
Public Opinion on European Health Policy, Lessons from the COVID-19 Pandemic


Abstract
:1. Introduction
2. Literature Review
- Cluster 1: addition, adult, burden, association, campus, cancer, child, concern, condition, cost, death, diagnosis, disease, difference, effect, evaluation, factor, gender, hospital, incidence, infection, intervention, lockdown, mental health, mortality, quality, public health policy, prevalence, restriction, risk, social distancing, symptom, treatment, transmission, vaccination.
- Cluster 2: access, action, activity, attitude, benefit, capacity, challenge, change, community, crisis, demand, economy, effort, emergency, employment, environment, evidence, experience, focus, future, government, health system, healthcare, impact, implementation, impact, income, importance, inequality, information, interest, knowledge, lack, opportunity, recommendation, response, relationship, sustainability, uncertainty, vulnerability, strategy.
- Cluster 3: collaboration, commission, control, decision, development, drug, economic, education, financial support, health research, health policy, horizon, innovation, medical research, ministry, national, national institute, partnership, practice, role, preparation.
- Cluster 4: account, coronavirus, effectiveness, epidemic, end, measure, mobility, outbreak, policy maker, prevention, spread, world, world health organization.
- Cluster 5: care, communication, epidemiology, ethic, frontier, general and internal, infectious disease, medical informatics, public health, social science, technology, topic, medicine, journal.
- Cluster 6: COVID, green, management.
3. Data and Methodology
4. Results
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Announces COVID-19 Outbreak a Pandemic. World Health Organization. 2020. Available online: http://www.euro.who.int/en/health-topics/health-mergencies/coronavirus-covid-19/news/news/2020/3/who-announces-covid-19-outbreak-a-pandemic (accessed on 15 March 2022).
- Nicola, M.; Alsafi, Z.; Sohrabi, C.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C. The socio-economic implications of the coronavirus and COVID-19 pandemic: A review. Int. J. Surg. Lond. Engl. 2020, 78, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Sohrabi, C.; Alsafi, Z.; O’Neill, N.; Khan, M.; Kerwan, A.; Al-Jabir, A. World Health Organization declares global emergency: A review of the 2019 novel coronavirus (COVID-19). Int. J. Surg. 2020, 76, 71–76. [Google Scholar] [CrossRef] [PubMed]
- Sturmberg, J.P.; Tsasis, P.; Hoemeke, L. COVID-19—An Opportunity to Redesign Health Policy Thinking. Int. J. Health Policy Manag. 2020, 14, 409–413. [Google Scholar] [CrossRef] [PubMed]
- Boulton, J. Complexity theory and implications for policy development. Emerg. Complex. Organ. 2010, 12, 31–40. [Google Scholar]
- Boswell, J.; Cairney, P.; St Denny, E. The politics of institutionalizing preventive health. Soc. Sci. Med. 2019, 228, 202–210. [Google Scholar] [CrossRef] [Green Version]
- Tsasis, P.; Evans, J.M.; Owen, S. Reframing the challenges to integrated care: A complex-adaptive systems perspective. Int. J. Integr. Care 2012, 12, e190. [Google Scholar] [CrossRef]
- Sturmberg, J.P. Health System Redesign. How to Make Health Care Person-Centered, Equitable, and Sustainable; Springer: Cham, Switzerland, 2018. [Google Scholar]
- Frasholli, D.; Hysa, E. Investment in health and economic inclusion of south eastern European countries. Rev. Stiinte Politice 2015, 46, 247. [Google Scholar]
- Jacobs, L.R.; Mettler, S. Why public opinion changes: The implications for health and health policy. J. Health Polit. Policy Law 2011, 36, 917–933. [Google Scholar] [CrossRef]
