
Prolonged Sleep Latency and Reduced REM Latency Are Associated with Depressive Symptoms in a Japanese Working Population

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
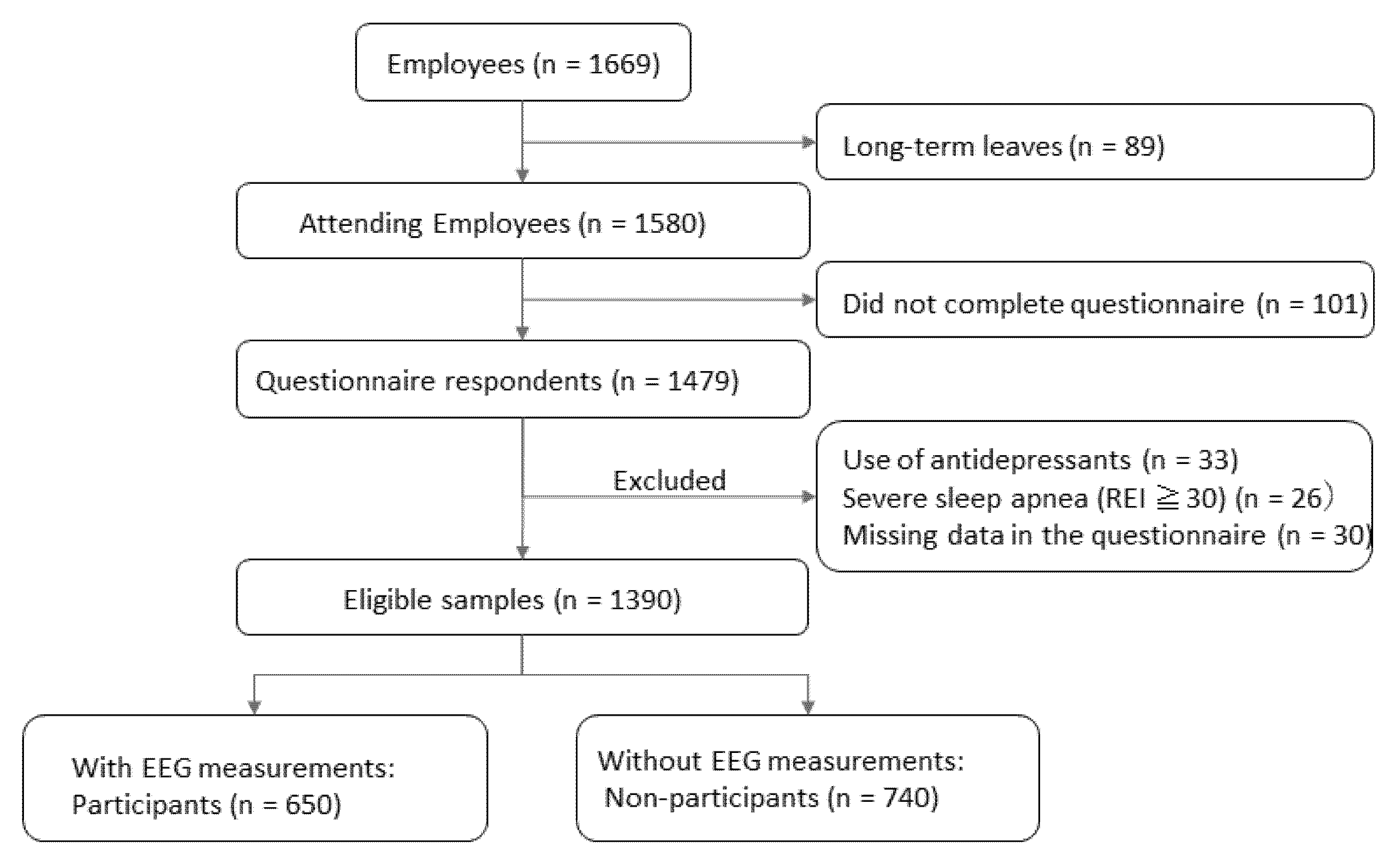
2.1. Participants
2.2. Questionnaires
2.3. Sleep Monitoring
2.4. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Murray, C.J.L.; Vos, T.; Lozano, R.; Naghavi, M.; Flaxman, A.D.; Michaud, C.; Ezzati, M.; Shibuya, K.; Salomon, J.A.; Abdalla, S.; et al. Disability-Adjusted Life Years (DALYs) for 291 Diseases and Injuries in 21 Regions, 1990–2010: A Systematic Analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2197–2223. [Google Scholar] [CrossRef]
- Rapaport, M.H.; Clary, C.; Fayyad, R.; Endicott, J. Quality-of-Life Impairment in Depressive and Anxiety Disorders. Am. J. Psychiatry 2005, 162, 1171–1178. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, J.; Almeida, T.C.; Ramos, C.; Sousa, S.; Brito, J. Bidirectional Relationship Between Perceived Stress and Insomnia Symptoms: The Role of Coping and Quality of Life. Sleep Biol. Rhythms 2021, 19, 23–31. [Google Scholar] [CrossRef]
- Kadotani, T.; Kadotani, H.; Arai, H.; Takami, M.; Ito, H.; Matsuo, M.; Yamada, N. Comparison of Self-Reported Scales and Structured Interviews for the Assessment of Depression in an Urban Male Working Population in Japan: A Cross-Sectional Survey. Sleep Sci. Pract. 2017, 1, 9. [Google Scholar] [CrossRef] [Green Version]
- Kawakami, N.; Takeshima, T.; Ono, Y.; Uda, H.; Hata, Y.; Nakane, Y.; Nakane, H.; Iwata, N.; Furukawa, T.A.; Kikkawa, T. Twelve-Month Prevalence, Severity, and Treatment of Common Mental Disorders in Communities in Japan: Preliminary Finding from the World Mental Health Japan Survey 2002–2003. Psychiatry Clin. Neurosci. 2005, 59, 441–452. [Google Scholar] [CrossRef]
- Pigeon, W.R.; Bishop, T.M.; Krueger, K.M. Insomnia as a Precipitating Factor in New Onset Mental Illness: A Systematic Review of Recent Findings. Curr. Psychiatry Rep. 2017, 19, 44. [Google Scholar] [CrossRef]
- Hertenstein, E.; Feige, B.; Gmeiner, T.; Kienzler, C.; Spiegelhalder, K.; Johann, A.; Jansson-Fröjmark, M.; Palagini, L.; Rücker, G.; Riemann, D.; et al. Insomnia as a Predictor of Mental Disorders: A Systematic Review and Meta-Analysis. Sleep Med. Rev. 2019, 43, 96–105. [Google Scholar] [CrossRef]
- Sunderajan, P.; Gaynes, B.N.; Wisniewski, S.R.; Miyahara, S.; Fava, M.; Akingbala, F.; DeVeaugh-Geiss, J.; Rush, A.J.; Trivedi, M.H. Insomnia in Patients with Depression: A STAR*D Report. CNS Spectr. 2010, 15, 394–404. [Google Scholar] [CrossRef]
