
Mental Health during the COVID-19 Crisis in Africa: A Systematic Review and Meta-Analysis

 , , ,
, , ,
Abstract
:1. Introduction
2. Methodology and Materials
2.1. Protocol Registration
2.2. Data Sources and Search Strategy
2.3. Eligibility Criteria
- Outcomes: reported the prevalence of depression, anxiety, or insomnia during COVID-19 pandemic.
- Measurements/Instruments: using any validated measurement tools or scales.
- Population: included adult participants including frontline HCWs, general HCWs, general adult population, or adult medical students from any African countries.
- Methodological design: cross-sectional or cohort.
- Language: published in English.
- Population: children, adolescents, or specific niche adult populations, such as patients, adults under quarantine, pregnant/postpartum women.
- Methodological design: non-primary studies, such as reviews or meta-analyses, qualitative or case studies without a validated instrument, interventional studies, interviews, or news reports.
- Measurements/Instruments: non-validated instruments measuring mental health outcomes (i.e., self-made questionnaire) or instruments missing a validated cutoff score to calculate the prevalence rate.
2.4. Screening and Data Extraction
2.5. Assessment of Bias Risk
2.6. Statistical Analysis
3. Results
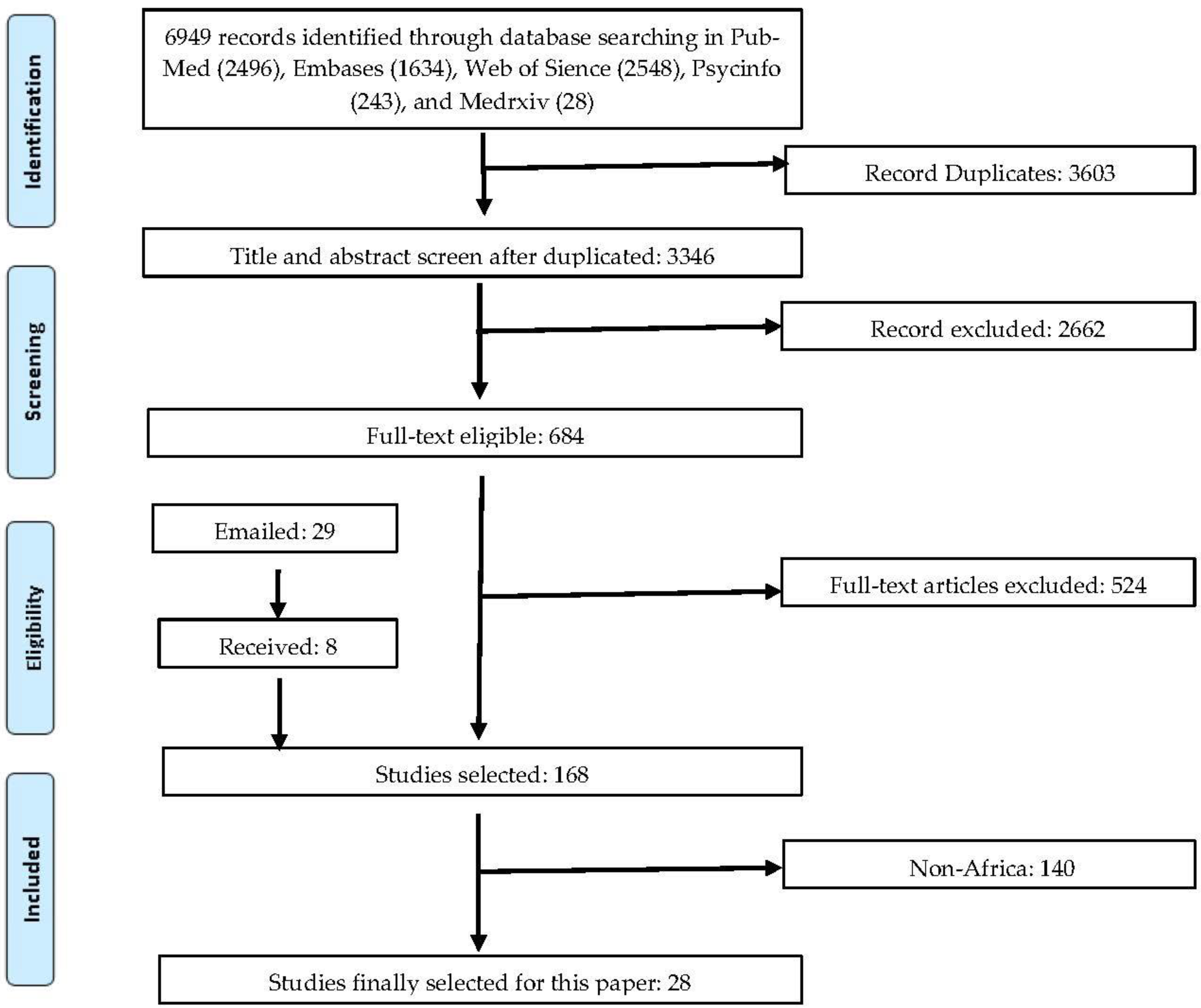
3.1. Study Screening
3.2. Study Characteristics
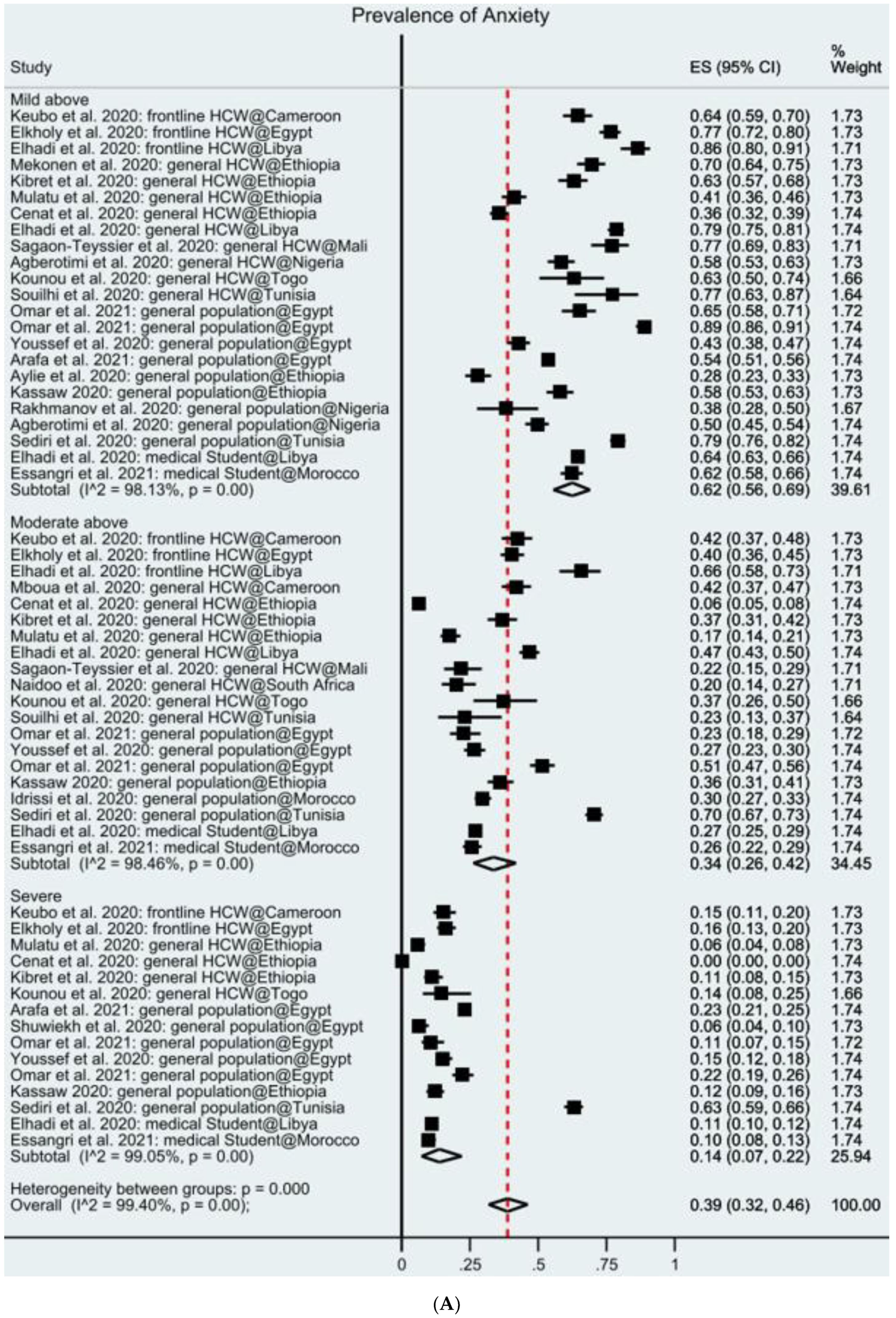
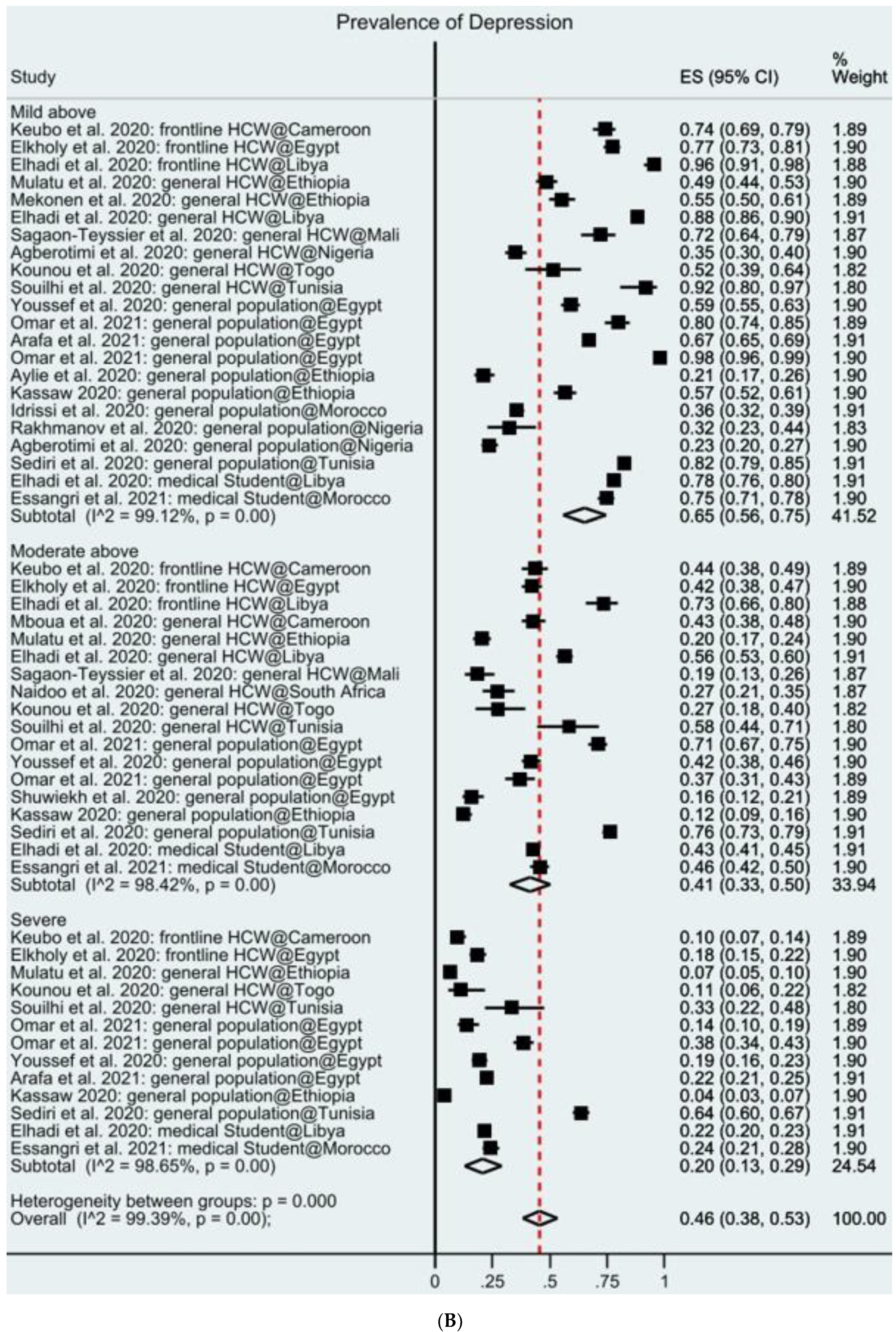
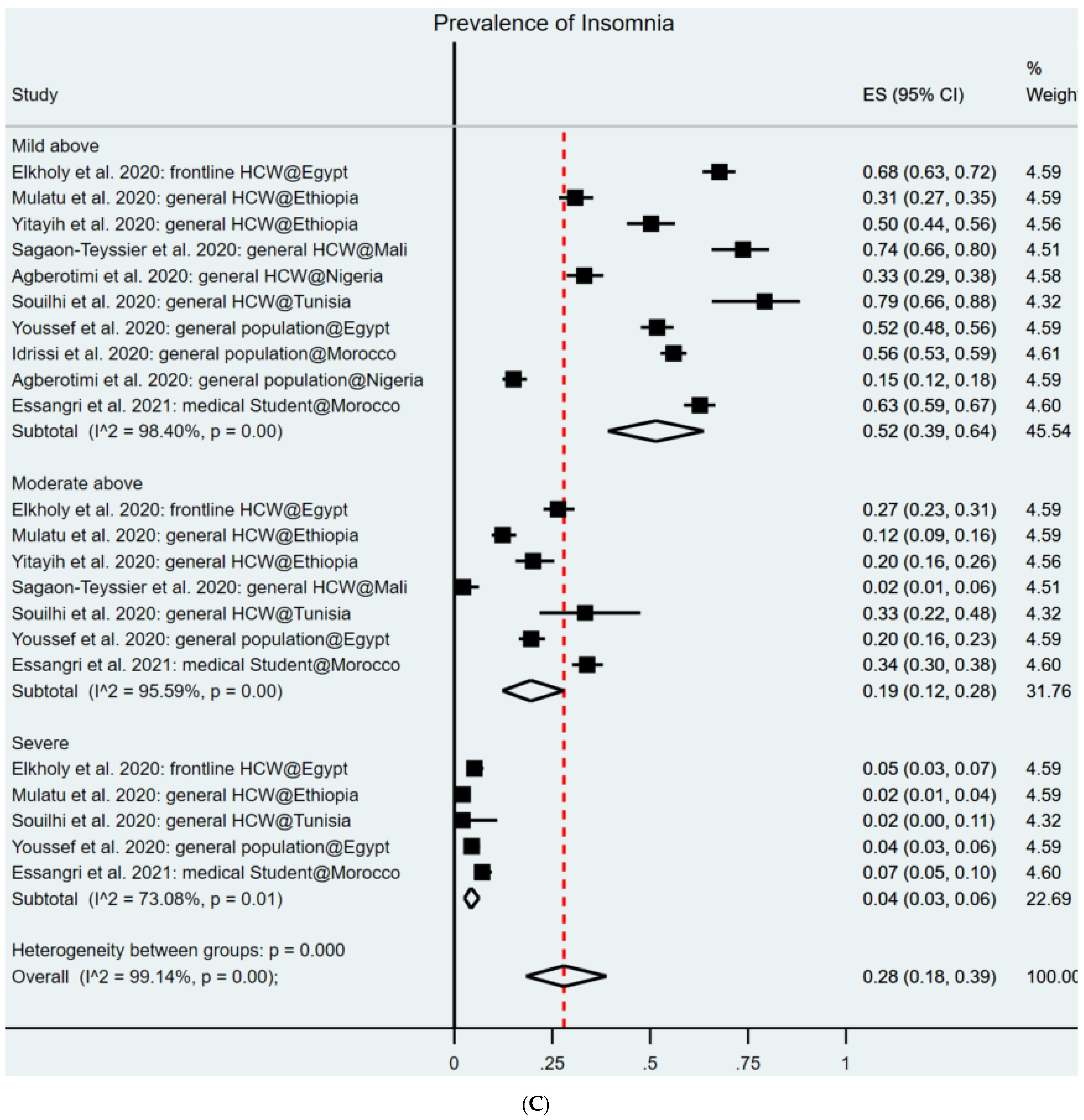
3.3. Pooled Prevalence Rates of Mental Health Symptoms
3.4. Study Quality
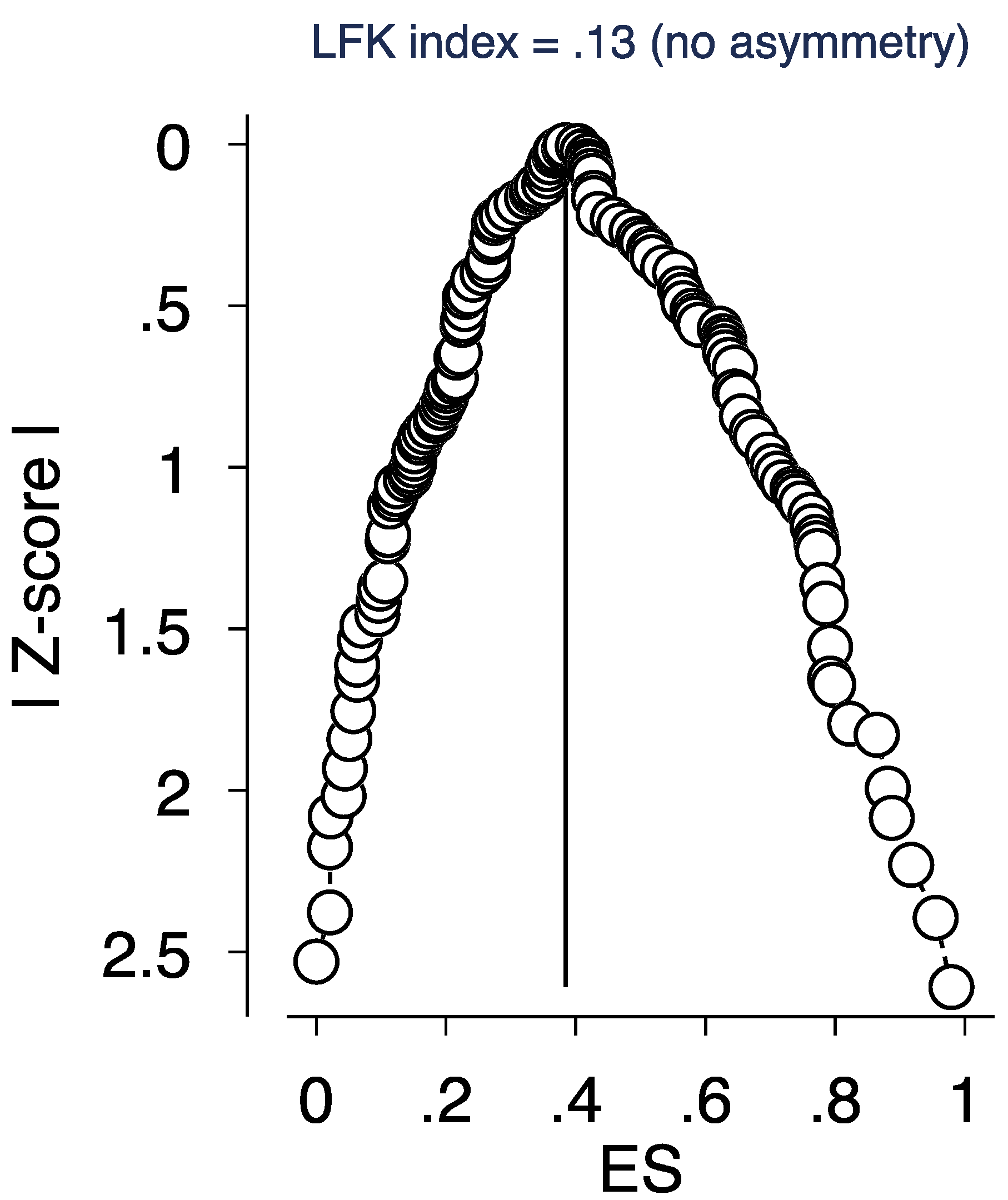
3.5. Sensitivity Analysis
4. Discussion
4.1. Comparisons of Results with Prior Meta-Analyses
4.2. Comparisons of COVID vs. Pre-COVID Findings in Africa
4.3. Practical Implications of Our Findings for Psychiatrists/Healthcare Organizations
4.4. Limitations and Future Work
5. Conclusions
Disclosure Statement
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. PRISMA Checklist

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Search Query | Search Topic | Search Keywords (Titles, Abstracts, and Subject Headings) with Boolean Operators |
|---|---|---|
| 1 | Exposure/Context | “Coronavirus” OR “COVID-19” OR “SARS-CoV-2” OR “2019-nCoV” |
| 2 | Outcome of interest | “Depression” OR “Depressive symptoms” OR “Depressive disorder*” OR “Anxiety” OR “Social Anxiety” or “Social Phobia” OR “Anxiety disorder*” OR “Insomnia” OR “Sleep disorder” OR “Depressive disorder*” |
| 3 | Epidemiological phenomenon | “Prevalence” OR “Incidence” OR “rate*” OR “ratio*” OR “Epidemiology*” OR “risk factor*” OR “relative risk” OR “disease burden” |
| 4 | Language | English |
| 5 | Time | February 2020–6 February 2021 |
| Intersection of four topics | 1 AND 2 AND 3 AND 4 AND 5 |
| Groups | Subgroups | Anxiety | Depression | Insomnia |
|---|---|---|---|---|
| Number of studies | 27 | 24 | 9 | |
| Number of samples | 31 | 26 | 10 | |
| Number of prevalence | 62 | 54 | 21 | |
| Number of participants | 14,847 | 12,688 | 4144 | |
| Aggregated | 37%, 95% CI: 31–44% | 45%, 95% CI: 38–53% | 28%, 95% CI: 18–40% | |
| Population | Frontline HCWs | 51%, 95% CI: 31–70% | 55%, 95% CI: 32–76% | 30%, 95% CI: 2–71% |
| General HCWs | 35%, 95% CI: 23–48% | 43%, 95% CI: 39–58% | 28%, 95% CI: 13–45% | |
| General population | 37%, 95% CI: 28–46% | 42%, 95% CI: 31–55% | 27%, 95% CI: 9–50% | |
| Medical student | 31%, 95% CI: 13–54% | 48%, 95% CI: 27–69% | 32%, 95% CI: 39–64% | |
| Severity | Above mild | 62%, 95% CI: 56–69% | 65%, 95% CI: 56–75% | 52%, 95% CI: 39–64% |
| Above moderate | 33%, 95% CI: 26–41% | 41%, 95% CI: 33–50% | 19%, 95% CI: 11–29% | |
| Severe | 14%, 95% CI: 07–31% | 20%, 95% CI: 13–29% | 4%, 95% CI: 3–6% | |
| Overall | 18%, 95% CI: 07–31% | 14%, 95% CI: 10–20% | NA | |
| Region | Sub-Sahara | 31%, 95% CI: 23–40% | 30%, 95% CI:22–40% | 24%, 95% CI:11–40% |
