
Purpose in Life in Older Adults: A Systematic Review on Conceptualization, Measures, and Determinants


Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility
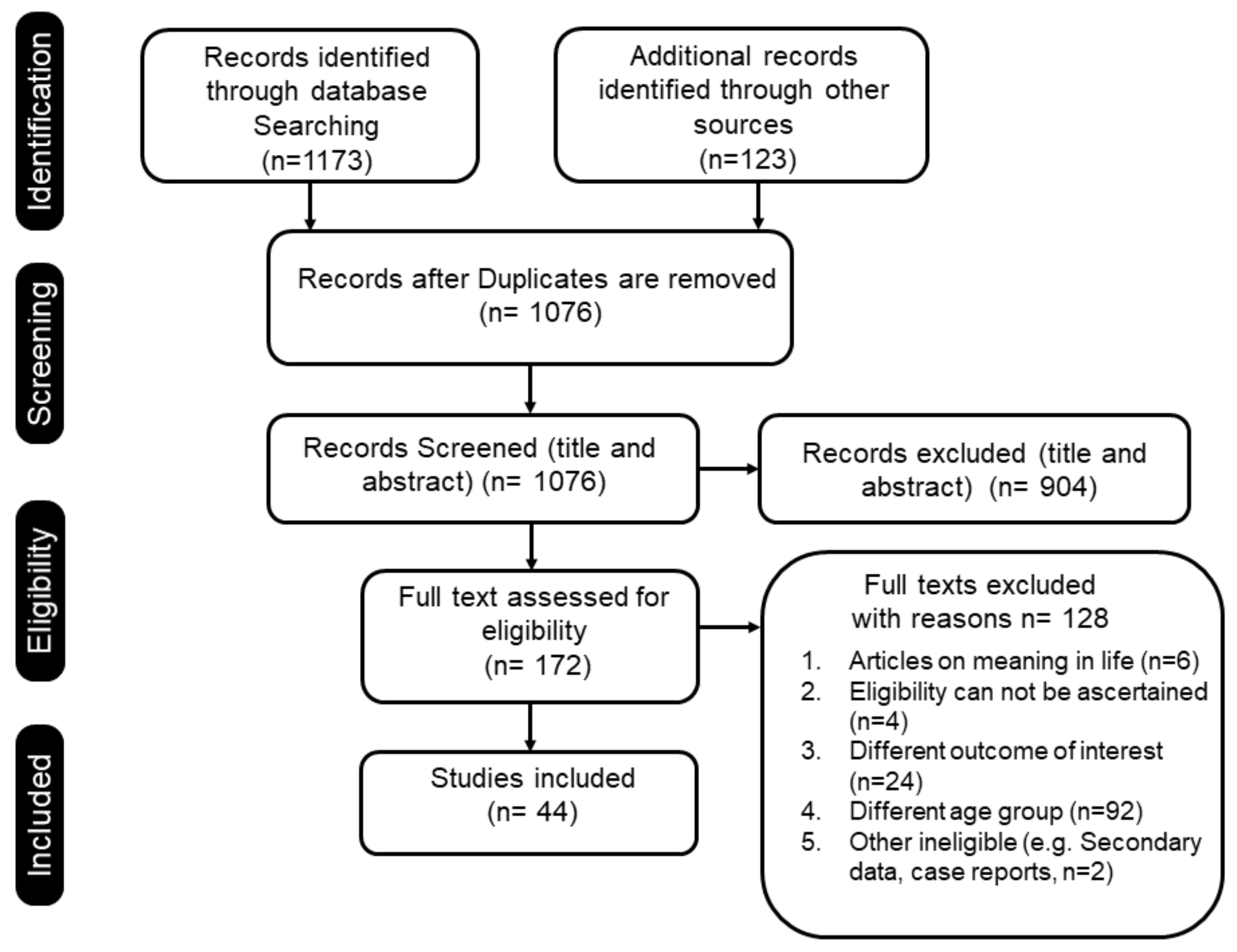
2.2. Information Source and Study Selection
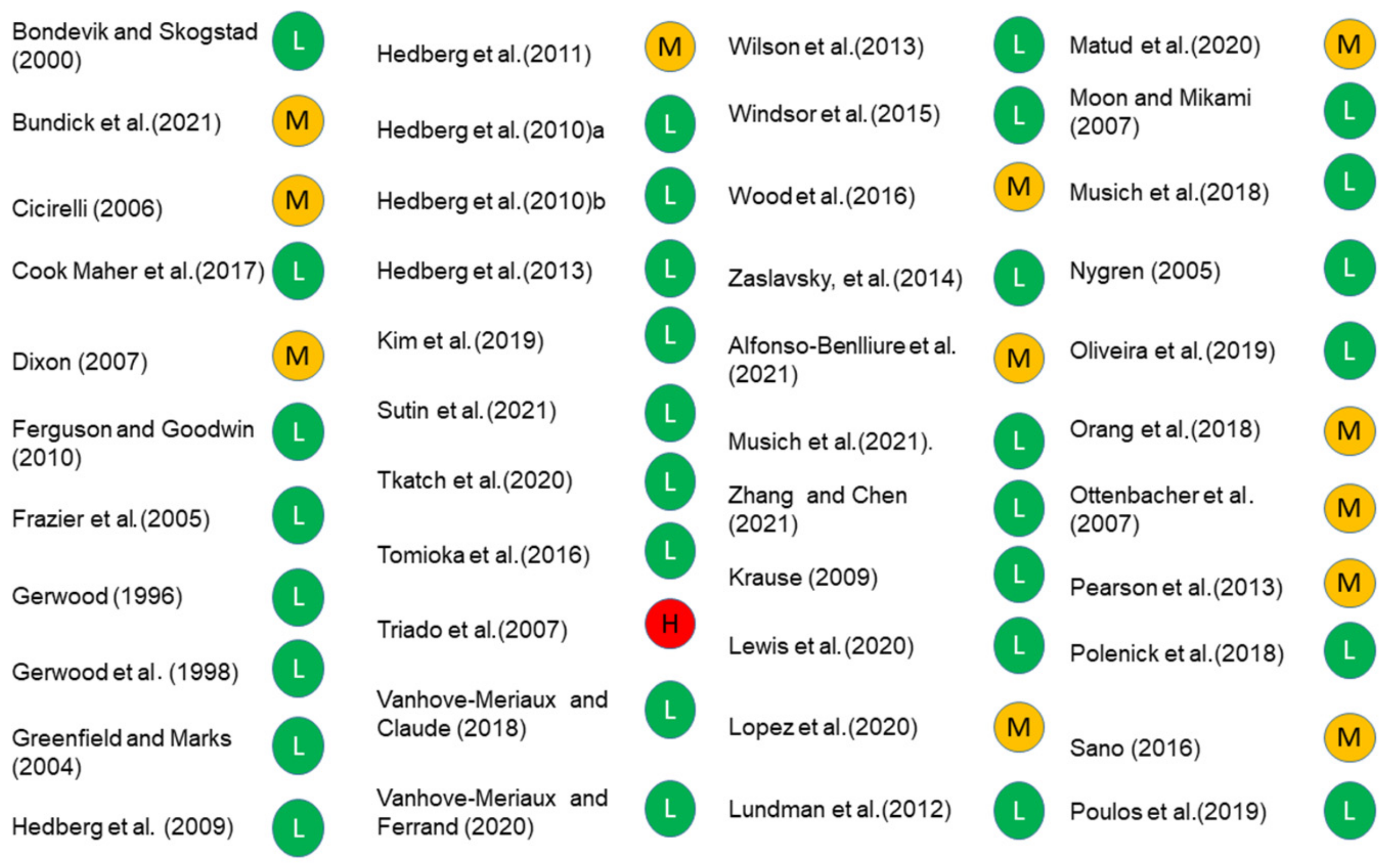
2.3. Risk of Bias (Rob) and Quality Assessments
2.4. Data Extraction and Synthesis
3. Results
3.1. Study Characteristics
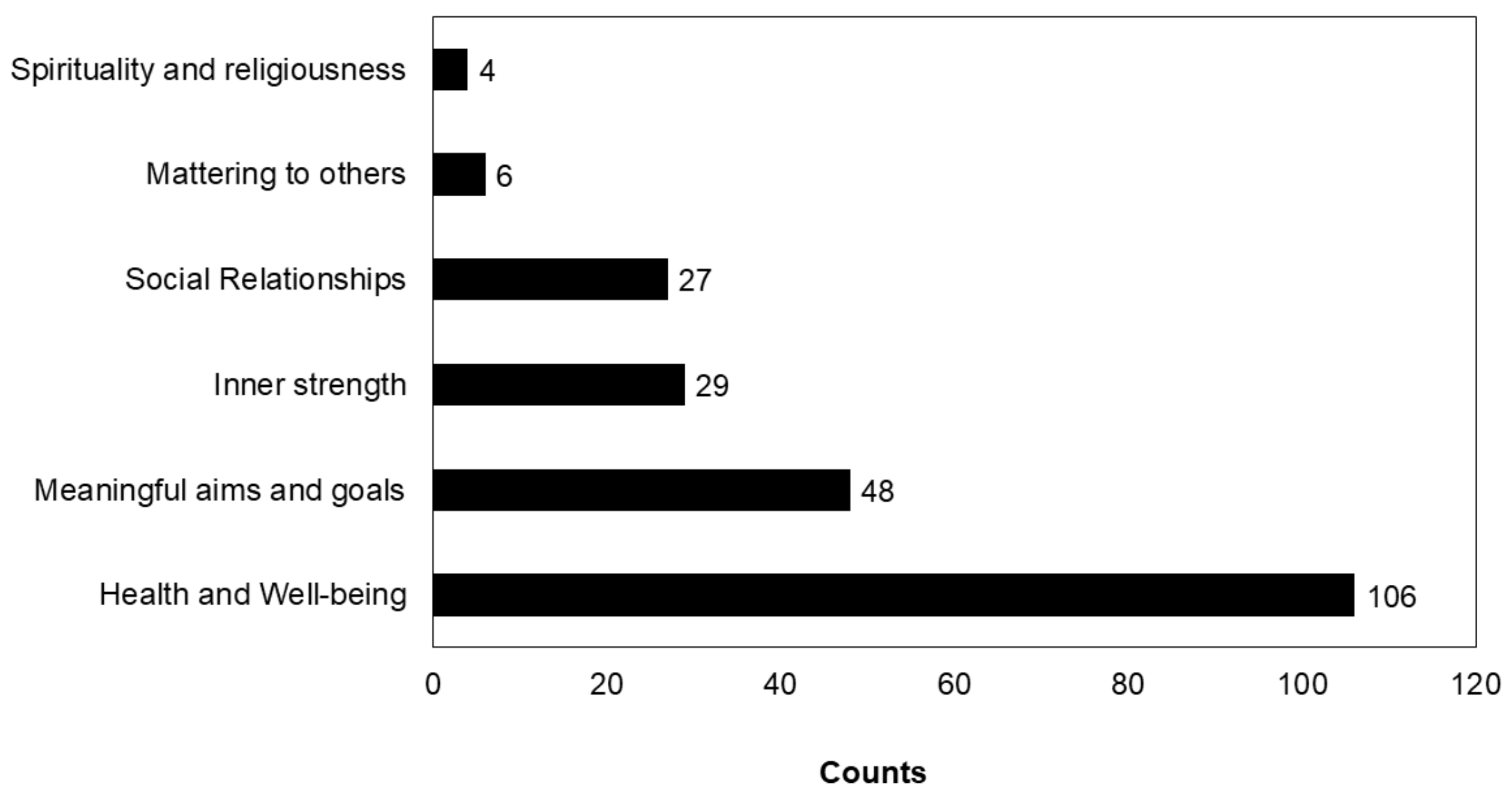
3.2. Conceptualization of PIL
3.3. Measures of PIL
3.3.1. Ryff’s Psychological Well-Being Scale (Ryff’s PWB Scale)
3.3.2. Purpose in Life Test (PIL Test)
3.3.3. NIH Tuberculosis Meaning and Purpose Scale Age 18+
3.3.4. Life Engagement Test (LET)
3.3.5. K-1 Scale
3.4. Determinants of PIL in Older Adults
3.4.1. Sociodemographic Determinants
3.4.2. Other Determinants
3.5. Summary of Evidence
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Yuen, M.; Lee, Q.A.Y.; Kam, J.; Lau, P.S.Y. Purpose in Life: A Brief Review of the Literature and Its Implications for School Guidance Programs. Psychol. Couns. Sch. 2017, 27, 55–69. [Google Scholar] [CrossRef] [Green Version]
- Frankl, V.E. Search for Meaning; Mount Mary College: Milwaukee, WI, USA, 1984; Available online: https://asmre.org/rfl/Ch04-TheSearchForMeaning.pdf (accessed on 3 April 2022).
- Frankl, V.E. Man’s Search for Meaning; Beacon Press: Boston, MA, USA, 2014; Available online: https://books.google.com.sg/books?id=EbltAAAAQBAJ&printsec=frontcover&dq=3.%09Frankl,+V.E.+Man%E2%80%99s+Search+for+Meaning;+Beacon+Press:+Boston,+MA,+USA,+2014.&hl=en&sa=X&ved=2ahUKEwi56Yu649H3AhWd7XMBHblCB1MQ6AF6BAgJEAI#v=onepage&q&f=false (accessed on 3 April 2022).
