
A Systematic Review on Caries Status of Older Adults

 , , , , and
, , , , and 
Abstract
:1. Introduction
2. Materials and Methods
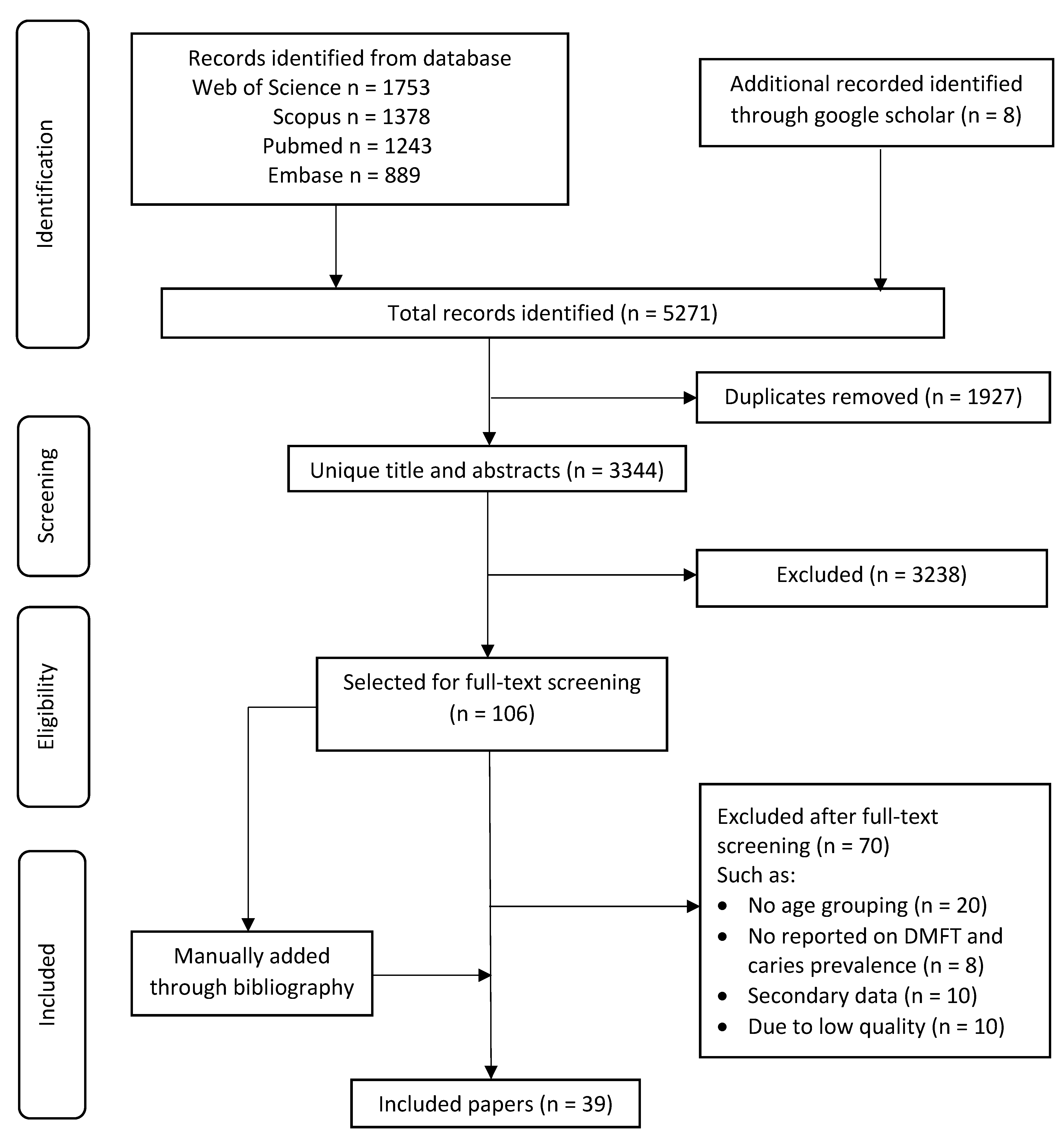
2.1. Search Strategy
2.2. Study Selection
2.3. Data Extraction and Quality Assessment
- Sample frame: Was the sample frame appropriate to address the target population?
- Sampling method: Were study participants sampled in an appropriate way?
- Sample size: Was the sample size adequate?
- Study setting: Were the study subjects and the setting described in detail?
- Sample coverage: Were the data analysed with sufficient coverage of the sample?
- Measure method: Were valid methods used for the identification of the condition?
- Outcome reliability: Were the measures for participants set out in a standard and reliable way?
- Statstical analysis: Was there appropriate statistical analysis?
- Response rate: Was the response rate adequate, and if not, was the low response rate managed appropriately?