| North Africa | 44%, 95% CI: 34–53% | 55%, 95% CI: 46–65% | 31%, 95% CI: 18–47% | |
| Instruments | GAD-7/PHQ-9 | 34%, 95% CI: 25–43% | 43%, 95% CI: 33–54% | NA |
| DASS-22 | 44%, 95% CI: 31–57% | 43%, 95% CI: 29–59% | ||
| Authors & Year | Data Collection Time | Country | Population | Sample Size | Outcome | Instrument |
|---|---|---|---|---|---|---|
| Agberotimi et al., 2020 | 20 March–19 April | Nigeria | GHCW, GP | 382, 502 | ANX, DEP, INS | GAD7, PHQ9, ISI |
| Arafa et al., 2021 | 16 April–30 April | Egypt | GP | 1629 | ANX, DEP | DASS21 |
| Aylie et al., 2020 | 15 May–15 June | Ethiopia | GP | 322 | ANX, DEP | DASS21 |
| Cenat et al., 2020 | 15 March–15 May | Togo, RDC, Rwanda | GP | 242, 626, 174 | ANX | HSCL |
| Elhadi et al., 2020 a | 20 April–1 May | Libya | Student | 2430 | ANX, DEP | GAD7, PHQ9 |
| Elhadi et al., 2020 b | 18 April–28 April | Libya | FHCW | 154 | ANX, DEP | HADS |
| Elhadi et al., 2020 c | 18 April–28 April | Libya | GHCW | 745 | ANX, DEP | HADS |
| Elkholy et al., 2020 | April–May | Egypt | FHCW | 457 | ANX, DEP, INS | GAD7, PHQ9, ISI |
| Essangri et al., 2021 | 8 April–18 April | Morocco | Student | 549 | ANX, DEP, INS | GAD7, PHQ9, ISI |
| Idrissi et al., 2020 | 1 April–1 May | Morocco | GP | 846 | ANX, DEP, INS | HARS, BDI, AIS |
| Kassaw 2020 | 10 March–30 March | Ethiopia | GP | 382 | ANX, DEP | DASS21 |
| Keubo et al., 2020 | 5 April–19 April | Cameroon | FHCW | 292 | ANX, DEP | HAD |
| Kibret et al., 2020 | 15 May–15 June | Ethiopia | GHCW | 305 | ANX | GAD7 |
| Kim et al., 2020 | 26 March–7 May | South Africa | GP | 211 | DEP | CESD10 |
| Kounou et al., 2020 | 18 May | Togo | GHCW | 62 | ANX, DEP | GAD7, PHQ9 |
| Mboua et al., 2020 | 5 April–19 April | Cameroon | GHCW | 332 | ANX, DEP | HADS |
| Mekonen et al., 2020 | 25 Sepetember–20 October | Ethiopia | GHCW | 302 | ANX, DEP | DASS21 |
| Mulatu et al., 2020 | 1 August–30 August | Ethiopia | GHCW | 420 | ANX, DEP, INS | GAD7, PHQ9, ISI |
| Naidoo et al., 2020 | 6 March * | South Africa | GHCW | 150 | ANX, DEP | GAD7, PHQ9 |
| Omar et al., 2021 | 30 March–30 June | Egypt | GP (M, F) | 217, 479 | ANX, DEP | GAD7, PHQ9 |
| Rakhmanov et al., 2020 | 21 April * | Nigeria | GP | 69 | ANX | SRQ21 |
| Sagaon-Teyssier et al., 2020 | 6 April–6 May | Mali | GHCW | 135 | ANX, DEP, INS | GAD7, PHQ9, ISI |
| Sediri et al., 2020 | 25 April–6 May | Tunisia | GP | 751 | ANX, DEP | DASS21 |
| Shuwiekh et al., 2020 | 28 April–25 May | Egypt | GP | 255 | ANX, DEP | GAD7, PHQ9 |
| Souilhi et al., 2020 | 22 September ** | Tunisia | GHCW | 48 | ANX, DEP, INS | GAD7, PHQ9, ISI |
| Teshome et al., 2020 | 20 May–20 June | Ethiopia | GHCW | 798 | ANX | GAD7 |
| Yitayih et al., 2020 | 22 March–28 March | Ethiopia | GHCW | 249 | INS | ISI |
| Youssef et al., 2020 | 1 April–30 April | Egypt | GP | 540 | ANX, DEP, INS | DASS21, ISI |
References
- Lone, S.A.; Ahmad, A. COVID-19 pandemic—An African perspective. Emerg. Microbes Infect. 2020, 9, 1300–1308. [Google Scholar] [CrossRef]
- Moore, M.; Gelfeld, B.; Adeyemi Okunogbe, C.P. Identifying future disease hot spots: Infectious disease vulnerability index. Rand Health Q. 2017, 6, 5. [Google Scholar]
- El-Sadr, W.M.; Justman, J. Africa in the Path of Covid-19. N. Engl. J. Med. 2020, 383, e11. [Google Scholar] [CrossRef]
- Dare, L.; Buch, E. The future of health care in Africa. BMJ 2005, 331, 1–2. [Google Scholar] [CrossRef] [Green Version]
- WHO. World Report on Ageing and Health; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Moosa, S.; Peersman, W.; Derese, A.; Kidd, M.; Pettigrew, L.M.; Howe, A.; Martinez-Bianchi, V.; De Maeseneer, J. Emerging role of family medicine in South Africa. BMJ Glob. Health 2018, 3, e000736. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moïsi, J.; Madhi, S.A.; Rees, H. Vaccinology in sub-Saharan Africa. BMJ Glob. Health 2019, 4, e001363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kassaw, C.; Pandey, D. COVID-19 Pandemic Related to Anxiety Disorder Among Communities Using Public Transport at Addis Ababa, Ethiopia, March 2020: Cross-sectional Study Design. Hum. Arenas 2021, 1–10. [Google Scholar] [CrossRef]