- Baumeister, R.F. Meanings of Life; Guilford Press: New York, NY, USA, 1991. [Google Scholar]
- Steger, M.F. Meaning in life. In Oxford Handbook of Positive Psychology, 2nd ed.; Snyder, C.R., Lopez, S.J., Eds.; Oxford University Press: New York, NY, USA, 2009; pp. 679–687. [Google Scholar]
- Steger, M.F. Experiencing meaning in life: Optimal functioning at the nexus of well-being, psychopathology, and spirituality. In The Human Quest for Meaning: Theories, Research, and Applications, 2nd ed.; Wong, P.T., Ed.; Routledge: New York, NY, USA, 2012; pp. 165–184. [Google Scholar]
- Reker, G.T.; Wong, P.T.P. Aging as an individual process: Toward a theory of personal meaning. In Emergent Theories of Aging; Birren, J.E., Bengtson, V.L., Eds.; Springer Pub. Co.: New York, NY, USA, 1988; pp. 214–246. [Google Scholar]
- Costin, V.; Vivian, L.V. Meaning is about mattering: Evaluating coherence, purpose, and existential mattering as precursors of meaning in life judgments. J. Personal. Soc. Psychol. 2020, 118, 864. [Google Scholar] [CrossRef] [PubMed]
- George, L.S.; Park, C.L. Are meaning and purpose distinct? An examination of correlates and predictors. J. Posit. Psychol. 2013, 8, 365–375. [Google Scholar] [CrossRef]
- Damon, W.; Menon, J.; Bronk, K.C. The development of purpose during adolescence. In Beyond the Self; Routledge: New York, NY, USA, 2019; pp. 119–128. Available online: https://www.taylorfrancis.com/chapters/edit/10.4324/9780203764688-2/development-purpose-adolescence-william-damon-jenni-menon-kendall-cotton-bronk (accessed on 20 November 2021).