3. Results
4. Discussion
4.1. Strengths and Limitations in This Study
4.2. Implications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Selwitz, R.H.; Ismail, A.I.; Pitts, N.B. Dental caries. Lancet 2007, 369, 51–59. [Google Scholar] [CrossRef]
- Petersen, P.E.; Bourgeois, D.; Ogawa, H.; Estupinan-Day, S.; Ndiaye, C. The global burden of oral diseases and risks to oral health. Bull. World Health Organ. 2005, 83, 661–669. [Google Scholar]
- Nordenram, G.; Davidson, T.; Gynther, G.; Helgesson, G.; Hultin, M.; Jemt, T.; Lekholm, U.; Nilner, K.; Norlund, A.; Rohlin, M.; et al. Qualitative studies of patients’ perceptions of loss of teeth, the edentulous state and prosthetic rehabilitation: A systematic review with meta-synthesis. Acta Odontol. Scand. 2012, 71, 937–951. [Google Scholar] [CrossRef]
- Kassebaum, N.J.; Bernabé, E.; Dahiya, M.; Bhandari, B.; Murray, C.J.; Marcenes, W. Global burden of untreated caries: A systematic review and metaregression. J. Dent. Res. 2015, 94, 650–658. [Google Scholar] [CrossRef]
- World Population Ageing 2019: 2019 Revision|Multimedia Library—United Nations Department of Economics and Social Affairs [Internet] Un.org. 2020. Available online: https://www.un.org/en/development/desa/population/publications/pdf/ageing/WorldPopulationAgeing2019-Highlights.pdf (accessed on 24 July 2020).
- Kassebaum, N.J.; Bernabé, E.; Dahiya, M.; Bhandari, B.; Murray, C.J.; Marcenes, W. Global Burden of Severe Tooth Loss: A Systematic Review and Meta-analysis. J. Dent. Res. 2014, 93, 20s–28s. [Google Scholar] [CrossRef] [Green Version]
- Chan, A.; Tamrakar, M.; Jiang, C.; Lo, E.; Leung, K.; Chu, C.-H. Common Medical and Dental Problems of Older Adults: A Narrative Review. Geriatrics 2021, 6, 76. [Google Scholar] [CrossRef]
- Twetman, S. Prevention of dental caries as a non-communicable disease. Eur. J. Oral Sci. 2018, 126, 19–25. [Google Scholar] [CrossRef] [Green Version]
- Petersen, P.E.; Baez, R.J.; World Health Organization. Oral Health Surveys: Basic Methods, 5th ed.; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- The Joanna Briggs Institute. Checklist for Prevalence Studies. Available online: https://jbi.global/sites/default/files/2019-05/JBI_Critical_Appraisal-Checklist_for_Prevalence_Studies2017_0.pdf (accessed on 16 August 2021).
- Gao, Y.B.; Hu, T.; Zhou, X.D.; Shao, R.; Cheng, R.; Wang, G.S.; Yang, Y.M.; Li, X.; Yuan, B.; Xu, T.; et al. Dental Caries in Chinese Elderly People: Findings from the 4th National Oral Health Survey. Chin. J. Dent. Res. 2018, 21, 213–220. [Google Scholar]
- Gao, Y.B.; Hu, T.; Zhou, X.D.; Shao, R.; Cheng, R.; Wang, G.S.; Yang, Y.M.; Li, X.; Yuan, B.; Xu, T.; et al. How Root Caries Differs between Middle-aged People and the Elderly: Findings from the 4th National Oral Health Survey of China. Chin. J. Dent. Res. 2018, 21, 221–229. [Google Scholar]
- Zhang, Q.; Jing, Q.; Gerritsen, A.E.; Witter, D.J.; Bronkhorst, E.M.; Creugers, N.H.J. Dental status of an institutionalized elderly population of 60 years and over in Qingdao, China. Clin. Oral Investig. 2015, 20, 1021–1028. [Google Scholar] [CrossRef] [Green Version]
- Gao, S.S.; Chen, K.J.; Duangthip, D.; Lo, E.C.M.; Chu, C.H. The Oral Health Status of Chinese Elderly People with and without Dementia: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2020, 17, 1913. [Google Scholar] [CrossRef] [Green Version]
- Wu, L.L.; Cheung, K.Y.; Lam, P.Y.P.; Gao, X. Oral health indicators for risk of malnutrition in elders. J. Nutr. Health Aging 2017, 22, 254–261. [Google Scholar] [CrossRef]
- Zhang, J.; Leung, K.C.M.; Chu, C.H.; Lo, E.C.M. Risk indicators for root caries in older adults using long-term social care facilities in Hong Kong. Community Dent. Oral Epidemiol. 2020, 48, 14–20. [Google Scholar] [CrossRef]
