
Treatment Preferences for Pharmacological versus Psychological Interventions among Primary Care Providers in Nepal: Mixed Methods Analysis of a Pilot Cluster Randomized Controlled Trial

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Training Strategies for Primary Care Providers: Standard mhGAP vs. RESHAPE
2.2. Data Collection and Analysis
2.2.1. Qualitative Data
2.2.2. Quantitative Data
3. Results
3.1. Qualitative Results
3.1.1. Participants and Overview of Themes
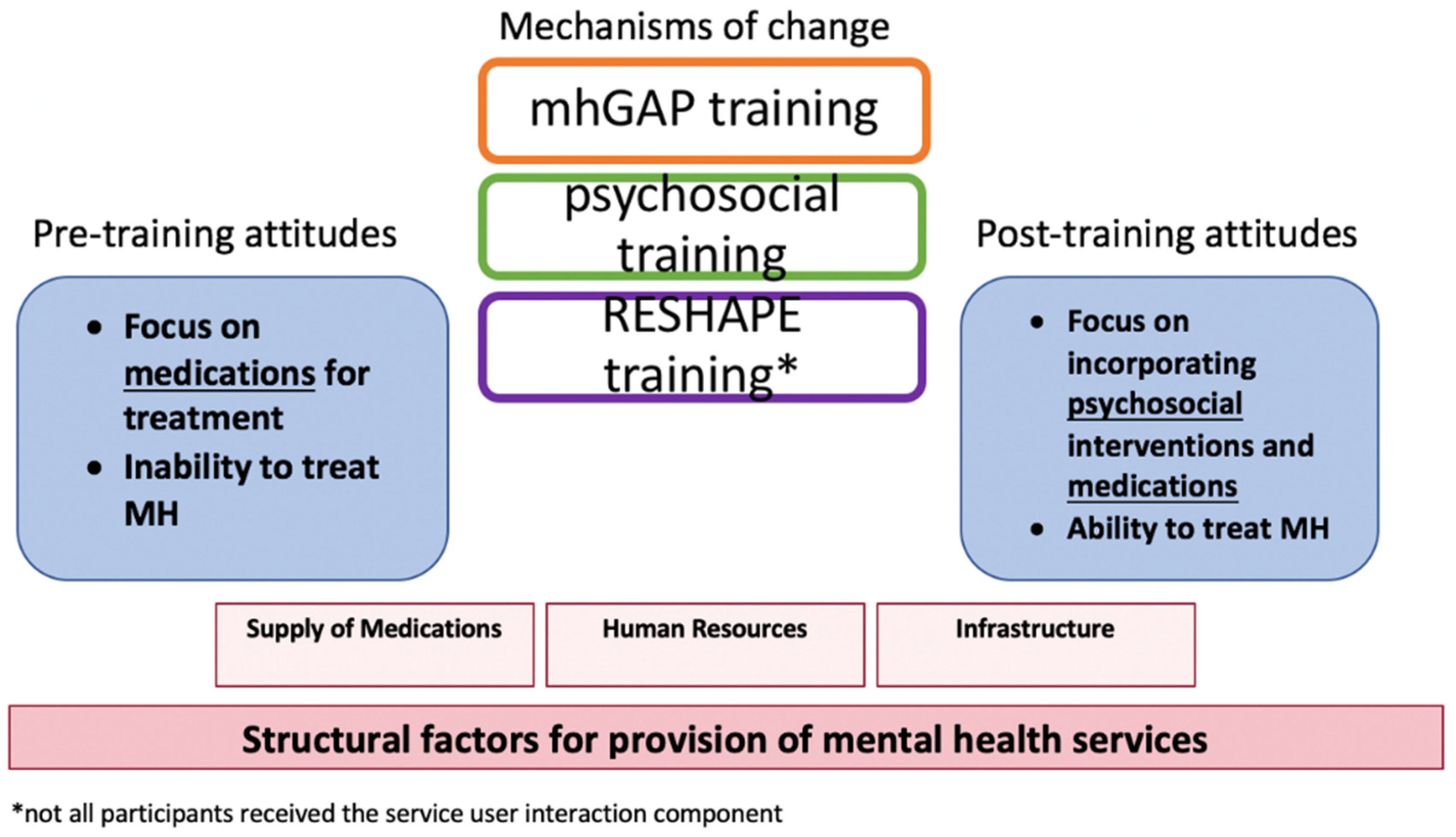
3.1.2. Attitudes toward Medications and Psychological Treatments Prior to Training
“When confronted with people who would complain of their mental health problems, we would try to bring awareness by explaining that mental health problems can be treated in a hospital with medication and such. We told the patients that they would be able to get back to their day-to-day activities just like they were before they had mental health problems.”—#15, RESHAPE prescriber, Male.
