
Slow-Wave EEG Activity Correlates with Impaired Inhibitory Control in Internet Addiction Disorder

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Measures
2.2.1. Internet Addiction and Impulsivity
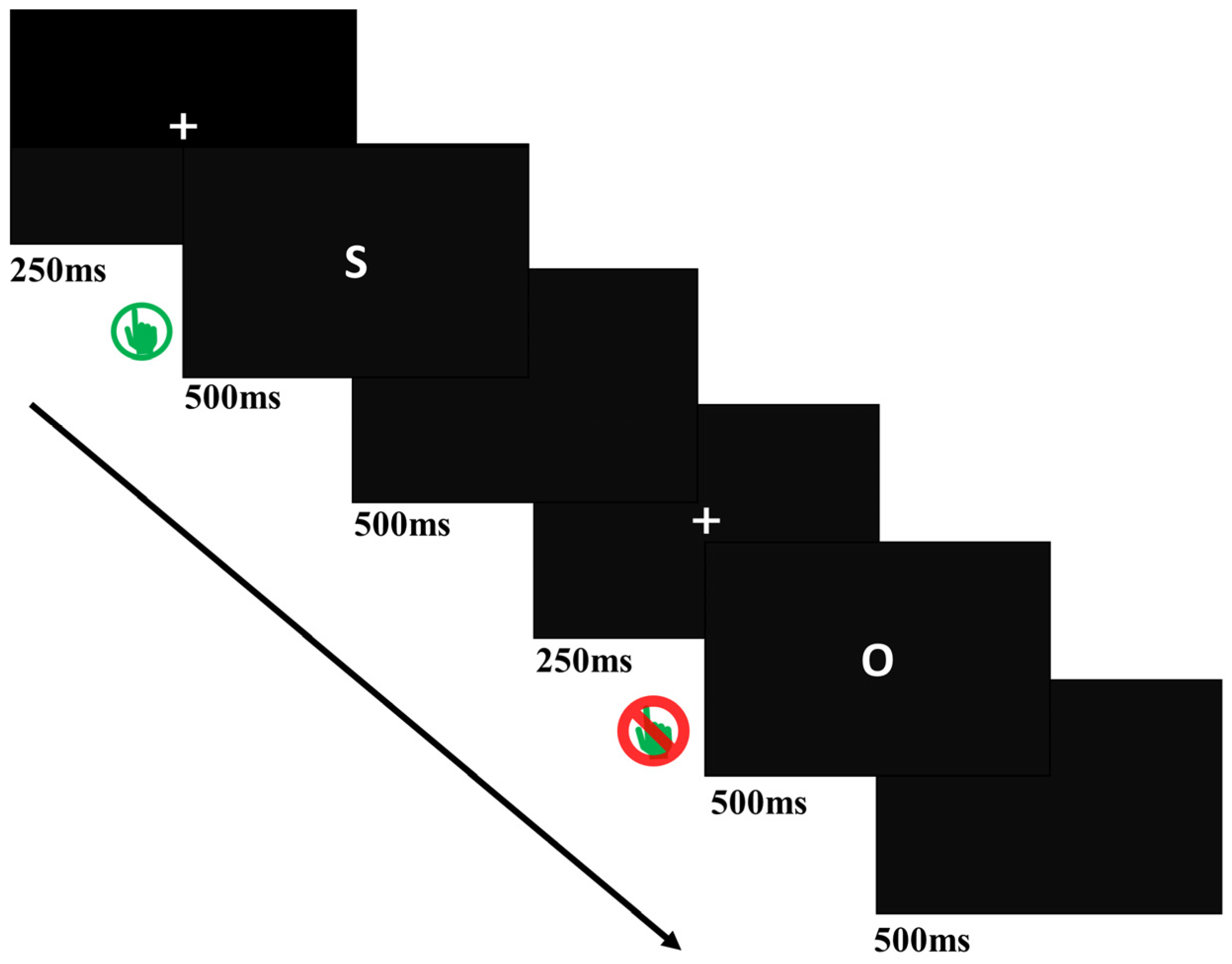
2.2.2. Go/NoGo Task
2.3. Procedure
2.4. EEG Recording and Pre-Processing
2.5. Statistical Analysis
2.5.1. Behavior Data
2.5.2. Resting-State EEG Data
3. Results
3.1. Behavioral Results
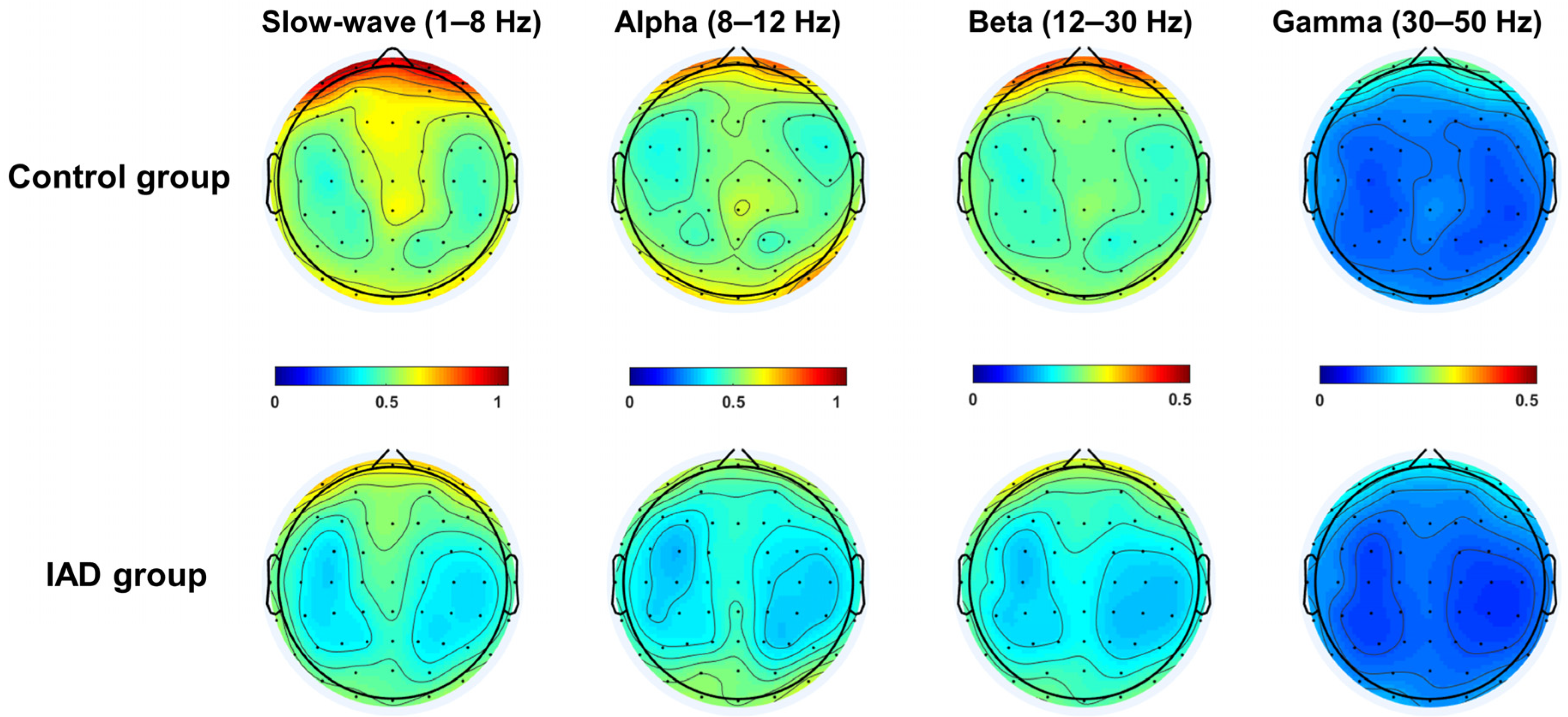
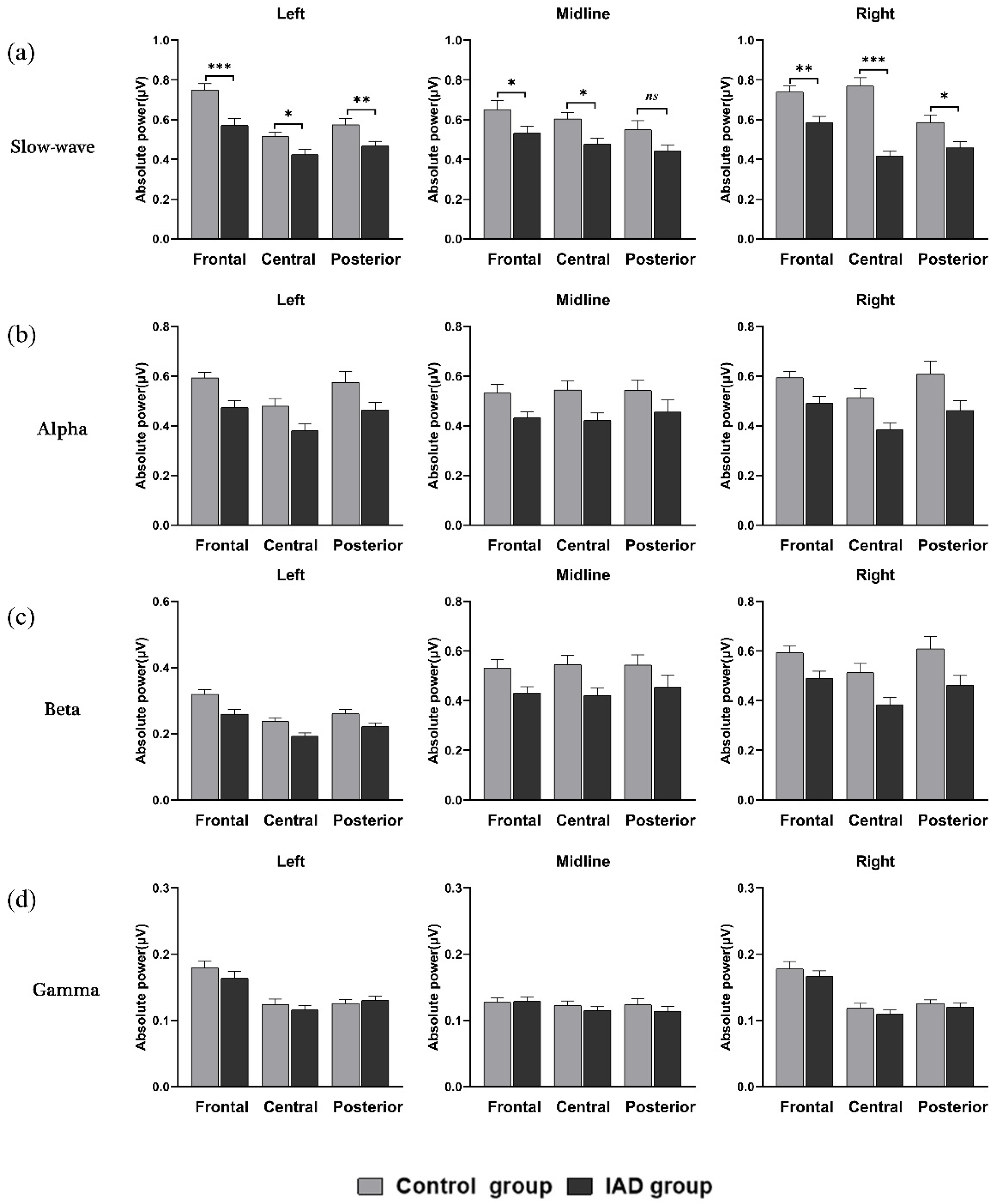
3.2. Resting-State Data Results
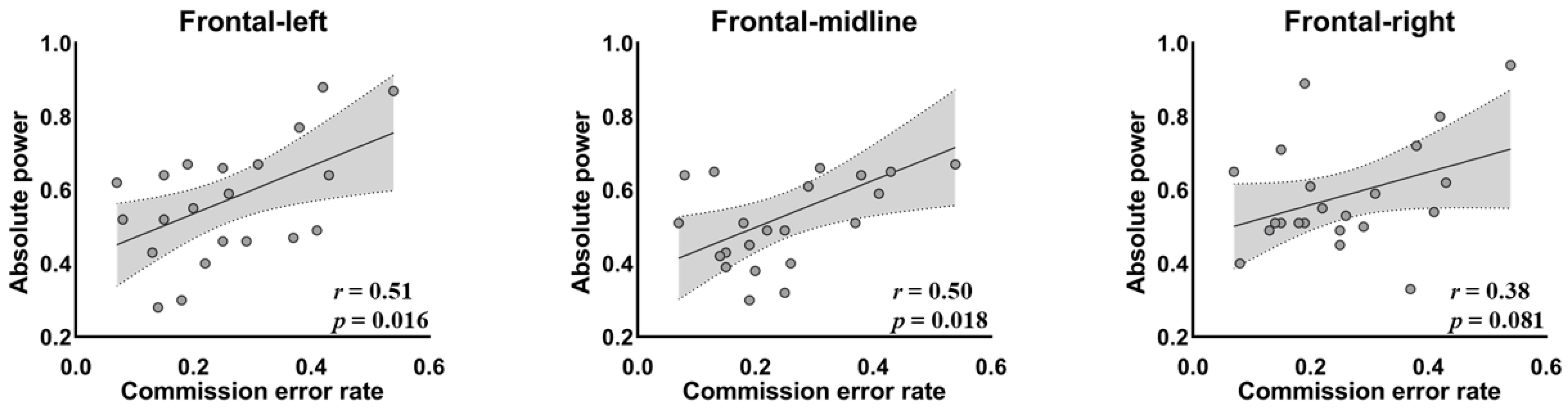
3.3. Correlation between Behavioral Variables and Frontal EEG Activity
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cheng, C.; Li, A.Y.-L. Internet Addiction Prevalence and Quality of (Real) Life: A Meta-Analysis of 31 Nations across Seven World Regions. Cyberpsychol. Behav. Soc. Netw. 2014, 17, 755–760. [Google Scholar] [CrossRef] [Green Version]