- Elhadi, M.; Msherghi, A.; Alkeelani, M.; Zorgani, A.; Zaid, A.; Alsuyihili, A.; Buzreg, A.; Ahmed, H.; Elhadi, A.; Khaled, A.; et al. Assessment of Healthcare Workers’ Levels of Preparedness and Awareness Regarding COVID-19 Infection in Low-Resource Settings. Am. J. Trop. Med. Hyg. 2020, 103, 828–833. [Google Scholar] [CrossRef]
- Agberotimi, S.F.; Akinsola, O.S.; Oguntayo, R.; Olaseni, A.O. Interactions between socioeconomic status and mental health out-comes in the nigerian context amid covid-19 pandemic: A comparative study. Front. Psychol. 2020, 11, 2655. [Google Scholar] [CrossRef]
- Elhadi, M.; Msherghi, A.; Elgzairi, M.; Alhashimi, A.; Bouhuwaish, A.; Biala, M.; Abuelmeda, S.; Khel, S.; Khaled, A.; Alsoufi, A.; et al. Psychological status of healthcare workers during the civil war and COVID-19 pandemic: A cross-sectional study. J. Psychosom. Res. 2020, 137, 110221. [Google Scholar] [CrossRef]
- Aylie, N.S.; Mekonen, M.A.; Mekuria, R.M. The Psychological Impacts of COVID-19 Pandemic Among University Students in Bench-Sheko Zone, South-west Ethiopia: A Community-based Cross-sectional Study. Psychol. Res. Behav. Manag. 2020, 13, 813–821. [Google Scholar] [CrossRef]
- Bareeqa, S.B.; Ahmed, S.I.; Samar, S.S.; Yasin, W.; Zehra, S.; Monese, G.M.; Gouthro, R.V. Prevalence of depression, anxiety and stress in china during COVID-19 pandemic: A systematic review with meta-analysis. Int. J. Psychiatry Med. 2021, 56, 210–227. [Google Scholar] [CrossRef]
- Pappa, S.; Ntella, V.; Giannakas, T.; Giannakoulis, V.G.; Papoutsi, E.; Katsaounou, P. Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic: A systematic review and meta-analysis. Brain. Behav. Immun. 2020, 88, 901–907. [Google Scholar] [CrossRef]
- Ren, X.; Huang, W.; Pan, H.; Huang, T.; Wang, X.; Ma, Y. Mental Health During the Covid-19 Outbreak in China: A Meta-Analysis. Psychiatr. Q. 2020, 91, 1033–1045. [Google Scholar] [CrossRef] [PubMed]
- Krishnamoorthy, Y.; Nagarajan, R.; Saya, G.K.; Menon, V. Prevalence of psychological morbidities among general population, healthcare workers and COVID-19 patients amidst the COVID-19 pandemic: A systematic review and meta-analysis. Psychiatry Res. 2020, 293, 113382. [Google Scholar] [CrossRef] [PubMed]
- Salari, N.; Khazaie, H.; Hosseinian-Far, A.; Ghasemi, H.; Mohammadi, M.; Shohaimi, S.; Daneshkhah, A.; Khaledi-Paveh, B.; Hosseinian-Far, M. The prevalence of sleep disturb-ances among physicians and nurses facing the COVID-19 patients: A systematic review and meta-analysis. Glob. Health 2020, 16, 92. [Google Scholar] [CrossRef]
- Kisely, S.; Warren, N.; McMahon, L.; Dalais, C.; Henry, I.; Siskind, D. Occurrence, prevention, and management of the psychological effects of emerging virus outbreaks on healthcare workers: Rapid review and meta-analysis. BMJ 2020, 369, m1642. [Google Scholar] [CrossRef] [PubMed]
- Salari, N.; Hosseinian-Far, A.; Jalali, R.; Vaisi-Raygani, A.; Rasoulpoor, S.; Mohammadi, M.; Khaledi-Paveh, B. Prevalence of stress, anxiety, depression among the general population during the COVID-19 pandemic: A systematic review and meta-analysis. Glob. Health 2020, 16, 57. [Google Scholar] [CrossRef]
- Chen, X.; Chen, J.; Zhang, M.; Chen, R.Z.; Dong, R.K.; Dong, Z.; Ye, Y.; Tong, L.; Chen, B.; Zhao, R.; et al. One Year of Evidence on Mental Health in the COVID-19 Cri-sis-A Systematic Review and Meta-Analysis. medRxiv 2021. [Google Scholar]
- de Pablo, G.S.; Vaquerizo-Serrano, J.; Catalan, A.; Arango, C.; Moreno, C.; Ferre, F.; Shin, J.I.; Sullivan, S.; Brondino, N.; Solmi, M.; et al. Impact of coronavirus syndromes on physical and mental health of health care workers: Systematic review and meta-analysis. J. Affect. Disord. 2020, 275, 48–57. [Google Scholar] [CrossRef]
