
Participants’ Perspective of Engaging in a Gym-Based Health Service Delivered Secondary Stroke Prevention Program after TIA or Mild Stroke

Abstract
:1. Introduction
2. Materials and Methods
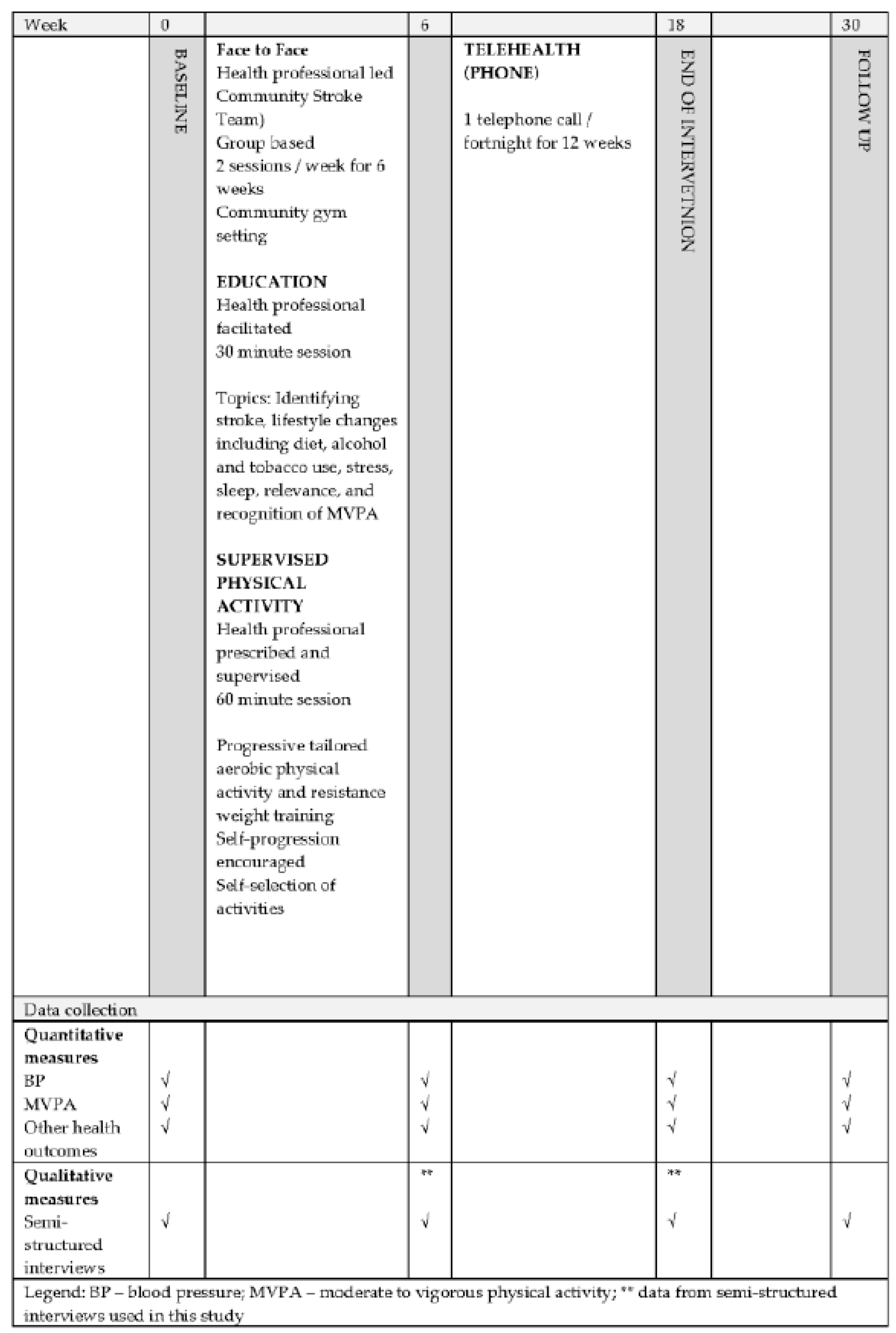
2.1. Study Design
2.2. Context
2.3. Recruitment
2.4. Sample
2.5. Generating Data
2.6. Data Analysis
2.7. Trustworthiness
3. Results
3.1. Results
3.2. Findings
3.3. What It Offered Me
3.3.1. Health Professional Support
- In person
- Helpful information
- Telehealth-based health coaching
3.3.2. Being in a Group
- Mutual support
- Exercising with others
3.3.3. Meeting My Needs
- Experience MVPA
- Convenience
3.4. What I Got out of It
3.4.1. Making Changes
- Thinking differently
- Doing it myself
3.4.2. Feeling Better
- Sense of fitness
- Psychological factors
4. Discussion
Implications for Policy and Practice
- Consistent face-to-face health professional interaction is critical for guidance, feedback, and support;
- A group setting offers the opportunity to share experiences, model exercise behaviour and offer relatedness through peer support;
- Tailoring interventions is necessary to meet individual needs and foster autonomy.
