
Intergenerational Effects of Discrimination on Black American Children’s Sleep Health


Abstract
:1. The Current Study
2. Materials and Methods
2.1. Participants
2.2. Procedure
2.3. Measures
2.3.1. Lifetime Experiences of Racial/Ethnic Discrimination and Gendered Racial Stress
“Have you ever experienced discrimination, been prevented from doing something, or been hassled or made to feel inferior in any of the following [nine] situations (i.e., at school, getting hired/getting a job, at work, getting housing, getting medical care, getting service at store/restaurant, getting credit/bank loans/mortgage, in public, with police/in courts) because of your race, ethnicity, or color?”
2.3.2. Prenatal Depressive Symptoms
2.3.3. Prenatal Sleep Quality
2.3.4. Maternal Depressive Symptoms at Child Age Two
2.3.5. Child Sleep Health at Child Age Two
2.3.6. Covariates
2.4. Data Analytic Plan
2.4.1. Preliminary Analyses
2.4.2. Primary Analyses
2.4.3. Sensitivity Analyses
3. Results
3.1. Participants
3.2. Main Effects of Women’s Exposure to Discrimination on Offspring Sleep Health
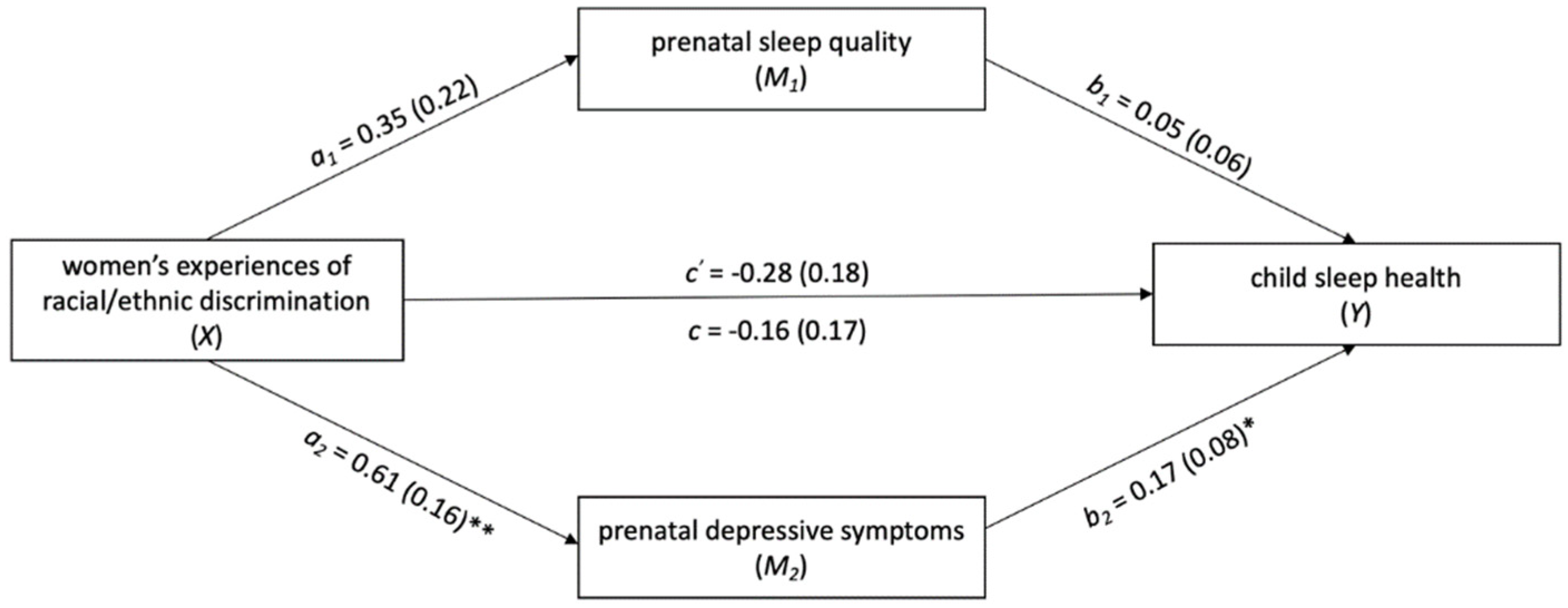
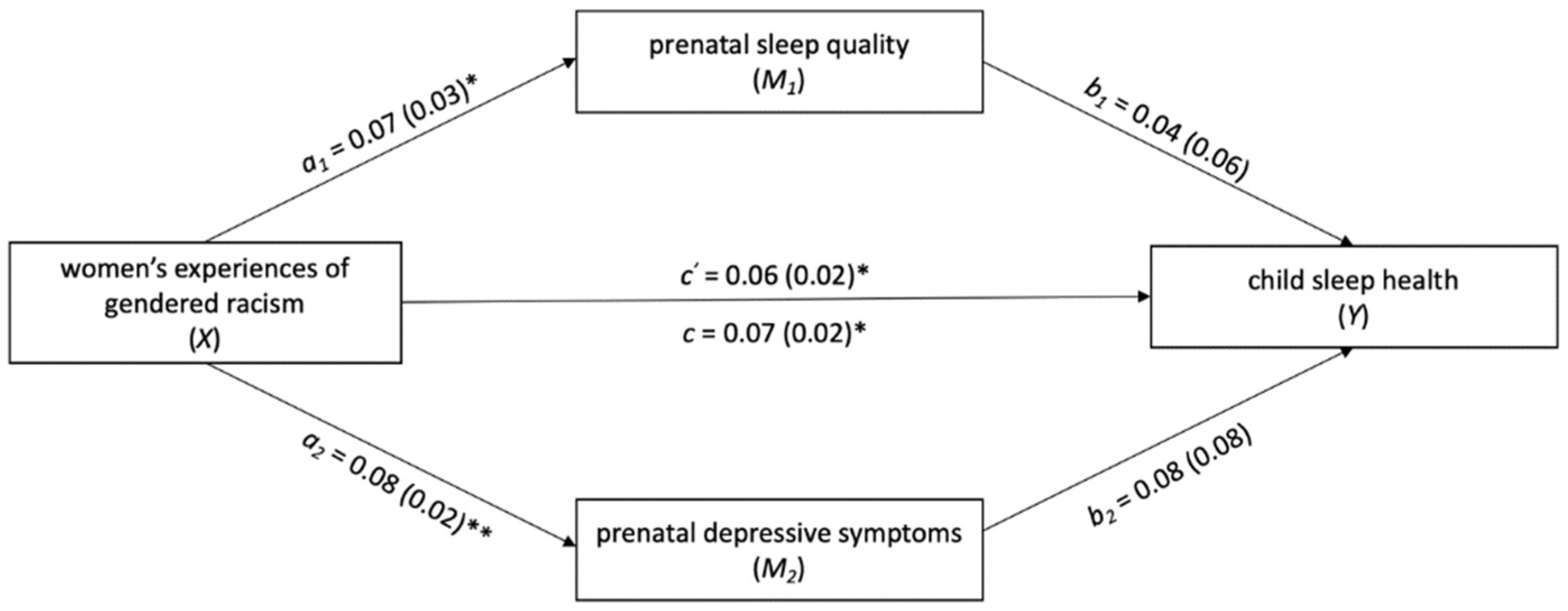
3.3. Examining Prenatal Sleep Quality and Prenatal Depressive Symptoms as Potential Mediators in the Association between Women’s Exposure to Discrimination and Child Sleep Health
3.4. Sensitivity Analyses
4. Discussion
4.1. Limitations
4.2. Strengths
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Williams, D.R.; Lawrence, J.A.; Davis, B.A.; Vu, C. Understanding how discrimination can affect health. Health Serv. Res. 2019, 54, 1374–1388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bowleg, L. The problem with the phrase women and minorities: Intersectionality-an important theoretical framework for public health. Am. J. Public Health 2012, 102, 1267–1273. [Google Scholar] [CrossRef] [PubMed]
- Crenshaw, K. Mapping the Margins: Intersectionality, Identity Politics, and Violence against Women of Color. Stanf. Law Rev. 1990, 43, 1241. [Google Scholar] [CrossRef]
- Lewis, J.A.; Williams, M.G.; Peppers, E.J.; Gadson, C.A. Applying intersectionality to explore the relations between gendered racism and health among black women. J. Couns. Psychol. 2017, 64, 475–486. [Google Scholar] [CrossRef] [PubMed]