- Usher, K.; Jackson, D.; Durkin, J.; Gyamfi, N.; Bhullar, N. Pandemic-related behaviours and psychological outcomes; A rapid literature review to explain COVID-19 behaviours. Int. J. Ment. Health Nurs. 2020, 29, 1018–1034. [Google Scholar] [CrossRef]
- Hong, Q.N.; Fàbregues, S.; Bartlett, G.; Boardman, F.; Cargo, M.; Dagenais, P.; Gagnon, M.-P.; Griffiths, F.; Nicolau, B.; O’Cathain, A.; et al. The Mixed Methods Appraisal Tool (MMAT) version 2018 for information professionals and researchers. Educ. Inf. 2018, 34, 285–291. [Google Scholar] [CrossRef] [Green Version]
- Hong, Q.N.; Gonzalez-Reyes, A.; Pluye, P. Improving the usefulness of a tool for appraising the quality of qualitative, quantitative and mixed methods studies, the Mixed Methods Appraisal Tool (MMAT). J. Eval. Clin. Pr. 2018, 24, 459–467. [Google Scholar] [CrossRef] [Green Version]
- Boderie, N.W.; Mölenberg, F.J.; Sheikh, A.; Bramer, W.M.; Burdorf, A.; van Lenthe, F.J.; Been, J.V. Assessing public support for extending smoke-free policies beyond enclosed public places and workplaces: Protocol for a systematic review and meta-analysis. BMJ Open 2021, 11, e040167. [Google Scholar] [CrossRef] [PubMed]
- Mekonnen, A.B.; Redley, B.; de Courten, B.; Manias, E. Potentially inappropriate prescribing and its associations with health-related and system-related outcomes in hospitalised older adults: A systematic review and meta-analysis. Br. J. Clin. Pharmacol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Behghadami, M.A.; Janati, A.; Sadeghibazargani, H.; Gholizadeh, M.; Rahmani, F.; Arab-Zozani, M.; Behghadam, M.A. Assessing Preparedness of Non-Hospital Health Centers to Provide Primary Emergency Care; A Systematic Review. Bull. Emerg. Trauma 2019, 7, 201–211. [Google Scholar] [CrossRef] [PubMed]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Cheung, M.W.-L.; Ho, R.C.M.; Lim, Y.; Mak, A. Conducting a meta-analysis: Basics and good practices. Int. J. Rheum. Dis. 2012, 15, 129–135. [Google Scholar] [CrossRef] [PubMed]
- Kim, A.W.; Nyengerai, T.; Mendenhall, E. Evaluating the mental health impacts of the COVID-19 pandemic: Perceived risk of COVID-19 infection and childhood trauma predict adult depressive symptoms in urban South Africa. Psychol. Med. 2020, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Naidoo, T.; Tomita, A.; Paruk, S. Burnout, anxiety and depression risk in medical doctors working in KwaZulu-Natal Province, South Africa: Evidence from a multi-site study of resource-constrained government hospitals in a generalised HIV epidemic setting. PLoS ONE 2020, 15, e0239753. [Google Scholar] [CrossRef] [PubMed]
- Souilhi, A.; Gabsi, A.; Letaief-Ksontini, F.; Chraiet, N.; Yahiaoui, Y.; Mghirbi, F.; Mokrani, A.; Meddeb, K.; Ayadi, M.; Rais, H.; et al. 1572P Psychological impact of the COVID-19 pandemic on health care workers in oncology in Tunisia. Ann. Oncol. 2020, 31, S957. [Google Scholar] [CrossRef]
- Elhadi, M.; Buzreg, A.; Bouhuwaish, A.; Khaled, A.; Alhadi, A.; Msherghi, A.; Alsoufi, A.; Alameen, H.; Biala, M.; Elgherwi, A.; et al. Psychological Impact of the Civil War and COVID-19 on Libyan Medical Students: A Cross-Sectional Study. Front. Psychol. 2020, 11, 570435. [Google Scholar] [CrossRef]
- Sediri, S.; Zgueb, Y.; Ouanes, S.; Ouali, U.; Bourgou, S.; Jomli, R.; Nacef, F. Women’s mental health: Acute impact of COVID-19 pan-demic on domestic violence. Arch. Womens Ment. Health 2020, 23, 749–756. [Google Scholar] [CrossRef]
- Rakhmanov, O.; Demir, A.; Dane, S. A brief communication: Anxiety and depression levels in the staff of a Nigerian private university during COVID 19 pandemic outbreak. J. Res. Med. Dent. Sci. 2020, 8, 118–122. [Google Scholar]
- Elkholy, H.; Tawfik, F.; Ibrahim, I.; Salah El-din, W.; Sabry, M.; Mohammed, S.; Hamza, M.; Alaa, M.; Fawzy, A.Z.; Ashmawy, R.; et al. Mental health of frontline healthcare work-ers exposed to COVID-19 in Egypt: A call for action. Int. J. Soc. Psychiatry 2020, 67, 522–531. [Google Scholar] [CrossRef]