- Greer, L.S.; de Ruijter, A.; Brooks, E. The COVID-19 Pandemic: Failing Forward in Public Health’ Forthcoming. In The Palgrave Handbook of European Union Crisis; Riddervold, M., Trondal, J., Newsome, A., Eds.; Palgrave Macmillan: Basingstoke, UK, 2020. [Google Scholar]
- Brooks, P.; Zank, H. Loss averse behavior. J. Risk Uncertain. 2005, 31, 301–325. [Google Scholar] [CrossRef]
- Burki, T. Outbreak of coronavirus disease 2019. Lancet Infect. Dis. 2020, 20, 292–293. [Google Scholar] [CrossRef]
- Pacces, A.M.; Weimer, M. From Diversity to Coordination: A European Approach to COVID-19. Eur. J. Risk Regul. 2020, 11, 283–296. [Google Scholar] [CrossRef] [Green Version]
- Renda, A.; Castro, R. Towards Stronger EU Governance of Health Threats after the COVID-19 Pandemic. Eur. J. Risk Regul. 2020, 11, 273–282. [Google Scholar] [CrossRef] [Green Version]
- Dimian, G.C.; Apostu, S.A.; Vasilescu, M.D.; Aceleanu, M.I.; Jablonsky, J. Vulnerability and resilience in health crises. Evidence from European countries. Technol. Econ. Dev. Econ. 2021, 27, 783–810. [Google Scholar] [CrossRef]
- Goldman, M.L.; Druss, B.G.; Horvitz-Lennon, M.; Norquist, G.S.; Ptakowski, K.K.; Brinkley, A.; Greiner, M.; Hayes, H.; Hepburn, B.; Jorgensen, S.; et al. Mental Health Policy in the Era of COVID-19. Psychiatr. Serv. 2020, 71, 1158–1162. [Google Scholar] [CrossRef] [PubMed]
- Raoofi, A.; Takian, A.; Sari, A.A.; Olyaeemanesh, A.; Haghighi, H.; Aarabi, M. COVID-19 Pandemic and Comparative Health Policy Learning in Iran. Arch. Iran. Med. 2020, 23, 220–234. [Google Scholar] [CrossRef] [Green Version]
- McBryde, E.S.; Meehan, M.T.; Adegboye, O.A.; Adekunle, A.I.; Caldwell, J.M.; Pak, A.; Rojas, D.P.; Williams, B.M.; Trauer, J.M. Role of modelling in COVID-19 policy development. Paediatr. Respir. Rev. 2020, 35, 57–60. [Google Scholar] [CrossRef]
- Meehan, M.T.; Rojas, D.P.; Adekunle, A.I.; Adegboye, O.A.; Caldwell, J.M.; Turek, E.; Williams, B.M.; Marais, B.J.; Trauer, J.M.; McBryde, E.S. Modelling insights into the COVID-19 pandemic. Paediatr. Respir. Rev. 2020, 35, 64–69. [Google Scholar] [CrossRef]
- Taylor, C. How New Zealand’s ‘Eliminate’ Strategy Brought New Coronavirus Cases Down to Zero. Library Catalog: www.cnbc.com Section: Health & Science. May 2020. Available online: https://www.cnbc.com/2020/05/05/how-new-zealand-brought-new-coronavirus-cases-down-to-zero.html (accessed on 6 March 2022).
- Press Conference—Australian Parliament House, ACT: Transcript 16 Apr. PM&C, Ed. ACT, Australia. 2020. Available online: https://www.pm.gov.au/media/press-conference-australian-parliament-house-act-15 (accessed on 12 January 2022).
- Boris Johnson: Full Speech on Modified Coronavirus Lockdown Plan. 10 May 2020. Available online: https://www.bbc.com/news/av/uk-politics-52605886 (accessed on 12 March 2022).
- Adjie, M.F.P. Indonesia’s R0, Explained. 2020. Available online: https://www.thejakartapost.com/news/2020/06/01/indonesias-r0-explained.html (accessed on 16 March 2022).
- Fofana, N.K.; Latif, F.; Sarfraz, S.; Bilal; Bashir, M.F.; Komal, B. Fear and agony of the pandemic leading to stress and mental illness: An emerging crisis in the novel coronavirus (COVID-19) outbreak. Psychiatry Res. 2020, 291, 113230. [Google Scholar] [CrossRef]
- Sharma, G.D.; Talan, G.; Jain, M. Policy response to the economic challenge from COVID-19 in India: A qualitative enquiry. J. Public Aff. 2020, 20, e2206. [Google Scholar] [CrossRef]
- Gourinchas, P.O. Flattening the pandemic and recession curves. Mitigating COVID Econ. Crisis Act Fast Do Whatever 2020, 31, 57–62. [Google Scholar]