- Dong, G.; DeVito, E.E.; Du, X.; Cui, Z. Impaired inhibitory control in ‘internet addiction disorder’: A functional magnetic resonance imaging study. Psychiatry Res. Neuroimaging 2012, 203, 153–158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turel, O.; Qahri-Saremi, H. Explaining unplanned online media behaviors: Dual system theory models of impulsive use and swearing on social networking sites. New Media Soc. 2018, 20, 3050–3067. [Google Scholar] [CrossRef]
- Young, K.S.; Rogers, R.C. The Relationship between Depression and Internet Addiction. CyberPsychol. Behav. 1998, 1, 25–28. [Google Scholar] [CrossRef] [Green Version]
- Lewczuk, K.; Nowakowska, I.; Lewandowska, K.; Potenza, M.N.; Gola, M. Frequency of use, moral incongruence and religiosity and their relationships with self-perceived addiction to pornography, internet use, social networking and online gaming. Addiction 2021, 116, 889–899. [Google Scholar] [CrossRef] [PubMed]
- Turel, O.; Bechara, A. A Triple-System Neural Model of Maladaptive Consumption. J. Assoc. Consum. Res. 2021, 6, 324–333. [Google Scholar] [CrossRef]
- Zhang, J.; Chen, S.; Jiang, Q.; Dong, H.; Zhao, Z.; Du, X.; Dong, G.-H. Disturbed craving regulation to gaming cues in internet gaming disorder: Implications for uncontrolled gaming behaviors. J. Psychiatr. Res. 2021, 140, 250–259. [Google Scholar] [CrossRef]
- Dong, G.; Lu, Q.; Zhou, H.; Zhao, X. Impulse inhibition in people with Internet addiction disorder: Electrophysiological evidence from a Go/NoGo study. Neurosci. Lett. 2010, 485, 138–142. [Google Scholar] [CrossRef]
- We Are Social & Hootsuite, Digital 2021: The Latest Insights into the ‘State of Digital’ (2021-01-27). 2021. Available online: https://wearesocial.com/uk/blog/2021/01/digital-2021-uk/ (accessed on 5 January 2022).