- Keubo, F.R.N.; Mboua, P.C.; Tadongfack, T.D.; Tchoffo, E.F.; Tatang, C.T.; Zeuna, J.I.; Noupoue, E.M.; Tsoplifack, C.B.; Folefack, G.O. Psychological distress among health care professionals of the three COVID-19 most affected Regions in Cameroon: Prevalence and associated factors. In Annales Médico-Psychologiques, Revue Psychiatrique; Elsevier Masson: Paris, France, 2021; Volume 179, pp. 141–146. [Google Scholar] [CrossRef]
- Sagaon-Teyssier, L.; Kamissoko, A.; Yattassaye, A.; Diallo, F.; Castro, D.R.; Delabre, R.; Pouradier, F.; Maradan, G.; Bourrelly, M.; Cissé, M.; et al. Assessment of mental health out-comes and associated factors among workers in community-based HIV care centers in the early stage of the COVID-19 outbreak in Mali. Health Policy Open 2020, 1, 100017. [Google Scholar] [CrossRef]
- Youssef, N.; Mostafa, A.; Ezzat, R.; Yosef, M.; El Kassas, M. Mental health status of health-care professionals working in quaran-tine and non-quarantine Egyptian hospitals during the COVID-19 pandemic. East Mediterr Health J. 2020, 26, 1155–1164. [Google Scholar] [CrossRef] [PubMed]
- Kassaw, C. The Magnitude of Psychological Problem and Associated Factor in Response to COVID-19 Pandemic Among Communities Living in Addis Ababa, Ethiopia, March 2020: A Cross-Sectional Study Design. Psychol. Res. Behav. Manag. 2020, 13, 631–640. [Google Scholar] [CrossRef]
- Idrissi, A.J.; Lamkaddem, A.; Benouajjit, A.; Ben El Bouaazzaoui, M.; El Houari, F.; Alami, M.; Labyad, S.; Chahidi, A.; Benjelloun, M.; Rabhi, S.; et al. Sleep quality and mental health in the context of COVID-19 pandemic and lockdown in Morocco. Sleep Med. 2020, 74, 248–253. [Google Scholar] [CrossRef] [PubMed]
- Shuwiekh, H.A.; Kira, I.A.; Sous, M.S.F.; Ashby, J.S.; Alhuwailah, A.; Baali, S.B.A.; Azdaou, C.; Oliemat, E.M.; Jamil, H.J. The differential mental health impact of COVID-19 in Arab countries. Curr. Psychol. 2020, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Cénat, J.M.; Dalexis, R.D.; Guerrier, M.; Noorishad, P.G.; Derivois, D.; Bukaka, J.; Birangui, J.P.; Adansikou, K.; Clorméus, L.A.; Kokou-Kpolou, C.K.; et al. Frequency and correlates of anxiety symp-toms during the COVID-19 pandemic in low-and middle-income countries: A multinational study. J. Psychiatr. Res. 2021, 132, 13–17. [Google Scholar] [CrossRef]
- Teshome, A.; Glagn, M.; Shegaze, M.; Tekabe, B.; Getie, A.; Assefa, G.; Getahun, D.; Kanko, T.; Getachew, T.; Yenesew, N.; et al. Generalized Anxiety Disorder and Its Associated Fac-tors Among Health Care Workers Fighting COVID-19 in Southern Ethiopia. Psychol. Res. Behav. Manag. 2020, 13, 907. [Google Scholar] [CrossRef] [PubMed]
- Mboua, P.C.; Keubo, F.R.N.; Fouaka, S.G.N. Anxiety and Depression Associated with the Management of COVID-19 among Healthcare Personnel in Cameroon. Evol. Psychiatr. 2020, 86, 131–139. [Google Scholar] [CrossRef] [PubMed]
- Yitayih, Y.; Mekonen, S.; Zeynudin, A.; Mengistie, E.; Ambelu, A. Mental health of healthcare professionals during the early stage of the COVID-19 pandemic in Ethiopia. BJPsych. Open 2021, 7, e1. [Google Scholar] [CrossRef]
- Kounou, K.B.; Guédénon, K.M.; Foli, A.A.D.; Gnassounou-Akpa, E. Mental health of medical professionals during the COVID-19 pandemic in Togo. Psychiatry Clin. Neurosci. 2020, 74, 559–560. [Google Scholar] [CrossRef]
- Essangri, H.; Sabir, M.; Benkabbou, A.; Majbar, M.A.; Amrani, L.; Ghannam, A.; Lekehal, B.; Mohsine, R.; Souadka, A. Predictive Factors for Impaired Mental Health among Medical Students during the Early Stage of the COVID-19 Pandemic in Morocco. Am. J. Trop. Med. Hyg. 2021, 104, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Kibret, S.; Teshome, D.; Fenta, E.; Hunie, M.; Tamire, T. Prevalence of anxiety towards COVID-19 and its associated factors among healthcare workers in a Hospital of Ethiopia. PLoS ONE 2020, 15, e0243022. [Google Scholar] [CrossRef]