- Lewis, T.T.; van Dyke, M.E. Discrimination and the Health of African Americans: The Potential Importance of Intersectionalities. Curr. Dir. Psychol. Sci. 2018, 27, 176–182. [Google Scholar] [CrossRef]
- Essed, P. Understanding Everyday Racism: An Interdisciplinary Theory; SAGE Publications: Newberry Park, CA, USA, 1991; Volume 2. [Google Scholar]
- Ertel, K.A.; James-Todd, T.; Kleinman, K.; Krieger, N.; Gillman, M.; Wright, R.; Rich-Edwards, J. Racial discrimination, response to unfair treatment, and depressive symptoms among pregnant black and African American women in the United States. Ann. Epidemiol. 2012, 22, 840–846. [Google Scholar] [CrossRef] [Green Version]
- Barker, D.J.P. Fetal origins of coronary heart disease. BMJ 1992, 311, 171–174. [Google Scholar] [CrossRef]
- Kinsella, M.T.; Monk, C. Impact of maternal stress, depression and anxiety on fetal neurobehavioral development. Clin. Obstet. Gynecol. 2009, 52, 425–440. [Google Scholar] [CrossRef] [Green Version]
- Giurgescu, C.; McFarlin, B.L.; Lomax, J.; Craddock, C.; Albrecht, A. Racial discrimination and the Black-White Gap in adverse birth outcomes: A review. J. Midwifery Women’s Health 2011, 56, 362–370. [Google Scholar] [CrossRef] [Green Version]
- Mustillo, S.; Krieger, N.; Gunderson, E.P.; Sidney, S.; Mccreath, H.; Kiefe, C.I. Self-reported experiences of racial discrimination and black-white differences in preterm and low-birthweight deliveries: The CARDIA study. Am. J. Public Health 2004, 94, 2125–2131. [Google Scholar] [CrossRef]
- Lu, M.C.; Kotelchuck, M.; Hogan, V.; Jones, L.; Wright, K.; Halfon, N. Closing the Black-White gap in birth outcomes: A life-course approach. Ethn. Dis. 2010, 20 (Suppl. 2), 62–76. [Google Scholar] [CrossRef]
- Sadeh, A.; Mindell, J.A.; Owens, J. Why care about sleep of infants and their parents? Sleep Med. Rev. 2011, 15, 335–337. [Google Scholar] [CrossRef]
- Powell, C.A.; Rifas-Shiman, S.L.; Oken, E.; Krieger, N.; Rich-Edwards, J.W.; Redline, S.; Taveras, E.M. Maternal experiences of racial discrimination and offspring sleep in the first 2 years of life: Project Viva cohort, Massachusetts, USA (1999–2002). Sleep Health 2020, 6, 463–468. [Google Scholar] [CrossRef] [PubMed]