- Pak, A.; Adegboye, O.A.; Adekunle, A.I.; Rahman, K.M.; McBryde, E.S.; Eisen, D.P. Economic consequences of the COVID-19 outbreak: The need for epidemic preparedness. Front. Publ. Health 2020, 8, 241. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.A.R.; Janjua, L.R.; Yu, Z. COVID-19: A Learning Opportunity to Improve Environmental Sustainability. In Carbon Capture; IntechOpen: London, UK, 2020; p. 43. [Google Scholar]
- Venetoklis, T. Exogenous shocks and citizens’ satisfaction with governmental policies: Can empirical evidence from the 2008 financial crisis help us understand better the effects of the COVID-19 pandemic? Qual. Quant. 2021, 55, 1973–2000. [Google Scholar] [CrossRef] [PubMed]
- Song, M.; Tian, X.; Wang, X. Influence of Health Education on KAP towards Infectious Atypical Pneumonia in Urban Residents of Beijing. Chin. J. Health Edu. 2003, 7, 34–35. [Google Scholar]
- Bener, A.; Al-Khal, A. Knowledge, attitude and practice towards SARS. J. R. Soc. Promot. Health 2004, 124, 167–170. [Google Scholar] [CrossRef]
- Huang, L.; Hong, X.; Ke, Y. An intervention study on hygienic knowledge, attitude and behavior of Middle East respiratory syndrome. Chin. Tropical. Med. 2016, 16, 827–829. [Google Scholar]
- Bawazir, A.; Al-Mazroo, E.; Jradi, H.; Ahmed, A.; Badri, M. MERS-CoV infection: Mind the public knowledge gap. J. Infect. Public Health 2017, 11, 89–93. [Google Scholar] [CrossRef]
- Alqahtani, A.S.; Rashid, H.; Basyouni, M.H.; Alhawassi, T.M.; BinDhim, N.F. Public response to MERS-CoV in the Middle East: iPhone survey in six countries. J. Infect. Public Health 2017, 10, 534–540. [Google Scholar] [CrossRef]
- Al-Mohrej, O.A.; Al-Shirian, S.D.; Al-Otaibi, S.K.; Tamim, H.M.; Masuadi, E.M.; Fakhoury, H.M. Is the Saudi public aware of Middle East respiratory syndrome? J. Infect Public Health 2016, 9, 259–266. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.; Jin, Y.L.; Zhu, L.J.; Fang, Z.M.; Wu, N.; Du, M.X.; Jiang, M.M.; Wang, J.; Yao, Y.S.; Zhong, H. Flexible optoelectronic devices based on metal halide perovskites. Nano Res. 2020, 13, 1997–2018. [Google Scholar] [CrossRef]
- Zhong, B.-L.; Luo, W.; Li, H.-M.; Zhang, Q.-Q.; Liu, X.-G.; Li, W.-T.; Li, Y. Knowledge, attitudes, and practices towards COVID-19 among Chinese residents during the rapid rise period of the COVID-19 outbreak: A quick online cross-sectional survey. Int. J. Biol. Sci. 2020, 16, 1745–1752. [Google Scholar] [CrossRef]
- Qi, Y.; Chen, L.H.; Zhang, L. Public practice, attitude and knowledge of coronavirus disease. J. Trop. Med. 2020, 20, 145–149. [Google Scholar]
- Li, W.; Liao, J.; Li, Q.; Baskota, M.; Wang, X.; Tang, Y.; Zhou, Q.; Wang, X.; Luo, X.; Ma, Y.; et al. Public health education for parents during the outbreak of COVID-19: A rapid review. Ann. Transl. Med. 2020, 8, 628. [Google Scholar] [CrossRef] [PubMed]
- Anders, R.L. Engaging nurses in health policy in the era of COVID-19. Nurs. Forum 2020, 56, 89–94. [Google Scholar] [CrossRef] [PubMed]
- WHO. Statement by Dr Zsuzsanna Jakab, WHO Regional Director for Europe, for International Women’s Day, World Health Organization. 2017. Available online: www.euro.who.int/en (accessed on 3 March 2022).
- Lundeberg, M.A.; Fox, P.W.; Punćochaŕ, J. Highly Confident but Wrong: Gender Differences and Similarities in Confidence Judgments. J. Educ. Psychol. 1994, 86, 114–121. [Google Scholar] [CrossRef]
- Agnew, J.R.; Anderson, L.; Gerlach, J.R.; Szykman, L.R. Who Chooses Annuities? An Experimental Investigation of the Role of Gender, Framing, and Defaults. Am. Econ. Rev. 2008, 98, 418–422. [Google Scholar] [CrossRef] [Green Version]
- Byrnes, J.P.; Miller, D.C.; Schafer, W.D. Gender differences in risk taking: A meta-analysis. Psychol. Bull. 1999, 125, 367–383. [Google Scholar] [CrossRef]