- Omar, S.S.; Dawood, W.; Eid, N.; Eldeeb, D.; Munir, A.; Arafat, W. Psychological and Sexual Health During the COVID-19 Pandemic in Egypt: Are Women Suffering More? Sex. Med. 2021, 9, 100295. [Google Scholar] [CrossRef]
- Arafa, A.; Mohamed, A.; Saleh, L.; Senosy, S. Psychological Impacts of the COVID-19 Pandemic on the Public in Egypt. Community Ment. Health J. 2021, 57, 64–69. [Google Scholar] [CrossRef]
- Mulatu, H.A.; Tesfaye, M.; Woldeyes, E.; Bayisa, T.; Fisseha, H.; Asrat, R. The prevalence of common mental disorders among health care professionals during the COVID-19 pandemic at a tertiary Hospital in East Africa. medRxiv 2020. [Google Scholar] [CrossRef]
- Mekonen, E.; Shetie, B.; Muluneh, N. The Psychological Impact of COVID-19 Outbreak on Nurses Working in the Northwest of Amhara Regional State Referral Hospitals, Northwest Ethiopia. Psychol. Res. Behav. Manag. 2021, 13, 1353–1364. [Google Scholar] [CrossRef]
- Elhadi, M.; Msherghi, A.; Elgzairi, M.; Alhashimi, A.; Bouhuwaish, A.; Biala, M.; Abuelmeda, S.; Khel, S.; Khaled, A.; Alsoufi, A.; et al. The mental well-being of frontline physicians working in civil wars under coronavirus disease 2019 pandemic conditions. Front. Psychiatry 2020, 11, 598720. [Google Scholar] [CrossRef]
- Hunter, J.P.; Saratzis, A.; Sutton, A.J.; Boucher, R.H.; Sayers, R.D.; Bown, M. In meta-analyses of proportion studies, funnel plots were found to be an inaccurate method of assessing publication bias. J. Clin. Epidemiol. 2014, 67, 897–903. [Google Scholar] [CrossRef]
- Chen, R.Z.; Zhang, S.X.; Xu, W.; Yin, A.; Dong, R.K.; Chen, B.Z. Meta-Analysis on Mental health disorders in Spain in the COVID-19 Crisis. medRxiv 2021. [Google Scholar]
- Hossain, M.; Rahman, M.; Trisha, N.F.; Tasnim, S.; Nuzhath, T.; Hasan, N.T.; Clark, H.; Das, A.; McKyer, E.L.J.; Ahmed, H.U.; et al. Prevalence of anxiety and depression in South Asia during COVID-19: A systematic review and meta-analysis. Heliyon 2021, 7, e06677. [Google Scholar] [CrossRef] [PubMed]
- Luo, M.; Guo, L.; Yu, M.; Jiang, W.; Wang, H. The psychological and mental impact of coronavirus disease 2019 (COVID-19) on medical staff and general public—A systematic review and meta-analysis. Psychiatry Res. 2020, 291, 113190. [Google Scholar] [CrossRef]
- Jahrami, H.; Bahammam, A.S.; Bragazzi, N.L.; Saif, Z.; Faris, M.; Vitiello, M.V. Sleep problems during the COVID-19 pandemic by population: A systematic review and meta-analysis. J. Clin. Sleep Med. 2021, 17, 299–313. [Google Scholar] [CrossRef] [PubMed]
- Kabiru, C.W.; O Izugbara, C.; Beguy, N. The health and wellbeing of young people in sub-Saharan Africa: An under-researched area? BMC Int. Health Hum. Rights 2013, 13, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ibrahim, A.K.; Kelly, S.J.; Glazebrook, C. Analysis of an Egyptian study on the socioeconomic distribution of depressive symp-toms among undergraduates. Soc. Psychiatry Psychiatr. Epidemiol. 2012, 47, 927–937. [Google Scholar] [CrossRef]
- Ghanem, M.; Gadallah, M.; Meky, F.; Mourad, S.; El Kholy, G. National Survey of Prevalence of Mental Disorders in Egypt: Preliminary survey. East. Mediterr. Health J. 2009, 15, 65–75. [Google Scholar] [CrossRef]
- Gelaye, B.; Lemma, S.; Deyassa, N.; Bahretibeb, Y.; Tesfaye, M.; Berhane, Y.; A Williams, M. Prevalence and Correlates of Mental Distress Among Working Adults in Ethiopia. Clin. Pr. Epidemiol. Ment. Health 2012, 8, 126–133. [Google Scholar] [CrossRef] [Green Version]
- Fekadu, A.; Medhin, G.; Selamu, M.; Hailemariam, M.; Alem, A.; Giorgis, T.W.; Breuer, E.; Lund, C.; Prince, M.; Hanlon, C. Population level mental distress in rural Ethiopia. BMC Psychiatry 2014, 14, 194. [Google Scholar] [CrossRef] [Green Version]
- Yimam, K.; Kebede, Y.; Azale, T. Prevalence of common mental disorders and associated factors among adults in Kombolcha Town, Northeast Ethiopia. J. Depress. Anxiety 2014, S1, 007. [Google Scholar] [CrossRef]