- Kumara-Raja, B.; Radha, G. Prevalence of root caries among elders living in residential homes of Bengaluru city, India. J. Clin. Exp. Dent. 2016, 8, e260–e267. [Google Scholar] [CrossRef]
- Singh, A.; Purohit, B.; Masih, N. Geriatric oral health predicaments in New Delhi, India. Geriatr. Gerontol. Int. 2015, 16, 37–45. [Google Scholar] [CrossRef]
- Ravi, P.; Rao, A.; Rajesh, G.; Shenoy, R.; Pai, M. Relationship between Geriatric Oral Health Assessment Index (GOHAI) and Oral Health Status of the Institutionalized Elderly in Mangalore, India. Indian J. Public Health Res. Dev. 2019, 10, 146. [Google Scholar] [CrossRef]
- Shivakumar, K.; Patil, S.; Kadashetti, V.; Raje, V. Oral health-related quality of life of institutionalized elderly in Satara District, India. J. Datta Meghe Inst. Med. Sci. Univ. 2018, 13, 183. [Google Scholar] [CrossRef]
- Valsan, I.; Joseph, J.; Janakiram, C.; Mohamed, S. Oral Health Status and Treatment Needs of Paniya Tribes in Kerala. J. Clin. Diagn. Res. 2016, 10, ZC12–ZC15. [Google Scholar] [CrossRef] [PubMed]
- Phalgune, D.; Salunke, S.; Shah, V.; Ostbye, T.; Gandhi, A.; Ogundare, M.O.; Sable, V. Prevalence of dental caries, oral health awareness and treatment-seeking behavior of elderly population in rural Maharashtra. Indian J. Dent. Res. 2019, 30, 332–336. [Google Scholar] [CrossRef]
- Athuluru, D.; Reddy, V.C.; Sudhir, K.; Kumar, R.S.K.; Gomasani, S.; Nagarakanti, S. An epidemiological data of oral health status and treatment needs of rural population of Nellore district, Andhra Pradesh, India. J. Indian Assoc. Public Health Dent. 2016, 14, 281. [Google Scholar] [CrossRef]
- Varghese, C.M.; Jesija, J.S.; Prasad, J.H.; Pricilla, R.A. Prevalence of oral diseases and risks to oral health in an urban community aged above 14 years. Indian J. Dent. Res. 2019, 30, 844–850. [Google Scholar] [CrossRef] [PubMed]
- Ngo, D.Y.J.; Thomson, W.M.; Subramaniam, M.; Abdin, E.; Ang, K.-Y. The oral health of long-term psychiatric inpatients in Singapore. Psychiatry Res. 2018, 266, 206–211. [Google Scholar] [CrossRef] [PubMed]
- Karaaslan, F.D.A.; Yiğit, U. Oral Health Status and Associated Factors in a Subpopulation of Turkish Patients. Cumhuriyet Dent. J. 2019, 22, 167–175. [Google Scholar] [CrossRef]
- Bozdemir, E.; Yilmaz, H.; Orhan, H. General health and oral health status in elderly dental patients in Isparta, Turkey. East. Mediterr. Health J. 2016, 22, 579–585. [Google Scholar] [CrossRef]
- Tanık, A. Evaluation of the relationship of CPITN and DMFT index of adult patients in Turkey with their demographic characteristics: An epidemiological study. Biotechnol. Biotechnol. Equip. 2019, 33, 1626–1634. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, M.S.; Jagomägi, T.; Voog-Oras, Ü.; Nguyen, T.; Saag, M. Oral Health Behaviour and Oral Health Status of Elderly Vietnamese. Oral Health Prev. Dent. 2018, 16, 153–161. [Google Scholar]
- Pham, T.A.V.; Nguyen, T.Q. Dental and periodontal problems of elderly people in Vietnamese nursing homes. Gerodontology 2018, 35, 192–199. [Google Scholar] [CrossRef]
- Tuuliainen, E.; Nen, K.A.-H.; Nihtilä, A.; Komulainen, K.; Nykänen, I.; Hartikainen, S.; Ahonen, R.; Tiihonen, M.; Suominen, A.-L. Oral Health and Hygiene and Association of Functional Ability: A Cross-Sectional Study Among Old Home Care Clients. Oral Health Prev. Dent. 2020, 18, 1–10. [Google Scholar]
- Sekundo, C.; Langowski, E.; Kilian, S.; Frese, C. Oral health and functional capacity of centenarians. Sci. Rep. 2020, 10, 1–10. [Google Scholar] [CrossRef]
- Aarabi, G.; Reissmann, D.R.; Seedorf, U.; Becher, H.; Heydecke, G.; Kofahl, C. Oral health and access to dental care—a comparison of elderly migrants and non-migrants in Germany. Ethn. Health 2017, 23, 703–717. [Google Scholar] [CrossRef] [PubMed]