“If a doctor prescribes those medicines, they stigmatize them as a ‘mad man’s doctor’ (Nepali: paagal ko daktar). But they don’t say that to us because we have also dealt with patients with tuberculosis, leprosy, and malaria. We deal with all these patients here and give medications for all these problems, and along with these, we have also started giving medicines for mental illness, and it’s been much easier for us.”—#18, RESHAPE prescriber, Male.
“Mental health stigma should be reduced. High class people don’t want others to know that they are mentally ill. They simply say that they have been cursed by some supernatural power. When they get cured by traditional healers, they feel as if god has cured them. But, if they take medicines from a health post, people look down upon them and say they had a mental disease and needed medicines to be cured. When we give them these medicines, they think that they are cured by medicines for crazy people.”—#49, RESHAPE prescriber, Male.
“Firstly, clients with mental issues used to come to us with physical problems such as headaches or fatigue or similar body issues. If a client came in with a headache, we simply prescribed cetamol (acetaminophen) and let them be on their way. We did not dig deeper into their problem.”—#16, RESHAPE, prescriber, Female.
“Sometimes the patients need psychiatric medicine, but they [health care workers] give out other medicines because these kinds of [physical] complaints also came from the clients. As I said earlier, the major learning I received is that now I can identify mental diseases like anxiety or depression, which earlier I would ignore just by giving some headache medicines.”—#14, RESHAPE prescriber, Male.
3.1.3. Attitudes toward Medications and Psychological Treatment after Training
“Interviewer: Now, after the training, what aspects of mental health services are you confident in providing?”“Respondent: After taking the mental health service help, if a client comes, I can differentiate between depression, psychosis, epilepsy, and alcohol withdrawal. Likewise, I can follow up with counseling. They say that for those with mental health issues, counseling can help solve half of their problems.”—#16, RESHAPE prescriber, Female.
“Both prescribers and non-prescribers are playing good roles. After we see a patient, we send the patient to the non-prescriber for counseling… When the patient comes for follow up visits, we can decide whether the patient needs medicines or only counseling. First, we send them for counseling, and after counseling only, we decide whether the medicines are required or not.”—#18, RESHAPE, prescriber, Male.
 ), which is the organ of memory and emotion. Psychological distress in the heart-mind is seen as commonplace, thus not highly stigmatized. By further understanding this term, participants came to recognize the necessity of talking to patients with mental illnesses by listening to their stories so that the healthcare worker can get to the root of the patient’s problem, as reported by both prescribers and non-prescribers:
), which is the organ of memory and emotion. Psychological distress in the heart-mind is seen as commonplace, thus not highly stigmatized. By further understanding this term, participants came to recognize the necessity of talking to patients with mental illnesses by listening to their stories so that the healthcare worker can get to the root of the patient’s problem, as reported by both prescribers and non-prescribers:“Before, when such patients with problems related to heart-mind used to come, we used to refer them directly, but now we look after the patients. We prescribe medicine to them, and we also provide them counseling so it has been very easy”—#12 RESHAPE prescriber, Male.
“In the case of heart-mind problems, I think counseling is very helpful. However, as cases differ, the use of medicine might also be required. I feel that the counseling is really important as through psychosocial counseling, we can reach the heart-mind of that person and know things, which might in turn be helpful in curing them”—#1, RESHAPE non-prescriber, Female.
“We had no idea about the counseling before. We used to ask them a few questions and then referred them to doctors or give them suggestion to meet them. But now, we try to understand their problems. Counseling is also as important as medication. If both the counseling and medication is provided to the patient, then it will help them to recover soon. There will be changes in their lives.”—#34. RESHAPE prescriber.
“I: What benefits do you think there were because of [aspirational figures’] involvement in the training?”“R: I mentioned about it before too. It helped us in part of counseling too. When we listened to what the health workers said, it made us feel that we can help [people with mental illness] for their treatment in our health post too. We can help them achieve the life they had before having this illness. It motivated us.”—#2, RESHAPE non-prescriber, Female.