- Carskadon, M.A.; Dement, W.C. Chapter 2—Normal Human Sleep: An Overview. In Principles and Practice of Sleep Medicine, 5th ed.; Saunders/Elsevier: Philadelphia, PA, USA, 2011. [Google Scholar]
- Meltzer, L.J.; Williamson, A.A.; Mindell, J.A. Pediatric sleep health: It matters, and so does how we define it. Sleep Med. Rev. 2021, 57, 101425. [Google Scholar] [CrossRef] [PubMed]
- Earnshaw, V.A.; Rosenthal, L.; Lewis, J.B.; Stasko, E.C.; Tobin, J.N.; Lewis, T.T.; Reid, A.E.; Ickovics, J.R. Maternal experiences with everyday discrimination and infant birth weight: A test of mediators and moderators among young, urban women of color. Ann. Behav. Med. 2013, 45, 13–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Francis, B.; Klebanoff, M.; Oza-Frank, R. Racial discrimination and perinatal sleep quality. Sleep Health 2017, 3, 300–305. [Google Scholar] [CrossRef]
- Cohen, M.F.; Corwin, E.J.; Johnson, D.A.; Dunn Amore, A.; Brown, A.L.; Barbee, N.R.; Brennan, P.A.; Dunlop, A.L. Discrimination is Associated with Poor Sleep Quality in Pregnant Black American Women. 2022, unpublished manuscript under review. [Google Scholar]
- O’Connor, T.G.; Caprariello, P.; Blackmore, E.R.; Gregory, A.M.; Glover, V.; Fleming, P. Prenatal mood disturbance predicts sleep problems in infancy and toddlerhood. Early Hum. Dev. 2007, 83, 451–458. [Google Scholar] [CrossRef] [Green Version]
- Palagini, L.; Drake, C.L.; Gehrman, P.; Meerlo, P.; Riemann, D. Early-life origin of adult insomnia: Does prenatal-early-life stress play a role? Sleep Med. 2015, 16, 446–456. [Google Scholar] [CrossRef]
- Santangeli, O.; Lehtikuja, H.; Palomäki, E.; Wigren, H.-K.; Paunio, T.; Porkka-Heiskanen, T. Sleep and Behavior in Cross-Fostering Rats: Developmental and Sex Aspects. Sleep 2016, 39, 2211–2221. [Google Scholar] [CrossRef] [Green Version]