- Pandey, J.; Jain, U. Worldviews and perceptions of environmental problems. Psychol. Stud. 2017, 62, 250–260. [Google Scholar] [CrossRef]
- Leung, T.; Sharma, P.; Adithipyangkul, P.; Hosie, P. Gender equity and public health outcomes: The COVID-19 experience. J. Bus. Res. 2020, 116, 193–198. [Google Scholar] [CrossRef]
- Ertac, S.; Gurdal, M.Y. Deciding to decide: Gender, leadership and risk-taking in groups. J. Econ. Behav. Organ. 2012, 83, 24–30. [Google Scholar] [CrossRef] [Green Version]
- Gebhard, C.; Regitz-Zagrosek, V.; Neuhauser, H.K.; Morgan, R.; Klein, S.L. Impact of sex and gender on COVID-19 outcomes in Europe. Biol. Sex Differ. 2020, 11, 29. [Google Scholar] [CrossRef]
- Baker, P.; White, A.; Morgan, R. Men’s health: COVID-19 pandemic highlights need for overdue policy action. Lancet 2020, 395, 1886–1888. [Google Scholar] [CrossRef]
- Betron, M.; Gottert, A.; Pulerwitz, J.; Shattuck, D.; Stevanovic-Fenn, N. Men and COVID-19: Adding a gender lens. Glob. Public Health 2020, 15, 1090–1092. [Google Scholar] [CrossRef] [PubMed]
- Serge, R.; Vandromme, J.; Charlotte, M. Are we equal in adversity? Does COVID-19 affect women and men differently? Maturitas 2020, 138, 62–68. [Google Scholar] [CrossRef]
- Beenackers, M.A.; Groeniger, J.O.; Kamphuis, C.B.; Van Lenthe, F.J. Urban population density and mortality in a compact Dutch city: 23-year follow-up of the Dutch GLOBE study. Health Place 2018, 53, 79–85. [Google Scholar] [CrossRef]
- Greiner, K.; Li, C.; Kawachi, I.; Hunt, D.; Ahluwalia, J.S. The relationships of social participation and community ratings to health and health behaviors in areas with high and low population density. Soc. Sci. Med. 2004, 59, 2303–2312. [Google Scholar] [CrossRef]
- Ma, W.M.H.; Harrison, M.B.; Coo, H.; Friedberg, E.; Buchanan, M.; VanDenKerkhof, E.G. Associations between chronic disease, age, and physical and mental health status Chronic Diseases in Canada. Chronic Dis. Can 2009, 29, 108–116. [Google Scholar]
- Sun, S.; Chen, J.; Johannesson, M.; Kind, P.; Xu, L.; Zhang, Y.; Burström, K. Population health status in China: EQ-5Q results, by age, sex and socio-economic status, from the National Health Services Survey 2008. Qual. Life Res. 2011, 20, 309–320. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.; Kim, S. Searching for General Model of Conspiracy Theories and Its Implication for Public Health Policy: Analysis of the Impacts of Political, Psychological, Structural Factors on Conspiracy Beliefs about the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2020, 18, 266. [Google Scholar] [CrossRef]
- Mao, J.; Yang, S.; Guo, Y. Are individuals from lower social classes more susceptible to conspiracy theories? An explanation from the compensatory control theory. Asian J. Soc. Psychol. 2020, 23, 372–383. [Google Scholar] [CrossRef]
- Golec de Zavala, A.; Federico, C.M. Collective narcissism and the growth of conspiracy thinking over the course of the 2016 United States presidential election: A longitudinal analysis. Eur. J. Soc. Psychol. 2018, 48, 1011–1018. [Google Scholar] [CrossRef]
- Douglas, K.M.; Uscinski, J.E.; Sutton, R.M.; Cichocka, A.; Nefes, T.; Ang, C.S.; Deravi, F. Understanding Conspiracy Theories. Political Psychol. 2019, 40, 3–35. [Google Scholar] [CrossRef] [Green Version]
- Uscinski, J.E.; Joseph, M. Parent. In American Conspiracy Theories; Oxford University Press: New York, NY, USA, 2014. [Google Scholar]
- Beland, L.; Brodeur, A.; Mikola, D.; Wright, T. The short-term economic consequences of COVID-19: Occupation tasks and mental health in Canada. SSRN 2022, 55, 214–247. [Google Scholar] [CrossRef]