- McKnight, P.E.; Kashdan, T.B. Purpose in Life as a System that Creates and Sustains Health and Well-Being: An Integrative, Testable Theory. Rev. Gen. Psychol. 2009, 13, 242–251. [Google Scholar] [CrossRef]
- Smith, B.W.; Zautra, A.J. The role of purpose in life in recovery from knee surgery. Int. J. Behav. Med. 2004, 11, 197–202. [Google Scholar] [CrossRef]
- Cohen, R.; Bavishi, C.; Rozanski, A. Purpose in Life and Its Relationship to All-Cause Mortality and Cardiovascular Events: A Meta-Analysis. Psychosom. Med. 2016, 78, 122–133. [Google Scholar] [CrossRef] [PubMed]
- Zilioli, S.; Slatcher, R.B.; Ong, A.D.; Gruenewald, T.L. Purpose in life predicts allostatic load ten years later. J. Psychosom. Res. 2015, 79, 451–457. [Google Scholar] [CrossRef] [Green Version]
- Harlow, L.L.; Newcomb, M.D.; Bentler, P.M. Depression, self-derogation, substance use, and suicide ideation: Lack of purpose in life as a mediational factor. J. Clin. Psychol. 1986, 42, 5–21. [Google Scholar] [CrossRef]
- Heisel, M.J.; Flett, G.L. Purpose in Life, Satisfaction with Life, and Suicide Ideation in a Clinical Sample. J. Psychopathol. Behav. Assess. 2004, 26, 127–135. [Google Scholar] [CrossRef]
- Aghababaei, N.; Błachnio, A. Purpose in life mediates the relationship between religiosity and happiness: Evidence from Poland. Ment. Health Relig. Cult. 2014, 17, 827–831. [Google Scholar] [CrossRef]
- Larissa, R. The Search for Purpose in Life: An Exploration of Purpose, the Search Process, and Purpose Anxiety; University of Pennsylvania: Philadelphia, PA, USA, 2014; Available online: https://repository.upenn.edu/mapp_capstone/60 (accessed on 15 September 2021).
- Pinquart, M. Creating and maintaining purpose in life in old age: A meta-analysis. Ageing Int. 2002, 27, 90–114. [Google Scholar] [CrossRef]
- Yemiscigil, A.; Powdthavee, N.; Whillans, A.V. The Effects of Retirement on Sense of Purpose in Life: Crisis or Opportunity? Psychol. Sci. 2021, 32, 1856–1864. [Google Scholar] [CrossRef] [PubMed]
- Shin, S.H.; Behrens, E.A.; Parmelee, P.A.; Kim, G. The Role of Purpose in Life in the Relationship between Widowhood and Cognitive Decline among Older Adults in the U.S. Am. J. Geriatr. Psychiatry 2022, 30, 383–391. [Google Scholar] [CrossRef] [PubMed]
- Kim, G.; Shin, S.H.; Scicolone, M.; Parmelee, P.A. Purpose in life protects against cognitive decline among older adults. Innov. Aging 2019, 3, S650–S651. [Google Scholar] [CrossRef]
- Boyle, P.A.; Buchman, A.S.; Barnes, L.L.; Bennett, D.A. Effect of a Purpose in Life on Risk of Incident Alzheimer Disease and Mild Cognitive Impairment in Community-Dwelling Older Persons. Arch. Gen. Psychiatry 2010, 67, 304. [Google Scholar] [CrossRef] [Green Version]
- Mota, N.P.; Tsai, J.; Kirwin, P.D.; Sareen, J.; Southwick, S.M.; Pietrzak, R.H. Purpose in Life is Associated with a Reduced Risk of Incident Physical Disability in Aging U.S. Military Veterans. Am. J. Geriatr. Psychiatry 2016, 24, 706–714. [Google Scholar] [CrossRef]
- Kim, E.S.; Sun, J.K.; Park, N.; Kubzansky, L.D.; Peterson, C. Purpose in life and reduced risk of myocardial infarction among older U.S. adults with coronary heart disease: A two-year follow-up. J. Behav. Med. 2013, 36, 124–133. [Google Scholar] [CrossRef]
- Zaslavsky, O.; Rillamas-Sun, E.; Woods, N.F.; Cochrane, B.B.; Stefanick, M.L.; Tindle, H.; Tinker, L.F.; LaCroix, A.Z. Association of the selected dimensions of eudaimonic well-being with healthy survival to 85 years of age in older women. Int. Psychogeriatr. 2014, 26, 2081–2091. [Google Scholar] [CrossRef] [Green Version]
- Scheier, M.F.; Wrosch, C.; Baum, A.; Cohen, S.; Martire, L.M.; Matthews, K.A.; Schulz, R.; Zdaniuk, B. The Life Engagement Test: Assessing Purpose in Life. J. Behav. Med. 2006, 29, 291–298. [Google Scholar] [CrossRef]
- Hill, P.L.; Edmonds, G.W.; Hampson, S.E. A purposeful lifestyle is a healthful lifestyle: Linking sense of purpose to self-rated health through multiple health behaviors. J. Health Psychol. 2019, 24, 1392–1400. [Google Scholar] [CrossRef]
- Czekierda, K.; Banik, A.; Park, C.L.; Luszczynska, A. Meaning in life and physical health: Systematic review and meta-analysis. Health Psychol. Rev. 2017, 11, 387–418. [Google Scholar] [CrossRef] [PubMed]
- Brandstätter, M.; Baumann, U.; Borasio, G.D.; Fegg, M.J. Systematic review of meaning in life assessment instruments. Psycho-Oncology 2012, 21, 1034–1052. [Google Scholar] [CrossRef] [PubMed]
- Irving, J.; Davis, S.; Collier, A. Aging with Purpose: Systematic Search and Review of Literature Pertaining to Older Adults and Purpose. Int. J. Aging Hum. Dev. 2017, 85, 403–437. [Google Scholar] [CrossRef]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B. Meta-analysis of observational studies in epidemiology: A proposal for reporting. Meta-analysis of Observational Studies in Epidemiology (MOOSE) group. JAMA-J. Am. Med. Assoc. 2000, 283, 2008–2012. [Google Scholar] [CrossRef]
- Stern, C.; Lizarondo, L.; Carrier, J.; Godfrey, C.; Rieger, K.; Salmond, S.; Apostolo, J.; Kirkpatrick, P.; Loveday, H. Methodological guidance for the conduct of mixed methods systematic reviews. JBI Evid. Implement. 2021, 19, 120–129. [Google Scholar] [CrossRef]
- World Health Organization. Ageing and Life Course Unit. Men, Ageing, and Health: Achieving Health across the Life Span. 2001. Available online: https://apps.who.int/iris/handle/10665/66941 (accessed on 17 November 2021).
- Goplen, C.M.; Verbeek, W.; Kang, S.H.; Jones, C.A.; Voaklander, D.C.; Churchill, T.A.; Beaupre, L.A. Preoperative opioid use is associated with worse patient outcomes after Total joint arthroplasty: A systematic review and meta-analysis. BMC Musculoskelet. Disord. 2019, 20, 234. [Google Scholar] [CrossRef] [PubMed]
- Hartling, L.; Fernandes, R.M.; Seida, J.; Vandermeer, B.; Dryden, D.M. From the trenches: A cross-sectional study applying the GRADE tool in systematic reviews of healthcare interventions. PLoS ONE 2012, 7, e34697. [Google Scholar] [CrossRef] [Green Version]
- AshaRani, P.V.; Hombali, A.; Seow, E.; Ong, W.J.; Tan, J.H.; Subramaniam, M. Non-pharmacological interventions for methamphetamine use disorder: A systematic review. Drug Alcohol Depend. 2020, 212, 108060. [Google Scholar] [CrossRef]
- Rajabzadeh, V.; Burn, E.; Sajun, S.Z.; Suzuki, M.; Bird, V.J.; Priebe, S. Understanding global mental health: A conceptual review. BMJ Glob. Health 2021, 6, e004631. [Google Scholar] [CrossRef]
- Gerwood, J.B. The Purpose-in-Life Test: A Comparison in Elderly People by Relational Status, Work, Spirituality, and Mood; The University of Toledo: Toledo, OH, USA, 1996; Volume 57, p. 0100. [Google Scholar]
- Gerwood, J.B.; LeBlanc, M.; Piazza, N. The purpose-in-life test and religious denomination: Protestant and Catholic scores in an elderly population. J. Clin. Psychol. 1998, 54, 49–53. [Google Scholar] [CrossRef]
- Bondevik, M.; Skogstad, A. Loneliness, Religiousness, and Purpose in Life in the Oldest Old. 2000. Available online: https://books.google.com/books/about/Loneliness_religiousness_and_purpose_in.html?hl=&id=YnudngEACAAJ (accessed on 16 September 2021).