3.1.4. Structural Factors
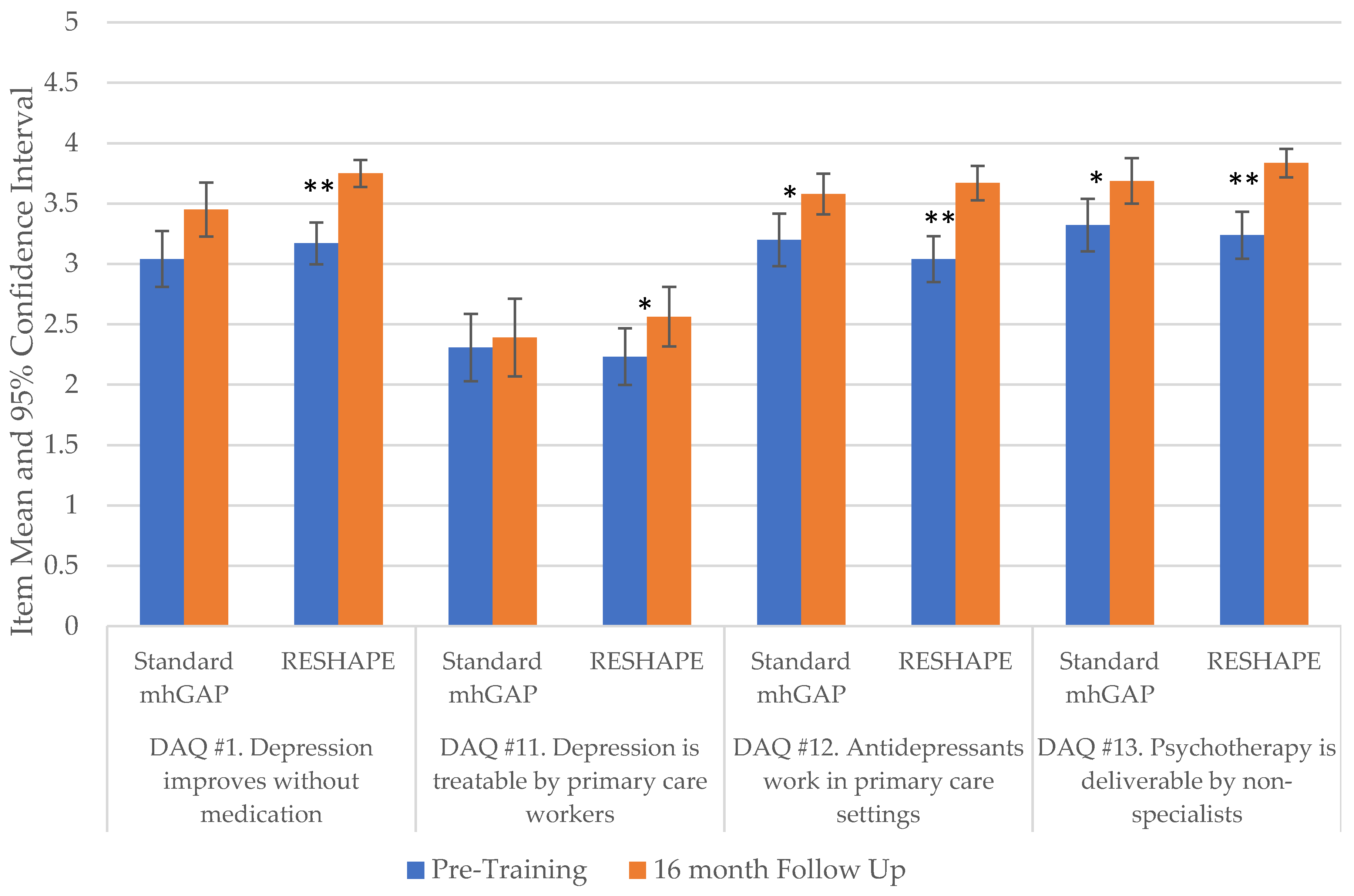
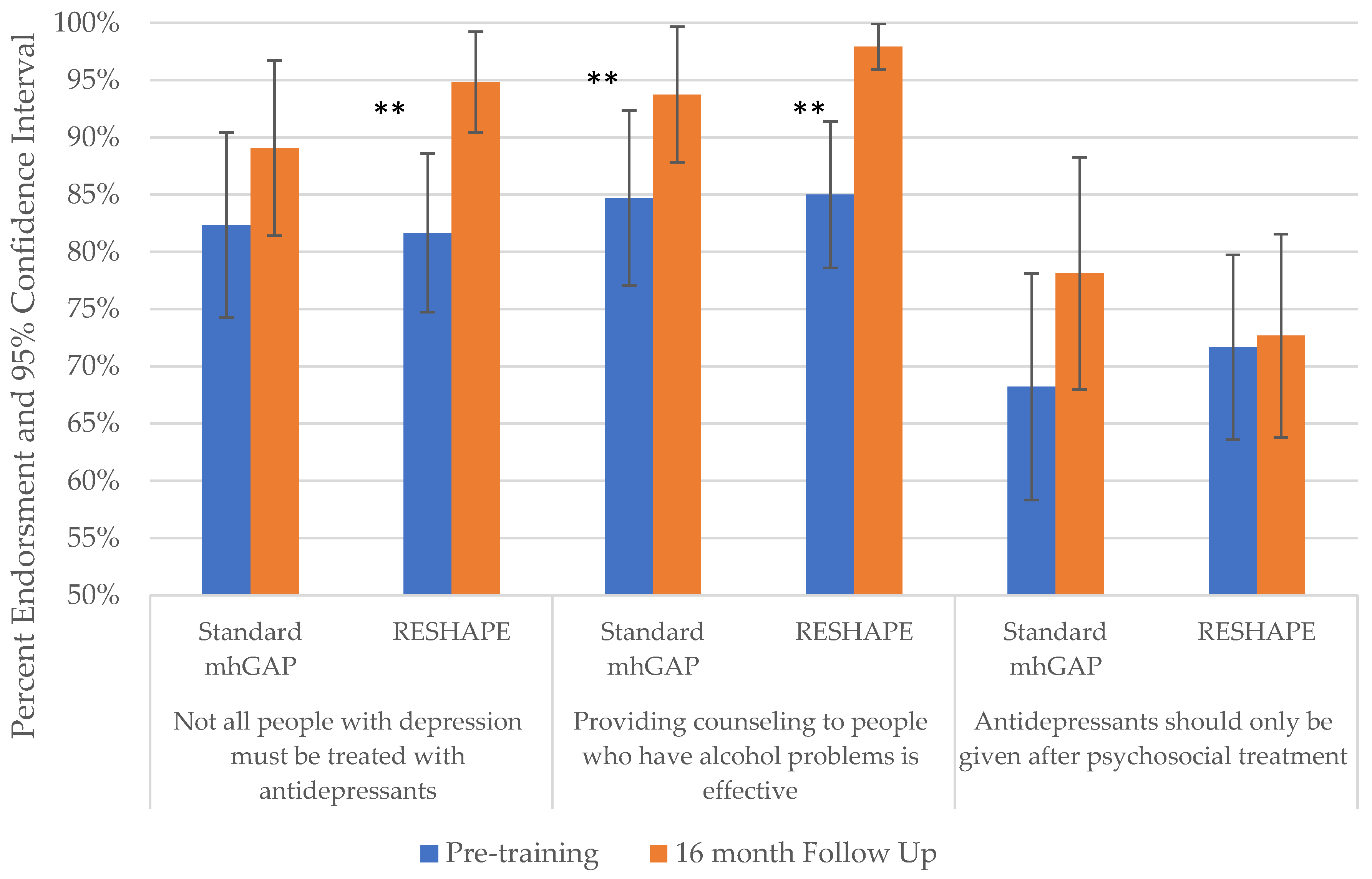
3.2. Quantitative Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Patel, V.; Chisholm, D.; Parikh, R.; Charlson, F.J.; Degenhardt, L.; Dua, T.; Ferrari, A.J.; Hyman, S.; Laxminarayan, R.; Levin, C.; et al. Addressing the burden of mental, neurological, and substance use disorders: Key messages from Disease Control Priorities, 3rd edition. Lancet 2016, 387, 1672–1685. [Google Scholar] [CrossRef] [Green Version]
- Singla, D.R.; Kohrt, B.A.; Murray, L.K.; Anand, A.; Chorpita, B.F.; Patel, V. Psychological treatments for the world: Lessons from low-and middle-income countries. Annu. Rev. Clin. Psychol. 2017, 13, 149–181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. mhGAP Training Manuals: For the mhGAP Intervention Guide for Mental, Neurological and Substance Use Disorders in Non-Specialized Health Settings–Version 2.0 (for Field Testing); World Health Organization (WHO/MSD/MER/17.6): Geneva, Switzerland, 2017; p. 656. [Google Scholar]
- Ventevogel, P. Integration of mental health into primary healthcare in low-income countries: Avoiding medicalization. Int. Rev. Psychiatry 2014, 26, 669–679. [Google Scholar] [CrossRef] [PubMed]
- Ola, B.; Crabb, J.; Adewuya, A.; Olugbile, F.; Abosede, O.A. The state of readiness of Lagos State Primary Health Care Physicians to embrace the care of depression in Nigeria. Community Ment. Health J. 2014, 50, 239–244. [Google Scholar] [CrossRef]
- Adewuya, A.O.; Adewumi, T.; Ola, B.; Abosede, O.; Oyeneyin, A.; Fasawe, A.; Idris, O. Primary health care workers’ knowledge and attitudes towards depression and its management in the MeHPric-P project, Lagos, Nigeria. Gen. Hosp. Psychiatry 2017, 47, 1–6. [Google Scholar] [CrossRef]
- Kohrt, B.A.; Harper, I. Navigating diagnoses: Understanding mind-body relations, mental health, and stigma in Nepal. Cult. Med. Psychiatry 2008, 32, 462–491. [Google Scholar] [CrossRef] [Green Version]
- Ecks, S. Eating Drugs: Psychopharmaceutical Pluralism in India; NYU Press: New York, NY, USA, 2013. [Google Scholar]
- Spagnolo, J.; Champagne, F.; Leduc, N.; Melki, W.; Piat, M.; Laporta, M.; Bram, N.; Guesmi, I.; Charfi, F. “We find what we look for, and we look for what we know”: Factors interacting with a mental health training program to influence its expected outcomes in Tunisia. BMC Public Health 2018, 18, 1398. [Google Scholar] [CrossRef] [Green Version]
- Cuijpers, P.; Gentili, C. Psychological treatments are as effective as pharmacotherapies in the treatment of adult depression: A summary from Randomized Clinical Trials and neuroscience evidence. Res. Psychother. Psychopathol. Process Outcome 2017, 20, 273. [Google Scholar] [CrossRef] [Green Version]
- Kamenov, K.; Twomey, C.; Cabello, M.; Prina, A.M.; Ayuso-Mateos, J.L. The efficacy of psychotherapy, pharmacotherapy and their combination on functioning and quality of life in depression: A meta-analysis. Psychol. Med. 2017, 47, 414–425. [Google Scholar] [CrossRef] [Green Version]
- Iseselo, M.K.; Ambikile, J.S. Medication challenges for patients with severe mental illness: Experience and views of patients, caregivers and mental health care workers in Dar es Salaam, Tanzania. Int. J. Ment. Health Syst. 2017, 11, 17. [Google Scholar] [CrossRef] [Green Version]