- Hayes, M.; Da Mata, C.; Cole, M.; McKenna, G.; Burke, F.; Allen, P.F. Risk indicators associated with root caries in independently living older adults. J. Dent. 2016, 51, 8–14. [Google Scholar] [CrossRef] [Green Version]
- Kamberi, B.; Koçani, F.; Begzati, A.; Kelmendi, J.; Ilijazi, D.; Berisha, N.; Kqiku, L. Prevalence of Dental Caries in Kosovar Adult Population. Int. J. Dent. 2016, 2016, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oscarson, N.; Espelid, I.; Jönsson, B. Is caries equally distributed in adults? A population-based cross-sectional study in Norway—the TOHNN-study. Acta Odontol. Scand. 2017, 75, 557–563. [Google Scholar] [CrossRef] [Green Version]
- Głowacka, B.; Konopka, T. Needs for gerodontological treatment in the elderly living in Lower Silesia. Dent. Med. Probl. 2019, 56, 89–96. [Google Scholar] [CrossRef] [Green Version]
- Skośkiewicz-Malinowska, K.; Malicka, B.; Ziętek, M.; Kaczmarek, U. Oral health condition and occurrence of depression in the elderly. Medicine 2018, 97, e12490. [Google Scholar] [CrossRef] [PubMed]
- Gavinha, S.M.; Melo, P.R.; Costa, L.G.; Monteiro, P.M.; Manso, M.C. Dental tooth decay profile in an institutionalized elder population of Northern Portugal. Braz. Dent. Sci. 2020, 23, 11. [Google Scholar] [CrossRef] [Green Version]
- Carausu, E.M.; Dascalu, C.G.; Zegan, G.; Burlea, L.S.; Lupu, I.C.; Antohe, I. The general and oral health status in older adults from rural environment of Iasi County, Romania. Rev. Cercet. Interv. Soc. 2017, 59, 187–208. [Google Scholar]
- Islas-Granillo, H.; Borges-Yañez, S.A.; Navarrete-Hernández, J.D.J.; Veras-Hernández, M.A.; Casanova-Rosado, J.F.; Minaya-Sánchez, M.; Casanova-Rosado, A.J.; Fernández-Barrera, M.Á.; Medina-Solís, C.E. Indicators of oral health in older adults with and without the presence of multimorbidity: A cross-sectional study. Clin. Interv. Aging 2019, 14, 219–224. [Google Scholar] [CrossRef] [Green Version]
- Heredia-Ponce, E.; Irigoyen-Camacho, M.E.; Sánchez-García, S. Oral Health Status of Institutionalized Older Women from Different Socioeconomic Positions. J. Health Care Poor Underserved 2017, 28, 1462–1476. [Google Scholar] [CrossRef] [PubMed]
- Anderson, L.; Martin, N.R.; Kelly, S.M.; A Brown, H. Oral Health Status of Older Adults Attending Senior Centers and Congregate Meal Sites in New Hampshire. J. Dent. Hyg. JDH 2016, 90, 128–134. [Google Scholar]
- D’Avila, O.; Wendland, E.; Hilgert, J.; Padilha, D.M.P.; Hugo, F. Association between Root Caries and Depressive Symptoms among Elders in Carlos Barbosa, RS, Brazil. Braz. Dent. J. 2017, 28, 234–240. [Google Scholar] [CrossRef] [Green Version]
- Kapellas, K.; Roberts-Thomson, K.F. National Study of Adult Oral Health 2017–18: Root caries. Aust. Dent. J. 2020, 65, 40–46. [Google Scholar] [CrossRef] [PubMed]
- Peres, K.G.; Ha, D.H.; Christofis, S. Trend and distribution of coronal dental caries in Australians adults. Aust. Dent. J. 2020, 65, S32–S39. [Google Scholar] [CrossRef] [PubMed]
- Abbass, M.M.; Abubakr, N.; Radwan, I.A.; Rady, D.; El Moshy, S.; Ramadan, M.; Ahmed, A.; Al Jawaldeh, A. The potential impact of age, gender, body mass index, socioeconomic status and dietary habits on the prevalence of dental caries among Egyptian adults: A cross-sectional study. F1000Research 2019, 8, 243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Msyamboza, K.P.; Phale, E.; Namalika, J.M.; Mwase, Y.; Samonte, G.C.; Kajirime, D.; Sumani, S.; Chalila, P.D.; Potani, R.; Mwale, G.C.; et al. Magnitude of dental caries, missing and filled teeth in Malawi: National Oral Health Survey. BMC Oral Health 2016, 16, 29. [Google Scholar] [CrossRef] [Green Version]
- Chikte, U.; Pontes, C.C.; Karangwa, I.; Kimmie-Dhansay, F.; Erasmus, R.; Kengne, A.P.; Matsha, T.E. Dental caries in a South African adult population: Findings from the Cape Town Vascular and Metabolic Health Study. Int. Dent. J. 2020, 70, 176–182. [Google Scholar] [CrossRef]