- Greenfield, E.A.; Marks, N.F. Formal volunteering as a protective factor for older adults’ psychological well-being. J. Gerontol. B Psychol. Sci. Soc. Sci. 2004, 59, S258–S264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frazier, C.; Mintz, L.B.; Mobley, M. A Multidimensional Look at Religious Involvement and Psychological Well-Being among Urban Elderly African Americans. J. Consult. Psychol. 2005, 52, 583–590. [Google Scholar] [CrossRef]
- Nygren, B.; Aléx, L.; Jonsén, E.; Gustafson, Y.; Norberg, A.; Lundman, B. Resilience, sense of coherence, purpose in life and self-transcendence in relation to perceived physical and mental health among the oldest old. Aging Ment. Health 2005, 9, 354–362. [Google Scholar] [CrossRef] [PubMed]
- Cicirelli, V.G. Fear of death in mid-old age. J. Gerontol. B Psychol. Sci. Soc. Sci. 2006, 61, P75–P81. [Google Scholar] [CrossRef] [Green Version]
- Dixon, A.L. Mattering in the Later Years: Older Adults’ Experiences of Mattering to Others, Purpose in Life, Depression, and Wellness. Adultspan J. 2007, 6, 83–95. [Google Scholar] [CrossRef]
- Triadó, C.; Villar, F.; Solé, C.; Celdrán, M. Construct Validity of Ryff’s Scale of Psychological Well-Being in Spanish Older Adults. Psychol. Rep. 2007, 100, S1151–S1164. [Google Scholar] [CrossRef]
- Moon, J.-S.; Mikami, H. Difference in subjective well-being between ethnic Korean and Japanese elderly residents in an urban community in Japan. Geriatr. Gerontol. Int. 2007, 7, 371–379. [Google Scholar] [CrossRef]
- Ottenbacher, M.E.; Kuo, Y.-F.; Ostir, G.V. Test-retest reliability of a psychological well-being scale in hospitalized older adults. Aging Clin. Exp. Res. 2007, 19, 424–429. [Google Scholar] [CrossRef] [Green Version]
- Hedberg, P.; Brulin, C.; Aléx, L. Experiences of purpose in life when becoming and being a very old woman. J. Women Aging 2009, 21, 125–137. [Google Scholar] [CrossRef]
- Krause, N. Meaning in Life and Mortality. J. Gerontol. B Psychol. Sci. Soc. Sci. 2009, 64B, 517–527. [Google Scholar] [CrossRef]
- Ferguson, S.J.; Goodwin, A.D. Optimism and well-being in older adults: The mediating role of social support and perceived control. Int. J. Aging Hum. Dev. 2010, 71, 43–68. [Google Scholar] [CrossRef] [PubMed]
- Hedberg, P.; Gustafson, Y.; Aléx, L.; Brulin, C. Depression in relation to purpose in life among a very old population: A five-year follow-up study. Aging Ment. Health 2010, 14, 757–763. [Google Scholar] [CrossRef] [PubMed]
- Hedberg, P.; Gustafson, Y.; Brulin, C. Purpose in life among men and women aged 85 years and older. Int. J. Aging Hum. Dev. 2010, 70, 213–229. [Google Scholar] [CrossRef] [PubMed]
- Hedberg, P.; Brulin, C.; Aléx, L.; Gustafson, Y. Purpose in life over a five-year period: A longitudinal study in a very old population. Int. Psychogeriatr. 2011, 23, 806–813. [Google Scholar] [CrossRef]
- Lundman, B.; Aléx, L.; Jonsén, E.; Lövheim, H.; Nygren, B.; Santamäki Fischer, R.; Strandberg, G.; Norberg, A. Inner strength in relation to functional status, disease, living arrangements, and social relationships among people aged 85 years and older. Geriatr. Nurs. 2012, 33, 167–176. [Google Scholar] [CrossRef]
- Hedberg, P.; Gustafson, Y.; Brulin, C.; Aléx, L. Purpose in life among very old men. Adv. Aging Res. 2013, 2, 100–105. [Google Scholar] [CrossRef] [Green Version]
- Wilson, R.S.; Boyle, P.A.; Segawa, E.; Yu, L.; Begeny, C.T.; Anagnos, S.E.; Bennett, D.A. The influence of cognitive decline on well-being in old age. Psychol. Aging 2013, 28, 304–313. [Google Scholar] [CrossRef] [Green Version]
- Pearson, E.L.; Windsor, T.D.; Crisp, D.A.; Butterworth, P.; Pilkington, P.D.; Anstey, K.J. Normative data and longitudinal invariance of the Life Engagement Test (LET) in a community sample of older adults. Qual. Life Res. 2013, 22, 327–331. [Google Scholar] [CrossRef]
- Windsor, T.D.; Curtis, R.G.; Luszcz, M.A. Sense of purpose as a psychological resource for aging well. Dev. Psychol. 2015, 51, 975–986. [Google Scholar] [CrossRef]
- Tomioka, K.; Kurumatani, N.; Hosoi, H. Relationship of Having Hobbies and a Purpose in Life with Mortality, Activities of Daily Living, and Instrumental Activities of Daily Living among Community-Dwelling Elderly Adults. J. Epidemiol. 2016, 26, 361–370. [Google Scholar] [CrossRef] [Green Version]
- Woods, N.F.; Rillamas-Sun, E.; Cochrane, B.B.; La Croix, A.Z.; Seeman, T.E.; Tindle, H.A.; Zaslavsky, O.; Bird, C.E.; Johnson, K.C.; Manson, J.E.; et al. Aging Well: Observations from the Women’s Health Initiative Study. J. Gerontol. A Biol. Sci. Med. Sci. 2016, 71, S3–S12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sano, N.; Kyougoku, M. An analysis of structural relationship among achievement motive on social participation, purpose in life, and role expectations among community dwelling elderly attending day services. PeerJ 2016, 4, e1655. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cook Maher, A.; Kielb, S.; Loyer, E.; Connelley, M.; Rademaker, A.; Mesulam, M.M.; Weintraub, S.; McAdams, D.; Logan, R.; Rogalski, E. Psychological well-being in elderly adults with extraordinary episodic memory. PLoS ONE 2017, 12, e0186413. [Google Scholar] [CrossRef] [PubMed]
- Vanhove-Meriaux, C.; Martinent, G.; Ferrand, C. Profiles of needs satisfaction and thwarting in older people living at home: Relationships with well-being and ill-being indicators. Geriatr. Gerontol. Int. 2018, 18, 470–478. [Google Scholar] [CrossRef] [PubMed]
- Musich, S.; Wang, S.S.; Kraemer, S.; Hawkins, K.; Wicker, E. Purpose in Life and Positive Health Outcomes among Older Adults. Popul. Health Manag. 2018, 21, 139–147. [Google Scholar] [CrossRef]
- Orang, S.R.; Ramshini, H.H.; Ramshini, M.; Orang, T. Investigating the Meaning of Life and Psychological Well-being, in Youth, Adults, and Elderly (A Comparative Study of Three Age Groups). Salmand-Iran. J. Ageing 2018, 13, 182–197. [Google Scholar] [CrossRef]