- Padmanathan, P.; Singh, M.; Mannarath, S.C.; Omar, M.; Raja, S. A rapid appraisal of access to and utilisation of psychotropic medicines in Bihar, India. Int. J. Ment. Health Syst. 2014, 8, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Upadhaya, N.; Jordans, M.J.; Gurung, D.; Pokhrel, R.; Adhikari, R.P.; Komproe, I.H. Psychotropic drugs in Nepal: Perceptions on use and supply chain management. Glob. Health 2018, 14, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kola, L.; Kohrt, B.A.; Hanlon, C.; Naslund, J.A.; Sikander, S.; Balaji, M.; Benjet, C.; Cheung, E.Y.L.; Eaton, J.; Gonsalves, P.; et al. COVID-19 mental health impact and responses in low-income and middle-income countries: Reimagining global mental health. Lancet Psychiatry 2021, 8, 535–550. [Google Scholar] [CrossRef]
- McHugh, R.K.; Whitton, S.W.; Peckham, A.D.; Welge, J.A.; Otto, M.W. Patient preference for psychological vs. pharmacological treatment of psychiatric disorders: A meta-analytic review. J. Clin. Psychiatry 2013, 74, 595. [Google Scholar] [CrossRef]
- Lake, J.; Helgason, C.; Sarris, J. Integrative Mental Health (IMH): Paradigm, research, and clinical practice. Explore 2012, 8, 50–57. [Google Scholar] [CrossRef]
- Pham, T.V.; Kaiser, B.N.; Koirala, R.; Maharjan, S.M.; Upadhaya, N.; Franz, L.; Kohrt, B.A. Traditional Healers and Mental Health in Nepal: A Scoping Review. Cult. Med. Psychiatry 2021, 45, 97–140. [Google Scholar] [CrossRef]
- Pham, T.V.; Koirala, R.; Kohrt, B.A. Satisfaction in the Soul: Common Factors Theory Applied to Traditional Healers in Rural Nepal. Ethos 2020, 48, 93–128. [Google Scholar] [CrossRef]
- Pham, T.V.; Koirala, R.; Kohrt, B.A. Traditional and biomedical care pathways for mental well-being in rural Nepal. Int. J. Ment. Health Syst. 2021, 15, 4. [Google Scholar] [CrossRef]
- Pham, T.V.; Koirala, R.; Wainberg, M.L.; Kohrt, B.A. Reassessing the Mental Health Treatment Gap: What Happens if We Include the Impact of Traditional Healing on Mental Illness? Community Ment. Health J. 2021, 57, 777–791. [Google Scholar] [CrossRef]
- Kohrt, B.A.; Jordans, M.J.D.; Turner, E.L.; Sikkema, K.J.; Luitel, N.P.; Rai, S.; Singla, D.R.; Lamichhane, J.; Lund, C.; Patel, V. Reducing stigma among healthcare providers to improve mental health services (RESHAPE): Protocol for a pilot cluster randomized controlled trial of a stigma reduction intervention for training primary healthcare workers in Nepal. Pilot Feasibility Stud. 2018, 4, 36. [Google Scholar] [CrossRef]
- Kohrt, B.A. Social Neuroscience in Global Mental Health: Case Study on Stigma Reduction in Nepal. In Culture, Mind, and Brain: Emerging Concepts, Models, and Applications; Kirmayer, L.J., Worthman, C.M., Kitayama, S., Lemelson, R., Cummings, C.A., Eds.; Cambridge University Press: Cambridge, UK, 2020; pp. 440–451. [Google Scholar]
- Kohrt, B.A.; Turner, E.L.; Rai, S.; Bhardwaj, A.; Sikkema, K.J.; Adelekun, A.; Dhakal, M.; Luitel, N.P.; Lund, C.; Patel, V.; et al. Reducing mental illness stigma in healthcare settings: Proof of concept for a social contact intervention to address what matters most for primary care providers. Soc. Sci. Med. 2020, 250, 112852. [Google Scholar] [CrossRef] [PubMed]
