
Severe Fever with Thrombocytopenia Syndrome with Necrotizing Lymphadenitis in a Patient who Underwent 18F-FDG PET/CT: A Case Report


Abstract
:1. Introduction
2. Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tsuru, M.; Suzuki, T.; Murakami, T.; Matsui, K.; Maeda, Y.; Yoshikawa, T.; Kurosu, T.; Shimojima, M.; Shimada, T.; Hasegawa, H.; et al. Pathological Characteristics of a Patient with Severe Fever with Thrombocytopenia Syndrome (SFTS) Infected with SFTS Virus through a Sick Cat’s Bite. Viruses 2021, 13, 204. [Google Scholar] [CrossRef] [PubMed]
- Casel, M.A.; Park, S.J.; Choi, Y.K. Severe Fever with Thrombocytopenia Syndrome Virus: Emerging Novel Phlebovirus and Their Control Strategy. Exp. Mol. Med. 2021, 53, 713–722. [Google Scholar] [CrossRef] [PubMed]
- Saijo, M. Pathophysiology of Severe Fever with Thrombocytopenia Syndrome and Development of Specific Antiviral Therapy. J. Infect. Chemother. 2018, 24, 773–781. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Korea Centers for Disease Control and Prevention. Infectious Diseases Surveillance Yearbook 2020; Korea Centers for Disease Control and Prevention (KCDC): Osong-eup, Korea, 2021. [Google Scholar]
- Yun, S.; Park, S.; Kim, Y.; Park, S.; Yu, M.; Kwon, H.; Kim, E.; Yu, K.; Jeong, H.; Ryou, J.; et al. Genetic and Pathogenic Diversity of Severe Fever with Thrombocytopenia Syndrome Virus (SFTSV) in South Korea. J. Clin. Investig. 2020, 5, e129531. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kang, C.K.; Choi, S.J.; Koh, J.; Jeon, Y.K.; Kim, K.H.; Chung, J.; Choe, P.G.; Kim, N.J.; Park, W.B.; Oh, M.D. 18F-FDG PET and Histopathologic Findings in a Patient with Severe Fever with Thrombocytopenia Syndrome. Ticks Tick Borne Dis. 2018, 9, 972–975. [Google Scholar] [CrossRef] [PubMed]
- Sakr, M. Cervical: Lymphadenopathy. Head Neck Endocr. Surg. 2016, 163–190. [Google Scholar]
- Fijten, G.H.; Blijham, G.H. Unexplained Lymphadenopathy in Family Practice. An Evaluation of the Probability of Malignant Causes and the Effectiveness of Physicians’ Workup. J. Fam. Pract. 1988, 27, 373–376. [Google Scholar] [CrossRef] [PubMed]
- Nagaraju, S.; Vaishnav, S.; Burke, L.H.; Norman, E.M. Histiocytic Necrotising Lymphadenitis (Kikuchi–Fujimoto Disease) of Axillary Lymph Nodes. BMJ Case Rep. 2015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, J.; Zhen, L.; Zhuang, H. Bone Marrow Metastases from Alveolar Rhabdomyosarcoma with Impressive FDG PET/CT Finding but Less-Revealing Bone Scintigraphy. Clin. Nucl. Med. 2013, 38, 988–991. [Google Scholar] [CrossRef] [PubMed]
- Jin, H.; Yuan, L.; Li, C.; Kan, Y.; Hao, R.; Yang, J. Diagnostic Performance of FDG PET or PET/CT in Prosthetic Infection after Arthroplasty: A Meta-Analysis. Q. J. Nucl. Med. Mol. Imaging Off. 2014, 58, 85–93. [Google Scholar]