- Dugovic, C.; Maccari, S.; Weibel, L.; Turek, F.W.; van Reeth, O. High corticosterone levels in prenatally stressed rats predict persistent paradoxical sleep alterations. J. Neurosci. 1999, 19, 8656–8664. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Field, T.; Diego, M.; Hernandez-Reif, M.; Figueiredo, B.; Schanberg, S.; Kuhn, C. Sleep disturbances in depressed pregnant women and their newborns. Infant Behav. Dev. 2007, 30, 127–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jenni, O.G.; Carskadon, M.A. Sleep behavior and sleep regulation from infancy through adolescence: Normative aspects. Sleep Med. Clin. 2012, 7, 529–538. [Google Scholar] [CrossRef]
- Armitage, R.; Flynn, H.; Hoffmann, R.; Vazquez, D.; Lopez, J.; Marcus, S. Early developmental changes in sleep in infants: The impact of maternal depression. Sleep 2009, 32, 693–696. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, Y.; Bird, A.; Peterson, E.; Underwood, L.; Morton, S.M.B.; Grant, C.C. Maternal Antenatal Depression and Early Childhood Sleep: Potential Pathways through Infant Temperament. J. Pediatr. Psychol. 2020, 45, 203–217. [Google Scholar] [CrossRef]
- Alvidrez, J.; Castille, D.; Laude-Sharp, M.; Rosario, A.; Tabor, D. The National Institute on Minority Health and Health Disparities Research Framework. Am. J. Public Health 2019, 109, S16–S20. [Google Scholar] [CrossRef]
- Newland, R.P.; Parade, S.H.; Dickstein, S.; Seifer, R. Goodness of fit between prenatal maternal sleep and infant sleep: Associations with maternal depression and attachment security. Infant Behav. Dev. 2017, 44, 179–188. [Google Scholar] [CrossRef] [Green Version]
- Tomfohr, L.M.; Buliga, E.; Letourneau, N.L.; Campbell, T.S.; Giesbrecht, G.F. Trajectories of Sleep Quality and Associations with Mood during the Perinatal Period. Sleep 2015, 38, 1237–1245. [Google Scholar] [CrossRef] [Green Version]
- Hayes, A.F.; Rockwood, N.J. Regression-based statistical mediation and moderation analysis in clinical research: Observations, recommendations, and implementation. Behav. Res. Ther. 2017, 98, 39–57. [Google Scholar] [CrossRef]
- Corwin, E.J.; Hogue, C.J.; Pearce, B.; Hill, C.C.; Read, T.D.; Mulle, J.; Dunlop, A.L. Protocol for the Emory University African American Vaginal, Oral, and Gut Microbiome in Pregnancy Cohort Study. BMC Pregnancy Childbirth 2017, 17, 161. [Google Scholar] [CrossRef]
- World Health Organization. Preterm Birth. 2018. Available online: https://www.who.int/news-room/fact-sheets/detail/preterm-birth (accessed on 7 February 2022).