- Kohrt, B.A.; Ottman, K.; Panter-Brick, C.; Konner, M.; Patel, V. Why we heal: The evolution of psychological healing and implications for global mental health. Clin. Psychol. Rev. 2020, 82, 101920. [Google Scholar] [CrossRef] [PubMed]
- Griffith, J.L.; Kohrt, B.A. Managing Stigma Effectively: What Social Psychology and Social Neuroscience Can Teach Us. Acad. Psychiatry 2016, 40, 339–347. [Google Scholar] [CrossRef] [PubMed]
- Kohrt, B.A.; Jordans, M.J.D.; Turner, E.L.; Rai, S.; Gurung, D.; Dhakal, M.; Bhardwaj, A.; Lamichhane, J.; Singla, D.R.; Lund, C.; et al. Collaboration with people with lived experience of mental illness to reduce stigma and improve primary care services in Nepal: A pilot cluster randomized clinical trial. JAMA Netw. Open 2021, 4, e2131475. [Google Scholar] [CrossRef]
- Lund, C.; Tomlinson, M.; De Silva, M.; Fekadu, A.; Shidhaye, R.; Jordans, M.; Petersen, I.; Bhana, A.; Kigozi, F.; Prince, M.; et al. PRIME: A programme to reduce the treatment gap for mental disorders in five low- and middle-income countries. PLoS Med. 2012, 9, e1001359. [Google Scholar] [CrossRef]
- Jordans, M.J.D.; Luitel, N.P.; Kohrt, B.A.; Rathod, S.D.; Garman, E.C.; De Silva, M.; Komproe, I.H.; Patel, V.; Lund, C. Community-, facility-, and individual-level outcomes of a district mental healthcare plan in a low-resource setting in Nepal: A population-based evaluation. PLoS Med. 2019, 16, e1002748. [Google Scholar] [CrossRef] [Green Version]
- Jordans, M.J.; Luitel, N.P.; Pokhrel, P.; Patel, V. Development and pilot testing of a mental healthcare plan in Nepal. Br. J. Psychiatry 2016, 208 (Suppl. S56), s21–s28. [Google Scholar] [CrossRef] [Green Version]
- Jordans, M.J.; Luitel, N.P.; Garman, E.; Kohrt, B.A.; Rathod, S.D.; Shrestha, P.; Komproe, I.H.; Lund, C.; Patel, V. Effectiveness of psychological treatments for depression and alcohol use disorder delivered by community-based counsellors: Two pragmatic randomised controlled trials within primary healthcare in Nepal. Br. J. Psychiatry 2019, 215, 485–493. [Google Scholar] [CrossRef] [Green Version]
- Rai, S.; Gurung, D.; Kaiser, B.N.; Sikkema, K.J.; Dhakal, M.; Bhardwaj, A.; Tergesen, C.; Kohrt, B.A. A service user co-facilitated intervention to reduce mental illness stigma among primary healthcare workers: Utilizing perspectives of family members and caregivers. Fam. Syst. Health 2018, 36, 198–209. [Google Scholar] [CrossRef]
- Kaiser, B.N.; Varma, S.; Carpenter-Song, E.; Sareff, R.; Rai, S.; Kohrt, B.A. Eliciting recovery narratives in global mental health: Benefits and potential harms in service user participation. Psychiatr. Rehabil. J. 2020, 43, 111–120. [Google Scholar] [CrossRef]
- QSR International. NVIVO Qualitative Data Analysis Software, 10th ed.; QSR International Pty Ltd.: Doncaster, Australia, 2012. [Google Scholar]
- MacQueen, K.M.; McLellan, E.; Kay, K.; Milstein, B. Codebook development for team-based qualitative analysis. Cam J. 1998, 10, 31–36. [Google Scholar] [CrossRef]
- Hennink, M.M.; Kaiser, B.N.; Marconi, V.C. Code Saturation Versus Meaning Saturation. Qual. Health Res. 2017, 27, 591–608. [Google Scholar] [CrossRef] [PubMed]
- Botega, N.; Mann, A.; Blizard, R.; Wilkinson, G. General practitioners and depression—First use of the Depression Attitude Questionnaire. Int. J. Methods Psychiatr. Res. 1992, 2, 169–180. [Google Scholar]