- Turel, O. Potential ‘dark sides’ of leisure technology use in youth. Commun. ACM 2019, 62, 24–27. [Google Scholar] [CrossRef]
- Turel, O.; He, Q.; Xue, G.; Xiao, L.; Bechara, A. Examination of Neural Systems Sub-Serving Facebook “Addiction”. Psychol. Rep. 2014, 115, 675–695. [Google Scholar] [CrossRef]
- Guangming Ribao. The Problem of Teenagers’ Internet Addiction Urgently Needs the Attention of the Whole Society (2018-09-27). 2018. Available online: https://m.gmw.cn/toutiao/2018-09/27/content_121676282.htm (accessed on 5 January 2022).
- Bu, H.; Chi, X.; Qu, D. Prevalence and predictors of the persistence and incidence of adolescent internet addiction in Mainland China: A two-year longitudinal study. Addict. Behav. 2021, 122, 107039. [Google Scholar] [CrossRef] [PubMed]
- CINIC. The 48th Statistical Report on China’s Internet Development. 2021. Available online: http://www.cnnic.net.cn/hlwfzyj/hlwxzbg/hlwtjbg/202109/t20210915_71543.htm (accessed on 5 December 2021).
- Pontes, H.M.; Szabo, A.D.; Griffiths, M. The impact of Internet-based specific activities on the perceptions of Internet addiction, quality of life, and excessive usage: A cross-sectional study. Addict. Behav. Rep. 2015, 1, 19–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yan, W.; Li, Y.; Sui, N. The Relationship between Recent Stressful Life Events, Personality Traits, Perceived Family Functioning and Internet Addiction among College Students. Stress Health 2014, 30, 3–11. [Google Scholar] [CrossRef] [PubMed]
- Gao, X.; Zhang, M.; Yang, Z.; Wen, M.; Huang, H.; Zheng, R.; Wang, W.; Wei, Y.; Cheng, J.; Han, S.; et al. Structural and Functional Brain Abnormalities in Internet Gaming Disorder and Attention-Deficit/Hyperactivity Disorder: A Comparative Meta-Analysis. Front. Psychiatry 2021, 12, 679437. [Google Scholar] [CrossRef]
- Heuer, A.; Mennig, M.; Schubö, A.; Barke, A. Impaired disengagement of attention from computer-related stimuli in Internet Gaming Disorder: Behavioral and electrophysiological evidence. J. Behav. Addict. 2021, 10, 77–87. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.-M.; Lee, J.; Choi, A.R.; Chung, S.J.; Park, M.; Koo, J.W.; Kang, U.G.; Choi, J.-S. Event-related brain response to visual cues in individuals with Internet gaming disorder: Relevance to attentional bias and decision-making. Transl. Psychiatry 2021, 11, 258. [Google Scholar] [CrossRef]
- Zhou, Z.; Zhou, H.; Zhu, H. Working memory, executive function and impulsivity in Internet-addictive disorders: A comparison with pathological gambling. Acta Neuropsychiatr. 2015, 28, 92–100. [Google Scholar] [CrossRef]
- Antons, S.; Matthias, B. Inhibitory control and problematic Internet-pornography use—The important balancing role of the insula. J. Behav. Addict. 2020, 9, 58–70. [Google Scholar] [CrossRef] [Green Version]
- Diamond, A. Executive Functions. Annu. Rev. Psychol. 2013, 64, 135–168. [Google Scholar] [CrossRef] [Green Version]
- Kräplin, A.; Scherbaum, S.; Kraft, E.-M.; Rehbein, F.; Bühringer, G.; Goschke, T.; Mößle, T. The role of inhibitory control and decision-making in the course of Internet gaming disorder. J. Behav. Addict. 2021, 9, 990–1001. [Google Scholar] [CrossRef]
- Dieter, J.; Hoffmann, S.; Mier, D.; Reinhard, I.; Beutel, M.; Vollstädt-Klein, S.; Kiefer, F.; Mann, K.; Leménager, T. The role of emotional inhibitory control in specific internet addiction—An fMRI study. Behav. Brain Res. 2017, 324, 1–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, J.-S.; Park, S.M.; Roh, M.-S.; Lee, J.-Y.; Park, C.-B.; Hwang, J.Y.; Gwak, A.R.; Jung, H.Y. Dysfunctional inhibitory control and impulsivity in Internet addiction. Psychiatry Res. 2014, 215, 424–428. [Google Scholar] [CrossRef] [PubMed]