- Smith, R.S. Compensating Wage Differentials and Public Policy: A Review. ILR Rev. 1979, 32, 339–352. [Google Scholar] [CrossRef]
- Eberhardt, M.S.; Ingram, D.D.; Makuc, D.M. Urban and Rural Health Chart-Book. Health, United States, 2001; National Center for Health Statistics: Hyattsville, MD, USA, 2001. [Google Scholar]
- Dong, H.; Kouyate, B.; Cairns, J.; Sauerborn, R. Inequality in willingness-to-pay for community-based health insurance. Health Policy 2005, 72, 149–156. [Google Scholar] [CrossRef]
- Onwujekwe, O.; Okereke, E.; Onoka, C.; Uzochukwu, B.; Kirigia, J.; Petu, A. Willingness to pay for community-based health insurance in Nigeria: Do economic status and place of residence matter? Health Policy Plan. 2009, 25, 155–161. [Google Scholar] [CrossRef]
- Nutley, S.M.; Walter, I.; Davies, H.T. Using Evidence How Research Can Inform Public Services; Policy Press: Bristol, UK, 2007. [Google Scholar]
- Dutil, L.; Irwin, R.; Finley, R.; Ng, L.K.; Avery, B.; Boerlin, P.; Bourgault, A.-M.; Cole, L.; Daignault, D.; Desruisseau, A.; et al. Ceftiofur resistance in Salmonella enterica serovar Heidelberg from chicken meat and humans, Canada. Emerg. Infect. Dis. 2010, 16, 48–54. [Google Scholar] [CrossRef]
- Currie, J.; Rossin-Slater, M. Early-Life Origins of Life-Cycle Well-Being: Research and Policy Implications. J. Policy Anal. Manag. 2014, 34, 208–242. [Google Scholar] [CrossRef] [Green Version]
- Stecker, C.; Tausendpfund, M. Multidimensional government-citizen congruence and satisfaction with democracy. Eur. J. Political Res. 2016, 55, 492–511. [Google Scholar] [CrossRef]
- Fiorina, M.P. Economic Retrospective Voting in American National Elections: A Micro-Analysis. Am. J. Political Sci. 1978, 22, 426. [Google Scholar] [CrossRef]
- Healy, A.; Malhotra, N. Retrospective Voting Reconsidered. Annu. Rev. Political Sci. 2013, 16, 285–306. [Google Scholar] [CrossRef]
- Dassonneville, R.; Lewis-Beck, M.S. A changing economic vote in Western Europe? long-term vs short-term forces. Eur. Polit. Sci. Rev. 2019, 11, 91–108. [Google Scholar] [CrossRef]
- Larsen, E.G.; Klemmensen, R.; Klitgaard, M.B. Bailout or bust? Government evaluations in the wake of a bailout. Eur. Political Sci. Rev. 2019, 11, 231–246. [Google Scholar] [CrossRef] [Green Version]
- Van de Walle, S.; Bouchaert, G. Public service performance and trust in governance: The problem of causality. Int. J. Public Adm. 2003, 26, 891–914. [Google Scholar] [CrossRef] [Green Version]
- Lyons, W.E.; Lowery, D.; Dehoog, R.H. The Politics of Dissatisfaction Citizens Services and Urban Institutions; M E Sharpe Inc.: Armonk, NY, USA, 1992. [Google Scholar]
- Van Ryzin, G.; Muzzio, D.; Immerwahr, S.; Gulick, L.; Martinez, E. Drivers and Consequences of Citizen Satisfaction: An Application of the American Customer Satisfaction Index Model to New York City. Public Adm. Rev. 2004, 64, 331–341. [Google Scholar] [CrossRef]
- Christensen, T.; Laegreid, P. Trust in government: The relative importance of service satisfaction political factors and demography. Public Perform. Manag. Rev. 2005, 28, 487–511. [Google Scholar]
- Van de Walle, S. Determinants of confidence in the civil service: An international comparison. In Cultural Aspects Public Management Reform; Schedler, K., Proeller, I., Eds.; Elsevier: Amsterdam, The Netherlands, 2007; pp. 171–201. [Google Scholar]
- Van Ryzin, G. Service quality administrative process and citizens’ evaluation of local government in the US public. Manag. Rev. 2015, 17, 425–442. [Google Scholar]
- Bouckaert, G.; Van de Walle, S. Comparing measures of citizen trust and user satisfaction as indicators of ‘good governance’: Difficulties in linking trust and satisfaction indicators. Int. Rev. Adm. Sci. 2003, 69, 329–343. [Google Scholar]
