
Women Tell All: A Comparative Thematic Analysis of Women’s Perspectives on Two Brief Counseling Interventions for Intimate Partner Violence

Abstract
:1. Introduction
2. Materials and Methods
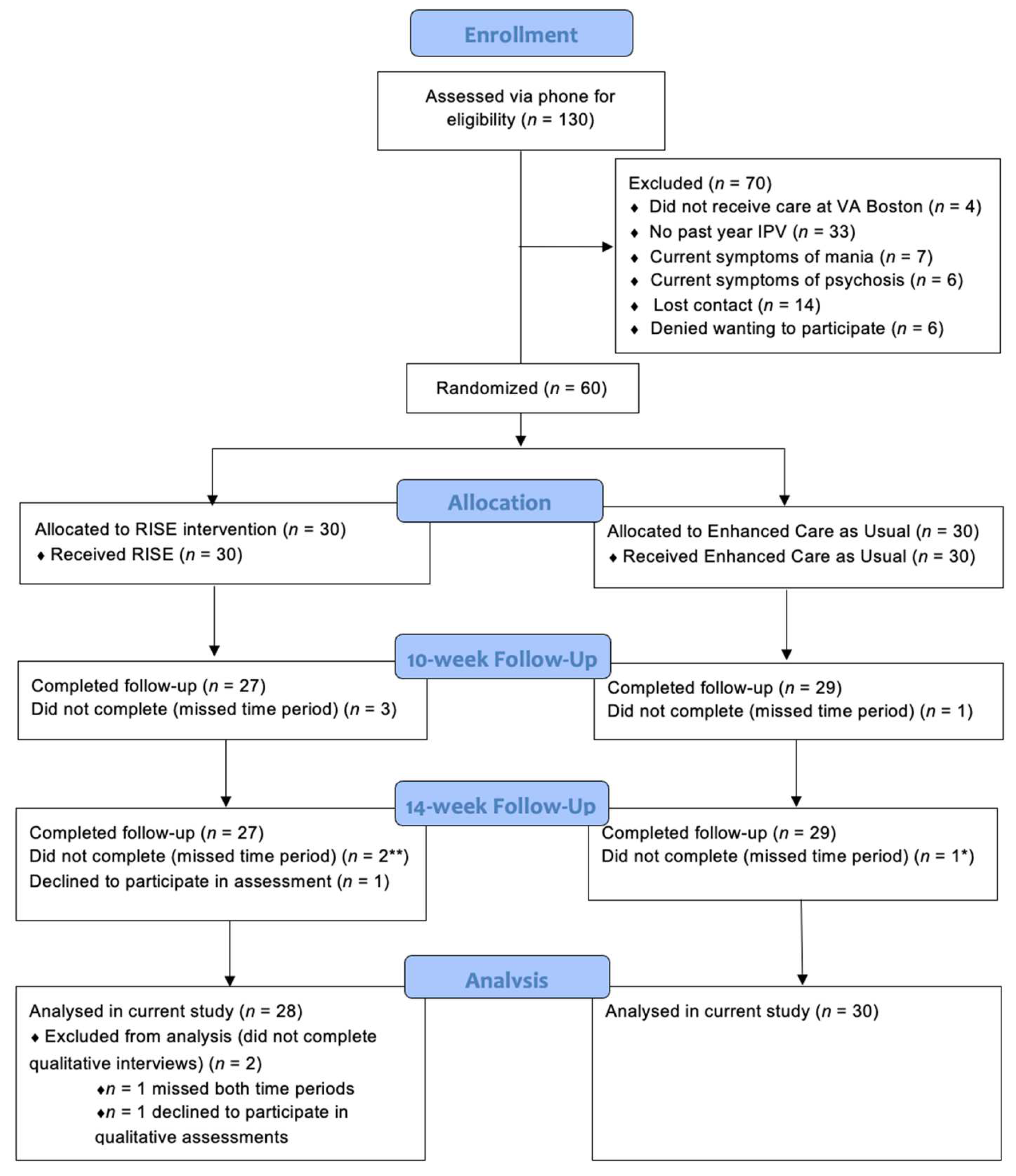
2.1. Design and Participants
2.2. Procedures
2.3. Intervention: Recovering from IPV through Strengths and Empowerment (RISE)
2.4. Intervention: Enhanced Care as Usual Condition (ECAU)
2.5. Interventionists
2.6. Approach
2.7. Data Analysis Strategy
3. Results
3.1. Perceived Impact of the Intervention
“RISE has empowered me to take much more control over the interpersonal relationships in my life (RISE, 101)”.
“It’s definitely made me realize and get some self-worth back and feel more empowered by my decisions (RISE, 102)”.
