
Effect of Smartphone App’s Intervention on Consumers’ Knowledge, Attitude, Practice, and Perception of Food Poisoning Prevention When Dining Out at Selected Rural Areas in Terengganu

 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Research Methodology
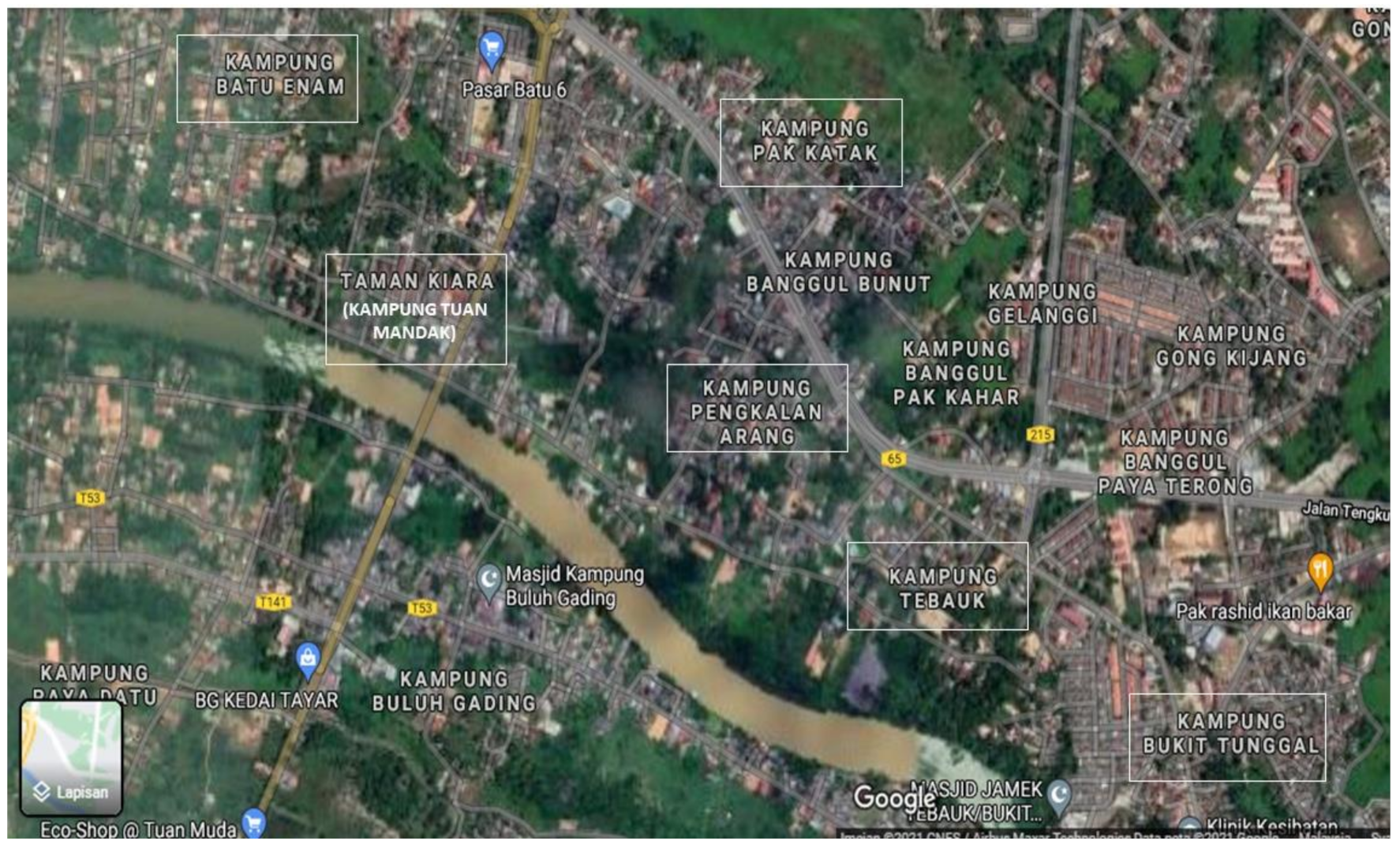
2.1. Study Location
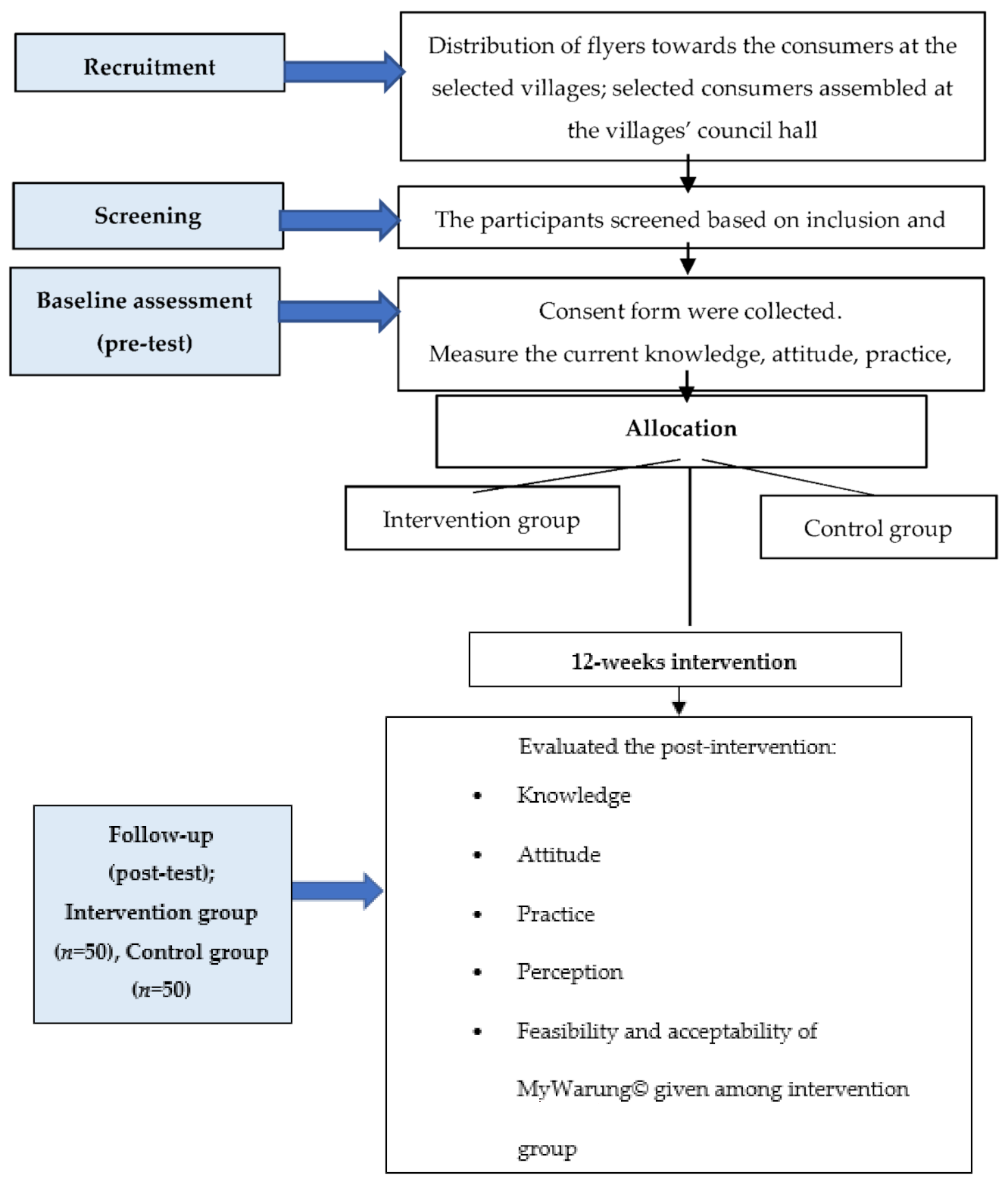
2.2. Study Design
2.3. Study Sampling
2.4. Instruments
2.4.1. MyWarung© Mobile Application
2.4.2. KAP2 Questionnaire
2.5. Recruitment and Data Collection
2.6. Intervention Protocol
2.7. Outcome Measures
2.8. Data Analysis
3. Results
3.1. Sociodemography
3.2. Between-Group Differences
3.3. Within-Group Differences
3.3.1. Effect of an Intervention Programme on Knowledge towards Food Poisoning and Its Prevention
3.3.2. Effect of an Intervention Programme on Food Poisoning Preventive Attitude
3.3.3. Effect of an Intervention Programme on Food Poisoning Preventive Practice
3.3.4. Effect of an Intervention Programme on Food Poisoning Preventive Perception
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Yusof, A.M.M.; Rahman, N.A.; Haque, M. Knowledge, attitude, and practice toward food poisoning among food handlers and dietetic students in a public university in Malaysia. J. Pharm. Bioallied Sci. 2018, 10, 232–239. [Google Scholar] [CrossRef]
- Centres for Disease Control and Prevention (CDC). Food Safety: Foodborne Illnesses and Germs. Available online: https://www.cdc.gov/foodsafety/foodborne-germs.html (accessed on 15 July 2019).
- Centres for Disease Control and Prevention (CDC). Foods That Can Cause Food Poisoning. Available online: https://www.cdc.gov/foodsafety/foods-linked-illness.html#fruits (accessed on 19 June 2021).