- Jost, J.T.; Federico, C.M.; Napier, J.L. Political Ideology: Its Structure, Functions, and Elective Affinities. Annu. Rev. Psychol. 2009, 60, 307–337. [Google Scholar] [CrossRef] [Green Version]
- Haugsgjerd, A. Moderation or radicalisation? How executive power affects right-wing populists’ satisfaction with democracy. Elect. Stud. 2018, 57, 31–45. [Google Scholar] [CrossRef] [Green Version]
- Ellegaard, O.; Wallin, J.A. The bibliometric analysis of scholarly production: How great is the impact? Scientometrics 2015, 105, 1809–1831. [Google Scholar] [CrossRef] [Green Version]
- Donthu, N.; Kumar, S.; Pandey, N.; Lim, W.M. Research Constituents, Intellectual Structure, and Collaboration Patterns in Journal of International Marketing: An Analytical Retrospective. J. Int. Mark. 2021, 29, 1–25. [Google Scholar] [CrossRef]
- Verma, S.; Gustafsson, A. Investigating the emerging COVID-19 research trends in the field of business and management: A bibliometric analysis approach. J. Bus. Res. 2020, 118, 253–261. [Google Scholar] [CrossRef] [PubMed]
- Donthu, N.; Kumar, S.; Pandey, N. A retrospective evaluation of Marketing Intelligence and Planning: 1983–2019. Mark. Intell. Plan. 2020, 39, 48–73. [Google Scholar] [CrossRef]
- Donthu, N.; Kumar, S.; Pattnaik, D. Forty-five years of Journal of Business Research: A bibliometric analysis. J. Bus. Res. 2019, 109, 1–14. [Google Scholar] [CrossRef]
- Donthu, N.; Kumar, S.; Mukherjee, D.; Pandey, N.; Lim, W.M. How to conduct a bibliometric analysis: An overview and guidelines. J. Bus. Res. 2021, 133, 285–296. [Google Scholar] [CrossRef]
- Broadus, R.N. Toward a definition of “bibliometrics”. Scientometrics 1987, 12, 373–379. [Google Scholar] [CrossRef]
- Pritchard, A. Statistical bibliography or bibliometrics? J. Doc. 1969, 25, 348–349. [Google Scholar]
- Wallin, J.A. Bibliometric Methods: Pitfalls and Possibilities. Basic Clin. Pharmacol. Toxicol. 2005, 97, 261–275. [Google Scholar] [CrossRef]
- Glanzel, W. Bibliometrics as a Research Field a Course on Theory and Application of Bibliometric Indicators. 2003. Available online: https://d1wqtxts1xzle7.cloudfront.net/36509837/10.1.1.97.5311-with-cover-page-v2.pdf?Expires=1649958743&Signature=ci-ECvw4JHYHOuyu4udl~0juU9mcVroocTtzrcUu0pJ4DwL5~Vwt5cBFNX-eif495dZHE6WBCV38Om5IfGQLxV-zEBg3lLB6Yr0CwrgIMtEhPRcpZrYgPxQRafFGyjNEAhf1lhuiIl-ZYD5cIGPhknOtRWDc7HaVgzwYxfbc1r9jWyCDS0sf4A8JAvM-vndNs8qSE9LfDroE3fqHOgC7MWHG5XAdfHrYrVMWJxXqAb6iI3MKQjjSMPsXjdWU-wsu~xmx~AQr~mE6tVqAETeNJb02aJFU1zneGdCbtq~YRbGp1ujiORLr0Izt53twNh2I3bArvFbrhh7Ip2-3D38aGQ__&Key-Pair-Id=APKAJLOHF5GGSLRBV4ZA (accessed on 3 March 2022).
- Song, Y.; Zhao, T. A Bibliometric Analysis of Global Forest Cology Research during 2002–2011. SpringerPlus 2013, 2, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Marshakova-Shaikevich, I. Bibliometric maps of field of science. Inf. Process. Manag. 2005, 41, 1534–1547. [Google Scholar] [CrossRef]
- Glänzel, W.; Schoepflin, U. Little scientometrics, big scientometrics and beyond. Scientometrics 1994, 30, 375–384. [Google Scholar] [CrossRef]
- Ellegaard, O.; Wallin, J.A. Identification of environmentally relevant chemicals in bibliographic databases: A comparative analysis. SpringerPlus 2013, 2, 255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ledolter, J. Data Mining and Business Analytics with R; John Wiley & Sons: Iowa City, IA, USA, 2013. [Google Scholar]
- Dascalu, S. The Successes and Failures of the Initial COVID-19 Pandemic Response in Romania. Front. Public Health 2020, 8, 344. [Google Scholar] [CrossRef] [PubMed]