- Nutt, D.J.; Wilson, S.; Paterson, L. Sleep Disorders as Core Symptoms of Depression. Dialogues Clin. Neurosci. 2008, 10, 329–336. [Google Scholar] [CrossRef]
- IsHak, W.W.; Bagot, K.; Thomas, S.; Magakian, N.; Bedwani, D.; Larson, D.; Brownstein, A.; Zaky, C. Quality of Life in Patients Suffering from Insomnia. Innov. Clin. Neurosci. 2012, 9, 13–26. [Google Scholar]
- Pillai, V.; Kalmbach, D.A.; Ciesla, J.A. A Meta-Analysis of Electroencephalographic Sleep in Depression: Evidence for Genetic Biomarkers. Biol. Psychiatry 2011, 70, 912–919. [Google Scholar] [CrossRef] [PubMed]
- Chesson, A.L.; Berry, R.B.; Pack, A.; American Academy of Sleep Medicine; American Thoracic Society; American College of Chest Physicians. Practice Parameters for the Use of Portable Monitoring Devices in the Investigation of Suspected Obstructive Sleep Apnea in Adults. Sleep 2003, 26, 907–913. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoshida, M.; Kashiwagi, K.; Kadotani, H.; Yamamoto, K.; Koike, S.; Matsuo, M.; Yamada, N.; Okawa, M.; Urade, Y. Validation of a Portable Single-Channel EEG Monitoring System. J. Oral Sleep Med. 2015, 1, 140–147. [Google Scholar]
- Matsuo, M.; Masuda, F.; Sumi, Y.; Takahashi, M.; Yamada, N.; Ohira, M.H.; Fujiwara, K.; Kanemura, T.; Kadotani, H. Comparisons of Portable Sleep Monitors of Different Modalities: Potential as Naturalistic Sleep Recorders. Front. Neurol. 2016, 7, 110. [Google Scholar] [CrossRef] [PubMed]
- Takami, M.; Kadotani, H.; Nishikawa, K.; Sumi, Y.; Nakabayashi, T.; Fujii, Y.; Matsuo, M.; Yamada, N. Quality of Life, Depression, and Productivity of City Government Employees in Japan: A Comparison Study Using the Athens Insomnia Scale and Insomnia Severity Index. Sleep Sci. Pract. 2018, 2, 4. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W. The PHQ-9: Validity of a Brief Depression Severity Measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Levis, B.; Benedetti, A.; Thombs, B.D.; DEPRESsion Screening Data (DEPRESSD) Collaboration. Accuracy of Patient Health Questionnaire-9 (PHQ-9) for Screening to Detect Major Depression: Individual Participant Data Meta-Analysis. BMJ 2019, 365, l1476. [Google Scholar] [CrossRef] [Green Version]
- Berry, R.; Albertario, C.; Harding, S.; Lloyd, R.M.; Plante, D.T.; Quan, S.F.; Troester, M.M.; Vaughn, B.V.; for the American Academy of Sleep Medicine. The AASM Manual for the Scoring of Sleep and Associated Events. Ver 2.5; American Academy of Sleep Medicine: Darien, IL, USA, 2018. [Google Scholar]