- World Health Organization (WHO). Food safety. Available online: https://www.who.int/news-room/fact-sheets/detail/food-safety (accessed on 9 June 2020).
- Yew, J.; Tang, H.; Shahril, M.R. Feasibility and acceptability of EatSAFE-StopWASTE © mobile app. Int. J. Eng. Technol. 2018, 7, 117–121. [Google Scholar]
- Malaysia Ministry of Health (MOH). Health Facts 2019: Reference Data for 2018, 2019; Malaysia Ministry of Health: Putrajaya, Malaysia, 2019; pp. 16–17. [Google Scholar]
- New, C.Y.; Ubong, A.; Premarathne, J.M.K.J.K.; Thung, T.Y.; Lee, E.; Chang, W.S.; Son, R. Microbiological food safety in Malaysia from the academician’s perspective. Food Res. 2017, 1, 183–202. [Google Scholar] [CrossRef]
- Bisholo, K.Z.; Ghuman, S.; Haffejee, F. Food-borne disease prevalence in rural villages in the Eastern Cape, South Africa. Afr. J. Prim. Health Care Fam. Med. 2018, 10, 1–5. [Google Scholar] [CrossRef]
- Chellaiyan, V.G.J.; Fasna, L.; Mallika, S.V. Food safety awareness and food handling practices among rural population of Tamil Nadu. Int. J. Community Med. Public Health 2018, 5, 1441–1447. [Google Scholar] [CrossRef]
- Mahmood, K.; Khalid, J.; Kamilah, H.; Ali, A.J.; Muhammad, L.; Ariffin, F. An empirical study of food safety, food handling, and food poisoning awareness among foreign students in Penang, Malaysia. Int. J. Adv. Sci. Eng. Inf. Technol. 2018, 8, 150–156. [Google Scholar] [CrossRef]
- Theng, L.S.; Adnan, S.A.B.M.; Jaafar, N.M.; Jaafar, S.N.; Mahyudin, N. Comparative study of consumers’ knowledge and attitudes towards food safety and purchase intention of night market foods containing poultry in low and high food poisoning cases states. Malays. Appl. Biol. 2017, 46, 131–141. [Google Scholar]