- Krieger, N.; Smith, K.; Naishadham, D.; Hartman, C.; Barbeau, E.M. Experiences of discrimination: Validity and reliability of a self-report measure for population health research on racism and health. Soc. Sci. Med. 2005, 61, 1576–1596. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jackson, F.M.; Hogue, C.R.; Phillips, M.T. The Development of a Race and Gender-Specific Stress Measure for African American Women: Jackson, Hogue, Phillips Contextualized Stress Measure. Ethn. Dis. 2005, 15, 594–600. [Google Scholar] [PubMed]
- Hendrix, C.L.; Dilks, D.D.; McKenna, B.G.; Dunlop, A.L.; Corwin, E.J.; Brennan, P.A. Maternal Childhood Adversity Associates with Frontoamygdala Connectivity in Neonates. Biol. Psychiatry Cogn. Neurosci. Neuroimaging 2021, 6, 470–478. [Google Scholar] [CrossRef] [PubMed]
- Cox, J.; Holden, J.; Sagovsky, R.; Wisner, K.; Parry, B.; Piontek, C. Edinburgh Postnatal Depression Scale (EDPS). Br. J. Psychiatry 1987, 150, 782–786. [Google Scholar] [CrossRef] [Green Version]
- Tandon, S.D.; Cluxton-Keller, F.; Leis, J.; Le, H.N.; Perry, D.F. A comparison of three screening tools to identify perinatal depression among low-income African American women. J. Affect. Disord. 2012, 136, 155–162. [Google Scholar] [CrossRef] [Green Version]
- Yu, L.; Buysse, D.J.; Germain, A.; Moul, D.E.; Stover, A.; Dodds, N.E.; Johnston, K.L.; Pilkonis, P.A. Development of Short Forms from the PROMISTM Sleep Disturbance and Sleep-Related Impairment Item Banks. Behav. Sleep Med. 2011, 10, 6–24. [Google Scholar] [CrossRef] [PubMed]
- Buysse, D.J.; Yu, L.; Moul, D.E.; Germain, A.; Stover, A.; Dodds, N.E.; Johnston, K.L.; Shablesky-Cade, M.A.; Pilkonis, P.A. Development and validation of patient-reported outcome measures for sleep disturbance and sleep-related impairments. Sleep 2010, 33, 781–792. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J.; Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Bei, B.; Pinnington, D.M.; Shen, L.; Blumfield, M.; Drummond, S.P.; Newman, L.K.; Manber, R. A scalable cognitive behavioural program to promote healthy sleep during pregnancy and postpartum periods: Protocol of a randomised controlled trial (the SEED project). BMC Pregnancy Childbirth 2019, 19, 254. [Google Scholar] [CrossRef]
- Mersky, J.P.; Lee, C.T.P.; Gilbert, R.M.; Goyal, D. Prevalence and Correlates of Maternal and Infant Sleep Problems in a Low-Income US Sample. Matern. Child Health J. 2020, 24, 196–203. [Google Scholar] [CrossRef]
- Nichd Seccyd. Children’s Sleep Habits Questionnaire (Abbreviated). Available online: https://njaap.org/wp-content/uploads/2016/04/Childrens-Sleep-Habits-Questionnaire.pdf (accessed on 28 February 2022).
- Bonuck, K.A.; Goodlin-Jones, B.L.; Schechter, C.; Owens, J. Modified Children’s sleep habits questionnaire for behavioral sleep problems: A validation study. Sleep Health 2017, 3, 136–141. [Google Scholar] [CrossRef] [PubMed]
- Oakes, J.M.; Rossi, P.H. The measurement of SES in health research: Current practice and steps toward a new approach. Soc. Sci. Med. 2003, 56, 769–784. [Google Scholar] [CrossRef]
- Cheng, P.; Cuellar, R.; Johnson, D.A.; Kalmbach, D.A.; Joseph, C.L.; Castelan, A.C.; Sagong, C.; Casement, M.D.; Drake, C.L. Racial discrimination as a mediator of racial disparities in insomnia disorder. Sleep Health 2020, 6, 543–549. [Google Scholar] [CrossRef] [PubMed]
- Gaston, S.A.; Feinstein, L.; Slopen, N.; Sandler, D.P.; Williams, D.R.; Jackson, C.L. Everyday and major experiences of racial/ethnic discrimination and sleep health in a multiethnic population of U.S. women: Findings from the Sister Study. Sleep Med. 2020, 71, 97–105. [Google Scholar] [CrossRef]
- Grandner, M.A.; Patel, N.P.; Gehrman, P.R.; Xie, D.; Sha, D.; Weaver, T.; Gooneratne, N. Who gets the best sleep? Ethnic and socioeconomic factors related to sleep complaints. Sleep Med. 2010, 11, 470–478. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chandler-Mather, N.; Occhipinti, S.; Donovan, C.; Shelton, D.; Dawe, S. An investigation of the link between prenatal alcohol exposure and sleep problems across childhood. Drug Alcohol Depend. 2021, 218, 108412. [Google Scholar] [CrossRef]
- Matricciani, L.; Paquet, C.; Galland, B.; Short, M.; Olds, T. Children’s sleep and health: A meta-review. Sleep Med. Rev. 2019, 46, 136–150. [Google Scholar] [CrossRef]
- Johnson, D.A.; Billings, M.E.; Hale, L. Environmental Determinants of Insufficient Sleep and Sleep Disorders: Implications for Population Health. Curr. Epidemiol. Rep. 2018, 5, 61–69. [Google Scholar] [CrossRef]
- IBM Corp. IBM SPSS Statistics for Macintosh; Version 26.0; IBM Software Business Analytics; IBM Corp: Armonk, NY, USA, 2019. [Google Scholar]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Appelbaum, M.; Cooper, H.; Kline, R.B.; Mayo-Wilson, E.; Nezu, A.M.; Rao, S.M. Journal article reporting standards for quantitative research in psychology: The APA Publications and Communications Board Task Force Report. Am. Psychol. 2018, 73, 947. [Google Scholar] [CrossRef]
- Hayes, A.F. The PROCESS macro for SPSS and SAS. 2016. Available online: https://Processmacro.org (accessed on 15 December 2021).