- Hao, R.; Yuan, L.; Kan, Y.; Li, C.; Yang, J. Diagnostic Performance of 18F-FDG PET/CT in Patients with Fever of Unknown Origin: A Meta-Analysis. Nucl. Med. Commun. 2013, 34, 682–688. [Google Scholar] [CrossRef] [PubMed]
- Zou, Q.; Jiao, J.; Yang, T.; Zhang, Y. Role of 18F-FDG PET/CT in the Assessment of Kikuchi-Fujimoto Disease and Its Differential Diagnosis from non-Hodgkin Lymphoma. J. Nucl. Med. 2019, 60, 1073. [Google Scholar]
- Deng, Y.; Li, X.; Xiang, Y.; Li, H.; Lu, P.; Yu, W. Application of 18F-FDG PET/CT in the Diagnosis of Extrapulmonary Tuberculosis. Rad. Infect. Dis. 2018, 5, 165–170. [Google Scholar] [CrossRef]
- Yuan, L.; Kan, Y.; Meeks, J.K.; Ma, D.; Yang, J. 18F-FDG PET/CT for Identifying the Potential Causes and Extent of Secondary Hemophagocytic Lymphohistiocytosis. Diagn. Interv. Radiol. 2016, 22, 471–475. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Tests | Results | Reference Range |
|---|---|---|
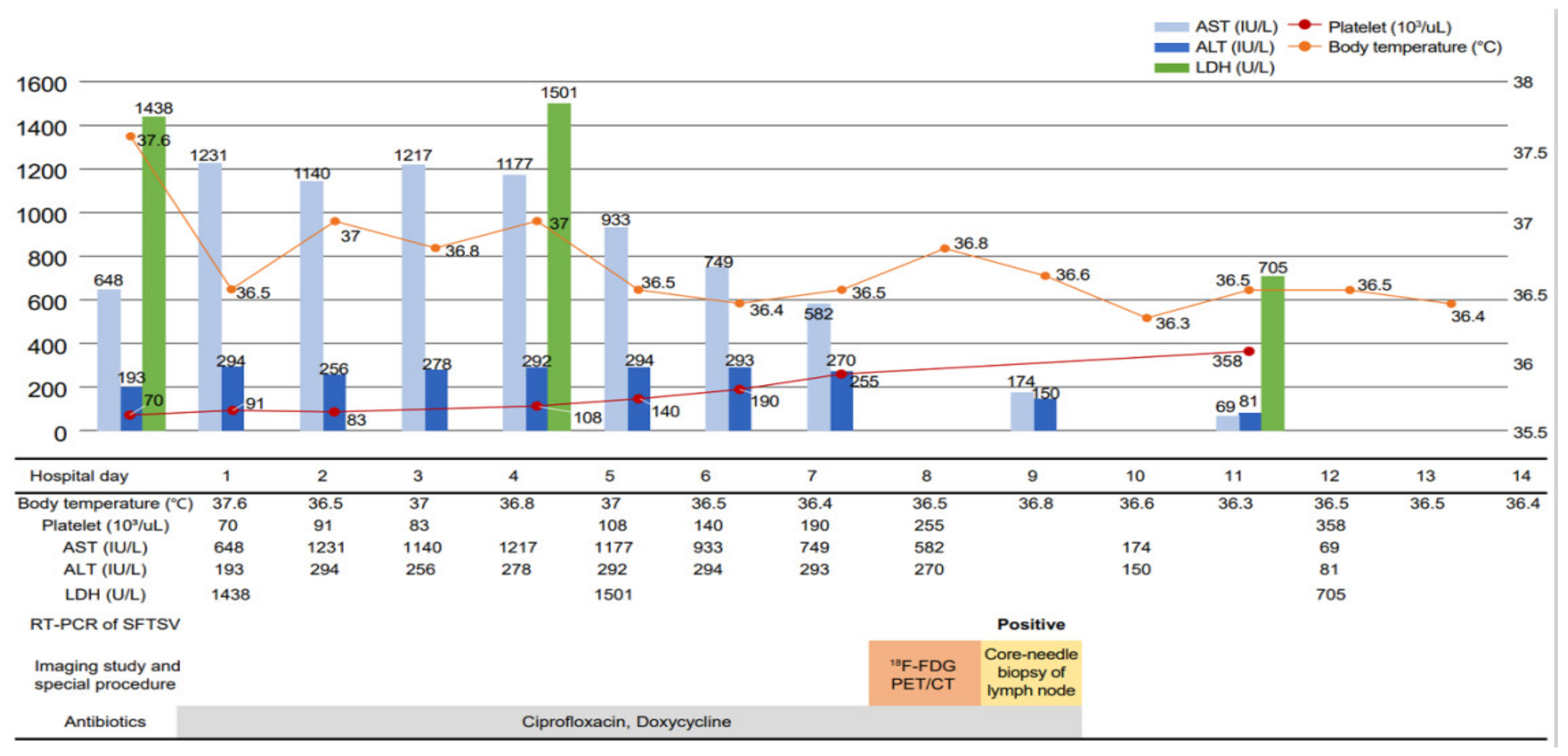
| WBC * (/uL) Neutrophil (/uL) Lymphocyte (/uL) Hemoglobin (g/dL) Platelet (/uL) C-reactive protein (mg/dL) ESR † (mm/h) Aspart aminotransferase, AST (IU/L) Alanine transaminase, ALT (IU/L) Lactate dehydrogenase, LDH (IU/L) Total bilirubin (mg/dL) Orientia tsutsugamushi antibody Hantaan virus antibody Leptospira antibody VDRL ‡ Anti-HIV § Anti-HCV ∥ Anti-HAV ** IgM Anti-HBs Ab/HBs Ag *** | 1590 970 380 11.9 70,000 0.39 15 648 193 1483 0.3 Negative Negative Negative Negative Negative Negative Negative Negative/negative | 4000–11,000 1700–7000 1000–4000 13.5–17.5 140,000–400,000 0–0.5 0–20 0–35 0–35 273–490 0.3–1.2 Negative Negative Negative Negative Negative Negative Negative Negative/negative |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, A.R.; Kim, T.; Shin, D.-H.; Lee, S.; Lim, S. Severe Fever with Thrombocytopenia Syndrome with Necrotizing Lymphadenitis in a Patient who Underwent 18F-FDG PET/CT: A Case Report. Int. J. Environ. Res. Public Health 2021, 18, 10488. https://doi.org/10.3390/ijerph181910488
Kim AR, Kim T, Shin D-H, Lee S, Lim S. Severe Fever with Thrombocytopenia Syndrome with Necrotizing Lymphadenitis in a Patient who Underwent 18F-FDG PET/CT: A Case Report. International Journal of Environmental Research and Public Health. 2021; 18(19):10488. https://doi.org/10.3390/ijerph181910488
Chicago/Turabian StyleKim, A Reum, Taehwa Kim, Dong-Hoon Shin, Sujin Lee, and Seungjin Lim. 2021. "Severe Fever with Thrombocytopenia Syndrome with Necrotizing Lymphadenitis in a Patient who Underwent 18F-FDG PET/CT: A Case Report" International Journal of Environmental Research and Public Health 18, no. 19: 10488. https://doi.org/10.3390/ijerph181910488