- Greig, J.D.; Todd, E.C.D.; Bartleson, C.A.; Michaels, B.S. Outbreaks where food workers have been implicated in the spread of foodborne disease. Part 1. Description of the problem, methods, and agents involved. J. Food Prot. 2007, 70, 1752–1761. [Google Scholar] [CrossRef] [Green Version]
- Ruby, G.E.; Fatimah, U.; Zainal, U.; Lihan, S.; Noorahya, N.; Radu, S. Predicting intention on safe food handling among adult consumers: A cross-sectional study in Sibu district, Malaysia. Food Control 2019, 106, 1–8. [Google Scholar] [CrossRef]
- Asma, A.; Wan Syakirah Alia, W.M.S.; Aziz, Y.; Hayati, M.Y. Energy contribution of NOVA food groups and socio-demographic determinants of ultra-processed groups among adults in Terengganu, Malaysia. Food Res. 2019, 3, 640–648. [Google Scholar] [CrossRef]
- Pawan, M.T.; Langgat, J.; Marzuki, K.M. Study on generation Y dining out behavior in Sabah, Malaysia. Int. J. Bus. Soc. Sci. 2014, 5, 92–101. [Google Scholar]
- Poulain, J.; Laporte, C.; Tibere, L.; Mognard, E.; Ragavan, N.; Ashrafzadeh, A.; Ismail, M.N. Malaysian Food Barometer (MFB): A study of the impact of compressed modernisation on food habits. Malays. J. Nutr. 2020, 26, 1–17. [Google Scholar] [CrossRef]
- Nee, S.O.; Sani, N.A. Assessment of knowledge, attitudes and practices (KAP) among food handlers at residential colleges and canteen regarding food safety. Sains Malays. 2011, 40, 403–410. [Google Scholar]
- Lim, T.; Yee, F.; Rosni, M.; Mohd, N. A structural modelling on food safety knowledge, attitude, and behaviour among Bum Bum Island community of Semporna, Sabah. Food Control 2015, 60, 241–246. [Google Scholar] [CrossRef]
- Ministry of Health Malaysia (MOH). Annual Report Food Safety and Quality Division; Ministry of Health Malaysia: Putrajaya, Malaysia, 2016; pp. 1–37. [Google Scholar]