“I didn’t realize I wasn’t taking care of myself or advocating for myself much. RISE gave me that confidence to start doing that (RISE, 103)”.
“In the past I wanted to be separated from him, but I realized I couldn’t do that. Now I am working towards that financial independence (RISE, 104)”.
“[RISE] opened my eyes and after every session, I would think about what the session was about. When I’m driving or when I have a quiet period, I would realize, ‘oh yeah, I do have this quality’ or ‘oh yes, I’ve been able to handle this problem.’ So, it made me see that I wasn’t as awful as I thought I was or as inadequate as I thought I was. It made me realize I’ve accomplished a lot more than I had realized (RISE, 104)”.
“[the intervention] covered all bases including every aspect of abuse in a relationship: physical, sexual, and emotional. I feel as though emotional abuse can be more detrimental than physical sometimes (ECAU, 105)”.
“It impacted me by teaching me that I’m not responsible and I don’t deserve specific treatment, like abuse. Whether it’s physical, emotional, mental (ECAU, 106)”.
“The wealth of information and contact information for resources in the pamphlet I took it home, and I poured over it for days. I googled every single thing, whether I thought I needed it or not. Stuff like that. But that whole thing made me feel not alone in this (ECAU, 107)”.
3.2. Application of Content
“I still have and use the handouts, especially the self-care handout. Sometimes it’s hard for me to do self-care, but with handouts it reminds me that I don’t have to do anything major. It can be something simple, like aromatherapy. Even if I don’t have the funds to go out. Just little things. It definitely adds up (RISE, 103)”.
“I have been weighing my pros and cons sometimes before I make difficult decisions (RISE, 108)”.
“[RISE] led me to reach out to a couple people just to make sure we were covered in case I had to use my safety plan. For me, that was a little bit more of going outside of my norm to ask for help, especially for the relationship situation (RISE, 109)”.
“[RISE] really impacted my physical health so much. I try to make plans to workout more or exercise or do things that were more towards my physical wellness. Emotionally, RISE kind of helped me to stabilize my emotional roller coaster on some days (RISE, 110)”.
“I liked that she gave me the pamphlet and went through it with me during the session. It was helpful. She gave me resources to help me and places to go in the VA for certain things (ECAU, 111)”.
“just to have that information was comforting (ECAU, 112)”.
“I felt like I had resources within the brochure. You gave me a lot of resources to use to feel better and get help to leave. So that was good (ECAU, 113)”.
“I’ve been evaluating my situation more clearly with information from the brochure (ECAU, 114)”.
3.3. Patient-Centered Approach
“I liked that we had a menu. Every week I got to pick because then I don’t have to sit there and wonder, ‘okay, what do I want to talk about today.’ She gave me options. If I didn’t want to deal with the feelings today and instead deal with coping with stress, that option and choice was very good for me (RISE, 108)”.
“I got to pick the topic based on what I was going through. That was very good. It helped me to think, ‘okay do I need to focus on this area a little bit more or that area.’ So, I liked that I was choosing myself but talking to somebody with expertise at the same time (RISE, 110)”.
“I liked the menu items in the beginning that we covered. It gave me a chance to figure out where I was currently at in my mental state, and where I am at in that relationship. So, I really liked that. It definitely catered to what I needed instead of, this is what we are going to do today regardless of what I feel. So, I liked that (RISE, 115)”.
“It is tailored to us, which is more specific, it’s more beneficial than just some random [other resource]... oh there’s an actual office just for Veterans like me, and you should go there (ECAU, 116)”.
“I wasn’t aware there was a space for us women with partner issues. I was very happy that I was able to get that information because I want to say that I haven’t received that anywhere. Then, after the session, I felt like I had a space to do so (ECAU, 117)”.
3.4. Implementation Recommendations
“I wish that it could have been more thorough and longer. Like if it became a permanent thing, I am sure that would fix the problem, but just the one a week and because it did have such a big impact on me, there wasn’t enough of it because now here I am, and now I’m on the other side of that, and there’s still a lot of work that needs to be done (RISE, 102)”.
“I wanted to do all the topics and there were six, but there were only six sessions. I wish it could have been longer. Some weeks I really wanted to go back over one topic, but then I wouldn’t be able to, I’d have to cut one out (RISE, 102)”.
“because that really helps you set goals and then it helps you keep them. To go back and look at the first goal that you set, you know, 20 weeks prior, would be extremely helpful to kind of just remind yourself like you made this progress, don’t let go of it. Just to kind of build habits so it is not like something that you do once, and you move on and you don’t do it again (RISE, 118)”.
“I feel like if I had more sessions, the more stuff would stick. Just being reassured that things weren’t my fault or things like that would stick more (ECAU, 112)”.