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Easton, J.D.; Saver, J.L.; Albers, G.W.; Alberts, M.J.; Chaturvedi, S.; Feldmann, E.; Hatsukami, T.S.; Higashida, R.T.; Johnston, S.C.; Kidwell, C.S.; et al. Definition and Evaluation of Transient Ischemic Attack. Stroke 2009, 40, 2276–2293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mendelson, S.J.; Prabhakaran, S. Diagnosis and Management of Transient Ischemic Attack and Acute Ischemic Stroke: A Review. JAMA 2021, 325, 1088–1098. [Google Scholar] [CrossRef]
- Roberts, P.S.; Krishnan, S.; Burns, S.P.; Ouellette, D.; Pappadis, M.R. Inconsistent Classification of Mild Stroke and Implications on Health Services Delivery. Arch. Phys. Med. Rehabil. 2020, 101, 1243–1259. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, J.K.; Capo-Lugo, C.E.; Akinwuntan, A.E.; Roberts, P.; Krishnan, S.; Belagaje, S.R.; Kovic, M.; Burns, S.P.; Hu, X.; Danzl, M.; et al. Classification of Mild Stroke: A Mapping Review. PMR 2019, 11, 996–1003. [Google Scholar] [CrossRef]
- Lynch, E.A.; Mackintosh, S.F.; Luker, J.A.; Hillier, S.L. Access to rehabilitation for patients with stroke in Australia. Med. J. Aust. 2019, 210, 21–26. [Google Scholar] [CrossRef] [Green Version]
- Faux, S.G.; Arora, P.; Shiner, C.T.; Thompson-Butel, A.G.; Klein, L.A. Rehabilitation and education are underutilized for mild stroke and TIA sufferers. Disabil. Rehabil. 2018, 40, 1480–1484. [Google Scholar] [CrossRef]
- Lioutas, V.-A.; Ivan, C.S.; Himali, J.J.; Aparicio, H.J.; Leveille, T.; Romero, J.R.; Beiser, A.S.; Seshadri, S. Incidence of Transient Ischemic Attack and Association With Long-term Risk of Stroke. JAMA 2021, 325, 373–381. [Google Scholar] [CrossRef] [PubMed]
- Fini, N.A.; Bernhardt, J.; Churilov, L.; Clark, R.; Holland, A.E. Adherence to physical activity and cardiovascular recommendations during the 2years after stroke rehabilitation discharge. Ann. Phys. Rehabil. Med. 2021, 64, 101455. [Google Scholar] [CrossRef] [PubMed]
- Ushio, M.; Kanaoka, M.; Kinoshita, Y.; Maeno, S.; Fujita, K. Moderate-to-vigorous physical activity and the risk of stroke recurrence in patients with a history of minor ischemic stroke in Japan: A retrospective analysis. Top Stroke Rehabil. 2018, 25, 591–598. [Google Scholar] [CrossRef]
- Deijle, I.A.; Van Schaik, S.M.; Van Wegen, E.E.; Weinstein, H.C.; Kwakkel, G.; Van den Berg-Vos, R.M. Lifestyle Interventions to Prevent Cardiovascular Events After Stroke and Transient Ischemic Attack: Systematic Review and Meta-Analysis. Stroke 2017, 48, 174–179. [Google Scholar] [CrossRef]
- Prior, P.L.; Suskin, N. Exercise for stroke prevention. Stroke Vasc. Neurol. 2018, 3, 59–68. [Google Scholar] [CrossRef]
- Faulkner, J.; Lambrick, D.; Woolley, B.; Stoner, L.; Wong, L.; McGonigal, G. Early Engagement in Exercise Improves Coronary Artery Disease Risk in Newly Diagnosed Transient Ischemic Attack Patients. Int. J. Stroke 2013, 8, E29. [Google Scholar] [CrossRef]
- Woolley, B.; Stoner, L.; Lark, S.; Wong, L.; Lanford, J.; Faulkner, J. Effect of early exercise engagement on arterial stiffness in patients diagnosed with a transient ischaemic attack. J. Hum. Hypertens. 2015, 29, 87–91. [Google Scholar] [CrossRef]
- Stroke Foundation. Clincial Guidelines for Stroke Manangement; Stroke Foundation: Melbourne, Australia, 2021. [Google Scholar]
- MacKay-Lyons, M.; Billinger, S.A.; Eng, J.J.; Dromerick, A.; Giacomantonio, N.; Hafer-Macko, C.; Macko, R.; Nguyen, E.; Prior, P.; Suskin, N.; et al. Aerobic Exercise Recommendations to Optimize Best Practices in Care After Stroke: AEROBICS 2019 Update. Phys. Ther. 2020, 100, 149–156. [Google Scholar] [CrossRef] [PubMed]