- Kane, L.; Ashbaugh, A.R. Simple and parallel mediation: A tutorial exploring anxiety sensitivity, sensation seeking, and gender. Quant. Methods Psychol. 2017, 13, 148–165. [Google Scholar] [CrossRef]
- Lin, W.; Wu, B.; Chen, B.; Lai, G.; Huang, S.; Li, S.; Liu, K.; Zhong, C.; Huang, W.; Yuan, S.; et al. Sleep Conditions Associate with Anxiety and Depression Symptoms among Pregnant Women during the Epidemic of COVID-19 in Shenzhen. J. Affect. Disord. 2021, 281, 567–573. [Google Scholar] [CrossRef] [PubMed]
- Lebel, C.; MacKinnon, A.; Bagshawe, M.; Tomfohr-Madsen, L.; Giesbrecht, G. Elevated depression and anxiety symptoms among pregnant individuals during the COVID-19 pandemic. J. Affect. Disord. 2020, 277, 5–13. [Google Scholar] [CrossRef]
- Dellagiulia, A.; Lionetti, F.; Fasolo, M.; Verderame, C.; Sperati, A.; Alessandri, G. Early impact of COVID-19 lockdown on children’s sleep: A 4-week longitudinal study. J. Clin. Sleep Med. 2020, 16, 1639–1640. [Google Scholar] [CrossRef]
- Nicholson, J.S.; Deboeck, P.R.; Howard, W. Attrition in developmental psychology: A review of modern missing data reporting and practices. Int. J. Behav. Dev. 2017, 41, 143–153. [Google Scholar] [CrossRef]
- Berry, O.O.; Tobón, A.L.; Njoroge, W.F.M. Social Determinants of Health: The Impact of Racism on Early Childhood Mental Health. Curr. Psychiatry Rep. 2021, 23, 23. [Google Scholar] [CrossRef]
- Heard-Garris, N.J.; Cale, M.; Camaj, L.; Hamati, M.C.; Dominguez, T.P. Transmitting Trauma: A systematic review of vicarious racism and child health. Soc. Sci. Med. 2018, 199, 230–240. [Google Scholar] [CrossRef]
- Glover, V. Prenatal stress and its effects on the fetus and the child: Possible underlying biological mechanisms. In Perinatal Programming of Neurodevelopment; Springer: New York, NY, USA, 2015; pp. 269–283. [Google Scholar]
- den Heuvel, V.I.M.; Hect, L.J.; Smarr, L.B.; Qawasmeh, T.; Kriegsfeld, J.L.; Barcelona, J.; Hijazi, E.K.; Thomason, E.M. Maternal stress during pregnancy alters fetal cortico-cerebellar connectivity in utero and increases child sleep problems after birth. Sci. Rep. 2021, 11, 2228. [Google Scholar] [CrossRef]
- Bei, B.; Pinnington, D.M.; Quin, N.; Shen, L.; Blumfield, M.; Wiley, J.F.; Drummond, S.P.; Newman, L.K.; Manber, R. Improving Maternal Sleep via a Scalable Cognitive Behavioural Intervention: Findings from a Randomised Controlled Trial from Pregnancy to Two Years Postpartum. Psychol. Med. 2021. [Google Scholar] [CrossRef]
- Sedov, I.D.; Cameron, E.E.; Madigan, S.; Tomfohr-Madsen, L.M. Sleep quality during pregnancy: A meta-analysis. Sleep Med. Rev. 2018, 38, 168–176. [Google Scholar] [CrossRef]
- Johnson, D.A.; Jackson, C.L.; Williams, N.J.; Alcántara, C. Are sleep patterns influenced by race/ethnicity—A marker of relative advantage or disadvantage? Evidence to date. Nat. Sci. Sleep 2019, 11, 79–95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McQuillan, M.E.; Bates, J.E.; Staples, A.D.; Deater-Deckard, K. Maternal stress, sleep, and parenting. J. Fam. Psychol. 2019, 33, 349–359. [Google Scholar] [CrossRef] [PubMed]
- Philbrook, L.E.; Teti, D.M. Bidirectional associations between bedtime parenting and infant sleep: Parenting quality, parenting practices, and their interaction. J. Fam. Psychol. 2016, 30, 431–441. [Google Scholar] [CrossRef]