- Ali, A.N.; William, A.F.; Prajapati, S.K.; Ahmed, N.Z. A KAP study on food safety and hygiene among private university students in Kedah state, Malaysia. J. Nat. Remedies 2018, 18, 114–121. [Google Scholar] [CrossRef] [Green Version]
- Odeyemi, O.A.; Sani, N.A.; Obadina, A.O.; Saba, C.K.S.; Bamidele, F.A.; Abughoush, M.; Aberoumand, A. Food safety knowledge, attitudes and practices among consumers in developing countries: An international survey. Food Res. Int. 2018, 116, 1386–1390. [Google Scholar] [CrossRef]
- Hosseintalaei, M.; Shahnazi, H.; Mohammadi, M. The relationship of perceived susceptibility and self-efficacy with the decayed, missing, and filled teeth in pregnant women: A study based on the health belief model. Biomed. Res. 2017, 28, 8142–8148. [Google Scholar]
- Abdullah, N.B.A.; Ismail, A.F. Food poisoning outbreaks among schoolchildren in Terengganu and their associated factors. Sains Malays. 2021, 50, 1027–1036. [Google Scholar] [CrossRef]
- Adebowale, O.O.; Kassim, I.O. Food safety and health: A survey of rural and urban household consumer practices, knowledge to food safety and food-related illnesses in Ogun state. Epidemiol. Biostat. Public Health 2017, 14, e12568. [Google Scholar] [CrossRef]
- Soon, J.M. Consumers’ awareness and trust toward food safety news on social media in Malaysia. J. Food Prot. 2020, 83, 452–459. [Google Scholar] [CrossRef]
- Ruby, G.E.; Fatimah, U.; Zainal, U.; Lihan, S.; Noorahya, N.; Radu, S. A cross-sectional study on food safety knowledge among adult consumers. Food Control 2019, 99, 98–105. [Google Scholar] [CrossRef]
- Nielsen. The U.S Digital Consumer Report—Nielsen 2014. Available online: https://www.nielsen.com/us/en/insights/report/2014/the-us-digital-consumer-report/ (accessed on 3 March 2020).