- Petersen, P.E. World Health Organization global policy for improvement of oral health—World Health Assembly 2007. Int. Dent. J. 2008, 58, 115–121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, J.; Zhang, S.S.; Zheng, S.G.; Xu, T.; Si, Y. Oral Health Status and Oral Health Care Model in China. Chin. J. Dent. Res. 2016, 19, 207–215. [Google Scholar]
- Do, L.G.; Roberts-Thomson, K.F. Dental caries experience in the Australian adult population. Aust. Dent. J. 2007, 52, 249–251. [Google Scholar] [PubMed]
- Petersen, P.E. The World Oral Health Report 2003: Continuous improvement of oral health in the 21st century—the approach of the WHO Global Oral Health Programme. Community Dent. Oral Epidemiol. 2003, 31, 3–24. [Google Scholar] [CrossRef]
- Chen, K.J.; Gao, S.S.; Duangthip, D.; Lo, E.C.M.; Chu, C.H. Prevalence of early childhood caries among 5-year-old children: A systematic review. J. Investig. Clin. Dent. 2018, 10, e12376. [Google Scholar] [CrossRef] [Green Version]
- Carvalho, J.C.; Schiffner, U. Dental Caries in European Adults and Senior Citizens 1996–2016: ORCA Saturday Afternoon Symposium in Greifswald, Germany—Part II. Caries Res. 2019, 53, 242–252. [Google Scholar] [CrossRef]
- Khalifa, N.; Allen, P.F.; Abu-Bakr, N.H.; E Abdel-Rahman, M.; O Abdelghafar, K. A survey of oral health in a Sudanese population. BMC Oral Health 2012, 12, 5. [Google Scholar] [CrossRef] [Green Version]
- Frencken, J. Caries Epidemiology and Its Challenges. Monogr. Oral Sci. 2018, 27, 11–23. [Google Scholar] [CrossRef]
- Kumar, S.; Tadakamadla, J.; Johnson, N.W. Effect of Toothbrushing Frequency on Incidence and Increment of Dental Caries: A Systematic Review and Meta-Analysis. J. Dent. Res. 2016, 95, 1230–1236. [Google Scholar] [CrossRef] [PubMed]
- Ma, L.-L.; Wang, X.; Yang, Z.-H.; Huang, D.; Weng, H.; Zeng, X.-T. Methodological quality (risk of bias) assessment tools for primary and secondary medical studies: What are they and which is better? Mil. Med. Res. 2020, 7, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Griffin, S.; Regnier, E.; Griffin, P.; Huntley, V. Effectiveness of Fluoride in Preventing Caries in Adults. J. Dent. Res. 2007, 86, 410–415. [Google Scholar] [CrossRef] [PubMed]
- Duangthip, D.; Wong, M.; Chu, C.H.; Lo, E. Caries arrest by topical fluorides in preschool children: 30-month results. J. Dent. 2018, 70, 74–79. [Google Scholar] [CrossRef]
- Hendre, A.D.; Taylor, G.W.; Chávez, E.M.; Hyde, S. A systematic review of silver diamine fluoride: Effectiveness and application in older adults. Gerodontology 2017, 34, 411–419. [Google Scholar] [CrossRef] [PubMed]
- Ekstrand, K. High Fluoride Dentifrices for Elderly and Vulnerable Adults: Does It Work and if So, Then Why? Caries Res. 2016, 50, 15–21. [Google Scholar] [CrossRef] [Green Version]
- Ev, L.D.; Damé-Teixeira, N.; Do, T.; Maltz, M.; Parolo, C.C.F. The role of Candida albicans in root caries biofilms: An RNA-seq analysis. J. Appl. Oral Sci. 2020, 28, e20190578. [Google Scholar] [CrossRef] [PubMed]
- Chan, A.K.Y.; Tsang, Y.C.; Chu, C.H.; Tsang, C.S.P. Aspirin as an Antifungal-Lock Agent in Inhibition of Candidal Biofilm Formation in Surgical Catheters. Infect. Drug Resist. 2021, 14, 1427–1433. [Google Scholar] [CrossRef] [PubMed]
- Peres, M.A.; Macpherson, L.M.D.; Weyant, R.J.; Daly, B.; Venturelli, R.; Mathur, M.R.; Listl, S.; Celeste, R.K.; Guarnizo-Herreño, C.C.; Kearns, C.; et al. Oral diseases: A global public health challenge. Lancet 2019, 394, 249–260. [Google Scholar] [CrossRef]
- Watt, R.G.; Daly, B.; Allison, P.; Macpherson, L.M.D.; Venturelli, R.; Listl, S.; Weyant, R.; Mathur, M.; Guarnizo-Herreño, C.C.; Celeste, R.K.; et al. Ending the neglect of global oral health: Time for radical action. Lancet 2019, 394, 261–272. [Google Scholar] [CrossRef]