- Kadri, N.; Agoub, M.; Assouab, F.; Tazi, M.A.; Didouh, A.; Stewart, R.; Moussaoui, D. Moroccan national study on prevalence of mental dis-orders: A community-based epidemiological study. Acta Psychiatr. Scand. 2010, 121, 71–74. [Google Scholar] [CrossRef] [PubMed]
- Kadri, N.; Agoub, M.; El Gnaoui, S.; Berrada, S.; Moussaoui, D. Prevalence of anxiety disorders: A population-based epidemio-logical study in metropolitan area of Casablanca, Morocco. Ann. Gen. Psychiatry. 2007, 6, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amoran, O.; Lawoyin, T.; Lasebikan, V. Prevalence of depression among adults in Oyo State, Nigeria: A comparative study of rural and urban communities. Aust. J. Rural. Health 2007, 15, 211–215. [Google Scholar] [CrossRef]
- Stanley, N.; Chinwe, E.S. Prevalence of Mental Disorders in Abakaliki, Ebonyi State, Southeastern Nigeria. J. Am. Psychiatr. Nurses Assoc. 2020, 1078390320951910. [Google Scholar] [CrossRef]
- Nwachukwu, C.E.; Olufunmilayo, E.O.; Otor, V.O.; Yakubu, A.O.; Akingbade, A.E.; Odefemi, O.F.; Ikwunne, B.N.; Kowe, T.F.; Morakinyo, O.E.; Oyebamiji, T.A.; et al. Common mental health problems and associated factors among medical students of University of Ibadan, Nigeria. J. Ment. Health 2021, 30, 315–322. [Google Scholar] [CrossRef]
- Chinawa, A.T.; Chinawa, J.M.; Aniwada, E.; Amadi, O.; Ndukuba, A.C.; Uwaezuoke, S.N. Spectrum of Anxiety Disorders Among Medical Students in a Nigerian Medical School: A Cross-Sectional Study With Standardized Screening Tools. J. Educ. Dev. Psychol. 2018, 8, 132. [Google Scholar] [CrossRef]
- Williams, D.R.; Herman, A.; Stein, D.; Heeringa, S.G.; Jackson, P.B.; Moomal, H.; Kessler, R.C. Twelve-month mental disorders in South Africa: Prevalence, service use and demographic correlates in the population-based South African Stress and Health Study. Psychol. Med. 2007, 38, 211–220. [Google Scholar] [CrossRef] [Green Version]
- Peltzer, K.; Pengpid, S. Social determinants of depression among adults in South Africa. J. Hum. Behav. Soc. Environ. 2020, 30, 525–532. [Google Scholar] [CrossRef]
- Munyandamutsa, N.; Nkubamugisha, P.M.; Gex-Fabry, M.; Eytan, A. Mental and physical health in Rwanda 14 years after the genocide. Soc. Psychiatry Psychiatr. Epidemiol. 2012, 47, 1753–1761. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sipsma, H.; Ofori-Atta, A.; Canavan, M.; Osei-Akoto, I.; Udry, C.; Bradley, E.H. Poor mental health in Ghana: Who is at risk? BMC Public Health 2013, 13, 288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dzator, J. Hard Times and Common Mental Health Disorders in Developing Countries: Insights from Urban Ghana. J. Behav. Health Serv. Res. 2012, 40, 71–87. [Google Scholar] [CrossRef] [PubMed]
- Nakimuli-Mpungu, E.; Bass, J.K.; Alexandre, P.; Mills, E.J.; Musisi, S.; Ram, M.; Katabira, E.; Nachega, J.B. Depression, alcohol use and adherence to an-tiretroviral therapy in sub-Saharan Africa: A systematic review. AIDS Behav. 2012, 16, 2101–2118. [Google Scholar] [CrossRef]
- Sankoh, O.; Sevalie, S.; Weston, M. Mental health in Africa. Lancet Glob. Health 2018, 6, e954–e955. [Google Scholar] [CrossRef]
- Okasha, A. Mental health in Africa: The role of the WPA. World Psychiatry 2002, 1, 32–35. [Google Scholar]
- Sweetland, A.C.; Belkin, G.S.; Verdeli, H. Measuring depression and anxiety in Sub-Saharan Africa. Depress. Anxiety 2014, 31, 223–232. [Google Scholar] [CrossRef] [Green Version]
- Stein, F.; Perry, M.; Banda, G.; Woolhouse, M.; Mutapi, F. Oxygen provision to fight COVID-19 in sub-Saharan Africa. BMJ Glob. Health 2020, 5, e002786. [Google Scholar] [CrossRef]
- Chang, A.Y.; Gómez-Olivé, F.X.; Payne, C.; Rohr, J.K.; Manne-Goehler, J.; Wade, A.N.; Wagner, R.G.; Montana, L.; Tollman, S.; A Salomon, J. Chronic multimorbidity among older adults in rural South Africa. BMJ Glob. Health 2019, 4, e001386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Programme UND. Human Development Report: 1995; The World Bank: Washington, DC, USA, 1995. [Google Scholar]