- Middelweerd, A.; Mollee, J.; Klein, M.M.; Manzoor, A.; Brug, J.; Te Velde, S.J. The use and effects of an app-based physical activity intervention “Active2Gether” in young adults: Quasi-experimental trial. JMIR Form. Res. 2020, 4, 1–19. [Google Scholar] [CrossRef] [Green Version]
- Ali, Z.C.; Silvioli, R.; Rajai, A.; Aslam, T.M. Feasibility of use of a mobile application for nutrition assessment pertinent to age-related macular degeneration (MANAGER2). Transl. Vis. Sci. Technol. 2017, 6, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Proudfoot, J.; Parker, G.; Pavlovic, D.H.; Manicavasagar, V.; Adler, E.; Whitton, A. Community attitudes to the appropriation of mobile phones for monitoring and managing depression, anxiety, and stress. J. Med. Internet Res. 2010, 12, 1–13. [Google Scholar] [CrossRef]
- Ibrahim, U.I.; Lin, L.P. Innovare academic sciences feasibility and acceptability of my electronic personal health record monitor (MY-EPHRM). Int. J. Pharm. Pharm. Sci. 2015, 7, 228–232. [Google Scholar]
- McKenzie, L.B.; Roberts, K.J.; Roxanne, C.; Rebecca, M.; Mahmoud, A.-R.; Elizabeth, G.K.; Wendy, C.S. A randomized controlled trial to evaluate the make safe happen app—A mobile technology-based safety behavior change intervention for increasing parents’ safety knowledge and actions. Inj. Epidemiol. 2018, 5, 1–9. [Google Scholar] [CrossRef]
- Salihah, N.; Lua, P.L.; Ahmad, A.; Shahril, M.R. “CandiTm”: A Malaysian-tailored dietary smartphone app for cancer patients and survivors. Malays. J. Public Health Med. 2017, 1, 32–40. [Google Scholar]
- Yaacob, N.A.; Fadhil, M.; Marzuki, M.; Yaacob, N.M. Effectiveness of the ColorApp. Mobile App for health education and promotion for colorectal cancer: Quasi-experimental study. JMIR Hum. Factor 2020, 7, 1–9. [Google Scholar] [CrossRef]
- Has, S.M.C.; Jaafar, S.N.A.; Chilek, T.Z.T. An assessment on pre-and post-food hygiene training on food safety’s Kap level among food handlers in Kuala Terengganu and Kuala Nerus. Malays. Appl. Biol. 2018, 47, 61–69. [Google Scholar]
- Kuala Terengganu City Council. Rancangan Kawasan Khas Pusat Pentadbiran Kuala Nerus 2014–2025, 1st ed.; Majlis Bandaraya Kuala Terengganu: Terengganu, Malaysia, 2014; pp. 1–32. [Google Scholar]
- Malaysia Ministry of Rural Development. Rural Development Policy; Malaysia Ministry of Rural Development: Putrajaya, Malaysia, 2016; pp. 1–11. [Google Scholar]
- Terengganu State Economic Planning Unit. Data Asas Negeri Terengganu; Terengganu State Economic Planning Unit: Terengganu, Malaysia, 2017; pp. 30–39. [Google Scholar]
- Kuala Nerus District and Land Office. Latar Belakang Daerah Kuala Nerus. Available online: http://pdtknerus.terengganu.gov.my/index.php?option=com_content&view=article&id=81&Itemid=97 (accessed on 7 February 2021).
- Department of Statistics Malaysia. Population and Housing Census. 2021. Available online: https://www.dosm.gov.my/v1/index.php?r=column/cone&menu_id=bDA2VkxRSU40STcxdkZ4OGJ0c1ZVdz09 (accessed on 7 February 2021).