{kind=link}
| Location | Median of Untreated Caries Prevalence | Median of Root Caries Prevalence |
|---|---|---|
| Global (20 countries, 39 studies) | 49% | 46% |
| Asia (5 countries, 20 studies) | 66% | 46% |
| Europe (8 countries, 10 studies) | 46% | 35% |
| North America (2 countries, 3 studies) | 25% | 95.3% |
| South America (1 country, 1 study) | - | 74% |
| Oceania (1 country, 2 studies) | 25% | 18% |
| Africa (3 countries, 3 studies) | 49% | - |
| Country [Ref.] | Sampling Method | Setting | Participants | Location | Types of Caries |
|---|---|---|---|---|---|
| Asia | |||||
| China [11] | Multistage Cluster | Community | 65–74 yrs; Female: 65% | Urban: 51% | Coronal |
| China [12] | Multistage Cluster | Community | 65–74 yrs; Female: 65% | Urban: 51% | Root |
| China [13] | Purposive | Residential home | ≥60 yrs; Female: 66% | Coronal | |
| China [14] | Consecutive | Day care centre | ≥65 yrs; Female: 76%; Dementia: 54% | Coronal | |
| China [15] | - | Community | 65–94 yrs; Female: 68%; Systemic disease: 71% | Coronal | |
| China [16] | Purposive | Community | ≥60 yrs; Female: 81% | Root | |
| India [17] | Cluster | Residential home | ≥60 yrs; Female: 60% | Root | |
| India [18] | Convenience | Community | ≥60 yrs; Female: 30% | Coronal | |
| India [19] | Not reported | Residential home | 60–69 yrs; Female: 60% | Coronal and Root | |
| India [20] | Simple Random | Residential home | ≥65 yrs; Female: 55% | Coronal | |
| India [21] | Stratified cluster | Community | 65–74 yrs | Rural: 98% | Coronal |
| India [22] | Stratified sampling | Community | ≥60 yrs; Female: 51% | Rural: 100% | Coronal |
| India [23] | Multistage cluster | Community | 65–74 yrs; Female: 50% | Rural:100% | Coronal |
| India [24] | Systematic Random | Community | ≥65 yrs | Urban:100% | Coronal |
| Singapore [25] | Random | Hospital | 60–80 yrs; Female: 27%; Psychiatric: 100% | Coronal | |
| Turkey [26] | - | Community | ≥65 yrs | Coronal | |
| Turkey [27] | Random | Community | ≥60 yrs; Female: 47%; Systematic disease: 90% | Coronal | |
| Turkey [28] | Not Reported | Community | 70–80 yrs | Coronal | |
| Vietnam [29] | Multistage Stratified | Community | ≥65 yrs; Female: 50% | Rural: 47% | Coronal |
| Vietnam [30] | - | Residential home | ≥60 yrs; Female: 55%; Systematic disease: 51% | Coronal and Root | |
| Europe | |||||
| Finland [31] | Random | Community | Age: ≥75; Female: 74; Functional disability: 100% | Coronal and Root | |
| Germany [32] | Census | Community | 100 yrs; Female: 84% | Coronal and Root | |
| Germany [33] | Convenience | Community | ≥60 yrs; Female: 52% | Coronal | |
| Ireland [34] | Advertisement | Community | ≥65 yrs; Female: 56% | Coronal and Root | |
| Kosovo [35] | Not Reported | Community | ≥65 yrs | Coronal | |
| Norway [36] | Random | Community | 65–79 yrs | Coronal | |
| Poland [37] | Random | Community | 65–74 yrs; Female: 52% | Coronal | |
| Poland [38] | Volunteer | Community | ≥65 yrs; Female: 64%; Depression: 30% | Coronal | |
| Portugal [39] | Probabilistic | Residential home | ≥60 yrs; Female: 70% | Coronal and Root | |
| Romania [40] | Not Reported | Community | 65–74 yrs; Female: 55% | Rural: 100% | Coronal |
| North America | |||||
| Mexico [41] | Not Reported | Community | ≥60 yrs; Female: 70% | Root | |
| Mexico [42] | Not Reported | Residential home | ≥60 yrs; Female: 100%; Systematic disease: 67% | Rural: 42% | Coronal |
| USA [43] | Not Reported | Community | ≥60 yrs; Female: 71% | Coronal | |
| South America | |||||
| Brazil [44] | Simple Random | Community | ≥60 yrs; Female: 49%; Depression: 11% | Rural: 47% | Root |
| Oceania | |||||
| Australia [45] | Not reported | Community | ≥75 yrs | Root | |
| Australia [46] | Not reported | Community | ≥75 yrs | Coronal | |
| Africa | |||||
| Egypt [47] | Convenience | Community | ≥65 yrs | Coronal | |