- Anghelache, C.; Anghel, M.-G.; Iacob, Ș.V.; Panait, M.; Rădulescu, I.G.; Brezoi, A.G.; Miron, A. The Effects of Health Crisis on Economic Growth, Health and Movement of Population. Sustainability 2022, 14, 4613. [Google Scholar] [CrossRef]
- Gao, X.; Sun, L. Modeling retirees’ investment behaviors in the presence of health expenditure risk and financial crisis risk. Econ. Model. 2020, 94, 442–454. [Google Scholar] [CrossRef]
- Pan, W.-F.; Wang, X.; Wu, G.; Xu, W. The COVID-19 pandemic and sovereign credit risk. China Financ. Rev. Int. 2021, 11, 287–301. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Description |
|---|---|
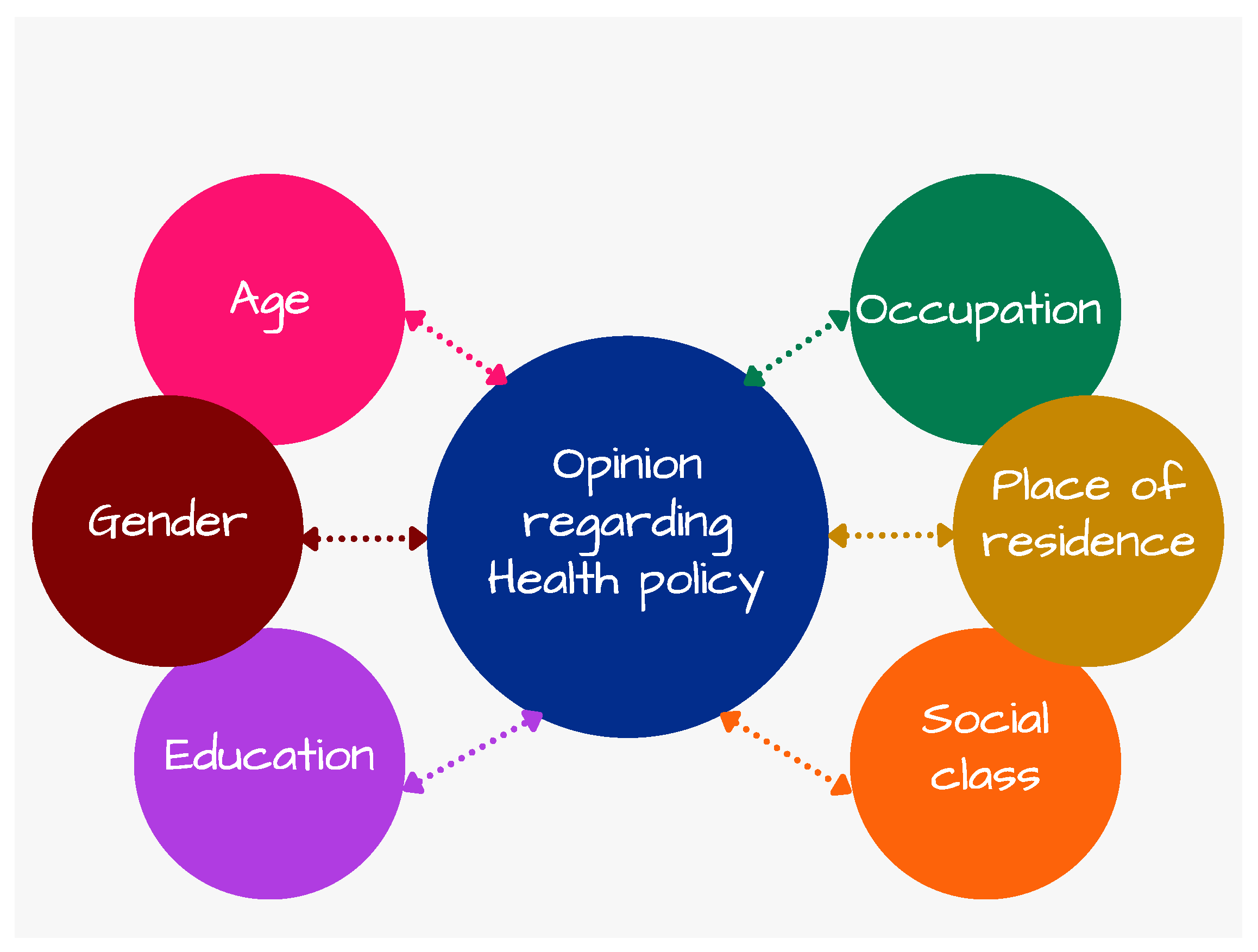
| Age | Age of the respondent, a categorial variable with four groups: 15 to 24 years, 25 to 39 years, 40 to 54 years, and 55 years or older. |
| Gender | Gender of the respondent, a binary variable with value 1 for men and 0 for women. |
| Education | Level of education, a categorial variable with three levels: low (up to 15 years of education), medium (between 16 and 19 years of schooling) and high (20 years of education or more). |
| Employment status | Employment status of the respondent, a categorial variable with three variants: employed (includes self-employed persons), retired, and unemployed or house persons. |
| Type of community | Place of residency, a binary variable with value 1 for urban and 0 for rural areas. |
| Social class | Social class of the respondent, a categorial variable with three levels: lower or working class, middle class and upper middle or higher class. This variable is used as a proxy for income or standard of living. |
| Financial consequences | Serious financial consequences due to the pandemic, a binary variable with value 1 indicating that the respondent was severely affected by the pandemic financially. The variable is used as a proxy for economically vulnerable individuals, due to pandemic. |
| Satisfaction COVID measures—local | A binary variable with value 1 indicating that the respondent is very satisfied or fairly satisfied with the measures taken by the local authorities to fight the coronavirus pandemic. |
| Satisfaction COVID measures—national | A binary variable with value 1 indicating that the respondent is very satisfied or fairly satisfied with the measures taken by the national government to fight the coronavirus pandemic. |
| Satisfaction COVID measures—EU | A binary variable with value 1 indicating that the respondent is very satisfied or fairly satisfied with the measures taken by the European Union to fight the coronavirus pandemic. |
| Health an important issue | A binary variable with value 1 indicating that the respondent considers health to be the most important issue at national level at the time of the interview. |
| Trust in health authorities | A binary variable with value 1 indicating that the respondent generally tends to trust the health authorities and medical staff in its country. |
| Trust in national government | A binary variable with value 1 indicating that the respondent generally tends to trust the national government. |
| Trust in EU | A binary variable with value 1 indicating that the respondent generally tends to trust the European Union. |
| Trust EU for pandemic | A binary variable with value 1 indicating that the respondent totally trusts or tends to trust that EU will make the right decisions in the future, considering its response to the coronavirus pandemic. |
| European health policy | A binary variable with value 1 indicating that the respondent agrees or totally agrees that the development of a European health policy should be a priority in the response to the coronavirus pandemic. |