- Aung, M.M.T.; Hassan, A.; Kadarman, N.; Hussin, T.M.A.R.; Barman, A.; Ismail, S.; Hashim, S.E. Knowledge, attitude, practices related to Dengue fever among rural population in Terengganu, Malaysia. Malays. J. Public Health Med. 2016, 16, 15–23. [Google Scholar]
- Jaafar, I.; Azmina Ibrahim, T.; Awanis Ahmad, N.; Abdul Kadir, A.; Razali Md Tomari, M. Waste generation and characteristization: Case study of Seberang Takir, Kuala Nerus, Terengganu, Malaysia. J. Phys. Conf. Ser. 2018, 1049. [Google Scholar] [CrossRef]
- Malaysian Communication and Multimedia Commission. In-Hand Phone Users Survey 2018, 1st ed.; Malaysian Communications and Multimedia Commission: Selangor, Malaysia, 2018; pp. 3–5. [Google Scholar]
- Al-Jaberi, M.A.; Juni, M.H.; Shahar, H.K.; Ismail, S.I.F.; Saeed, M.A.; Ying, L.P. Effectiveness of an educational intervention in reducing new international postgraduates’ acculturative stress in Malaysian public universities: Protocol for a cluster randomized controlled trial. JMIR Res. Protoc. 2020, 9, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Des Jarlais, D.C.; Lyles, C.; Crepaz, N. Improving the reporting quality of nonrandomized evaluations of behavioral and public health interventions: The TREND statement. Am. J. Public Health 2004, 94, 361–366. [Google Scholar] [CrossRef] [PubMed]
- Eysenbach, G. Consort-ehealth: Improving and standardizing evaluation reports of web-based and mobile health interventions. J. Med. Internet Res. 2011, 13, 1–10. [Google Scholar] [CrossRef]
- Alzoubi, M.M.; Hayati, K.S.; Rosliza, A.M.; Ahmad, A.A.; Al-Hamdan, Z.M. Total quality management intervention for enhancing nursing commitment and performance in Jordanian hospital: Protocol of a quasi-experimental study. Int. J. Adv. Sci. Res. Dev. 2018, 5, 1–10. [Google Scholar] [CrossRef]
- Thiese, M.S. Observational and interventional study design types: An overview. Biochem. Med. 2014, 24, 199–210. [Google Scholar] [CrossRef]
- Hirschmann, R. Malaysia: Share of Rural Population. 2021. Available online: https://www.statista.com/statistics/760965/malaysia-share-of-rural-population/ (accessed on 16 April 2021).
- Sharif Ishak, S.I.Z.; Chin, Y.S.; Mohd Taib, M.N.; Chan, Y.M.; Mohd Shariff, Z. Effectiveness of a school-based intervention on knowledge, attitude and practice on healthy lifestyle and body composition in Malaysian adolescents. BMC Pediatrics 2020, 20, 1–12. [Google Scholar] [CrossRef]
- Attri, J.P.; Kaur, H. Basic concepts for sample size calculation: Critical step for any clinical trials. Saudi J. Anaesth. 2016, 10, 65–68. [Google Scholar] [CrossRef]
- Charan, J.; Biswas, T. How to calculate sample size for different study designs in medical research? Indian J. Psychol. Med. 2013, 35, 121–126. [Google Scholar] [CrossRef] [Green Version]
- Nik Rosmawati, N.H.; Wan Manan, W.M.; Noor Izani, N.J.; Nik Nurain, N.H.; Razlina, A.R. The effect of food safety education on handwashing practices in school canteens’ food handlers. Sains Malays. 2018, 47, 2119–2128. [Google Scholar] [CrossRef]
- Mu, W.; Spaargaren, G.; Lansink, A.O. Mobile apps for green food practices and the role for consumers: A case study on dining out practices with Chinese and Dutch young consumers. Sustainability 2019, 11, 1275. [Google Scholar] [CrossRef] [Green Version]
- Zyoud, S.; Shalabi, J.; Imran, K.; Ayaseh, L.; Radwany, N.; Salameh, R.; Al-Jabi, S. Knowledge, attitude and practices among parents regarding food poisoning: A cross-sectional study from Palestine. BMC Public Health 2019, 19, 1–10. [Google Scholar] [CrossRef]
- Malaysia Ministry of Health (MOH). Keracunan Makanan—Portal MyHealth. 2012. Available online: http://www.myhealth.gov.my/keracunan-makanan/ (accessed on 11 April 2021).
