
“It Depends on Where You Are and What Job You Do”: Differences in Tobacco Use across Career Fields in the United States Air Force

 , , and
, , and
Abstract
:1. Introduction
The Current Study
2. Materials and Methods
2.1. Focus Group Procedures
2.2. Data Analysis
3. Results
3.1. Broad Perceptions of Tobacco Use across Career Fields
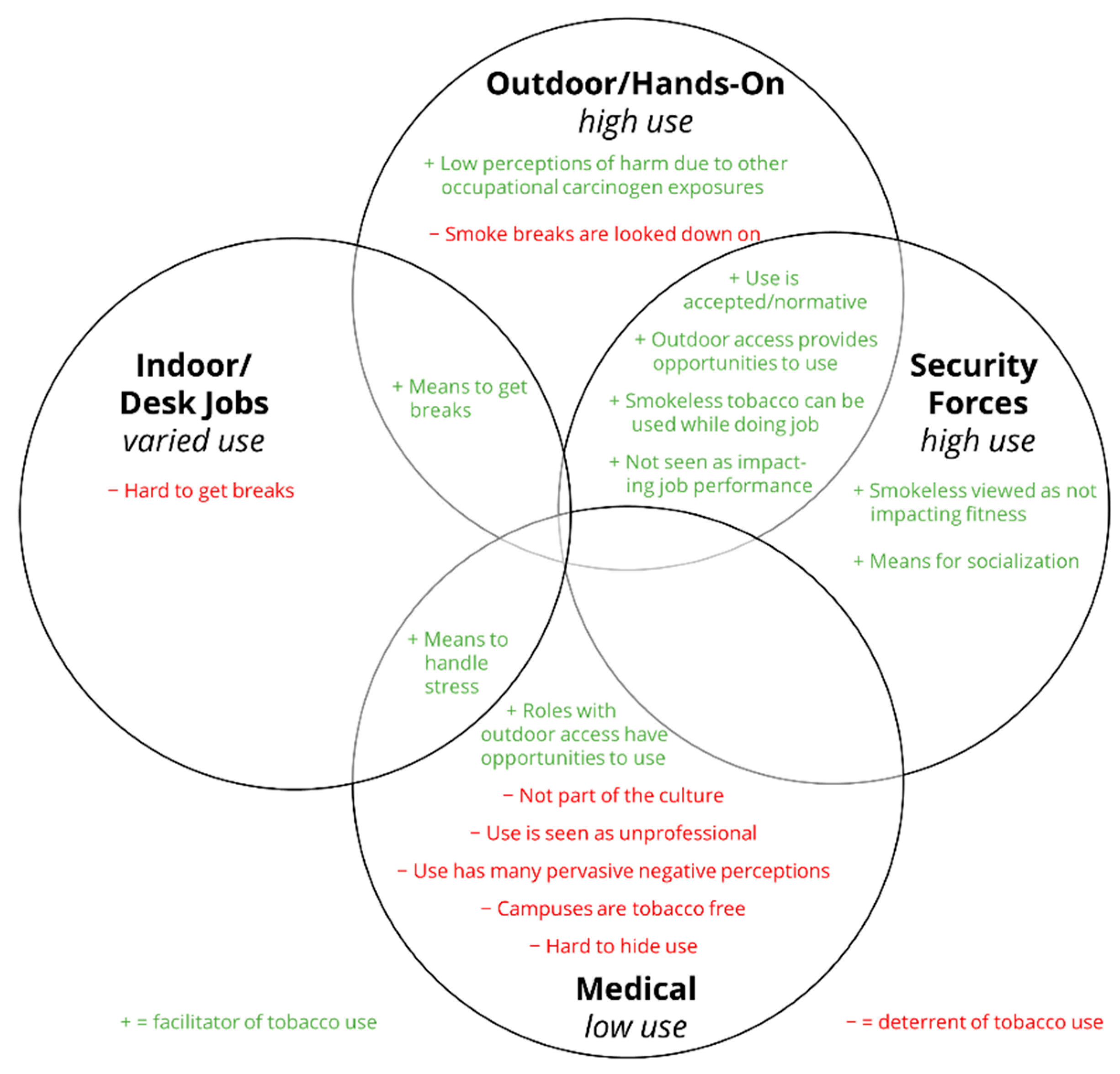
3.2. Descriptions of Tobacco Use by Career Field
4. Discussion
Limitations
5. Conclusions
6. Disclaimer
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Asfar, T.; Arheart, K.L.; Dietz, N.A.; Caban-Martinez, A.J.; Fleming, L.E.; Lee, D.J. Changes in cigarette smoking behavior among US young workers from 2005 to 2010: The role of cccupation. Nicotine Tob. Res. 2016, 18, 1414–1423. [Google Scholar] [CrossRef] [PubMed]
- Little, M.; Fahey, M.; Klesges, R.; McMurry, T.; Talcott, G. Evaluating the effects of a brief tobacco intervention in the U.S. Air Force. Nicotine Tob. Res. 2020, 22, 1569–1577. [Google Scholar] [CrossRef] [PubMed]
- Little, M.A.; Fahey, M.C.; Wang, X.-Q.; Talcott, G.W.; McMurry, T.; Klesges, R.C. Trends in tobacco use among young adults presenting for military service in the United States Air Force between 2013 and 2018. Subst. Abus. Misuse 2021, 56, 370–376. [Google Scholar] [CrossRef]
- Meadows, S.O.; Engel, C.C.; Collins, R.L.; Beckman, R.L.; Cefalu, M.; Hawes-Dawson, J.; Doyle, M.; Kress, A.M.; Sontag-Padilla, L.; Ramchand, R.; et al. 2015 Department of Defense Health Related Behaviors Survey (HRBS). Rand Health Q. 2018, 8, 5. [Google Scholar] [PubMed]
- Syamlal, G.; King, B.A.; Mazurek, J.M. Tobacco use among working adults—United States, 2014–2016. MMWR Morb. Mortal. Wkly. Rep. 2017, 66, 1130–1135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ham, D.C.; Przybeck, T.; Strickland, J.R.; Luke, D.A.; Bierut, L.J.; Evanoff, B.A. Occupation and workplace policies predict smoking behaviors: Analysis of national data from the current population survey. J. Occup. Environ. Med. 2011, 53, 1337–1345. [Google Scholar] [CrossRef] [Green Version]
- Hammond, D. Smoking behaviour among young adults: Beyond youth prevention. Tob. Control 2005, 14, 181–185. [Google Scholar] [CrossRef] [Green Version]
- Fagan, P.; Moolchan, E.T.; Lawrence, D.; Fernander, A.; Ponder, P.K. Identifying health disparities across the tobacco continuum. Addiction 2007, 102 (Suppl. S2), 5–29. [Google Scholar] [CrossRef]
