
Chicago/Turabian StyleWechsberg, Wendee M., Isa van der Drift, Brittni N. Howard, Bronwyn Myers, Felicia A. Browne, Courtney Peasant Bonner, Tara Carney, Jacqueline Ndirangu, and Yukiko Washio. 2022. "Gender and Context Matter: Behavioral and Structural Interventions for People Who Use Alcohol and Other Drugs in Africa" International Journal of Environmental Research and Public Health 19, no. 14: 8661. https://doi.org/10.3390/ijerph19148661