- Le, T.M.; Potvin, S.; Zhornitsky, S.; Li, C.-S.R. Distinct patterns of prefrontal cortical disengagement during inhibitory control in addiction: A meta-analysis based on population characteristics. Neurosci. Biobehav. Rev. 2021, 127, 255–269. [Google Scholar] [CrossRef] [PubMed]
- Hong, S.-B.; Zalesky, A.; Cocchi, L.; Fornito, A.; Choi, E.-J.; Kim, H.-H.; Suh, J.-E.; Kim, C.-D.; Kim, J.-W.; Yi, S.-H. Decreased Functional Brain Connectivity in Adolescents with Internet Addiction. PLoS ONE 2013, 8, e57831. [Google Scholar] [CrossRef] [Green Version]
- Liu, J.; Esmail, F.; Li, L.; Kou, Z.; Li, W.; Gao, X.; Wang, Z.; Tan, C.; Zhang, Y.; Zhou, S. Decreased frontal lobe function in people with Internet addiction disorder. Neural Regen. Res. 2013, 8, 3225. [Google Scholar] [CrossRef]
- Liu, J.; Li, W.; Zhou, S.; Zhang, L.; Wang, Z.; Zhang, Y.; Jiang, Y.; Li, L. Functional characteristics of the brain in college students with internet gaming disorder. Brain Imaging Behav. 2016, 10, 60–67. [Google Scholar] [CrossRef]
- Zhu, Y.; Zhang, H.; Tian, M. Molecular and Functional Imaging of Internet Addiction. BioMed Res. Int. 2015, 2015, 378675. [Google Scholar] [CrossRef]
- Ko, C.-H.; Hsiao, S.; Liu, G.-C.; Yen, J.-Y.; Yang, M.-J.; Yen, C.-F. The characteristics of decision making, potential to take risks, and personality of college students with Internet addiction. Psychiatry Res. 2010, 175, 121–125. [Google Scholar] [CrossRef]
- He, Q.; Turel, O.; Brevers, D.; Bechara, A. Excess social media use in normal populations is associated with amygdala-striatal but not with prefrontal morphology. Psychiatry Res. Neuroimaging 2017, 269, 31–35. [Google Scholar] [CrossRef]
- Luijten, M.; Machielsen, M.; Veltman, D.; Hester, R.; de Haan, L.; Franken, I. Systematic review of ERP and fMRI studies investigating inhibitory control and error processing in people with substance dependence and behavioural addictions. J. Psychiatry Neurosci. 2014, 39, 149–169. [Google Scholar] [CrossRef] [Green Version]
- Gao, L.; Zhang, J.; Xie, H.; Nie, Y.; Zhao, Q.; Zhou, Z. Effect of the mobile phone-related background on inhibitory control of problematic mobile phone use: An event-related potentials study. Addict. Behav. 2020, 108, 106363. [Google Scholar] [CrossRef]
- Zhou, Y.; Yao, M.; Fang, S.; Gao, X. A dual-process perspective to explore decision making in internet gaming disorder: An ERP study of comparison with recreational game users. Comput. Hum. Behav. 2021, 128, 107104. [Google Scholar] [CrossRef]
- Choi, J.-S.; Park, S.M.; Lee, J.; Hwang, J.Y.; Jung, H.Y.; Choi, S.-W.; Kim, D.J.; Oh, S.; Lee, J.-Y. Resting-state beta and gamma activity in Internet addiction. Int. J. Psychophysiol. 2013, 89, 328–333. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.J.; Lee, J.-Y.; Oh, S.; Park, M.; Jung, H.Y.; Sohn, B.K.; Choi, S.-W.; Kim, D.J.; Choi, J.-S. Associations between prospective symptom changes and slow-wave activity in patients with Internet gaming disorder: A resting-state EEG study. Medicine 2017, 96, e6178. [Google Scholar] [CrossRef] [PubMed]
- Burleigh, T.; Griffiths, M.D.; Sumich, A.; Wang, G.Y.; Kuss, D.J. Gaming disorder and internet addiction: A systematic review of resting-state EEG studies. Addict. Behav. 2020, 107, 106429. [Google Scholar] [CrossRef]
- Cavanagh, J.F.; Zambrano-Vazquez, L.; Allen, J.J.B. Theta lingua franca: A common mid-frontal substrate for action monitoring processes. Psychophysiology 2012, 49, 220–238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huster, R.J.; Enriquez-Geppert, S.; Lavallee, C.F.; Falkenstein, M.; Herrmann, C.S. Electroencephalography of response inhibition tasks: Functional networks and cognitive contributions. Int. J. Psychophysiol. 2013, 87, 217–233. [Google Scholar] [CrossRef] [PubMed]