- Polenick, C.A.; Kales, H.C.; Birditt, K.S. Perceptions of Purpose in Life within Spousal Care Dyads: Associations with Emotional and Physical Caregiving Difficulties. Ann. Behav. Med. 2018, 52, 77–87. [Google Scholar] [CrossRef]
- De Oliveira, D.V.; de Oliveira, D.V.; Ribeiro, C.C.; Pico, R.E.R.; Murari, M.O.; Freire, G.L.M.; Contreira, A.R.; do Nascimento Júnior, J.R.A. Is life satisfaction associated with the purpose in life of elderly hydrogymnastics practitioners? Motriz Rev. Educ. Fis. 2019, 25, 1–7. [Google Scholar] [CrossRef]
- Poulos, R.G.; Marwood, S.; Harkin, D.; Opher, S.; Clift, S.; Cole, A.M.D.; Rhee, J.; Beilharz, K.; Poulos, C.J. Arts on prescription for community-dwelling older people with a range of health and wellness needs. Health Soc. Care Community 2019, 27, 483–492. [Google Scholar] [CrossRef] [Green Version]
- Sutin, A.R.; Luchetti, M.; Stephan, Y.; Terracciano, A. Purpose in Life and Motoric Cognitive Risk Syndrome: Replicable Evidence from Two National Samples. J. Am. Geriatr. Soc. 2021, 69, 381–388. [Google Scholar] [CrossRef]
- Tkatch, R.; Wu, L.; MacLeod, S.; Ungar, R.; Albright, L.; Russell, D.; Murphy, J.; Schaeffer, J.; Yeh, C.S. Reducing loneliness and improving well-being among older adults with animatronic pets. Aging Ment. Health 2021, 25, 1239–1245. [Google Scholar] [CrossRef] [PubMed]
- Vanhove-Meriaux, C.; Martinent, G.; Ferrand, C. Adaptation and Validation of the French Psychological Need Frustration Scale for Older Adults. Ageing Int. 2020, 45, 99–117. [Google Scholar] [CrossRef]
- Lewis, N.A.; Reesor, N.; Hill, P.L. Perceived barriers and contributors to sense of purpose in life in retirement community residents. Ageing Soc. 2020, 1–17. [Google Scholar] [CrossRef]
- López, J.; Perez-Rojo, G.; Noriega, C.; Carretero, I.; Velasco, C.; Martinez-Huertas, J.A.; López-Frutos, P.; Galarraga, L. Psychological well-being among older adults during the COVID-19 outbreak: A comparative study of the young–old and the old–old adults. Int. Psychogeriatr. 2020, 32, 1365–1370. [Google Scholar] [CrossRef] [PubMed]
- Matud, M.P.; Bethencourth, J.M.; Ibanez, I.; Fortes, D. Gender and psychological well-being in older adults. Int. Psychogeriatr. 2020, 32, 1293–1302. [Google Scholar] [CrossRef] [PubMed]
- Bundick, M.J.; Remington, K.; Morton, E.; Colby, A. The contours of purpose beyond the self in midlife and later life. Appl. Dev. Sci. 2021, 25, 62–82. [Google Scholar] [CrossRef]
- Alfonso-Benlliure, V.; Mayordomo, T.; Sales, A.; Mélendez, J.C. Divergent Thinking in Older Adults: Understanding its Role in Well-being. J. Happiness Stud. 2021, 22, 3285–3298. [Google Scholar] [CrossRef]
- Musich, S.; Wang, S.H.S.; Schaeffer, J.A.; Kraemer, S.; Wicker, E.; Yeh, C.S. The additive impact of multiple psychosocial protective factors on selected health outcomes among older adults. Geriatr. Nurs. 2021, 42, 502–508. [Google Scholar] [CrossRef]
- Zhang, Z.; Chen, W. Longitudinal Associations between Physical Activity and Purpose in Life among Older Adults: A Cross-Lagged Panel Analysis. J. Aging Health 2021, 33, 941–952. [Google Scholar] [CrossRef]
- Crumbaugh, J.C.; Maholick, L.T. An experimental study in existentialism: The psychometric approach to frankl’s concept of noogenic neurosis. J. Clin. Psychol. 1964, 20, 200–207. [Google Scholar] [CrossRef]
- Ryff, C.D. Psychological Well-Being Scale. In PsycTESTS Dataset; American Psychological Association: Washington, DC, USA, 2012. [Google Scholar] [CrossRef]
- Abbott, R.A.; Ploubidis, G.B.; Huppert, F.A.; Kuh, D.; Wadsworth, M.E.J.; Croudace, T.J. Psychometric evaluation and predictive validity of Ryff’s psychological well-being items in a UK birth cohort sample of women. Health Qual. Life Outcomes 2006, 4, 76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crumbaugh, J.C.; Maholick, L.T. Purpose in Life Test. In PsycTESTS Dataset; American Psychological Association: Washington, DC, USA, 2011. [Google Scholar] [CrossRef]
- Davies, G.; Klaassen, D.; Längle, A. Purpose in Life Test. In Encyclopedia of Quality of Life and Well-Being Research; Springer: Dordrecht, The Netherlands, 2014; pp. 5238–5243. [Google Scholar] [CrossRef]
- Reker, G.T.; Fry, P.S. Factor structure and invariance of personal meaning measures in cohorts of younger and older adults. Personal. Individ. Differ. 2003, 35, 977–993. [Google Scholar] [CrossRef]
- Salsman, J.M.; Lai, J.-S.; Hendrie, H.C.; Butt, Z.; Zill, N.; Pilkonis, P.A.; Peterson, C.; Stoney, C.M.; Brouwers, P.; Cella, D. Assessing psychological well-being: Self-report instruments for the NIH Toolbox. Qual. Life Res. 2014, 23, 205–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ryff, C.D.; Keyes, C.L.M. The structure of psychological well-being revisited. J. Personal. Soc. Psychol. 1995, 69, 719–727. [Google Scholar] [CrossRef]
- Fisher, C.D. Conceptualizing and Measuring Wellbeing at Work. Wellbeing 2014, 3, 1–25. [Google Scholar] [CrossRef]
- Krok, D. The Role of Meaning in Life within the Relations of Religious Coping and Psychological Well-Being. J. Relig. Health 2015, 54, 2292–2308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Damon, W.; Menon, J.; Bronk, K.C. The Development of Purpose during Adolescence. Appl. Dev. Sci. 2003, 7, 119–128. [Google Scholar] [CrossRef]
- Moran, S.; Bundick, M.J.; Malin, H.; Reilly, T.S. How supportive of their specific purposes do youth believe their family and friends are? J. Adolesc. Res. 2013, 28, 348–377. [Google Scholar] [CrossRef]
- Wang, Z.; Koenig, H.G.; Ma, H.; Shohaib, S.A. Religion, Purpose in Life, Social Support, and Psychological Distress in Chinese University Students. J. Relig. Health 2016, 55, 1055–1064. [Google Scholar] [CrossRef]
- Ryff, C.D. Happiness is everything, or is it? Explorations on the meaning of psychological well-being. J. Personal. Soc. Psychol. 1989, 57, 1069–1081. [Google Scholar] [CrossRef]
- Frankl, V.E. The Will to Meaning: Foundations and Applications of Logotherapy. Plume. 2014. Available online: https://books.google.com/books/about/The_Will_to_Meaning.html?hl=&id=6xQpngEACAAJ (accessed on 17 November 2021).