- Brown, J.C. African Development Indicators 1998/99; The World Bank: Washington, DC, USA, 1998. [Google Scholar]





| Characteristics | Total Number of Studies/Samples * | Percent (%) | Number of Participants | Percent (%) | Level of Analysis |
|---|---|---|---|---|---|
| Overall | 28/32 | 100 | 15,071 | 100 | |
| Population | 32 | 100 | Sample | ||
| Frontline HCWs | 3 | 9.4 | 919 | 6.1 | |
| General HCWs | 12 | 37.5 | 3928 | 26.1 | |
| General population | 15 | 46.8 | 7245 | 48.1 | |
| Medical students | 2 | 6.3 | 2979 | 19.8 | |
| Outcome # | 137 | Prevalence | |||
| Anxiety | 62 | 45.3 | 14,847 | 98.5 | |
| Depression | 54 | 39.4 | 12,688 | 84.2 | |
| Insomnia | 21 | 15.3 | 4144 | 27.5 | |
| Severity # | 137 | Prevalence | |||
| Above mild | 55 | 40.2 | 6174 | 41.0 | |
| Above moderate | 45 | 32.9 | 3511 | 23.3 | |
| Above severe | 33 | 24.1 | 4133 | 27.4 | |
| Overall | 4 | 2.8 | 1253 | 8.3 | |
| Sampling Country | 32 | Sample | |||
| Cameroon | 2 | 6.3 | 624 | 4.1 | |
| Egypt | 6 | 18. | 3593 | 23.8 | |
| Ethiopia | 7 | 21.8 | 2778 | 18.4 | |
| Libya | 3 | 9.3 | 3329 | 22.1 | |
| Mali | 1 | 3.1 | 135 | 0.9 | |
| Morocco | 2 | 6.3 | 1395 | 9.3 | |
| Nigeria | 3 | 9.3 | 953 | 6.3 | |
| RDC | 1 | 3.1 | 626 | 4.2 | |
| Rwanda | 1 | 3.1 | 174 | 1.2 | |
| South Africa | 2 | 6.3 | 361 | 2.4 | |
| Togo | 2 | 6.3 | 304 | 2.0 | |
| Tunisia | 2 | 6.3 | 799 | 5.3 | |
| Quality | Article | ||||
| High | 3 | 21.4 | 2621 | 17.4 | |
| Medium | 22 | 78.6 | 12,450 | 82.6 | |
| Design | Article | ||||
| Cohort | 1 | 3.3 | 211 | 1.4 | |
| Cross-sectional | 27 | 96.7 | 14,860 | 98.6 | |
| Data collection time | Article | ||||
| The first six months | 22 | 80.2 | |||
| After the first six months | 6 | 19.8 | 12,450 | 82.6 | |
| Mean (median) | Range | 2621 | 17.4 | ||
| Number of participants | 471 (327) | 48–2430 | - | - | Sample |
| Female proportion | 53.1% (56.6%) | 0–100% | - | - | Sample |
| Response rate | 54.9% (49.0%) | 18.2–94.2% | - | - | Sample |
| First-Level Subgroup | Second-Level Subgroup | Prevalence (%) | 95% CI (%) | p Value * |
|---|---|---|---|---|
| Aggregated | 39 | 34–44 | <0.001 | |
| Outcome | Anxiety | 37 | 31–44 | <0.001 |
| Depression | 45 | 38–53 | <0.001 | |
| Insomnia | 28 | 18–40 | <0.001 | |
| Population | Frontline HCWs | 49 | 35–63 | <0.001 |
| General HCWs | 36 | 28–45 | <0.001 | |
| General population | 38 | 31–45 | <0.001 | |
| Medical students | 38 | 25–52 | <0.001 | |
| Severity | Above mild | 62 | 56–67 | <0.001 |
| Above moderate | 34 | 29–40 | <0.001 | |
| Above severe | 14 | 10–20 | <0.001 | |
| Overall | 17 | 09–27 | <0.001 | |
| Region | Sub-Saharan Africa | 30 | 24–36 | <0.001 |
| North Africa | 46 | 40 -53 | <0.001 | |
| Quality | Studies with medium quality | 51 | 40–63 | <0.001 |
| Studies with high quality | 37 | 32–42 | <0.001 | |
| Data collection time | The first six months | 42 | 36–47 | <0.001 |
| After the first six months | 26 | 17–35 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, J.; Farah, N.; Dong, R.K.; Chen, R.Z.; Xu, W.; Yin, J.; Chen, B.Z.; Delios, A.Y.; Miller, S.; Wan, X.; et al. Mental Health during the COVID-19 Crisis in Africa: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 10604. https://doi.org/10.3390/ijerph182010604
Chen J, Farah N, Dong RK, Chen RZ, Xu W, Yin J, Chen BZ, Delios AY, Miller S, Wan X, et al. Mental Health during the COVID-19 Crisis in Africa: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2021; 18(20):10604. https://doi.org/10.3390/ijerph182010604
Chicago/Turabian StyleChen, Jiyao, Nusrat Farah, Rebecca Kechen Dong, Richard Z. Chen, Wen Xu, Jin Yin, Bryan Z. Chen, Andrew Yilong Delios, Saylor Miller, Xue Wan, and et al. 2021. "Mental Health during the COVID-19 Crisis in Africa: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 18, no. 20: 10604. https://doi.org/10.3390/ijerph182010604