“I think that the brochure she showed was really good, but with the brochure, I noticed after being here, I had a really hard day after that, and the day after. I think it was because of the brochure and how simplified it was (ECAU, 119)”.
“Just, it just seemed a little overwhelming. I actually feel like, hmm, maybe to have a couple more sessions so you don’t feel so stressed (ECAU, 120)”.
“I definitely would have said maybe a couple more sessions to get it all out to that one person and see that one person a few times and start to kind of build a relationship (ECAU, 121)”.
“Maybe doing telecommunication or skype videos. Cause I think that would have a greater impact...you could reach a lot more people. If they can’t get to you, they can literally just use their phone or computer and still talk to that person as long as they are in a safe space. And maybe they don’t feel comfortable [in the medical center] and they feel comfortable in their house talking (RISE, 122)”.
“I almost think it’s better over the phone because I am in my own comfortable space. I am not rushing to get into a hospital. Getting through traffic. I was resistant to doing therapy over the phone, but now, I have adapted to it, and I actually prefer it more (RISE, 123)”.
“I was completely comfortable with telehealth. The only time I wasn’t was when I was at my boyfriend’s mom’s house. I was like in my car doing it. It was my own fault for forgetting that I had the session, but my window was down, I think someone might have overheard me. But normally if I am home, I am completely comfortable (RISE, 118)”.
4. Discussion
Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Trial Registration
References
- World Health Organization. Violence Against Women Prevalence Estimates, 2018: Global, Regional and National Prevalence Estimates for Intimate Partner Violence against Women and Global and Regional Prevalence Estimates for Non-Partner Sexual Violence Against Women; WHO: Geneva, Switzerland, 2021. [Google Scholar]
- Smith, S.G.; Zhang, X.; Basile, K.C.; Merrick, M.T.; Wang, J.; Kresnow, M.-J.; Chen, J. The National Intimate Partner and Sexual Violence Survey: 2015 Data Brief–Updated Release; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2018. [Google Scholar]
- Thompson, R.S.; Bonomi, A.E.; Anderson, M.; Reid, R.J.; Dimer, J.A.; Carrell, D.; Rivara, F.P. Intimate Partner Violence: Prevalence, Types, and Chronicity in Adult Women. Am. J. Prev. Med. 2006, 30, 447–457. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ellsberg, M.; Jansen, H.A.; Heise, L.; Watts, C.H.; Garcia-Moreno, C.; WHO Multi-country Study on Women’s Health and Domestic Violence against Women Study Team. Intimate partner violence and women’s physical and mental health in the WHO multi-country study on women’s health and domestic violence: An observational study. Lancet 2008, 371, 1165–1172. [Google Scholar] [CrossRef]
- Benight, C.C.; Bandura, A. Social cognitive theory of posttraumatic recovery: The role of perceived self-efficacy. Behav. Res. Ther. 2004, 42, 1129–1148. [Google Scholar] [CrossRef] [PubMed]
- Dardis, C.M.; Dichter, M.E.; Iverson, K.M. Empowerment, PTSD and revictimization among women who have experienced intimate partner violence. Psychiatry Res. 2018, 266, 103–110. [Google Scholar] [CrossRef]
- Johnson, D.M.; Worell, J.; Chandler, R.K. Assessing Psychological Health and Empowerment in Women: The Personal Progress Scale Revised. Women Health 2005, 41, 109–129. [Google Scholar] [CrossRef]
- McLean, C.; Follette, V.M. Acceptance and Commitment Therapy as a Non-Pathologizing Intervention Approach for Survivors of Trauma. J. Trauma Dissociation 2015, 17, 138–150. [Google Scholar] [CrossRef]