- Malaysia Ministry of Health (MOH). Panduan Memilih Premis Makanan Yang Bersih—PORTAL MyHEALTH. 2014. Available online: http://www.myhealth.gov.my/panduan-memilih-premis-makanan-yang-bersih/ (accessed on 11 April 2021).
- Knight-agarwal, C.; Davis, D.L.; Williams, L.; Davey, R.; Cox, R. Development and Pilot Testing of the Eating4two Mobile Phone App to Monitor Gestational Weight Gain. JMIR MHealth UHealth. 2015, 3, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Low, W.Y.; Jani, R.; Halim, H.A.; Alias, A.A.; Moy, F.M. Determinants of food hygiene knowledge among youths: A cross-sectional online study. Food Control 2016, 59, 88–93. [Google Scholar] [CrossRef]
- Ismail, S.N.S.; Rangga, J.U.; Rasdi, I.; Rahman, U.R.A.; Samah, M.A.A. Mobile apps application to improve safety and health knowledge, attitude and practice among university students. Malays. J. Med. Health Sci. 2018, 14, 47–55. [Google Scholar]
- Nik Rosmawati, N.H.; Wan Muda, W.M.; Noor Izani, N.J.; Nik Nurain, N.H.; Razlina, A.R. Effect of food safety training on food handlers’ knowledge and practices: A randomized controlled trial. Br. Food J. 2016, 118, 795–808. [Google Scholar] [CrossRef]
- Gupta, V.; Khanna, K.; Gupta, R.K. A study on the street food dimensions and its effects on consumer attitude and behavioural intentions. Tour. Rev. 2018, 73, 374–388. [Google Scholar] [CrossRef]
- Karanicolas, P.J.; Farrokhyar, F.; Bhandari, M. Blinding: Who, what, when, why, how. Can. J. Surg. 2010, 53, 345–348. [Google Scholar]
- Koo, H.C.; Poh, B.K.; Ruzita, A.T. GReat-Child TrialTM based on social cognitive theory improved knowledge, attitudes and practices toward whole grains among Malaysian overweight and obese children. BMC Public Health 2019, 19, 1–13. [Google Scholar] [CrossRef]
- David, B.B.; Marianne, B.; Kathy, L.; Mary, K.B.; James, S.; Ilima, K.; Xia, L. Evaluation of immediate and 12-week effects of a smartphone sun-safety mobile application: A randomized trial. JAMA Derm. 2015, 151, 505–512. [Google Scholar] [CrossRef]
- Tang, Y.H.; Chong, M.C.; Chua, Y.P.; Chui, P.L.; Tang, L.Y.; Rahmat, N. The effect of mobile messaging apps on cardiac patient knowledge of coronary artery disease risk factors and adherence to a healthy lifestyle. J. Clin. Nurs. 2018, 27, 4311–4320. [Google Scholar] [CrossRef]
- Roberts, K.J.; McAdams, R.J.; Kristel, O.V.; Szymanski, A.M.; McKenzie, L.B. Qualitative and quantitative evaluation of the make safe happen app: Mobile technology–based safety behavior change intervention for parents. JMIR Pediatrics Parent. 2019, 2, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Tong, Y.; Chai, L.; Lei, S.; Liu, M.; Yang, L. Effects of Tai Chi on self-efficacy: A systematic review. Evid. Based Complementary Altern. Med. 2018, 2018, 1701372. [Google Scholar] [CrossRef] [Green Version]
- Goodman, S.; Morrongiello, B.; Meckling, K. A randomized, controlled trial evaluating the efficacy of an online intervention targeting vitamin D intake, knowledge and status among young adults. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Kuhn, E.; Kanuri, N.; Hoffman, J.E.; Garvert, D.W.; Ruzek, J.I.; Taylor, C.B. A randomized controlled trial of a smartphone app for posttraumatic stress disorder symptoms. J. Consult. Clin. Psychol. 2017, 85, 267–273. [Google Scholar] [CrossRef]