- Lempp, H.; Abayneh, S.; Gurung, D.; Kola, L.; Abdulmalik, J.; Evans-Lacko, S.; Semrau, M.; Alem, A.; Thornicroft, G.; Hanlon, C. Service user and caregiver involvement in mental health system strengthening in low-and middle-income countries: A cross-country qualitative study. Epidemiol. Psychiatr. Sci. 2018, 27, 29–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haddad, M.; Menchetti, M.; McKeown, E.; Tylee, A.; Mann, A. The development and psychometric properties of a measure of clinicians’ attitudes to depression: The revised Depression Attitude Questionnaire (R-DAQ). BMC Psychiatry 2015, 15, 7. [Google Scholar] [CrossRef] [Green Version]
- James, B.O.; Jenkins, R.; Lawani, A.O.; Omoaregba, J.O. Depression in primary care: The knowledge, attitudes and practice of general practitioners in Benin City, Nigeria. S. Afr. Fam. Pract. 2012, 54, 55–60. [Google Scholar] [CrossRef]
- Koschorke, M.; Oexle, N.; Ouali, U.; Cherian, A.V.; Deepika, V.; Mendon, G.B.; Gurung, D.; Kondratova, L.; Muller, M.; Lanfredi, M.; et al. Perspectives of healthcare providers, service users, and family members about mental illness stigma in primary care settings: A multi-site qualitative study of seven countries in Africa, Asia, and Europe. PLoS ONE 2021, 16, e0258729. [Google Scholar] [CrossRef]
- Patel, V.; Chowdhary, N.; Rahman, A.; Verdeli, H. Improving access to psychological treatments: Lessons from developing countries. Behav. Res. Ther. 2011, 49, 523–528. [Google Scholar] [CrossRef] [Green Version]
- Varma, S. Where There are only Doctors: Counselors as Psychiatrists in Indian-Administered Kashmir. Ethos 2012, 40, 517–535. [Google Scholar] [CrossRef]
- Gurung, D.; Upadhyaya, N.; Magar, J.; Giri, N.P.; Hanlon, C.; Jordans, M.J. Service user and care giver involvement in mental health system strengthening in Nepal: A qualitative study on barriers and facilitating factors. Int. J. Ment. Health Syst. 2017, 11, 30. [Google Scholar] [CrossRef] [Green Version]
- Givens, J.L.; Katz, I.R.; Bellamy, S.; Holmes, W.C. Stigma and the acceptability of depression treatments among African Americans and whites. J. Gen. Intern. Med. 2007, 22, 1292–1297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kohrt, B.A.; Hruschka, D.J. Nepali concepts of psychological trauma: The role of idioms of distress, ethnopsychology and ethnophysiology in alleviating suffering and preventing stigma. Cult. Med. Psychiatry 2010, 34, 322–352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jordans, M.J.; Keen, A.S.; Pradhan, H.; Tol, W.A. Psychosocial counselling in Nepal: Perspectives of counsellors and beneficiaries. Int. J. Adv. Couns. 2007, 29, 57–68. [Google Scholar] [CrossRef] [Green Version]
- Tergesen, C.L.; Gurung, D.; Dhungana, S.; Risal, A.; Basel, P.; Tamrakar, D.; Amatya, A.; Park, L.P.; Kohrt, B.A. Impact of Service User Video Presentations on Explicit and Implicit Stigma toward Mental Illness among Medical Students in Nepal: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2021, 18, 2143. [Google Scholar] [CrossRef]
- Gurung, D.; Poudyal, A.; Wang, Y.L.; Neupane, M.; Bhattarai, K.; Wahid, S.S.; Aryal, S.; Heim, E.; Gronholm, P.; Thornicroft, G.; et al. Stigma against mental health disorders in Nepal conceptualised with a ‘what matters most’ framework: A scoping review. Epidemiol. Psychiatr. Sci. 2022, 31, e11. [Google Scholar] [CrossRef] [PubMed]