- Harper, J.; Malone, S.M.; Bernat, E.M. Theta and delta band activity explain N2 and P3 ERP component activity in a go/no-go task. Clin. Neurophysiol. 2014, 125, 124–132. [Google Scholar] [CrossRef] [Green Version]
- Messel, M.S.; Raud, L.; Hoff, P.K.; Stubberud, J.; Huster, R.J. Frontal-midline theta reflects different mechanisms associated with proactive and reactive control of inhibition. NeuroImage 2021, 241, 118400. [Google Scholar] [CrossRef]
- Lee, J.Y.; Park, S.M.; Kim, Y.J.; Kim, D.J.; Choi, S.-W.; Kwon, J.S.; Choi, J.-S. Resting-state EEG activity related to impulsivity in gambling disorder. J. Behav. Addict. 2017, 6, 387–395. [Google Scholar] [CrossRef] [Green Version]
- Moretta, T.; Buodo, G. Response inhibition in problematic social network sites use: An ERP study. Cogn. Affect. Behav. Neurosci. 2021, 21, 868–880. [Google Scholar] [CrossRef] [PubMed]
- Bai, Y.; Fan, F.M. A Study on the Internet Dependence of College Students: The Revising and Applying of a Measurement. Psychol. Dev. Educ. 2005, 4, 99–104. [Google Scholar]
- Gao, F.Q.; Geng, J.Y.; Ren, Y.Q.; Yang, H.Y.; Han, L. Mediating effect of perceived social support and relative deprivation among life events and internet addiction in college students. Chin. Ment. Health J. 2017, 31, 734–738. [Google Scholar]
- Zhang, J.; Zhang, Y.J.; Shen, L.J. Attentional bias characteristics of different levels of over-users in mobile network under different time-course conditions. Chin. Ment. Health J. 2019, 33, 545–549. [Google Scholar]
- Cao, F.; Su, L.; Liu, T.; Gao, X. The relationship between impulsivity and Internet addiction in a sample of Chinese adolescents. Eur. Psychiatry 2007, 22, 466–471. [Google Scholar] [CrossRef]
- Mottram, A.J.; Fleming, M.J. Extraversion, Impulsivity, and Online Group Membership as Predictors of Problematic Internet Use. CyberPsychol. Behav. 2009, 12, 319–321. [Google Scholar] [CrossRef]
- Smith, G.T.; Fischer, S.; Cyders, M.A.; Annus, A.M.; Spillane, N.S.; McCarthy, D.M. On the Validity and Utility of Discriminating Among Impulsivity-Like Traits. Assessment 2007, 14, 155–170. [Google Scholar] [CrossRef]
- Whiteside, S.P.; Lynam, D.R. The Five Factor Model and impulsivity: Using a structural model of personality to understand impulsivity. Pers. Individ. Differ. 2001, 30, 669–689. [Google Scholar] [CrossRef]
- Delorme, A.; Makeig, S. EEGLAB: An Open Source Toolbox for Analysis of Single-Trial EEG Dynamics Including Independent Component Analysis. J. Neurosci. Methods 2004, 134, 9–21. [Google Scholar] [CrossRef] [Green Version]
- Thatcher, R.; North, D.; Biver, C. EEG and intelligence: Relations between EEG coherence, EEG phase delay and power. Clin. Neurophysiol. 2005, 116, 2129–2141. [Google Scholar] [CrossRef]
- Barry, R.J.; Clarke, A.R.; Johnstone, S. A review of electrophysiology in attention-deficit/hyperactivity disorder: I. Qualitative and quantitative electroencephalography. Clin. Neurophysiol. 2003, 114, 171–183. [Google Scholar] [CrossRef]
- Şalvarlı, I.; Griffiths, M.D. The Association between Internet Gaming Disorder and Impulsivity: A Systematic Review of Literature. Int. J. Ment. Health Addict. 2019, 20, 92–118. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.; Hwang, J.Y.; Park, S.M.; Jung, H.Y.; Choi, S.-W.; Kim, D.J.; Lee, J.-Y.; Choi, J.-S. Differential resting-state EEG patterns associated with comorbid depression in Internet addiction. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2014, 50, 21–26. [Google Scholar] [CrossRef]