- Potter, L.C.; Morris, R.; Hegarty, K.; García-Moreno, C.; Feder, G. Categories and health impacts of intimate partner violence in the World Health Organization multi-country study on women’s health and domestic violence. Int. J. Epidemiol. 2021, 50, 652–662. [Google Scholar] [CrossRef]
- Bonomi, A.E.; Anderson, M.L.; Rivara, F.P.; Thompson, R.S. Health Care Utilization and Costs Associated with Physical and Nonphysical-Only Intimate Partner Violence. Health Serv. Res. 2009, 44, 1052–1067. [Google Scholar] [CrossRef] [Green Version]
- Sorrentino, A.E.; Iverson, K.M.; Tuepker, A.; True, G.; Cusack, M.; Newell, S.; Dichter, M.E. Mental health care in the context of intimate partner violence: Survivor perspectives. Psychol. Serv. 2021, 18, 512–522. [Google Scholar] [CrossRef]
- Musa, A.; Chojenta, C.; Geleto, A.; Loxton, D. The associations between intimate partner violence and maternal health care service utilization: A systematic review and meta-analysis. BMC Women’s Health 2019, 19, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Miller, E.; McCaw, B. Intimate Partner Violence. N. Engl. J. Med. 2019, 380, 850–857. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Curry, S.J.; Krist, A.H.; Owens, D.K.; Barry, M.J.; Caughey, A.B.; Davidson, K.; Doubeni, C.A.; Epling, J.W.; Grossman, D.C. Screening for Intimate Partner Violence, Elder Abuse, and Abuse of Vulnerable Adults: US Preventive Services Task Force final recommendation statement. JAMA J. Am. Med. Assoc. 2018, 320, 1678–1687. [Google Scholar] [CrossRef] [Green Version]
- Feltner, C.; Wallace, I.; Berkman, N.; Kistler, C.E.; Middleton, J.C.; Barclay, C.; Higginbotham, L.; Green, J.T.; Jonas, D.E. Screening for Intimate Partner Violence, Elder Abuse, and Abuse of Vulnerable Adults: Evidence report and systematic review for the US Preventive Services Task Force. JAMA J. Am. Med. Assoc. 2018, 320, 1688–1701. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bair-Merritt, M.H.; Lewis-O’Connor, A.; Goel, S.; Amato, P.; Ismailji, T.; Jelley, M.; Lenahan, P.; Cronholm, P. Primary Care–Based Interventions for Intimate Partner Violence: A systematic review. Am. J. Prev. Med. 2014, 46, 188–194. [Google Scholar] [CrossRef]
- Johnson, D.M.; Zlotnick, C.; Hoffman, L.; Palmieri, P.A.; Johnson, N.L.; Holmes, S.C.; Ceroni, T.L. A Randomized Controlled Trial Comparing HOPE Treatment and Present-Centered Therapy in Women Residing in Shelter With PTSD From Intimate Partner Violence. Psychol. Women Q. 2020, 44, 539–553. [Google Scholar] [CrossRef]
- Iverson, K.M.; Shenk, C.; Fruzzetti, A.E. Dialectical behavior therapy for women victims of domestic abuse: A pilot study. Prof. Psychol. Res. Pract. 2009, 40, 242–248. [Google Scholar] [CrossRef] [Green Version]
- Blackwood, J.; Armstrong, M.J.; Schaefer, C.; Graham, I.D.; Knaapen, L.; Straus, S.E.; Urquhart, R.; Gagliardi, A.R. How do guideline developers identify, incorporate and report patient preferences? An international cross-sectional survey. BMC Health Serv. Res. 2020, 20, 1–10. [Google Scholar] [CrossRef]
- Tarzia, L.; Bohren, M.A.; Cameron, J.; Garcia-Moreno, C.; O’Doherty, L.; Fiolet, R.; Hooker, L.; Wellington, M.; Parker, R.; Koziol-McLain, J.; et al. Women’s experiences and expectations after disclosure of intimate partner abuse to a healthcare provider: A qualitative meta-synthesis. BMJ Open 2020, 10, e041339. [Google Scholar] [CrossRef]
- Greene, S. A Framework for Making Patient-Centered Care Front and Center. Perm. J. 2012, 16, 49–53. [Google Scholar] [CrossRef] [Green Version]
- Goodman, L.A.; Thomas, K.; Cattaneo, L.B.; Heimel, D.; Woulfe, J.; Chong, S.K. Survivor-Defined Practice in Domestic Violence Work: Measure development and preliminary evidence of link to empowerment. J. Interpers. Violence 2016, 31, 163–185. [Google Scholar] [CrossRef]