- Kleindorfer, D.O.; Towfighi, A.; Chaturvedi, S.; Cockroft, K.M.; Gutierrez, J.; Lombardi-Hill, D.; Kamel, H.; Kernan, W.N.; Kittner, S.J.; Leira, E.C.; et al. 2021 Guideline for the Prevention of Stroke in Patients With Stroke and Transient Ischemic Attack: A Guideline From the American Heart Association/American Stroke Association. Stroke 2021, 52, e364–e467. [Google Scholar] [CrossRef] [PubMed]
- Boss, H.M.; Deijle, I.A.; Van Schaik, S.M.; de Melker, E.C.; van den Berg, B.T.J.; Weinstein, H.C.; Geerlings, M.I.; Kappelle, L.J.; Van den Berg-Vos, R.M. Cardiorespiratory Fitness after Transient Ischemic Attack and Minor Ischemic Stroke: Baseline Data of the MoveIT Study. J. Stroke Cereb. Dis. 2017, 26, 1114–1120. [Google Scholar] [CrossRef] [PubMed]
- Hendrickx, W.; Vlietstra, L.; Valkenet, K.; Wondergem, R.; Veenhof, C.; English, C.; Pisters, M.F. General lifestyle interventions on their own seem insufficient to improve the level of physical activity after stroke or TIA: A systematic review. BMC Neurol. 2020, 20, 168. [Google Scholar] [CrossRef] [PubMed]
- Faulkner, J.; Stoner, L.; Lanford, J.; Jolliffe, E.; Mitchelmore, A.; Lambrick, D. Long-Term Effect of Participation in an Early Exercise and Education Program on Clinical Outcomes and Cost Implications, in Patients with TIA and Minor, Non-Disabling Stroke. Transl. Stroke Res. 2017, 8, 220–227. [Google Scholar] [CrossRef] [Green Version]
- Heron, N.; O’Connor, S.; Kee, F.; Mant, J.; Cupples, M.; Donnelly, M. Usability and Acceptability of a Novel Secondary Prevention Initiative Targeting Physical Activity for Individuals after a Transient Ischaemic Attack or “Minor” Stroke: A Qualitative Study. Int. J. Env. Res. Public Health 2020, 17, 8788. [Google Scholar] [CrossRef]
- Janssen, H.; Catchpole, C.; Sweetapple, A.; Mason, G.; Colvin, D.; Carlos, A.; English, C.; Ada, L.; Callister, R.; Sammut, M.; et al. Supporting Lifestyle and Activity Modification after a Transient Ischemic Attack (S+SLAM-TIA): Measuring the Value of Implementing an Evidence Based Secondary Stroke Prevention Program into a Health Service; NSW Government Agency for Clinical Innovation: St Leonards, Australia, 2018. [Google Scholar]
- Turner, G.M.; McMullan, C.; Atkins, L.; Foy, R.; Mant, J.; Calvert, M. TIA and minor stroke: A qualitative study of long-term impact and experiences of follow-up care. BMC Fam. Pract. 2019, 20, 176. [Google Scholar] [CrossRef] [Green Version]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Charmaz, K. Constructing Grounded Theory, 2nd ed.; SAGE Publications: London, UK, 2014. [Google Scholar]
- Neergaard, M.A.; Olesen, F.; Andersen, R.S.; Sondergaard, J. Qualitative description—The poor cousin of health research? BMC Med Res. Methodol. 2009, 9, 52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sandelowski, M. Whatever happened to qualitative description? Res. Nurs. Health 2000, 23, 334–340. [Google Scholar] [CrossRef]
- Chafe, R. The Value of Qualitative Description in Health Services and Policy Research. Health Policy 2017, 12, 12–18. [Google Scholar] [CrossRef] [Green Version]
- Janssen, H. Supporting Lifestyle and Activity Modification After a Transient Ischaemic Attack; Australian Government NSW Ministry of Health, Ed.; Agency for Clincial Innovation: Sydney, Australia, 2018. [Google Scholar]
- Geldens, N.; Crowfoot, G.; Sweetapple, A.; Vyslysel, G.; Mason, G.; English, C.; Janssen, H. Patient readiness for risk-reduction education and lifestyle change following transient ischemic attack. Disabil. Rehabil. 2021, 43, 400–405. [Google Scholar] [CrossRef]