- García-Alandete, J. Does Meaning in Life Predict Psychological Well-Being?: An Analysis Using the Spanish Versions of the Purpose-In-Life Test and the Ryff’s Scales. Eur. J. Psychother. Couns. 2015, 3, 89–98. [Google Scholar] [CrossRef]
- Tang, F.; Morrow-Howell, N. Involvement in voluntary organizations: How older adults access volunteer roles? J. Gerontol. Soc. Work 2008, 51, 210–227. [Google Scholar] [CrossRef] [PubMed]
- Sheng, L.K. Positive Psychological Attributes and Retirement Satisfaction. CFA Dig. 2015, 45. [Google Scholar] [CrossRef]
- Umberson, D.; Crosnoe, R.; Reczek, C. Social Relationships and Health Behavior across the Life Course. Annu. Rev. Sociol. 2010, 36, 139–157. [Google Scholar] [CrossRef] [Green Version]
- Umberson, D.; Montez, J.K. Social Relationships and Health: A Flashpoint for Health Policy. J. Health Soc. Behav. 2010, 51, S54–S66. [Google Scholar] [CrossRef] [Green Version]
- Lundman, B.; Aléx, L.; Jonsén, E.; Norberg, A.; Nygren, B.; Fischer, R.S.; Strandberg, G. Inner strength—A theoretical analysis of salutogenic concepts. Int. J. Nurs. Stud. 2010, 47, 251–260. [Google Scholar] [CrossRef]
- Nkyi, A.K.; Ninnoni, J.P.K. Depression, Purpose in Life, Loneliness and Anxiety among Patients with Substance Use Disorders in Ankaful Psychiatric Hospital in Ghana. Int. Psychosoc. Rehabil. 2020, 7, 263–271. [Google Scholar] [CrossRef]
- Cotton Bronk, K. Purpose in Life: A Critical Component of Optimal Youth Development; Springer Science Business Media: Berlin/Heidelberg, Germany, 2014. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| No. | Study ID | Country | Setting | Design | Population | Number of Participants | Outcome Measures |
|---|---|---|---|---|---|---|---|
| 1 | Gerwood (1996) [39] | USA | Community, senior citizen centers | Cross sectional | Older adults 65 and above | n = 130 | Demographic questionnaire, CEDS, and the 20-items Purpose in Life scale (by Crumbaugh and Maholick, PIL Test-C). |
| 2 | * Gerwood et al. (1998) [40] | USA | Community, senior citizen centers | Cross sectional | Older adults 65 and above | n = 130 | Demographic questionnaire (for Spirituality) and PIL Test-C (20-items). |
| 3 | Bondevik and Skogstad (2000) [41] | Norway | Community and nursing home | Cross sectional | Older adults: 80 years and above | n = 110 for older adults from community; N = 111 those from nursing homes | Short Form Scale of the Revised UCLA Loneliness Scale; PIL test-C (20-items); A single item to measure religiosity (Would you say that religion means anything to you?) |
| 4 | Greenfield and Marks (2004) [42] | USA | Community | Cross sectional | Older adults 65–74 years | n = 373 | Negative and positive affect scale; Ryff’s PWB Index (3-item); Major role-identity absences questionnaire. |
| 5 | Frazier et al. (2005) [43] | USA | Community: Senior centers, and public service organizations. | Cross sectional | Older adults 65 and above | n = 86 | Multidimensional Measure of Religious Involvement for African Americans; Ryff’s PWB scale (14-item). |
| 6 | Nygren (2005) [44] | Sweden | Community | Cross sectional | Older adults 85 years of age or older | n = 125 n = 26 participants were 95 years or older, n = 46 were 90 years of age, and n = 53 were 85 years of age | The Swedish version of the PIL Scale-C (20-item); The Resilience Scale; SOC Scale: STS; SF-36 Health Survey. |
| 7 | Cicirelli (2006) [45] | USA | Community | Cross sectional | Older adults: young old group (60–74 years) and mid old group (75–84 years) | n = 192; young-old group n = 132 and mid-old group n = 60. | Self-rating of health, 2-items scale for Discrepancy between expected and desired time to live; PIL Scale-C (20-items); MFDS. |
| 8 | Dixon (2007) [46] | USA | Community (retirement community) | Cross sectional | Older adults above 70 years | n = 167 | Interpersonal Mattering Scale; 20-item PIL Test-C; Short version of the Geriatric Depression Rating Scale; Older Adult Wellness Evaluation. |
| 9 | Triado et al. (2007) [47] | Spain | Community, retired individuals | Cross sectional study | Retired persons ages 65 and older | n = 422; n (men) = 200 n (women) = 222 | Spanish version of the Ryff’s PWB Scale (9-items); Spanish version of Life Satisfaction Index; Philadelphia Geriatric Scale. |
| 10 | Moon and Mikami (2007) [48] | Japan | Community | Cross sectional | Older adults 65 years of age or older | n = 425 (n = 204 ethnic Korean residents; n = 221 for Japanese residents) | CGA for Activities of Daily Living, TMIG Index of Competence, short version of GDS-15 in Japanese and Korean visual horizontal analogue scale items to capture “sense of purpose in life”, self-reported medical history, and receipt of public assistance. |
| 11 | Ottenbacher et al. (2007) [49] | USA | Hospitalized inpatient sample (acute cases) | Cross sectional study | Older adults 65 years of age or older | n = 40 | Ryff’s PWB scale (9-items) |
| 12 | Hedberg et al. (2009) [50] | Sweden | Community: town and rural areas | Qualitative | Women aged 85 and above | n = 30 women | PIL Test-C (20-items) for screening and the qualitative interview included various aspects of their lives, such as experiences of aging; difficult and positive life events; and experiences of loneliness, comfort, spirituality, and purpose in life. |
| 13 | Krause (2009) [51] | USA | Community | Cohort study | Older adults above 65 years | n = 1361 | Informant report for mortality status; MIL scale (2-items for PIL); Self-rated health; Acute and chronic health conditions check list; Questions on Functional disability and Frequency of attendance at religious services; Emotional support scale. |
| 14 | Ferguson and Goodwin (2010) [52] | Australia | Community retirement villages, volunteer organizations and community organizations | Cross sectional | Older adults 65 to 94 years | n = 225 | PIL subscale (14-items) of Ryff’s PWB scale; Affect Balance Scales (5-item subscale of Positive Affect scale); Revised Life Orientation Test (Dispositional optimism); The Social Support Questionnaire; Short Form. A scale (perceived control). |
| 15 | Hedberg et al. (2010a) [53] | Sweden | Community: town and rural areas | Longitudinal cohort | Elderly above 85 years | n = 149; women n = 88, men n = 61 | GDS-15; OBS; OBS Scale; MADRS; DSM-IV; PIL Test-C (20-items). |
| 16 | Hedberg et al. (2010b) [54] | Sweden | Community: town and rural areas | Cross sectional | Elderly between 85 to 103 years of age. | n = 189; women n = 120, men n = 69 | PIL Test-C (20-item); PGCM scale; GQL instrument; SF-36 Health survey; Katz Activity of Daily Living Index; sociodemographic questionnaire (social relations). |
| 17 | Hedberg et al. (2011) [55] | Sweden | Community: town and rural areas | Longitudinal study cohorts | Elderly above 85 years | n = 51 (42 women and 9 men) | PIL Test-C (20-item); GDS; The Minimal Nutritional Assessment; The Barthel Index for ADL (for PA), The Mini-Mental State Examination. |
| 18 | Lundman et al. (2012) [56] | Sweden | Community | Cross-sectional | Older adults 85 years and above | n = 185 | The Swedish version of the PIL Scale-C; The Resilience Scale; SOC scale; STS scale; GDS-15; ADL scale; Self-reported measures for Living Arrangements and Social Relationships. |
| 19 | Hedberg et al. (2013) [57] | Sweden | Community: town and rural areas | Qualitative | Men above 85 years | n = 30 | Interviews included questions about various aspects of their experiences of becoming and being very old. |
| 20 | Wilson et al. (2013) [58] | USA | Community (retirement communities, subsidized housing facilities, local churches, and social service agencies) | Cohort study | Older adults aged 65 years or older. | n (initial) = 1049 n (additional analysis) = 560 | Ryff’s PWB scale (10-items; annually); Between 2008 and 2011, 18-item version of Ryff’s PWB Scales administered once to a subgroup; Cognitive tests for annual measures Episodic Semantic, working memory; Perceptual speed and Visuospatial ability; Guidelines of the joint working group of NINDS and SARDA; CESD; Katz disability scale. |