- Kulkarni, S. Intersectional Trauma-Informed Intimate Partner Violence (IPV) Services: Narrowing the Gap between IPV Service Delivery and Survivor Needs. J. Fam. Violence 2019, 34, 55–64. [Google Scholar] [CrossRef]
- Grillo, A.R.; Danitz, S.B.; Dichter, M.E.; Driscoll, M.A.; Gerber, M.R.; Hamilton, A.B.; Wiltsey-Stirman, S.; Iverson, K.M. Strides Toward Recovery From Intimate Partner Violence: Elucidating Patient-Centered Outcomes to Optimize a Brief Counseling Intervention for Women. J. Interpers. Violence 2019, 36, 8431–8453. [Google Scholar] [CrossRef] [PubMed]
- Lyon, A.R.; Koerner, K. User-centered design for psychosocial intervention development and implementation. Clin. Psychol. Sci. Pract. 2016, 23, 180–200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iverson, K.M.; King, M.W.; Gerber, M.R.; Resick, P.A.; Kimerling, R.; Street, A.E.; Vogt, D. Accuracy of an Intimate Partner Violence Screening Tool for Female VHA Patients: A Replication and Extension. J. Trauma. Stress 2015, 28, 79–82. [Google Scholar] [CrossRef] [PubMed]
- Kimerling, R.; Iverson, K.M.; Dichter, M.E.; Rodriguez, A.L.; Wong, A.; Pavao, J. Prevalence of Intimate Partner Violence among Women Veterans who Utilize Veterans Health Administration Primary Care. J. Gen. Intern. Med. 2016, 31, 888–894. [Google Scholar] [CrossRef] [Green Version]
- Murdoch, M. Women veterans’ experiences with domestic violence and with sexual harassment while in the military. Arch. Fam. Med. 1995, 4, 411–418. [Google Scholar] [CrossRef] [Green Version]
- Iverson, K.M.; Vogt, D.; Dichter, M.E.; Carpenter, S.L.; Kimerling, R.; Street, A.E.; Gerber, M.R. Intimate Partner Violence and Current Mental Health Needs Among Female Veterans. J. Am. Board Fam. Med. 2015, 28, 772–776. [Google Scholar] [CrossRef] [Green Version]
- Dichter, M.E.; Cerulli, C.; Bossarte, R.M. Intimate Partner Violence Victimization Among Women Veterans and Associated Heart Health Risks. Women’s Health Issues 2011, 21, S190–S194. [Google Scholar] [CrossRef]
- Ortabag, T.; Ozdemir, S.; Bebis, H.; Ceylan, S. Perspectives of Young Adult Men Regarding Violence against Women: A Cross-sectional Study from Turkey. J. Fam. Violence 2014, 29, 665–674. [Google Scholar] [CrossRef]
- Dighton, G.; Roberts, E.; Hoon, A.E.; Dymond, S. Gambling problems and the impact of family in UK armed forces veterans. J. Behav. Addict. 2018, 7, 355–365. [Google Scholar] [CrossRef]
- Zamorski, M.A.; Wiens-Kinkaid, M.E. Cross-sectional prevalence survey of intimate partner violence perpetration and victimization in Canadian military personnel. BMC Public Health 2013, 13, 1019. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dichter, M.E.; Sorrentino, A.; Bellamy, S.; Medvedeva, E.; Roberts, C.B.; Iverson, K.M. Disproportionate Mental Health Burden Associated With Past-Year Intimate Partner Violence Among Women Receiving Care in the Veterans Health Administration. J. Trauma. Stress 2017, 30, 555–563. [Google Scholar] [CrossRef] [PubMed]
- Iverson, K.M.; Vogt, D.; Maskin, R.M.; Smith, B.N. Intimate Partner Violence Victimization and Associated Implications for Health and Functioning Among Male and Female Post-9/11 Veterans. Med. Care 2017, 55, S78–S84. [Google Scholar] [CrossRef] [PubMed]
- Portnoy, G.A.; Relyea, M.R.; Street, A.E.; Haskell, S.G.; Iverson, K.M. A Longitudinal Analysis of Women Veterans’ Partner Violence Perpetration: The Roles of Interpersonal Trauma and Posttraumatic Stress Symptoms. J. Fam. Violence 2019, 35, 361–372. [Google Scholar] [CrossRef]
- Bartlett, B.A.; Iverson, K.M.; Mitchell, K.S. Intimate partner violence and disordered eating among male and female veterans. Psychiatry Res. 2018, 260, 98–104. [Google Scholar] [CrossRef] [PubMed]
- Iverson, K.M.; Danitz, S.B.; Shayani, D.R.; Vogt, D.; Stirman, S.W.; Hamilton, A.B.; Mahoney, C.T.; Gerber, M.R.; Dichter, M.E. Recovering from Intimate Partner Violence through Strengths and Empowerment: Findings from a Randomized Clinical Trial. J. Clin. Psychiatry 2021, 83, 38188. [Google Scholar] [CrossRef]