- Sadeh, A.; Tikotzky, L.; Scher, A. Parenting and infant sleep. Sleep Med. Rev. 2010, 14, 89–96. [Google Scholar] [CrossRef]
- Taylor, J.K. Structural Racism and Maternal Health Among Black Women. J. Law Med. Ethics 2020, 48, 506–517. [Google Scholar] [CrossRef] [PubMed]
- Tomfohr-Madsen, L.; Cameron, E.E.; Dhillon, A.; MacKinnon, A.; Hernandez, L.; Madigan, S.; Tough, S. Neighborhood socioeconomic status and child sleep duration: A systematic review and meta-analysis. Sleep Health 2020, 6, 550–562. [Google Scholar] [CrossRef]
- MacKinnon, A.L.; Tomfohr-Madsen, L.; Tough, S. Neighborhood Socio-Economic Factors and Associations with Infant Sleep Health. Behav. Sleep Med. 2020, 19, 458–470. [Google Scholar] [CrossRef]
- Grimes, M.; Camerota, M.; Propper, C.B. Neighborhood deprivation predicts infant sleep quality. Sleep Health 2019, 5, 148–151. [Google Scholar] [CrossRef]
- Goodman, S.H.; Gotlib, I.H. Risk for psychopathology in the children of depressed mothers: A developmental model for understanding mechanisms of transmission. Psychol. Rev. 1999, 106, 458–490. [Google Scholar] [CrossRef]
- Gee, G.C.; Walsemann, K.M.; Brondolo, E. A life course perspective on how racism may be related to health inequities. Am. J. Public Health 2012, 102, 967–974. [Google Scholar] [CrossRef]
- Picklesimer, A.H.; Billings, D.; Hale, N.; Blackhurst, D.; Covington-Kolb, S. The effect of CenteringPregnancy group prenatal care on preterm birth in a low-income population. Am. J. Obstet. Gynecol. 2012, 206, 415.e1–415.e7. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | Imputed Data (N = 205) |
|---|---|
| M (SD) or n (%) | |
| Maternal Age (years) | 25.11 (4.75) |
| Primiparous Women | 76 (37.1%) |
| In a Relationship and Cohabitating | 98 (47.8%) |
| Education | - |
| 8th Grade or Less | 1 (0.5%) |
| Some High School | 36 (17.6%) |
| Graduated High School or GED | 81 (39.5%) |
| Some College or Technical School | 52 (25.4%) |
| Graduated College | 26 (12.7%) |
| Some Graduate Work or Degree | 9 (4.4%) |
| Income | - |
| <100% of the Federal Poverty Level | 97 (47.3%) |
| 100–132% of the Federal Poverty Level | 37 (18.0%) |
| 133–149% of the Federal Poverty Level | 11 (5.4%) |
| 150–199% of the Federal Poverty Level | 24 (11.7%) |
| 200–299% of the Federal Poverty Level | 19 (9.3%) |
| 300–399% of the Federal Poverty Level | 6 (2.9%) |
| ≥400% of the Federal Poverty Level | 11 (5.4%) |
| Prenatal Substance Use | - |
| Tobacco | 30 (14.6%) |
| Alcohol | 14 (6.8%) |
| Racial/Ethnic Discrimination (EOD) a | 2.09 (2.28) |
| Gendered Racial Stress (JHP) b | 96.45 (19.57) |
| Maternal Depressive Symptoms (EPDS) c, mid-pregnancy | 7.54 (5.64) |
| Maternal Sleep Quality (PROMIS) d, mid-pregnancy | 21.78 (7.16) |
| Gestational Weeks at Birth | 38.69 (1.52) |
| Child Sex | 102 female (49.8%) |
| Child Age (months) | 25.84 (2.76) |
| Child Sleep Health (CSHQ), age two e | 36.34 (5.43) |
| Maternal Depressive Symptoms (EPDS), child age two | 5.58 (4.85) |
| Number of People in the Home, child age two | 4.34 (1.60) |
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| (1) Maternal Age | - | ||||||||||
| (2) SES | 0.42 ** | - | |||||||||