| 21 | Pearson et al. (2013) [59] | Australia | Community | Cohort study | Older adults aged 55 years of age or older | n = 545, 55–64 years n = 300, 65–74 years n = 167, 75 years and older n = 74 | LET (6-items) |
| 22 | Zaslavsky et al. (2014) [26] | USA | Community | Cohort study | Women 85 years and older | n = 8880 | All chronic conditions and disability (except diabetes) were diagnosed by a clinician while diabetes was captured based on self-report; Ryff PWB scale (7-item); Keyes scale for PG. |
| 23 | Windsor et al. (2015) [60] | Australia | Community | Cohort study Longitudinal | Older adults aged 65 and above. | n = 1475 | PIL subscale from Ryff’s PWB scale (3-item); Items on Functional disability (sum of two mobility items and five items assessing difficulties with physical movement and lifting/ handling objects); Single item on self-rated health; CESD scale; Digit Symbol Substitution subscale of the revised WAIS (speed of processing); Boston Naming Task for episodic memory. |
| 24 | Tomioka et al. (2016) [61] | Japan | Community | Cohort study | Older adults aged 65 and older | n (total, mortality study) = 1853 n (ADL study) = 1556 n (IADL study) = 1399 | Barthel index for ADL; TMIG Index of Competence; Single item for PIL; CPS for cognitive functions; GDS; Information about mortality, death and migration were obtained from the Shimoichi Town Hall; vital statuses of the participants were determined through the residential registration cards and death certificates. |
| 25 | Woods et al. (2016) [62] | USA | Community | Cohort study | Women 80 years and older | n = 26,704 | ADL scale, major causes of morbidity, Perceived Health Scale. And questionnaire on Independent living and physical function for measuring successful aging; BRS; Self-Mastery; Confidence, Environmental Mastery and Self-control for effective aging; Optimal aging measured using emotional Well-being Scale and asking “Have you been happy” and “you enjoyed life most of the time”; Satisfaction with Life Scale, Positive Relations (Social Support Scale) and Satisfaction with Current QOL. Eudemonic well-being measured using PG subscale and PIL Subscale (8-items) from Ryff’s PWB Scales. |
| 26 | Sano (2016) [63] | Japan | Community, day-service centers | Cross-sectional | Older adults. No age limits specified. Mean age of participants was 77.1 + 8.7 years old | n = 281 n (male) = 127, n (female) = 154 | SAMR and SOPI for Achievement motive; K-1 scale for PIL (16-items); Role expectation checklist. |
| 27 | Cook Maher et al. (2017) [64] | USA | Community | Longitudinal study cohorts | Older adults above 80 years | n = 50; Super agers n = 31, cognitively average older adults n = 19 | Ryff’s PWB questionnaire (42-items). |
| 28 | Vanhove-Meriaux and Claude (2018) [65] | France | Community, non-nursing home | Cross-sectional study | Older adults, age 65 years and older | n = 182 n (women) = 102 n (men) = 80 | Subscales of the French version of the Psychological Need Thwarting Scale—Older Adults; Psychological needs satisfaction was measured using three different questionnaires; French version of the Ryff’s PWB scales (14-items); French version of the subjective vitality scale; French version of the Rosenberg self-esteem Scale; French versions of the Positive and Negative Affect Schedule; French version of the GDS. |
| 29 | Musich et al. (2018) [66] | US | Community | Cross sectional | Older adults 65 years of age or older | n = 4563 | NIH Tuberculosis Meaning and Purpose Scale Age 18+ (7-items) for PIL; BRS; ISEL; Self-reported measures on HL and reliance on faith; Health care utilization, compliance and expenditures measured through claims submitted, adherence to treatment protocol or medication adherence; Veteran’s RAND 12-item QOL scale. |
| 30 | Orang et al. (2018) [67] | Iran | Community | Cross sectional | Young (aged 17–25 years), middle-aged (aged 26–46 years), and older adults (aged 65–80 years) | n = 215 n = 84 young (aged 17–25 years), n = 59 middle-aged (aged 26–46 years), and n = 72 older adults (aged 65–80 years) | Stareg’s MIL Scale; Ryff’s PWB scale. |
| 31 | Polenick et al. (2018) [68] | USA | Community | Cross sectional | Older adults 65 years of age or older | n = 315 | PIL subscale of Ryff’s PWB scale (1-item); Self-reports for Caregiving difficulties and gender. |
| 32 | Kim et al. (2019) [22] | South Korea | Community | Cross sectional | Older adults above 50; Age groups 50–59 years, 60–69 years, 70–79 years, 80 and above. | N = 11,525 | PIL was measured through a modified scale created by combining five items from the Ryff Measures of Psychological Wellbeing and two additional items from Personal Growth and Self-Acceptance. |
| 33 | Oliveira et al. (2019) [69] | Brazil | Community | Cross sectional | Older adults 60 years of age or older | n = 92; n = 61 were 60–69 years old n = 31 were 70 years old or over | Sociodemographic questionnaire (use of medicine, patterns of PA, et c); The Satisfaction with Life Scale; Ryff PWB scale (10-item). |
| 34 | Poulos et al. (2019) [70] | Australia | Community | Mixed methods | Older adults 65 years of age or older | n = 127 | Open-ended questions; WEMWBS; measures for Frailty; Focus group interviews |
| 35 | Sutin et al. (2020) [71] | USA | Community | Cross-sectional and longitudinal multi-cohort design | HRS: American and their spouses, 65 years and above NHATS: Participants aged 65 years and above from Medicare beneficiaries | Baseline sample: n = 6785 in HRS, n = 5665 in NHATS longitudinal sample: n = 4616 in HRS, n = 2877 in NHATS | HRS measured PIL using Ryff’s PWB scale (7-items) while NHATS used a single item; TICSm for cognitive function in HRS while sum of 3 tasks (memory, orientation and executive functions) in NHATS; HRS use 26 item version of MDI, NHATS use 10 item version of MDI; CESDS and PHQ-2; chronic conditions checklist of 7 conditions; Single items for PA. |
| 36 | Tkatch et al. (2020) [72] | USA | Community | Longitudinal cohort | Older adults above 65 years old | n (T1) = 216 n (T1 + 2) = 168 n (T1 + 2 + 3) = 125 | HCC risk score for Clinical health status; Veteran’s RAND(VR-12); short version of the UCLE Loneliness Scale; BRS; NIH Tuberculosis Meaning and Purpose Scale Age 18+ (7-item); LOT-R for optimism. |
| 37 | Vanhove-Meriaux and Ferrand (2020) [73] | France | Community | Cross-sectional study | Older adults, above 65 years older | n = 154 | French version of the PNFS-OA (BPNF); French version Ryff’s PWB scale (14 items); French version of the subjective vitality scale; PANAS; French version of the Rosenberg Self-Esteem. |
| 38 | Lewis et al. (2020) [74] | Canada | Community, Retirement individuals | Qualitative study | Older adults between the ages of 71 and 94 years (mean = 85.22 years) | n = 18 | PIL sub-section of Ryff’s PWB scale (7-items); IADL Scale; Perceived Isolation Scale; GDS. |
| 39 | Lopez et al. (2020) [75] | Spain | Community | Cross sectional | Young-old (60–70 years) and Old-old (71–80 years). | n = 878 | The Family APGAR; BRCS; Gratitude subscale of the Values in Action Inventory of Strengths-Short Form; AAQ-II; PG and PIL subscale of Ryff’s PWB scale (6-items). |
| 40 | Matud et al. (2020) [76] | Spain | Community | Cross sectional | Older adults 65 years of age or older | n = 1201 | Spanish version of the Ryff’s PWB Scale (38-items (6 items for PIL)); scales of masculinity and femininity of the BSRI; Spanish version of the York Self-Esteem Inventory; Social Support Scale. |