- Teague, A.K.; Hahna, N.D.; McKinney, C.H. Group Music Therapy with Women who have Experienced Intimate Partner Violence. Music Ther. Perspect. 2006, 24, 80–86. [Google Scholar] [CrossRef]
- Cort, N.A.; Cerulli, C.; Poleshuck, E.L.; Bellenger, K.M.; Xia, Y.; Tu, X.; Mazzotta, C.M.; Talbot, N.L. Interpersonal psychotherapy for depressed women with histories of intimate partner violence. Psychol. Trauma Theory Res. Pract. Policy 2014, 6, 700–707. [Google Scholar] [CrossRef]
- Johnson, D.M.; Zlotnick, C.; Perez, S. Cognitive behavioral treatment of PTSD in residents of battered women’s shelters: Results of a randomized clinical trial. J. Consult. Clin. Psychol. 2011, 79, 542–551. [Google Scholar] [CrossRef] [Green Version]
- Straus, M.A.; Hamby, S.L.; Boney-McCoy, S.; Sugarman, D.B. The Revised Conflict Tactics Scales (CTS2) development and preliminary psychometric data. J. Fam. Issues 1996, 17, 283–316. [Google Scholar] [CrossRef]
- Miller, W.R.; Rollnick, S. Motivational Interviewing: Helping People Change; Guilford Press: New York, NY, USA, 2012. [Google Scholar]
- Iverson, K.M.; Danitz, S.B.; Driscoll, M.; Vogt, D.; Hamilton, A.B.; Gerber, M.R.; Stirman, S.W.; Shayani, D.R.; Suvak, M.K.; Dichter, M.E. Recovering from intimate partner violence through Strengths and Empowerment (RISE): Development, pilot testing, and refinement of a patient-centered brief counseling intervention for women. Psychol. Serv. 2021. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, A.B.; Finley, E.P. Qualitative methods in implementation research: An introduction. Psychiatry Res. 2019, 280, 112516. [Google Scholar] [CrossRef] [PubMed]
- Lewinski, A.A.; Crowley, M.J.; Miller, C.; Bosworth, H.B.; Jackson, G.L.; Steinhauser, K.; White-Clark, C.; McCant, F.; Zullig, L.L. Applied Rapid Qualitative Analysis to Develop a Contextually Appropriate Intervention and Increase the Likelihood of Uptake. Med. Care 2021, 59, S242–S251. [Google Scholar] [CrossRef] [PubMed]
- Averill, J.B. Matrix Analysis as a Complementary Analytic Strategy in Qualitative Inquiry. Qual. Health Res. 2002, 12, 855–866. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.C.; Cluss, P.A.; Ranieri, L.; Hawker, L.; Buranosky, R.; Dado, D.; McNeil, M.; Scholle, S.H. Health care interventions for intimate partner violence: What women want. Women’s Health Issues 2005, 15, 21–30. [Google Scholar] [CrossRef] [PubMed]
- Iverson, K.M.; Stirman, S.W.; Street, A.E.; Gerber, M.R.; Carpenter, S.L.; Dichter, M.E.; Bair-Merritt, M.; Vogt, D.; Carpenter, L.S. Female veterans’ preferences for counseling related to intimate partner violence: Informing patient-centered interventions. Gen. Hosp. Psychiatry 2016, 40, 33–38. [Google Scholar] [CrossRef]
- Trevillion, K.; Hughes, B.; Feder, G.; Borschmann, R.; Oram, S.; Howard, L.M. Disclosure of domestic violence in mental health settings: A qualitative meta-synthesis. Int. Rev. Psychiatry 2014, 26, 430–444. [Google Scholar] [CrossRef] [Green Version]
- Chorpita, B.F.; Daleiden, E.L.; Weisz, J.R. Modularity in the design and application of therapeutic interventions. Appl. Prev. Psychol. 2005, 11, 141–156. [Google Scholar] [CrossRef]
- Palinkas, L.A.; Weisz, J.R.; Chorpita, B.F.; Levine, B.; Garland, A.F.; Hoagwood, K.E.; Landsverk, J. Continued Use of Evidence-Based Treatments After a Randomized Controlled Effectiveness Trial: A Qualitative Study. Psychiatr. Serv. 2013, 64, 1110–1118. [Google Scholar] [CrossRef]
- Gerber, M.R.; Elisseou, S.; Sager, Z.S.; Keith, J.A. Trauma-Informed Telehealth in the COVID-19 Era and Beyond. Fed. Pract. 2020, 37, 302–308. [Google Scholar] [CrossRef]