- Kohrt, B.A.; Schafer, A.; Willhoite, A.; van’t Hof, E.; Pedersen, G.A.; Watts, S.; Ottman, K.; Carswell, K.; van Ommeren, M. Ensuring Quality in Psychological Support (WHO EQUIP): Developing a competent global workforce. World Psychiatry 2020, 19, 115–116. [Google Scholar] [CrossRef]
- Watts, S.; Hall, J.; Pedersen, G.A.; Ottman, K.; Carswell, K.; Van’t Hof, E.; Kohrt, B.A.; Schafer, A. The WHO EQUIP Foundational Helping Skills Trainer’s Curriculum. World Psychiatry 2021, 20, 449–450. [Google Scholar] [CrossRef]
- Kohrt, B.A.; Jordans, M.J.; Rai, S.; Shrestha, P.; Luitel, N.P.; Ramaiya, M.K.; Singla, D.R.; Patel, V. Therapist competence in global mental health: Development of the ENhancing Assessment of Common Therapeutic factors (ENACT) rating scale. Behav. Res. Ther. 2015, 69, 11–21. [Google Scholar] [CrossRef] [Green Version]
- Kohrt, B.A.; Mutamba, B.B.; Luitel, N.P.; Gwaikolo, W.; Onyango Mangen, P.; Nakku, J.; Rose, K.; Cooper, J.; Jordans, M.J.D.; Baingana, F. How competent are non-specialists trained to integrate mental health services in primary care? Global health perspectives from Uganda, Liberia, and Nepal. Int. Rev. Psychiatry 2018, 30, 182–198. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Day 1 a | Day 2 a | Day 3 a | Day 4 a | Day 5 | |
| Morning session | Introduction to training Objectives | * Aspirational figure testimonial, and common myths Introduction to psychosocial problems, causes and symptoms | * In-person PWLE recovery stories with Q&A Communication skills | Psychosocial skills training | Introduction to psychiatric diagnoses and mhGAP-IG |
| Afternoon session | Intro to mental health and psychosocial concept Pre-tests | Introduction to psychosocial support | Communication skills | Psychosocial skills training * Reducing Stigma | mhGAP curriculum |
| Day 6 | Day 7 | Day 8 | Day 9 | Day 10 a | |
| Morning session | Psychiatric history taking skills Epilepsy assessment, diagnosis | Depression and suicide assessment and diagnosis | Psychosis and bipolar assessment and diagnosis | Alcohol and drug use disorder assessment diagnosis and management * In-person PWLE recovery story with Q&A | Documentation and supervision |
| Afternoon session | * In-person PWLE recovery story with Q&A Clinical patient evaluation | * In-person PWLE recovery story with Q&A Clinical patient evaluation | * In-person PWLE recovery story with Q&A Clinical patient evaluation | * Challenges and barriers: collaborative problem solving | Post-test |
| Theme | Sub-Theme * | Description |
|---|---|---|
| PCPs’ reported attitudes prior to mental health training | (1) Stigma towards MH medications | Stigma exists towards those who take and those who prescribe medications for mental illnesses |
| (2) Focus on physical symptoms and treatment of those | PCPs focused on treating somatic symptoms rather than the underlying psychological ones and thus prescribed medications to treat the physical symptoms | |
| (3) Easy, cheap, and quick mode of treatment | Medications are perceived by healthcare workers to be easy to prescribe and a cost-effective method of treatment | |