- QSR International Pty Ltd. Nvivo Version 12.1; QSR International: Doncaster, Australia, 2020. [Google Scholar]
- Lincoln, Y.; Guba, E. Establishing Trustworthiness. In Naturalistic Inquiry; Sage: Newbury Park, CA, USA, 1985; pp. 295–297. [Google Scholar]
- Sammut, M.; Fini, N.; Haracz, K.; Nilsson, M.; English, C.; Janssen, H. Increasing time spent engaging in moderate-to-vigorous physical activity by community-dwelling adults following a transient ischemic attack or non-disabling stroke: A systematic review. Disabil. Rehabil. 2020, 42, 1–16. [Google Scholar] [CrossRef]
- Sammut, M.; Haracz, K.D.S.; Crowfoot, G.; Fini, N.; Nilsson, M.; English, C.; Janssen, H. Physical Activity after Transient Ischemic Attack and Mild Stroke is ‘Business as usual’; University of Newcastle: Callaghan, Australia, 2020. [Google Scholar]
- Brouwer-Goossensen, D.; den Hertog, H.M.; Mastenbroek-de Jong, M.A.; van Gemert-Pijnen, L.J.E.W.C.; Taal, E. Patient perspectives on health-related behavior change after transient ischemic attack or ischemic stroke. Brain Behav. 2021, 11, e01993. [Google Scholar] [CrossRef] [PubMed]
- Débora Pacheco, B.; Guimarães Caetano, L.C.; Amorim Samora, G.; Sant’Ana, R.; Fuscaldi Teixeira-Salmela, L.; Scianni, A.A. Perceived barriers to exercise reported by individuals with stroke, who are able to walk in the community. Disabil. Rehabil. 2021, 43, 331–337. [Google Scholar] [CrossRef]
- Morris, J.H.; Oliver, T.; Kroll, T.; Joice, S.; Williams, B. Physical activity participation in community dwelling stroke survivors: Synergy and dissonance between motivation and capability. A qualitative study. Physiotherapy 2017, 103, 311–321. [Google Scholar] [CrossRef] [Green Version]
- Jansson, A.-S.B.; Carlsson, G. Physical activity on prescription at the time of stroke or transient ischemic attack diagnosis—From a patient perspective. Disabil. Rehabil. 2021, 43, 1121–1128. [Google Scholar] [CrossRef]
- Howlett, N.; Trivedi, D.; Troop, N.A.; Chater, A.M. Are physical activity interventions for healthy inactive adults effective in promoting behavior change and maintenance, and which behavior change techniques are effective? A systematic review and meta-analysis. Transl. Behav. Med. 2018, 9, 147–157. [Google Scholar] [CrossRef] [PubMed]
- Ntoumanis, N.; Ng, J.Y.Y.; Prestwich, A.; Quested, E.; Hancox, J.E.; Thøgersen-Ntoumani, C.; Deci, E.L.; Ryan, R.M.; Lonsdale, C.; Williams, G.C. A meta-analysis of self-determination theory-informed intervention studies in the health domain: Effects on motivation, health behavior, physical, and psychological health. Health Psychol. Rev. 2021, 15, 214–244. [Google Scholar] [CrossRef] [Green Version]
- Ryan, R.M. Promoting Health Through Autonomy Rather than Control. In ISBNPA Theories of Motivation Webinar: Understanding and Changing Health Behaviours from a Self-Determination Theory 2015; ISBNPA: Phoenix, AZ, USA, 2015. [Google Scholar]
- Murcia, J.; Román, M.; Galindo, C.; Alonso, N.; González-Cutre, D. Peers’ Influence on Exercise Enjoyment: A Self-Determination Theory Approach. J. Sports Sci. Med. 2008, 7, 23–31. [Google Scholar] [PubMed]
- Vansteenkiste, M.; Ryan, R.; Soenens, B. Basic psychological need theory: Advancements, critical themes, and future directions. Motiv. Emot. 2020, 44, 1–31. [Google Scholar] [CrossRef] [Green Version]
- Teixeira, P.J.; Carraça, E.V.; Markland, D.; Silva, M.N.; Ryan, R.M. Exercise, physical activity, and self-determination theory: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ng, J.Y.Y.; Ntoumanis, N.; Thøgersen-Ntoumani, C.; Deci, E.; Ryan, R.; Duda, J.; Williams, G. Self-Determination Theory Applied to Health Contexts: A Meta-Analysis. Perspect. Psychol. Sci. 2012, 7, 325–340. [Google Scholar] [CrossRef]