- Rossi, F.S.; Shankar, M.; Buckholdt, K.; Bailey, Y.; Israni, S.T.; Iverson, K.M. Trying Times and Trying Out Solutions: Intimate Partner Violence Screening and Support for Women Veterans During COVID-19. J. Gen. Intern. Med. 2020, 35, 2728–2731. [Google Scholar] [CrossRef]
- Moring, J.C.; Dondanville, K.A.; Fina, B.A.; Hassija, C.; Chard, K.; Monson, C.; LoSavio, S.T.; Wells, S.Y.; Morland, L.A.; Kaysen, D.; et al. Cognitive Processing Therapy for Posttraumatic Stress Disorder via Telehealth: Practical Considerations During the COVID-19 Pandemic. J. Trauma. Stress 2020, 33, 371–379. [Google Scholar] [CrossRef] [PubMed]
- Rivas, C.; Ramsay, J.; Sadowski, L.; Davidson, L.L.; Dunnes, D.; Eldridge, S.; Hegarty, K.; Taft, A.; Feder, G. Advocacy Interventions to Reduce or Eliminate Violence and Promote the Physical and Psychosocial Well-Being of Women who Experience Intimate Partner Abuse: A Systematic Review. Campbell Syst. Rev. 2016, 12, 1–202. [Google Scholar] [CrossRef]
- Chamberlain, L.; Levenson, R. Addressing intimate partner violence, reproductive and sexual coercion. In A Guide for Obstetric, Gynecologic and Reproductive Health Care Settings, 2nd ed.; Futures Without Violence: San Francisco, CA, USA, 2012; Volume 1. [Google Scholar] [CrossRef]
- Ghandour, R.M.; Campbell, J.C.; Lloyd, J. Screening and Counseling for Intimate Partner Violence: A Vision for the Future. J. Women’s Health 2015, 24, 57–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iverson, K.M.; Huang, K.; Wells, S.Y.; Wright, J.D.; Gerber, M.; Wiltsey-Stirman, S. Women Veterans’ Preferences for Intimate Partner Violence Screening and Response Procedures Within the Veterans Health Administration. Res. Nurs. Health 2014, 37, 302–311. [Google Scholar] [CrossRef]
- Dyer, K.E.; Moreau, J.L.; Finley, E.; Bean-Mayberry, B.; Farmer, M.M.; Bernet, D.; Kress, A.; Lewis, J.L.; Batuman, F.K.; Haskell, S.G.; et al. Tailoring an evidence-based lifestyle intervention to meet the needs of women Veterans with prediabetes. Women Health 2020, 60, 748–762. [Google Scholar] [CrossRef]
- Anderson, K.M.; Renner, L.M.; Danis, F.S. Recovery: Resilience and growth in the aftermath of domestic violence. Violence Against Women 2012, 18, 1279–1299. [Google Scholar] [CrossRef] [Green Version]
- Beeble, M.L.; Bybee, D.; Sullivan, C.M.; Adams, A.E. Main, mediating, and moderating effects of social support on the well-being of survivors of intimate partner violence across 2 years. J. Consult. Clin. Psychol. 2009, 77, 718–729. [Google Scholar] [CrossRef]
- Ogbe, E.; Harmon, S.; Van den Bergh, R.; Degomme, O. A systematic review of intimate partner violence interventions focused on improving social support and/ mental health outcomes of survivors. PLoS ONE 2020, 15, e0235177. [Google Scholar] [CrossRef]
- Foa, E.B.; Rothbaum, B.O. Treating the Trauma of Rape: Cognitive Behavioral Therapy for PTSD; Guilford: New York, NY, USA, 1998. [Google Scholar]
- Gerber, M.R.; Iverson, K.M.; Dichter, M.E.; Klap, R.; Latta, R.E. Women Veterans and Intimate Partner Violence: Current State of Knowledge and Future Directions. J. Women’s Health 2014, 23, 302–309. [Google Scholar] [CrossRef]
- McCauley, H.L.; Blosnich, J.R.; Dichter, M.E. Adverse Childhood Experiences and Adult Health Outcomes Among Veteran and Non-Veteran Women. J. Women’s Health 2015, 24, 723–729. [Google Scholar] [CrossRef] [PubMed]
- Frayne, S.M.; Saechao, F.; Maisel, N.C.; Friedman, S.A.; Finlay, A.; Berg, E.; Balasubramanian, V.; Dally, S.K.; Ananth, L.; Romodan, Y.; et al. Sociodemographics, utilization, costs of care, and health profile. In Sourcebook: Women Veterans in the Veterans Health Administration; Department of Veterans Affairs: Washington, DC, USA, 2014; Volume 3. [Google Scholar]


{kind=link}
| Sociodemographic Characteristics a | RISE (n = 28) | ECAU (n = 30) | Statistic | p-Value |
|---|---|---|---|---|