| Malawi [48] | Multistage | Community | 65–74 yrs | Coronal | |
| South Africa [49] | Consecutive | Community | ≥65 yrs | Coronal |
| Caries Prevalence | Sample Size | DMFT ± SD | DT ± SD | Diagnostic Criteria | Country (Ref.) |
|---|---|---|---|---|---|
| 43–99% | 21–4331 | 9.2–26.7 | 1–6.4 | Asia | |
| 99% * | 791 | - | 5.8 ± 4 | WHO | Vietnam [30] |
| 98% | 4431 | 13.3 ± 9.3 | 3.3 ± 4.2 | WHO | China [11] |
| 89% | 258 | 14.3 ± 8.7 | 6.4 ± 5.5 | WHO | Vietnam [29] |
| 77% | 248 | 16.4 ± 9 | - | WHO | India [18] |
| 76% | 352 | - | - | WHO | India [22] |
| 56% | 165 | 18.5 ± 13.1 | - | WHO | India [21] |
| 49% | 192 | 12 ± 9.7 | 1.6 ±2.2 | WHO | India [23] |
| 47% | 195 | - | 1 ± 1.5 | WHO | China [15] |
| 47% * | 175 | 20.3 ± 10.2 | 2.2 ± 3.6 | WHO | India [19] |
| 43% | 23 | - | - | WHO | India [24] |
| - | 709 | 19.1 ± 7.3 | - | WHO | Turkey [27] |
| - * | 512 | 15.1 ± 8.2 | - | WHO | China [13] |
| - | 392 (65–74) | 21.9 ± 5.2 | - | WHO | Turkey [26] |
| - | 429 (75+) | 23.6 ± 4.7 | - | ||
| - * | 150 | 23.9 | - | WHO | India [20] |
| - * | 129 | 22.5 ± 7.9 | 2.1 ± 3.1 | WHO | China [14] |
| - | 99 | 19.2 ± 9.3 | 2.3 ± 2.6 | ||
| - * | 64 | 26.7 ± 6.4 | 3.5 ±5.1 | WHO | Singapore [25] |
| - | 21 | 9.2 ± 4.8 | 1 ± 0.7 | WHO | Turkey [28] |
| 21–59% | 55–1626 | 17.8–27.5 | 0.5–5.3 | Europe | |
| 59% | 196 | - | - | - | Romania [40] |
| 50% * | 372 | 25.6 ± 7.3 | 1.7 ± 2.3 | WHO | Portugal [39] |
| 49% | 387 | 17.8 | 1.1 | WHO | Poland [37] |
| 42% | 1626 (65–74) | 18 ± 9.9 | 1.1 ± 2 | WHO | Kosovo [35] |
| - | 273 (75+) | 23.2 ± 9.4 | 0.5 ± 1.5 | ||
| 30% | 269 | - | 0.8 ± 1.8 | WHO | Finland [31] |
| - | 500 | 27.5 ± 5 | 1.5 ± 2.7 | WHO | Poland [38] |
| - | 334 | 23.5 ± 5 | - | WHO | Ireland [34] |
| - | 308 | 22.5 | 0.8 | 5-grade scale | Norway [36] |
| - | 61 (migrant) | 24.8 ± 3.9 | 5.3 ± 4.6 | Barmes | Germany [33] |
| - | 51(non-migrant) | 23.4 ± 4.6 | 2.1 ± 2.8 | ||
| - | 55 | 25.2 ± 3.9 | 1.2 | WHO | Germany [32] |
| 25% | 170–512 | - | 1.9 | North America | |
| 25% | 512 | - | - | - | USA [43] |
| - * | 170 | - | 1.9 ± 3.5 | WHO | Mexico [42] |
| 25% | 433 | - | - | Oceania | |
| 25% | 433 | - | - | WHO | Australia [46] |
| 42–99% | 12–683 | 6.9–30.1 | 0.2–3.4 | Africa | |
| - | 243 (65–74) | 29.7 ± 5.9 | 0.3 ± 1.3 | WHO | South Africa [49] |
| 99% | 74 (75+) | 30.1 ± 6.1 | 0.2 ± 1.6 | ||
| 49% | 683 | 6.9 | 1.41 | WHO | Malawi [48] |
| 42% | 12 | 11.4 ± 7.6 | 3.4 ± 7.4 | WHO | Egypt [47] |
| Root Caries Prevalence | Sample Size | DT ± SD | Diagnostic Criteria | Countries (Ref.) |
|---|---|---|---|---|
| 30–96% | 175–4431 | 0.7–6 | Asia | |
| 96% * | 791 | 6 ± 4.2 | WHO | Vietnam [30] |
| 62% | 4431 | 2.6 ± 3.7 | WHO | China [12] |
| 46% * | 312 | - | Banting | India [17] |
| 40% * | 175 | - | WHO | India [19] |
| 30% * | 353 | 0.7 ± 1.7 | ICDAS | China [16] |
| 8–54% | 55–372 | 0.1–3.4 | Europe | |
| 54% * | 372 | 3.4 ± 3.6 | WHO | Portugal [39] |
| 35% | 55 | 1.1 ± 1.5 | WHO | Germany [32] |
| 8% | 269 | 0.1 ± 0.6 | WHO | Finland [31] |
| 95% | 139 | North America | ||
| 95% * | 139 | - | WHO | Mexico [41] |
| 74% | 390 | South America | ||
| 74% | 390 | - | WHO | Brazil [44] |
| 18% | 433 | Oceania | ||
| 18% | 433 | - | WHO | Australia [45] |
| Country of Study [Ref.] | Household Income | Education Level | Living Region | Dietary Habit | Brushing Habit | Dental Visit |
|---|---|---|---|---|---|---|
| Egypt [47] | Y | Y | - | Y | Y | - |
| Australia [46] | Y | - | Y | - | - | Y |
| China [12] | - | Y | - | Y | - | Y |
| Norway [36] | - | - | - | Y | Y | Y |
| India [17] | Y | - | - | Y | Y | - |
| Australia [45] | Y | - | Y | - | - | |
| China [11] | Y | - | - | Y | - | |
| Brazil [44] | - | - | Y | - | Y | - |
| Portugal [39] | - | - | - | - | Y | - |
| Turkey [28] | - | Y | - | - | - | - |
| USA [43] | Y | - | - | - | - | |