| (3) Prenatal Tobacco Use | 0.01 | −0.18 * | - | ||||||||
| (4) Prenatal Alcohol Use | 0.15 * | 0.06 | 0.33 ** | - | |||||||
| (5) Racial/Ethnic Discrimination | 0.11 | 0.16 * | 0.04 | 0.09 | - | ||||||
| (6) Gendered Racial Stress | 0.12 | −0.06 | 0.05 | 0.15 * | 0.26 ** | - | |||||
| (7) Sleep Quality, mid-pregnancy | 0.13 | 0.09 | 0.07 | 0.03 | 0.18 ** | 0.23 ** | - | ||||
| (8) Depressive Symptoms, mid-pregnancy | 0.02 | −0.02 | 0.10 | 0.07 | 0.31 ** | 0.36 ** | 0.44 ** | - | |||
| (9) Child Sleep Health | 0.11 | −0.03 | 0.07 | 0.04 | −0.02 | 0.27 ** | 0.15 ** | 0.20 ** | - | ||
| (10) Child Age (in months, age two) | −0.06 | 0.05 | −0.09 | −0.13 | 0.01 | 0.03 | 0.19 ** | 0.12 | −0.07 | - | |
| (11) Number of People in the Home, child age two | −0.02 | −0.25 ** | −0.01 | −0.02 | 0.03 | −0.09 | 0.01 | −0.06 | 0.03 | 0.02 | - |
| (12) Maternal Depressive Symptoms, child age two | 0.001 | −0.03 | 0.06 | −0.10 | 0.20 ** | 0.20 ** | 0.26 ** | 0.40 ** | 0.15 * | 0.13 | 0.08 |
| B (SE) | 95% CI (B) | β | t | p | |
|---|---|---|---|---|---|
| Model 1. Unadjusted Effects of Racial/ Ethnic Discrimination | −0.05 (0.17) | [−0.38–0.28] | −0.02 | −0.31 | 0.76 |
| Model 2. Effects of Racial/Ethnic Discrimination + adjustment for maternal age, SES, prenatal substance use, child age, number of people in the home at child age two | −0.07 (0.17) | [−0.41–0.27] | −0.03 | −0.41 | 0.68 |
| Model 3. Effects of Racial/Ethnic Discrimination + adjustment for maternal age, SES, prenatal substance use, child age, number of people in the home at child age two, maternal depressive symptoms at child age two | −0.16 (0.17) | [−0.50–0.19] | −0.07 | −0.90 | 0.37 |
| B (SE) | 95% CI (B) | β | t | p | |
|---|---|---|---|---|---|
| Model 1. Unadjusted Effects of Gendered Racial Stress | 0.07 (0.02) | [0.04–0.11] | 0.27 | 3.92 | <0.001 |
| Model 2. Effects of Gendered Racial Stress + adjustment for maternal age, SES, prenatal substance use, child age, number of people in the home at child age two | 0.07 (0.02) | [0.04–0.11] | 0.26 | 3.75 | <0.001 |
| Model 3. Effects of Gendered Racial Stress + adjustment for maternal age, SES, prenatal substance use, child age, number of people in the home at child age two, maternal depressive symptoms at child age two | 0.07 (0.02) | [0.03–0.11] | 0.24 | 3.34 | 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cohen, M.F.; Dunlop, A.L.; Johnson, D.A.; Dunn Amore, A.; Corwin, E.J.; Brennan, P.A. Intergenerational Effects of Discrimination on Black American Children’s Sleep Health. Int. J. Environ. Res. Public Health 2022, 19, 4021. https://doi.org/10.3390/ijerph19074021
Cohen MF, Dunlop AL, Johnson DA, Dunn Amore A, Corwin EJ, Brennan PA. Intergenerational Effects of Discrimination on Black American Children’s Sleep Health. International Journal of Environmental Research and Public Health. 2022; 19(7):4021. https://doi.org/10.3390/ijerph19074021
Chicago/Turabian StyleCohen, Madeleine F., Anne L. Dunlop, Dayna A. Johnson, Alexis Dunn Amore, Elizabeth J. Corwin, and Patricia A. Brennan. 2022. "Intergenerational Effects of Discrimination on Black American Children’s Sleep Health" International Journal of Environmental Research and Public Health 19, no. 7: 4021. https://doi.org/10.3390/ijerph19074021