| Age, M (SD) | 38.0 (11.0) | 40.5 (13) | t = 0.79 | 0.44 |
| Race/Ethnicity | χ2 = 4.60 | 0.47 | ||
| Black | 7 (25.0) | 5 (16.7) | ||
| White/Caucasian | 19 (67.9) | 16 (53.3) | ||
| Asian | 1 (3.6) | 2 (6.7) | ||
| Native American | 0 (0) | 1 (3.3) | ||
| Other Race | 0 (0) | 3 (10) | ||
| Multiple Races | 1 (3.6) | 4 (13.3) | ||
| White Non-Hispanic | 27 (96.4) | 25 (83.3) | χ2 = 0.21 | 0.64 |
| Non-White/Hispanic | 1 (3.6) | 5 (16.7) | ||
| Sexual Orientation | χ2 = 2.24 | 0.53 | ||
| Heterosexual | 18 (64.3) | 24 (80) | ||
| Lesbian/Gay | 3 (10.7) | 1 (3.3) | ||
| Bisexual | 5 (17.9) | 4 (13.3) | ||
| Pansexual | 2 (7.1) | 1 (3.3) | ||
| Relationship Status | χ2 = 6.13 | 0.29 | ||
| Married/Cohabitating | 7 (25) | 5 (16.7) | ||
| LT/NM | 7 (25) | 5 (16.7) | ||
| NM/NLT | 3 (10.7) | 1 (3.3) | ||
| Single | 7 (25.0) | 8 (26.7) | ||
| Separated | 2 (7.1) | 9 (30) | ||
| Other | 2 (7.1) | 2 (6.7) | ||
| Income | χ2 = 8.59 | 0.28 | ||
| Less than $15,000 | 2 (7.1) | 4 (13.3) | ||
| $15,000–$24,999 | 2 (7.1) | 4 (13.3) | ||
| $25,000–34,999 | 3 (10.7) | 3 (10) | ||
| $35,000–$44,999 | 5 (17.9) | 2 (6.7) | ||
| $45,000–$54,999 | 3 (10.7) | 6 (20) | ||
| $55,000–$64,999 | 2 (7.1) | 5 (16.7) | ||
| $65,000–$74,999 | 3 (10.7) | 0 (0) | ||
| $75,000 or more | 8 (28.6) | 5 (16.7) | ||
| Employment Status | χ2 = 28.15 | 0.001 | ||
| Employed Full Time * | 16 (57.1) | 8 (27.6) | ||
| Employed Part Time | 5 (17.9) | 4 (13.8) | ||
| Student Full Time | 4 (14.3) | 7 (24.1) | ||
| Student Part Time | 2 (6.9) | 1 (3.4) | ||
| Unpaid Volunteer | 3 (10.7) | 7 (23.3) | ||
| Retired or Other | 5 (19.9) | 4 (13.8) | ||
| Education | χ2 = 3.48 | 0.63 | ||
| Vocational/Tech College | 3 (10.7) | 5 (16.7) | ||
| Some College/Associate | 14 (50) | 16 (53.3) | ||
| Bachelor’s Degree | 6 (21.4) | 4 (13.3) | ||
| Master’s/Doctoral Degree | 5 (17.9) | 5 (16.7) | ||
| Military Branch | χ2 = 4.40 | 0.49 | ||
| Army | 15 (53.6) | 16 (53.3) | ||
| Navy | 3 (10.7) | 4 (13.3) | ||
| Air Force | 5 (17.9) | 2 (6.7) | ||
| Marine Corps | 4 (14.3) | 4 (13.3) | ||
| Years of Military Service M (SD) | 6.9 (5.6) | 7.1 (8.9) | t = 0.09 | 0.93 |
| IPV Experience | χ2 = 3.31 | 0.19 | ||
| Past-Year Psychological IPV | 28 (100) | 30 (100) | ||
| Past-Year Physical IPV | 16 (57.1) | 24 (80) | ||
| Past-Year Sexual IPV | 15 (53.6) | 11 (36.7) | ||
| Length of IPV in Relationship | χ2 = 3.00 | 0.81 | ||
| Less than 6 months | 6 (21.4) | 3 (10) | ||
| Between 6 months and 1 year | 6 (21.4) | 5 (16.7) | ||
| Between 1 and 3 years | 6 (21.4) | 6 (20.0) | ||
| Between 3 and 5 years | 4 (14.3) | 5 (16.7) | ||
| Between 5 and 7 years | 2 (7.1) | 2 (6.7) | ||
| Between 7 and 9 years | 0 (0) | 1 (3.3) | ||
| 10+ years | 4 (14.3) | 7 (23.3) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shayani, D.R.; Danitz, S.B.; Low, S.K.; Hamilton, A.B.; Iverson, K.M. Women Tell All: A Comparative Thematic Analysis of Women’s Perspectives on Two Brief Counseling Interventions for Intimate Partner Violence. Int. J. Environ. Res. Public Health 2022, 19, 2513. https://doi.org/10.3390/ijerph19052513
Shayani DR, Danitz SB, Low SK, Hamilton AB, Iverson KM. Women Tell All: A Comparative Thematic Analysis of Women’s Perspectives on Two Brief Counseling Interventions for Intimate Partner Violence. International Journal of Environmental Research and Public Health. 2022; 19(5):2513. https://doi.org/10.3390/ijerph19052513
Chicago/Turabian StyleShayani, Danielle R., Sara B. Danitz, Stephanie K. Low, Alison B. Hamilton, and Katherine M. Iverson. 2022. "Women Tell All: A Comparative Thematic Analysis of Women’s Perspectives on Two Brief Counseling Interventions for Intimate Partner Violence" International Journal of Environmental Research and Public Health 19, no. 5: 2513. https://doi.org/10.3390/ijerph19052513