- Nelson, D.E.; Kirkendall, R.S.; Lawton, R.L.; Chrismon, J.H.; Merritt, R.K.; Arday, D.A.; Giovino, G.A. Surveillance for smoking-attributable mortality and years of potential life lost, by state--United States, 1990. MMWR CDC Surveill. Summ. 1994, 43, 1–8. [Google Scholar]
- Pirrie, M.; McGrath, H.; Garcia, J.M.; Lambraki, I.; Pieters, K. Literature Review: Workplace Tobacco Cessation Initiatives for Young Adults; Propel Centre for Population Health Impact, University of Waterloo: Waterloo, ON, USA, 2012. [Google Scholar]
- Katainen, A. Social class differences in the accounts of smoking—Striving for distinction? Sociol. Health Illn. 2010, 32, 1087–1101. [Google Scholar] [CrossRef]
- Sorensen, G.; Quintiliani, L.; Pereira, L.; Yang, M.; Stoddard, A. Work experiences and tobacco use: Findings from the gear up for health study. J. Occup. Environ. Med. 2009, 51, 87–94. [Google Scholar] [CrossRef] [PubMed]
- Khorrami, Z.; Zolala, F.; Haghdoost, A.; Sadatmoosavi, A.; Ben Taleb, Z.; Kondracki, A.; Ward, K.D.; Shahbaz, M.; Ebrahimi Kalan, M. Job-related stress and tobacco smoking: A systematic review. J. Workplace Behav. Health 2021, 36, 259–277. [Google Scholar] [CrossRef]
- Richardson, L.K.; Frueh, B.C.; Acierno, R. Prevalence estimates of combat-related post-traumatic stress disorder: Critical review. Aust. N. Z. J. Psychiatry 2010, 44, 4–19. [Google Scholar] [CrossRef] [Green Version]
- Brooks, S.K.; Greenberg, N. Non-deployment factors affecting psychological wellbeing in military personnel: Literature review. J. Ment. Health 2018, 27, 80–90. [Google Scholar] [CrossRef] [PubMed]
- Porter, K.J.; Krukowski, R.A.; Bonilla, G.; McKenna, L.; Talcott, G.; Little, M. Using the socio-ecological model to explore facilitators and deterrents to tobacco use among airmen in technical training. Mil. Med. 2021, usab075. [Google Scholar] [CrossRef]
- NVivo Qualitative Data Analysis Software; v12; QSR International Pty Ltd.: Doncaster, Australia, 2018.
- Hsieh, H.F.; Shannon, S.E. Three approaches to qualitative content analysis. Qual. Health Res. 2005, 15, 1277–1288. [Google Scholar] [CrossRef] [PubMed]
- Pebley, K.; Krukowski, R.A.; Porter, K.; Little, M.A. Descriptive and injunctive norms related to e-cigarettes. Mil. Med. 2020, 185, e1919–e1922. [Google Scholar] [CrossRef]
- Secretary of the Air Force Tobacco Free Living (AFI 48-104). 2019. Available online: https://static.e-publishing.af.mil/production/1/af_sg/publication/afi48-104/afi48-104.pdf (accessed on 30 April 2022).