- Organization for Economic Co-Operation and Development. Time Use Across the World. Gend Data Portal. 2020. Available online: https://www.oecd.org/gender/data/OECD_1564_TUSupdatePortal.xlsx (accessed on 30 November 2021).
- Ma, Y.; Goldstein, M.R.; Davis, R.B.; Yeh, G.Y. Profile of Subjective-Objective Sleep Discrepancy in Patients with Insomnia and Sleep Apnea. J. Clin. Sleep Med. 2021, 17, 2155–2163. [Google Scholar] [CrossRef]
- Tsuchiyama, K.; Nagayama, H.; Kudo, K.; Kojima, K.; Yamada, K. Discrepancy Between Subjective and Objective Sleep in Patients with Depression. Psychiatry Clin. Neurosci. 2003, 57, 259–264. [Google Scholar] [CrossRef]
- Zhai, L.; Zhang, H.; Zhang, D. Sleep Duration and Depression Among Adults: A Meta-Analysis of Prospective Studies. Depress. Anxiety 2015, 32, 664–670. [Google Scholar] [CrossRef]
- Yu, J.; Rawtaer, I.; Fam, J.; Jiang, M.J.; Feng, L.; Kua, E.H.; Mahendran, R. Sleep Correlates of Depression and Anxiety in an Elderly Asian Population. Psychogeriatrics 2016, 16, 191–195. [Google Scholar] [CrossRef]
- Mason, E.C.; Harvey, A.G. Insomnia Before and After Treatment for Anxiety and Depression. J. Affect. Disord. 2014, 168, 415–421. [Google Scholar] [CrossRef] [PubMed]
- Tsuno, N.; Besset, A.; Ritchie, K. Sleep and Depression. J. Clin. Psychiatry 2005, 66, 1254–1269. [Google Scholar] [CrossRef] [PubMed]
- Palagini, L.; Baglioni, C.; Ciapparelli, A.; Gemignani, A.; Riemann, D. REM Sleep Dysregulation in Depression: State of the Art. Sleep Med. Rev. 2013, 17, 377–390. [Google Scholar] [CrossRef]
- Mendlewicz, J. Sleep Disturbances: Core Symptoms of Major Depressive Disorder Rather Than Associated or Comorbid Disorders. World J. Biol. Psychiatry 2009, 10, 269–275. [Google Scholar] [CrossRef] [PubMed]
- Clark, C.; Dupont, R.; Golshan, S.; Gillin, J.C.; Rapaport, M.H.; Kelsoe, J.R. Preliminary Evidence of an Association Between Increased REM Density and Poor Antidepressant Response to Partial Sleep Deprivation. J. Affect. Disord. 2000, 59, 77–83. [Google Scholar] [CrossRef]
- Sandor, P.; Shapiro, C.M. Sleep Patterns in Depression and Anxiety: Theory and Pharmacological Effects. J. Psychosom. Res. 1994, 38 (Suppl. 1), 125–139. [Google Scholar] [CrossRef]
- Wilson, S.; Argyropoulos, S. Antidepressants and Sleep: A Qualitative Review of the Literature. Drugs 2005, 65, 927–947. [Google Scholar] [CrossRef]