- Wegmann, E.; Müller, S.M.; Turel, O.; Brand, M. Interactions of impulsivity, general executive functions, and specific inhibitory control explain symptoms of social-networks-use disorder: An experimental study. Sci. Rep. 2020, 10, 3866. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balconi, M.; Venturella, I.; Finocchiaro, R. Evidences from Rewarding System, FRN and P300 Effect in Internet-Addiction in Young People. Brain Sci. 2017, 7, 81. [Google Scholar] [CrossRef] [Green Version]
- Khanbabaei, S.; Abdollahi, M.H.; Shahgholian, M. The predictive role of working memory and impulsivity in internet addiction, an investigation about the mediating role of time perception. Pers. Individ. Differ. 2022, 185, 111280. [Google Scholar] [CrossRef]
- Lei, W.; Liu, K.; Chen, G.; Tolomeo, S.; Liu, C.; Peng, Z.; Liu, B.; Liang, X.; Huang, C.; Xiang, B.; et al. Blunted reward prediction error signals in internet gaming disorder. Psychol. Med. 2020, 1–10. [Google Scholar] [CrossRef]
- Darnai, G.; Perlaki, G.; Zsidó, A.N.; Inhóf, O.; Orsi, G.; Horváth, R.; Nagy, S.A.; Lábadi, B.; Tényi, D.; Kovács, N.; et al. Internet addiction and functional brain networks: Task-related fMRI study. Sci. Rep. 2019, 9, 15777. [Google Scholar] [CrossRef]
- Park, M.; Jung, M.H.; Lee, J.; Choi, A.R.; Chung, S.J.; Kim, B.; Kim, D.J.; Choi, J.-S. Neurophysiological and Cognitive Correlates of Error Processing Deficits in Internet Gaming Disorder. Cereb. Cortex 2020, 30, 4914–4921. [Google Scholar] [CrossRef]
- Ko, C.-H.; Hsieh, T.-J.; Chen, C.-Y.; Yen, C.-F.; Chen, C.-S.; Yen, J.-Y.; Wang, P.-W.; Liu, G.-C. Altered brain activation during response inhibition and error processing in subjects with Internet gaming disorder: A functional magnetic imaging study. Eur. Arch. Psychiatry Clin. Neurosci. 2014, 264, 661–672. [Google Scholar] [CrossRef]
- Ioannidis, K.; Hook, R.; Goudriaan, A.E.; Vlies, S.; Fineberg, N.A.; Grant, J.E.; Chamberlain, S.R. Cognitive deficits in problematic internet use: Meta-analysis of 40 studies. Br. J. Psychiatry 2019, 215, 639–646. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yuan, K.; Yu, D.; Bi, Y.; Wang, R.; Li, M.; Zhang, Y.; Dong, M.; Zhai, J.; Li, Y.; Lu, X.; et al. The left dorsolateral prefrontal cortex and caudate pathway: New evidence for cue-induced craving of smokers. Hum. Brain Mapp. 2017, 38, 4644–4656. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yuan, K.; Yu, D.; Cai, C.; Feng, D.; Li, Y.; Bi, Y.; Liu, J.; Zhang, Y.; Jin, C.; Li, L.; et al. Frontostriatal circuits, resting state functional connectivity and cognitive control in internet gaming disorder. Addict. Biol. 2017, 22, 813–822. [Google Scholar] [CrossRef] [PubMed]
- Yuan, K.; Yu, D.; Zhao, M.; Li, M.; Wang, R.; Li, Y.; Manza, P.; Shokri-Kojori, E.; Wiers, C.E.; Wang, G.J.; et al. Abnormal frontostriatal tracts in young male tobacco smokers. Neuroimage 2018, 183, 346–355. [Google Scholar] [CrossRef] [PubMed]
- Geng, X.; Hu, Y.; Gu, H.; Salmeron, B.J.; Adinoff, B.; Stein, E.A.; Yang, Y. Salience and default mode network dysregulation in chronic cocaine users predict treatment outcome. Brain 2017, 140, 1513–1524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, Y.; Salmeron, B.J.; Krasnova, I.N.; Gu, H.; Lu, H.; Bonci, A.; Cadet, J.L.; Stein, E.A.; Yang, Y. Compulsive drug use is associated with imbalance of orbitofrontal- and prelimbic-striatal circuits in punishment-resistant individuals. Proc. Natl. Acad. Sci. USA 2019, 116, 9066–9071. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Control (M ± SD) | IAD (M ± SD) | or t | p | Cohen’s d | |