- Delaney, H.; MacGregor, A.; Amos, A. “Tell them you smoke, you’ll get more breaks”: A qualitative study of occupational and social contexts of young adult smoking in Scotland. BMJ Open 2018, 8, e023951. [Google Scholar] [CrossRef] [Green Version]
- McKee, S.A.; Sinha, R.; Weinberger, A.H.; Sofuoglu, M.; Harrison, E.L.; Lavery, M.; Wanzer, J. Stress decreases the ability to resist smoking and potentiates smoking intensity and reward. J. Psychopharmacol. 2011, 25, 490–502. [Google Scholar] [CrossRef] [Green Version]
- Cambron, C.; Hopkins, P.; Burningham, C.; Lam, C.; Cinciripini, P.; Wetter, D.W. Socioeconomic status, mindfulness, and momentary associations between stress and smoking lapse during a quit attempt. Drug Alcohol Depend. 2020, 209, 107840. [Google Scholar] [CrossRef]
- Department of Defense. Department of Defense Announces Fiscal Year 2018 Recruiting and Retention Numbers—End of Year Report. 18 November 2018. Available online: https://www.defense.gov/News/Releases/Release/Article/1691314/department-of-defense-announces-fiscal-year-2018-recruiting-and-retention-numbe/ (accessed on 7 July 2022).
- Segal, D.; Segal, M. America’s Military Population. Popul. Bull. 2004, 59, 8–9. [Google Scholar]
- Dall, T.M.; Zhang, Y.; Chen, Y.J.; Wagner, R.C.A.; Hogan, P.F.; Fagan, N.K.; Olaiya, S.T.; Tornberg, D.N. Cost associated with being overweight and with obesity, high alcohol consumption, and tobacco use within the military health system’s TRICARE prime-enrolled population. Am. J. Health Promot. 2007, 22, 120–139. [Google Scholar] [CrossRef] [PubMed]
- U.S. Government Accountability Office. GAO-19-438R, Transitioning Servicemembers: Information on Military Employment Assistance Centers; U.S. Government Accountability Office: Washington, DC, USA, 2019.
- Krukowski, R.A.; Porter, K.; Boothe, T.; Talcott, G.W.; Little, M.A. “Nobody views it as a negative thing to smoke”: A qualitative study of the relationship between United States Air Force culture and tobacco use. Mil. Psychol. 2021, 33, 409–416. [Google Scholar] [CrossRef] [PubMed]
- Farrelly, M.C.; Nonnemaker, J.; Davis, K.C.; Hussin, A. The influence of the national truth campaign on smoking initiation. Am. J. Prev. Med. 2009, 36, 379–384. [Google Scholar] [CrossRef] [PubMed]
- Bray, R.M.; Rae Olmsted, K.L.; Williams, J.; Sanchez, R.P.; Hartzell, M. Progress toward healthy people 2000 objectives among U.S. military personnel. Prev. Med. 2006, 42, 390–396. [Google Scholar] [CrossRef]


{kind=link}
| Career Field Category | Description | Example Career Fields |
|---|---|---|
| Outdoor/Hands-on Jobs | Career fields in which Airmen work in hands-on careers that often provide them direct and frequent access to outdoor spaces. | Careers on the flight line Careers in maintenance Civil engineering |
| Indoor/Desk Jobs | Career fields that require Airmen to work indoors, often at specific workstations. | Intel Air Traffic Control |
| Medical | Career fields in which Airmen work in medical facilities. While most Airmen in this career field category have direct patient care, some do not as they maintain the medical and facility equipment. | Clinicians Medical Technicians Technicians who maintain medical and healthcare setting system equipment |
| Security Forces | Career fields in which Airmen are often outside on base patrol or guard duty. | Police Special Forces |
| Perception | Exemplar Quote |
|---|---|
| Tobacco use is part of Air Force and military culture |
|
| Tobacco use is not the same across career fields |
|
| Tobacco use rates may be higher in career fields that work outdoors and/or engage in hands-on tasks than those than are more “desk” or indoor oriented |
|
| Career Category | Exemplar Quotes |
|---|---|
| Outdoor/Hands-On Jobs |
|
| Indoor/Desk Jobs |
|
| Medical |
|
| Security Forces |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Horn, T.L.; Porter, K.J.; Pebley, K.N.; Krukowski, R.A.; Little, M.A. “It Depends on Where You Are and What Job You Do”: Differences in Tobacco Use across Career Fields in the United States Air Force. Int. J. Environ. Res. Public Health 2022, 19, 8598. https://doi.org/10.3390/ijerph19148598
Horn TL, Porter KJ, Pebley KN, Krukowski RA, Little MA. “It Depends on Where You Are and What Job You Do”: Differences in Tobacco Use across Career Fields in the United States Air Force. International Journal of Environmental Research and Public Health. 2022; 19(14):8598. https://doi.org/10.3390/ijerph19148598
Chicago/Turabian StyleHorn, Tori L., Kathleen J. Porter, Kinsey N. Pebley, Rebecca A. Krukowski, and Melissa A. Little. 2022. "“It Depends on Where You Are and What Job You Do”: Differences in Tobacco Use across Career Fields in the United States Air Force" International Journal of Environmental Research and Public Health 19, no. 14: 8598. https://doi.org/10.3390/ijerph19148598