- Argyropoulos, S.V.; Wilson, S.J. Sleep Disturbances in Depression and the Effects of Antidepressants. Int. Rev. Psychiatry 2005, 17, 237–245. [Google Scholar] [CrossRef]
- Wang, Y.Q.; Li, R.; Zhang, M.Q.; Zhang, Z.; Qu, W.M.; Huang, Z.L. The Neurobiological Mechanisms and Treatments of REM Sleep Disturbances in Depression. Curr. Neuropharmacol. 2015, 13, 543–553. [Google Scholar] [CrossRef] [Green Version]
- Tazawa, Y.; Wada, M.; Mitsukura, Y.; Takamiya, A.; Kitazawa, M.; Yoshimura, M.; Mimura, M.; Kishimoto, T. Actigraphy for Evaluation of Mood Disorders: A Systematic Review and Meta-Analysis. J. Affect. Disord. 2019, 253, 257–269. [Google Scholar] [CrossRef] [PubMed]
- Bromet, E.; Andrade, L.H.; Hwang, I.; Sampson, N.A.; Alonso, J.; de Girolamo, G.; de Graaf, R.; Demyttenaere, K.; Hu, C.; Iwata, N.; et al. Cross-National Epidemiology of DSM-IV Major Depressive Episode. BMC Med. 2011, 9, 90. [Google Scholar] [CrossRef] [PubMed]
- Wilsmore, B.R.; Grunstein, R.R.; Fransen, M.; Woodward, M.; Norton, R.; Ameratunga, S. Sleep Habits, Insomnia, and Daytime Sleepiness in a Large and Healthy Community-Based Sample of New Zealanders. J. Clin. Sleep Med. 2013, 9, 559–566. [Google Scholar] [CrossRef] [PubMed]
- Plante, D.T.; Finn, L.A.; Hagen, E.W.; Mignot, E.; Peppard, P.E. Subjective and Objective Measures of Hypersomnolence Demonstrate Divergent Associations with Depression Among Participants in the Wisconsin Sleep Cohort Study. J. Clin. Sleep Med. 2016, 12, 571–578. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Variable | Participants | Non-Participants | p-Value |
|---|---|---|---|
| (n = 650) | (n = 740) | ||
| Male, n (%) | 268 (41.2) | 222 (30.0) | <0.001 |
| Age, yrs. (SD) | 44.7 (11.5) | 46.6 (12.9) | 0.003 |
| BMI, kg/m2 (SD) | 22.3 (3.32) | 22.5 (3.70) | 0.900 |
| PHQ-9 score (SD) | 4.79 (4.77) | 3.90 (4.33) | <0.001 |
| Depressive symptoms, n (%) | 134 (20.6) | 163 (22.0) | 0.522 |
| Subjective sleep duration, min (SD) | 362 (70.6) | 382 (74.3) | <0.001 |
| SPT, min (SD) | 364 (79.1) | - | |
| SL, min (SD) | 18.0 (15.4) | - | |
| REML, min (SD) | 78.2 (38.6) | - | |
| SE, % | 87.0 (6.80) | - | |
| TST, min (SD) | 335 (72.6) | - | |
| WASO, min (SD) | 28.7 (22.6) | - |
| No Depressive Symptoms (PHQ-9 < 10) | Depressive Symptoms (PHQ-9 ≥ 10) | p-Value | |
|---|---|---|---|
| (n = 516) | (n = 134) | ||
| Age, years, mean (SD) | 44.8 (11.5) | 42.2 (11.5) | 0.575 |
| Male, n (%) | 221 (42.8) | 47 (35.1) | 0.063 |