|---|---|---|---|---|---|
| Gender (male/female) | 9/14 | 8/14 | 1.000 | - | |
| Age(year) | 19.26 ± 0.92 | 19.64 ± 1.26 | t(43) = −1.15 | 0.256 | 0.35 |
| CIAS-R | 38.00 ± 5.89 | 63.36 ± 6.58 | t(43) = −13.64 | <0.001 | 4.07 |
| UPPS-P | 124.78 ± 18.31 | 145.59 ± 28.03 | t(43) = −2.96 | 0.005 | 0.88 |
| NU | 26.74 ± 5.96 | 33.50 ± 6.04 | t(43) = −3.78 | <0.001 | 1.13 |
| PU | 29.48 ± 8.08 | 34.14 ± 8.45 | t(42.65) = −1.89 | 0.065 | 0.56 |
| SS | 27.65 ± 7.23 | 28.59 ± 9.64 | t(43) = −0.37 | 0.713 | 0.11 |
| Lack of Premeditation | 20.78 ± 4.04 | 22.77 ± 6.72 | t(34.17) = −1.20 | 0.233 | 0.36 |
| Lack of Perseverance | 20.13 ± 3.42 | 26.59 ± 6.22 | t(43) = −4.35 | <0.001 | 1.30 |
| Control (M ± SD) (n = 23) | IAD (M ± SD) (n = 22) | t/F | p | Cohen’s d or | |
|---|---|---|---|---|---|
| Go RTs (ms) | 336.61 ± 20.59 | 318.98 ± 27.09 | t(43) = 2.46 | 0.018 | 0.74 |
| NoGo error RTs (ms) | 289.19 ± 19.58 | 274.84 ± 25.40 | t(43) = 2.13 | 0.039 | 0.64 |
| Omission error rate | 0.03 ± 0.02 | 0.02 ± 0.02 | F (1, 43) = 3.55 | 0.066 | 0.08 |
| Commission error rate | 0.16 ± 0.10 | 0.25 ± 0.13 | F (1, 43) = 8.91 | 0.005 | 0.17 |
| Position | MControl | SDControl | MIAD | SDIAD | Conhen’s d |
|---|---|---|---|---|---|
| F-L | 0.75 | 0.15 | 0.57 | 0.16 | 1.16 |
| F-M | 0.65 | 0.22 | 0.53 | 0.16 | 0.62 |
| F-R | 0.74 | 0.15 | 0.58 | 0.15 | 1.06 |
| C-L | 0.51 | 0.11 | 0.42 | 0.13 | 0.75 |
| C-M | 0.60 | 0.15 | 0.48 | 0.14 | 0.83 |
| C-R | 0.77 | 0.20 | 0.42 | 0.11 | 2.17 |
| P-L | 0.57 | 0.15 | 0.47 | 0.10 | 0.78 |
| P-M | 0.55 | 0.21 | 0.44 | 0.15 | 0.60 |
| P-R | 0.59 | 0.18 | 0.46 | 0.14 | 0.81 |
| Absolute Power (μV) | F | p | Post Hoc | |
|---|---|---|---|---|
| Slow-wave (1–8 Hz) | ||||
| Groups | 20.76 | <0.001 | 0.33 | |
| Groups × Regions | 4.04 | 0.022 | 0.09 | Control > IAD in all regions; Control: F > C > P; IAD: F > C, P |
| Groups × Sites | 6.43 | 0.004 | 0.13 | Control > IAD in all sites; Control: R > L, M; IAD: N.S. |
| Groups× Regions × Sites | 5.12 | 0.002 | 0.11 | Except for P-M, Control > IAD in other regions |
| Alpha (8–12 Hz) | ||||
| Groups | 9.45 | 0.003 | 0.19 | |
| Groups × Regions | 0.05 | 0.93 | 0.001 | |
| Groups × Sites | 0.40 | 0.664 | 0.01 | |
| Groups × Regions × Sites | 0.33 | 0.571 | 0.01 | |
| Beta (12–30 Hz) | ||||
| Groups | 16.98 | <0.001 | 0.28 | |
| Groups × Regions | 0.13 | 0.869 | 0.003 | |
| Groups × Sites | 0.33 | 0.685 | 0.01 | |
| Groups × Regions × Sites | 0.34 | 0.804 | 0.01 | |
| Gamma (30–50 Hz) | ||||
| Group | 0.94 | 0.339 | 0.02 | |
| Groups × Regions | 0.33 | 0.701 | 0.01 | |
| Groups × Sites | 0.06 | 0.916 | 0.001 | |
| Groups × Regions × Sites | 0.81 | 0.496 | 0.02 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Qi, Y.; Liu, Y.; Yan, Z.; Hu, S.; Zhang, X.; Zhao, J.; Turel, O.; He, Q. Slow-Wave EEG Activity Correlates with Impaired Inhibitory Control in Internet Addiction Disorder. Int. J. Environ. Res. Public Health 2022, 19, 2686. https://doi.org/10.3390/ijerph19052686
Qi Y, Liu Y, Yan Z, Hu S, Zhang X, Zhao J, Turel O, He Q. Slow-Wave EEG Activity Correlates with Impaired Inhibitory Control in Internet Addiction Disorder. International Journal of Environmental Research and Public Health. 2022; 19(5):2686. https://doi.org/10.3390/ijerph19052686
Chicago/Turabian StyleQi, Yawei, Yuting Liu, Ziyou Yan, Shiqi Hu, Xinhe Zhang, Jia Zhao, Ofir Turel, and Qinghua He. 2022. "Slow-Wave EEG Activity Correlates with Impaired Inhibitory Control in Internet Addiction Disorder" International Journal of Environmental Research and Public Health 19, no. 5: 2686. https://doi.org/10.3390/ijerph19052686