- Gillison, F.B.; Rouse, P.; Standage, M.; Sebire, S.J.; Ryan, R.M. A meta-analysis of techniques to promote motivation for health behaviour change from a self-determination theory perspective. Health Psychol. Rev. 2019, 13, 110–130. [Google Scholar] [CrossRef]
- Ryan, R.M.; Deci, E.L. Self-Determination Theory: Basic Psychological Needs in Motivation, Development and Wellness; Guilford Press: New York, NY, USA, 2017; Volume 38, p. 231. [Google Scholar]
- Deci, E.L.; Ryan, R.M. Self-determination theory in health care and its relations to motivational interviewing: A few comments. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 24. [Google Scholar] [CrossRef] [Green Version]
- Deci, E.L.; Olafsen, A.H.; Ryan, R.M. Self-determination Theory in work organisations: The state of a science. Annu. Rev. Organ. Psychol. Organ. Behavour. 2017, 4, 19–43. [Google Scholar] [CrossRef]
- Aitken, D.; Buchbinder, R.; Jones, G.; Winzenberg, T. Interventions to improve adherence to exercise for chronic musculoskeletal pain in adults. Aust. Fam. Physician 2015, 44, 39–42. [Google Scholar] [PubMed]
- Yalom, I.D.; Leszcz, M. Theory and Practice of Group Psychotherapy, 5th ed.; Basic Books: New York, NY, USA, 2008. [Google Scholar]


{kind=link}
| Characteristic | Participants (n = 30) |
|---|---|
| Age (years), mean (SD), range | 66 (10), 42 to 86 |
| ≤65, n (%) | 15 (50) |
| ≥66 n (%) | 15 (50) |
| Sex, n (%) | |
| Female | 13 (43) |
| BMI, (kg/m2), n (%) | |
| Normal (≤24.9) | 8 (27) |
| Overweight (25–29.5) | 10 (33) |
| Obese (≥ 30) | 12 (40) |
| Diagnosis, n (%) | |
| TIA | 10 (33) |
| Ischemic stroke | 16 (54) |
| Haemorrhagic stroke | 4 (13) |
| Time since stroke event (days), mean (SD) n=28 | 160 (137) |
| Fatigue Assessment score at baseline, n (%) | |
| Fatigue (24–34) | 9 (30) |
| Severe fatigue (≥ 35) | 2 (7) |
| Depression, Anxiety and Stress Scale (DASS) score ≥ 7, n (%) | |
| Cumulative total | 21 (70) |
| Depression | 12 (40) |
| Anxiety | 13 (43) |
| Stress | 17 (57) |
| CONCEPT | CATEGORY | SUBCATEGORY |
|---|---|---|
| WHAT IT OFFERED ME | Health Professional support | In-person Helpful Information Telehealth-based health coaching |
| Being in a group | Mutual support Exercising with others | |
| Meeting my needs | Experiencing MVPA Convenience | |
| WHAT I GOT OUT OF IT | Making changes | Thinking differently Doing it myself |
| Feeling better | Sense of fitness Psychological factors |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sammut, M.; Haracz, K.; English, C.; Shakespeare, D.; Crowfoot, G.; Nilsson, M.; Janssen, H. Participants’ Perspective of Engaging in a Gym-Based Health Service Delivered Secondary Stroke Prevention Program after TIA or Mild Stroke. Int. J. Environ. Res. Public Health 2021, 18, 11448. https://doi.org/10.3390/ijerph182111448
Sammut M, Haracz K, English C, Shakespeare D, Crowfoot G, Nilsson M, Janssen H. Participants’ Perspective of Engaging in a Gym-Based Health Service Delivered Secondary Stroke Prevention Program after TIA or Mild Stroke. International Journal of Environmental Research and Public Health. 2021; 18(21):11448. https://doi.org/10.3390/ijerph182111448
Chicago/Turabian StyleSammut, Maria, Kirsti Haracz, Coralie English, David Shakespeare, Gary Crowfoot, Michael Nilsson, and Heidi Janssen. 2021. "Participants’ Perspective of Engaging in a Gym-Based Health Service Delivered Secondary Stroke Prevention Program after TIA or Mild Stroke" International Journal of Environmental Research and Public Health 18, no. 21: 11448. https://doi.org/10.3390/ijerph182111448