| Variable | 2020 | 2021 | ||||
|---|---|---|---|---|---|---|
| N | Mean | Std. Deviation | N | Mean | Std. Deviation | |
| European health policy | 26,678 | 0.280 | 0.449 | 27,409 | 0.245 | 0.430 |
| Age | 33,055 | 3.018 | 1.019 | 38,699 | 2.964 | 1.012 |
| Gender | 33,055 | 0.464 | 0.499 | 38,718 | 0.484 | 0.500 |
| Education | 29,840 | 2.252 | 0.684 | 32,815 | 2.377 | 0.664 |
| Employment status | 30,818 | 1.434 | 0.627 | 38,718 | 1.764 | 1.036 |
| Type of community | 33,052 | 0.669 | 0.471 | 38,707 | 0.675 | 0.468 |
| Social class | 32,707 | 1.588 | 0.648 | 38,366 | 1.597 | 0.681 |
| Financial consequences | 31,442 | 0.547 | 0.498 | 38,367 | 0.506 | 0.500 |
| Health an important issue | 32,549 | 0.322 | 0.467 | 38,717 | 0.414 | 0.493 |
| Satisfaction COVID measures—national | 32,188 | 0.671 | 0.470 | 38,425 | 0.508 | 0.500 |
| Satisfaction COVID measures—EU | 29,712 | 0.544 | 0.498 | 36,824 | 0.517 | 0.500 |
| Trust in health authorities | 27,315 | 0.799 | 0.401 | 26,997 | 0.806 | 0.396 |
| Trust in national government | 26,775 | 0.446 | 0.497 | 37,616 | 0.428 | 0.495 |
| Trust in EU | 29,956 | 0.506 | 0.500 | 36,739 | 0.548 | 0.498 |
| Valid N (listwise) | 18,161 | 21,002 | ||||
| Explanatory Variables | MODEL 1-Year 2020 | MODEL 2-Year 2021 | |||
|---|---|---|---|---|---|
| B | Exp (B) | B | Exp (B) | ||
| Constant | −1.175 * | 0.309 | −1.653 * | 0.192 | |
| Age | Age (15–24 years)-ref | ||||
| Age (25–39 years) | −0.014 | 0.986 | 0.215 ** | 1.240 | |
| Age (40–54 years) | 0.038 | 1.038 | 0.139 | 1.149 | |
| Age (55 years and older) | 0.059 | 1.061 | 0.169 | 1.184 | |
| Gender (1 = man) | 0.038 | 1.039 | 0.070 ** | 1.073 | |
| Education | Low (up to 15 years)-ref | ||||
| Medium (16–19 years) | 0.083 | 1.087 | 0.149 ** | 1.161 | |
| High (20 years or more) | 0.045 | 1.046 | −0.019 | 0.981 | |
| Employment status | Employed-ref | ||||
| Retired | 0.131 * | 1.140 | 0.123 * | 1.131 | |
| Unemployed or house persons | 0.024 | 1.024 | −0.055 | 0.946 | |
| Type of community (1 = urban) | −0.065 | 0.937 | 0.058 | 1.060 | |
| Social class | Middle class-ref | ||||
| Lower or working class | −0.036 | 0.965 | 0.000 | 1.000 | |
| Upper middle or higher class | −0.085 | 0.918 | −0.210 * | 0.810 | |
| Serios financial consequences due to pandemics | 0.026 | 1.027 | 0.226 * | 1.254 | |
| Health-the most important issue | 0.251 * | 1.285 | 0.217 * | 1.242 | |
| Satisfaction COVID measures-national | 0.046 ** | 1.047 | −0.052 | 0.949 | |
| Satisfaction COVID measures-EU | −0.057 * | 0.944 | 0.118 * | 1.125 | |
| Trust-health authorities | 0.043 | 1.044 | −0.048 | 0.953 | |
| Trust-national government | 0.004 | 1.004 | −0.159 * | 0.853 | |
| Trust-EU | 0.123 * | 1.131 | 0.192 * | 1.212 | |
| Number of individuals included in the analysis | 19,486 | 21,002 | |||
| Nagelkerke R Square | 0.09 | 0.17 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vasilescu, M.D.; Apostu, S.A.; Militaru, E.; Hysa, E. Public Opinion on European Health Policy, Lessons from the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 4813. https://doi.org/10.3390/ijerph19084813
Vasilescu MD, Apostu SA, Militaru E, Hysa E. Public Opinion on European Health Policy, Lessons from the COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2022; 19(8):4813. https://doi.org/10.3390/ijerph19084813
Chicago/Turabian StyleVasilescu, Maria Denisa, Simona Andreea Apostu, Eva Militaru, and Eglantina Hysa. 2022. "Public Opinion on European Health Policy, Lessons from the COVID-19 Pandemic" International Journal of Environmental Research and Public Health 19, no. 8: 4813. https://doi.org/10.3390/ijerph19084813