| India [18] | - | Y | - | - | - | - |
| Quality (Score) | Sample Frame | Sampling Method | Sample Size | Study Setting | Sample Coverage | Measure Method | Outcome Reliability | Statistical Analysis | Response Rate | Country [Ref.] |
|---|---|---|---|---|---|---|---|---|---|---|
| Asia | ||||||||||
| Good (8) | Y | Y | Y | Y | - | Y | Y | Y | Y | China [14] |
| Good (8) | Y | Y | Y | Y | - | Y | Y | Y | Y | China [11] |
| Good (8) | Y | Y | Y | Y | - | Y | Y | Y | Y | China [12] |
| Good (8) | Y | Y | Y | Y | - | Y | Y | Y | Y | India [17] |
| Good (8) | Y | Y | Y | Y | - | Y | Y | Y | Y | Turkey [28] |
| Good (8) | Y | Y | Y | Y | - | Y | Y | Y | Y | Vietnam [29] |
| Good (7) | Y | Y | Y | Y | - | Y | - | Y | Y | India [23] |
| Good (7) | - | Y | Y | Y | - | Y | Y | Y | Y | India [21] |
| Moderate (6) | - | - | Y | Y | - | Y | Y | Y | Y | China [15] |
| Moderate (6) | - | Y | Y | Y | - | Y | Y | Y | - | India [19] |
| Moderate (6) | - | - | Y | Y | - | Y | Y | Y | Y | India [20] |
| Moderate (6) | Y | Y | Y | Y | - | - | - | Y | Y | India [24] |
| Moderate (6) | - | - | Y | Y | - | Y | Y | Y | Y | Turkey [26] |
| Moderate (6) | Y | Y | Y | - | - | Y | - | Y | Y | Vietnam [30] |
| Moderate (5) | - | - | Y | - | - | Y | Y | Y | Y | China [16] |
| Moderate (5) | - | - | - | Y | - | Y | Y | Y | Y | China [13] |
| Moderate (5) | - | - | Y | Y | - | Y | - | Y | Y | India [22] |
| Moderate (5) | - | Y | - | Y | - | - | Y | Y | Y | Singapore [25] |
| Moderate (4) | - | - | - | Y | - | Y | Y | Y | - | India [18] |
| Moderate (4) | - | Y | - | - | - | Y | - | Y | Y | Turkey [27] |
| Europe | ||||||||||
| Good (8) | Y | Y | Y | Y | Y | Y | - | Y | Y | Germany [32] |
| Good (8) | Y | Y | Y | Y | - | Y | Y | Y | Y | Kosovo [35] |
| Good (8) | Y | Y | Y | Y | - | Y | Y | Y | Y | Norway [36] |
| Good (7) | - | Y | Y | Y | - | Y | Y | Y | Y | Finland [31] |
| Good (7) | - | Y | Y | Y | Y | - | Y | Y | Y | Romania [40] |
| Moderate (6) | - | - | Y | Y | - | Y | Y | Y | Y | Poland [38] |
| Moderate (6) | - | - | Y | Y | - | Y | Y | Y | Y | Portugal [39] |
| Moderate (5) | - | - | - | Y | Y | Y | - | Y | Y | Germany [33] |
| Moderate (5) | Y | - | - | Y | Y | Y | - | Y | - | Poland [37] |
| Moderate (4) | - | - | - | Y | - | Y | Y | Y | - | Ireland [34] |
| North America | ||||||||||
| Moderate (6) | Y | Y | Y | - | Y | - | - | Y | Y | USA [43] |
| Moderate (5) | - | - | - | - | Y | Y | Y | Y | Y | Mexico [41] |
| Moderate (4) | - | - | - | Y | - | Y | Y | Y | - | Mexico [42] |
| South America | ||||||||||
| Good (8) | Y | Y | Y | Y | - | Y | Y | Y | Y | Brazil [44] |
| Oceania | ||||||||||
| Good (7) | Y | Y | Y | Y | - | Y | Y | - | Y | Australia [45] |
| Good (7) | Y | Y | Y | Y | - | Y | Y | - | Y | Australia [46] |
| Africa | ||||||||||
| Good (8) | Y | Y | Y | Y | - | Y | Y | Y | Y | Malawi [48] |
| Moderate (6) | - | Y | Y | Y | - | Y | Y | - | Y | Egypt [47] |
| Moderate (6) | Y | Y | - | Y | - | Y | Y | Y | - | South Africa [49] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chan, A.K.Y.; Tamrakar, M.; Jiang, C.M.; Lo, E.C.M.; Leung, K.C.M.; Chu, C.H. A Systematic Review on Caries Status of Older Adults. Int. J. Environ. Res. Public Health 2021, 18, 10662. https://doi.org/10.3390/ijerph182010662
Chan AKY, Tamrakar M, Jiang CM, Lo ECM, Leung KCM, Chu CH. A Systematic Review on Caries Status of Older Adults. International Journal of Environmental Research and Public Health. 2021; 18(20):10662. https://doi.org/10.3390/ijerph182010662
Chicago/Turabian StyleChan, Alice Kit Ying, Manisha Tamrakar, Chloe Meng Jiang, Edward Chin Man Lo, Katherine Chiu Man Leung, and Chun Hung Chu. 2021. "A Systematic Review on Caries Status of Older Adults" International Journal of Environmental Research and Public Health 18, no. 20: 10662. https://doi.org/10.3390/ijerph182010662