| (4) Medications are the quick way back to normal | Perception that medications equate to a quick and easy way to get a MH patient back to doing daily activities | |
| PCP’s reported learning after training | (1) Endorsement of counseling | Healthcare workers became aware of the technique of counseling and endorsed the efficacy of counseling as a treatment for MH patients |
| (2) Listen and spend time with patients to understand their problems | Participants expressed the necessity to listen to patients to understand the root of the symptoms that brought he/she to the health post | |
| (3) Increased knowledge of mental illness | Through the training, PCPs expressed that their knowledge about MH disorders relevant to their geographic area had increased | |
| (4) Increased cooperation between prescribers and non-prescribers streamlined services | With the training, there has been an increase in the cooperation between the prescribers and non-prescribers helping serve the patients better. Non-prescribers perform counseling and can spend time with patients, then prescribers provide prescriptions. | |
| Attributions for changes in knowledge and attitudes | (1) Psychosocial content | Techniques for how to interact with people with MH disorders |
| (2) mhGAP content | General knowledge of mental health disorders | |
| (3) RESHAPE content | Addition of in-person PWLEs’ testimonials |
| Baseline Demographics | N (%) |
|---|---|
| Gender | |
| Female | 96 (46.8%) |
| Male | 109 (53.2%) |
| Age | |
| 21–29 years | 74 (36.1%) |
| 30–39 years | 56 (27.3%) |
| 40–49 years | 52 (25.4%) |
| 50+ years | 23 (11.2%) |
| Caste/Ethnicity | |
| High caste groups | 144 (70.2%) |
| Lower caste groups and ethnic minorities | 61 (29.8%) |
| Type of primary care provider | |
| Non-prescriber A | 95 (46.3%) |
| Prescriber B | 110 (53.7%) |
| Years working in healthcare servicesC | |
| <1 year | 10 (4.9%) |
| 1–5 years | 62 (30.2%) |
| 6–10 years | 25 (12.2%) |
| >10 years | 107 (52.2%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bhardwaj, A.; Gurung, D.; Rai, S.; Kaiser, B.N.; Cafaro, C.L.; Sikkema, K.J.; Lund, C.; Luitel, N.P.; Kohrt, B.A. Treatment Preferences for Pharmacological versus Psychological Interventions among Primary Care Providers in Nepal: Mixed Methods Analysis of a Pilot Cluster Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2022, 19, 2149. https://doi.org/10.3390/ijerph19042149
Bhardwaj A, Gurung D, Rai S, Kaiser BN, Cafaro CL, Sikkema KJ, Lund C, Luitel NP, Kohrt BA. Treatment Preferences for Pharmacological versus Psychological Interventions among Primary Care Providers in Nepal: Mixed Methods Analysis of a Pilot Cluster Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2022; 19(4):2149. https://doi.org/10.3390/ijerph19042149
Chicago/Turabian StyleBhardwaj, Anvita, Dristy Gurung, Sauharda Rai, Bonnie N. Kaiser, Cori L. Cafaro, Kathleen J. Sikkema, Crick Lund, Nagendra P. Luitel, and Brandon A. Kohrt. 2022. "Treatment Preferences for Pharmacological versus Psychological Interventions among Primary Care Providers in Nepal: Mixed Methods Analysis of a Pilot Cluster Randomized Controlled Trial" International Journal of Environmental Research and Public Health 19, no. 4: 2149. https://doi.org/10.3390/ijerph19042149