| BMI, kg/m2, mean (SD) | 22.3 (3.32) | 22.7 (3.31) | 0.205 |
| SPT, min (SD) | 362 (78.9) | 369 (79.9) | 0.360 |
| SL, min (SD) | 17.3 (13.8) | 20.7 (20.3) | 0.024 |
| REML, min (SD) | 79.9 (39.5) | 71.7 (34.3) | 0.027 |
| Awakening, times (SD) | 24.8 (12.1) | 25.6 (11.6) | 0.451 |
| δ-power value of the first sleep cycle, μV2/min (SD) | 2220 (1700) | 2050 (1330) | 0.284 |
| SE, % | 87.0 (6.74) | 87.1 (7.06) | 0.871 |
| Model Terms | OR | 95% CI | p-Value |
|---|---|---|---|
| Age | |||
| 1-year increment | 0.98 | 0.96–1.00 | 0.108 |
| BMI | |||
| 1-unit increment | 1.06 | 0.99–1.12 | 0.056 |
| Sex | |||
| Female | 1.38 | 0.85–2.24 | 0.187 |
| Occupation | |||
| Management and clerical | 1.00 | Reference | |
| Educational instruction | 0.89 | 0.52–1.51 | 0.656 |
| Healthcare and healthcare support | 0.90 | 0.45–1.78 | 0.755 |
| Temporary and commissioned | 1.92 | 0.73–5.01 | 0.187 |
| Others | 1.53 | 0.53–4.39 | 0.428 |
| SPT | |||
| 1-min increment | 1.00 | 0.99–1.00 | 0.735 |
| SL | |||
| 1-min increment | 1.02 | 1.01–1.04 | 0.009 |
| REML | |||
| 1-min increment | 0.99 | 0.99–1.00 | 0.040 |
| Awakening | |||
| 1-time increment | 1.02 | 0.99–1.04 | 0.127 |
| δ-power value of the first sleep stage per minute | |||
| 1 increment | 1.00 | 1.00–1.00 | 0.114 |
| SE | |||
| 1-percent increment | 1.05 | 0.99–1.11 | 0.056 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Omichi, C.; Kadotani, H.; Sumi, Y.; Ubara, A.; Nishikawa, K.; Matsuda, A.; Ozeki, Y.; the NinJaSleep Study Group. Prolonged Sleep Latency and Reduced REM Latency Are Associated with Depressive Symptoms in a Japanese Working Population. Int. J. Environ. Res. Public Health 2022, 19, 2112. https://doi.org/10.3390/ijerph19042112
Omichi C, Kadotani H, Sumi Y, Ubara A, Nishikawa K, Matsuda A, Ozeki Y, the NinJaSleep Study Group. Prolonged Sleep Latency and Reduced REM Latency Are Associated with Depressive Symptoms in a Japanese Working Population. International Journal of Environmental Research and Public Health. 2022; 19(4):2112. https://doi.org/10.3390/ijerph19042112
Chicago/Turabian StyleOmichi, Chie, Hiroshi Kadotani, Yukiyoshi Sumi, Ayaka Ubara, Kohei Nishikawa, Arichika Matsuda, Yuji Ozeki, and the NinJaSleep Study Group. 2022. "Prolonged Sleep Latency and Reduced REM Latency Are Associated with Depressive Symptoms in a Japanese Working Population" International Journal of Environmental Research and Public Health 19, no. 4: 2112. https://doi.org/10.3390/ijerph19042112