| 41 | Bundick et al. (2021) [77] | USA | Community | Cross sectional | Older adults of 2 age groups 50–64 (midlife sample), and 65 and older (later life sample). | n = 1198; midlife sample: n = 799; later life sample n = 399. | WHO-HPQ; A new survey measure (10 items on a 5-point scale) for PIL and Purpose in Life (PIL) subscale of Ryff’s PWB scales (9-items); Empathic Concern subscale of Davis’s Interpersonal Reactivity Index (IRI). LGS for Generativity; GQ-6 for gratitude; Satisfaction with Life Scale; PGIS; BWSS. |
| 42 | Alfonso-Benlliure et al. (2021) [78] | Spain | Community | Cross sectional | Aged 65 years or older. | n = 152 | MMSE for cognitive impairment; CESDS; TCI-A; Ryff’s PWB scale (items not reported). |
| 43 | Musich et al. (2021) [79] | USA | Community | Cross-sectional | At least 65 years of age with minimum of 12 month continuous medical plan enrolment (AARP Medicare Supplement Insured) | n = 3573 | LET (6-items); BRS; LOT-R; Wallston’s MHLC scale; Social Network Index; PHQ-2; Veterans Rand-12 (VR-12); Healthcare utilization and expenditure captured from administrative medical claims as IP admissions or ER visits and paid medical claims within the one-year pre-survey period. |
| 44 | Zhang and Chen (2021) [80] | USA | Community | Cohort study | Older adults 65 years and older | n (T1) = 4591 n (T2) = 3687 n (T3) = 2818 | Three items assessing the frequency of PA (vigorous, moderate and light-intensity PA); PIL subscale from Ryff’s PWB scale (7 items). |
| No. | Study ID | Health and Well-Being | Meaningful Aims and Goals | Inner Strength | Social Relationships | Mattering to Others | Spirituality and Religiousness |
|---|---|---|---|---|---|---|---|
| 1 | Gerwood et al. (1998) [40] | √ | |||||
| 2 | Bondevik and Skogstad (2000) [41] | √ | √ | √ | √ | √ | |
| 3 | Greenfield and Marks (2004) [42] | √ | √ | ||||
| 4 | Frazier et al. (2005) [43] | √ | √ | √ | √ | ||
| 5 | Nygren (2005) [44] | √ | √ | √ | |||
| 6 | Cicirelli (2006) [45] | √ | |||||
| 7 | Dixon (2007) [46] | √ | √ | √ | √ | ||
| 8 | Triado et al. (2007) [47] | √ | √ | ||||
| 9 | Moon and Mikami (2007) [48] | √ | |||||
| 10 | Hedberg et al. (2009) [50] | √ | √ | √ | |||
| 11 | Krause (2009) [51] | √ | √ | √ | |||
| 12 | Ferguson and Goodwin (2010) [52] | √ | √ | ||||
| 13 | Hedberg et al. (2010a) [53] | √ | √ | ||||
| 14 | Hedberg et al. (2010b) [54] | √ | √ | √ | |||
| 15 | Hedberg et al. (2011) [55] | √ | √ | √ | |||
| 16 | Lundman et al. (2012) [56] | √ | √ | ||||
| 17 | Hedberg et al. (2013) [57] | √ | √ | √ | √ | √ | |
| 18 | Wilson et al. (2013) [58] | √ | √ | ||||
| 19 | Pearson et al. (2013) [59] | √ | |||||
| 20 | Zaslavsky et al. (2014) [26] | √ | √ | √ | |||
| 21 | Windsor et al. (2015) [60] | √ | √ | √ | |||
| 22 | Tomioka et al. (2016) [61] | √ | |||||
| 23 | Woods et al. (2016) [62] | √ | |||||
| 24 | Sano (2016) [63] | √ | √ | ||||
| 25 | Cook Maher et al. (2017) [64] | √ | |||||
| 26 | Vanhove-Meriaux and Claude (2018) [65] | √ | √ | √ | √ | ||
| 27 | Musich et al. (2018) [66] | √ | √ | √ | |||
| 28 | Polenick et al. (2018) [68] | √ | √ | ||||
| 29 | Kim et al. (2019) [22] | √ | |||||
| 30 | Oliveira et al. (2019) [69] | √ | √ | ||||
| 31 | Poulos et al. (2019) [70] | √ | √ | √ | √ | ||
| 32 | Sutin et al. (2020) [71] | √ | √ | ||||
| 33 | Tkatch et al. (2020) [72] | √ | √ | √ | |||
| 34 | Vanhove-Meriaux and Ferrand (2020) [73] | √ | √ | √ | |||
| 35 | Lewis et al. (2020) [74] | √ | √ | √ | |||
| 36 | Lopez et al. (2020) [75] | √ | √ | √ | |||
| 37 | Matud et al. (2020) [76] | √ | √ | √ | √ | ||
| 38 | Bundick et al. (2021) [77] | √ | √ | ||||
| 39 | Alfonso-Benlliure et al. (2021) [78] | √ | √ | ||||
| 40 | Musich et al. (2021) [79] | √ | √ | √ | √ | √ | |
| 41 | Zhang and Chen (2021) [80] | √ | √ |
| No: | Study ID | Determinants |
|---|---|---|
| 1 | Gerwood (1996) [39] | Depression Spirituality |
| 2 | Gerwood (1998) [40] | Spirituality |
| 3 | Bondevik (2000) [41] | Religiousness Loneliness |
| 4 | Greenfield (2004) [42] | Role identity (volunteering moderate PIL and role identity) |
| 5 | Frazier (2005) [43] | Religious involvements |
| 6 | Nygren (2005) [44] | Resilience, sense of coherence, self-transcendence and perceived mental health |
| 7 | Cicirelli (2006) [45] | Fear of body loss Health |
| 8 | Dixon (2007) [46] | Overall wellness Mattering to others Depression |
| 9 | Triado (2007) [47] * | Personal growth Age Education Income |
| 10 | Moon (2007) [48] | Subjective well being |
| 11 | Ottenbacher (2007) [49] | Self-acceptance Positive Relation Environmental Mastery Personal Growth |
| 13 | Krause (2009) [51] | Self-rated Heath/fewer functional disabilities Mortality |
| 14 | Ferguson (2010) [52] | Optimism Perception of control (mediates relation between optimism and PIL) |
| 16 | Hedberg (2010) [53,54] | Attitude towards aging Having family Musculoskeletal symptoms |
| 17 | Hedberg (2011) [55] | Gender (women) Depression |
| 18 | Lundman (2012) [56] | Resilience, sense of coherence, self-transcendence |
| 20 | Wilson (2013) [58] | Global cognition/cognitive function |
| 21 | Pearson (2013) [59] | Education |
| 22 | Zaslavsky (2014) [26] | Health Disability Mortality |
| 23 | Windsor (2015) [60] | Memory Disability Decline of speed Health Depression Delayed mortality |
| 24 | Tomioka (2016) [61] | Higher mortality Instrumental activities of daily living |
| 25 | Woods (2016) [62] | Higher education Higher family income Marital status (married) Smoking status (non-smokers) Alcohol use (<1 drinks week) |
| 26 | Sano (2016) [63] | Achievement motive (Direct), Social participation Role expectation |
| 28 | Vanhove-Meriaux, (2018) [65] | High satisfaction need Low thwarting need Competence (extend to which people interact with environment) and relatedness need satisfactions (extend of a secure sense of belongingness and connectedness) |
| 29 | Musich (2018) [66] | High resilience High social support Strong alliance with faith High health literacy Good health Financial stress, living alone and >80 y had negative relation with PIL Reduced medical and drug expenditure Utilisation and expenditure Higher QoL Compliance with medication protocols Preventive service utilization |
| 31 | Polenick (2018) [68] | Gender specific fewer Emotional caregiving difficulties (females) Fewer physical care giving difficulties |
| 32 | Kim (2019) [22] | Higher cognition Decline in cognition |
| 33 | Oliveira (2019) [69] | Life satisfaction |
| 35 | Sutin (2020) [71] | Lower risk of concurrent motoric cognitive risk |
| 37 | Vanhove-Meriaux (2020) [73] | Basic psychological need frustration (predictor) Basic psychological need satisfaction |
| 39 | Lopez (2020) [75] | Perceived health, family functioning, resilience, gratitude and acceptance Loss of a loved one |
| 41 | Bundick (2021) [77] | Gender (female) Race/ethnicity Age |
| 42 | Alfonso-Benlliure (2021) [78] | Positive relationship with others Personal growth Environmental mastery Self-acceptance Life satisfaction Divergent thinking |
| 43 | Zhang and Chen (2021) [80] | Intensity of physical activity (predicted) Female gender, married, white/Caucasian, older at baseline, higher levels of education, better self-rated health, and fewer chronic conditions |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
AshaRani, P.; Lai, D.; Koh, J.; Subramaniam, M. Purpose in Life in Older Adults: A Systematic Review on Conceptualization, Measures, and Determinants. Int. J. Environ. Res. Public Health 2022, 19, 5860. https://doi.org/10.3390/ijerph19105860
AshaRani P, Lai D, Koh J, Subramaniam M. Purpose in Life in Older Adults: A Systematic Review on Conceptualization, Measures, and Determinants. International Journal of Environmental Research and Public Health. 2022; 19(10):5860. https://doi.org/10.3390/ijerph19105860
Chicago/Turabian StyleAshaRani, PV, Damien Lai, JingXuan Koh, and Mythily Subramaniam. 2022. "Purpose in Life in Older Adults: A Systematic Review on Conceptualization, Measures, and Determinants" International Journal of Environmental Research and Public Health 19, no. 10: 5860. https://doi.org/10.3390/ijerph19105860