- Scheerman, J.F.M.; van Meijel, B.; van Empelen, P.; Verrips, E.H.W.; van Loveren, C.; Twisk, J.W.R.; Kramer, G.J.C. The effect of using a mobile application (‘WhiteTeeth’) on improving oral hygiene: A randomized controlled trial. Int. J. Dent. Hyg. 2019, 1–11. [Google Scholar] [CrossRef]
- Ul Haq, N.; Hassali, M.A.; Shafie, A.A.; Saleem, F.; Farooqui, M.; Aljadhey, H. A cross-sectional assessment of knowledge, attitude and practice towards Hepatitis B among healthy population of Quetta, Pakistan. BMC Public Health 2012, 12, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Osaili, T.M.; Obeidat, B.A.; Abu Jamous, D.O.; Bawadi, H.A. Food safety knowledge and practices among college female students in the north of Jordan. Food Control 2011, 22, 269–276. [Google Scholar] [CrossRef]
- Syahira, S.; Huda, B.Z.; Mohd Rafee, B.B. Factors associated with the level of food safety knowledge among form four students in Hulu Langat district, Selangor. Int. J. Public Health Clin. Sci. 2019, 6, 252–261. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.K.; Abdul Halim, H.; Thong, K.L.; Chai, L.C. Assessment of food safety knowledge, attitude, self-reported practices, and microbiological hand hygiene of food handlers. Int. J. Environ. Res. Public Health 2017, 14, 55. [Google Scholar] [CrossRef] [Green Version]
- Abdullahi, A.; Hassan, A.; Kadarman, N.; Saleh, A.; Baraya, Y.S.; Lua, P.L. Food safety knowledge, attitude, and practice toward compliance with abattoir laws among the abattoir workers in Malaysia. Int. J. Gen. Med. 2016, 9, 79–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dora-Liyana, A.L.; Mahyudin, N.A.; Ismail-Fitry, M.R.; Ahmad-Zaki, A.; Rasiyuddin, H. Food safety and hygiene knowledge, attitude and practices among food handlers at boarding schools in the northern region of Malaysia. Int. J. Acad. Res. Bus. Soc. Sci. 2018, 8, 238–266. [Google Scholar] [CrossRef]
- Norhaslinda, R.; Norhayati, A.; Mohd Adzim, K.R. Knowledge, attitudes and practices (KAP) on good manufacturing practices (GMP) among food handlers in Terengganu hospitals. Int. J. Pharm. Pharm. Sci. 2016, 8, 53–59. [Google Scholar] [CrossRef]
- Malhotra, R.; Lal, P.; Prakash, S.K.; Daga, M.K.; Kishore, J. Evaluation of a health education intervention on knowledge and attitudes of food handlers working in a medical college in Delhi, India. Asia Pac. J. Public Health 2008, 20, 277–286. [Google Scholar] [CrossRef]
- Mohd Firdaus, S.A.; Son, R.; Mohhiddin, O.; Toh, P.S.; Chai, L.C. Food court hygiene assessment and food safety knowledge, attitudes and practices of food handlers in Putrajaya. Int. Food Res. J. 2015, 22, 1843–1854. [Google Scholar]
- Shahar, S.; Vanoh, D.; Mat Ludin, A.F.; Singh, D.K.A.; Hamid, T.A. Factors associated with poor socioeconomic status among Malaysian older adults: An analysis according to urban and rural settings. BMC Public Health 2019, 19, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Nadiah, W.A.; Norsa, B.; Naing, N.N.; Abdullah, M.R. The effectiveness of health education package on knowledge, attitude and practice (KAP) of influenza A (H1N1) among school children in Malaysia. Int. Med. J. 2012, 19, 141–145. [Google Scholar]
- Fadda, M.; Galimberti, E.; Fiordelli, M.; Romanò, L.; Zanetti, A.; Schulz, P.J. Effectiveness of a smartphone app to increase parents’ knowledge and empowerment in the MMR vaccination decision: A randomized controlled trial. Hum. Vaccines Immunother. 2017, 13, 2512–2521. [Google Scholar] [CrossRef]
- Mummah, S.; Robinson, T.N.; Mathur, M.; Farzinkhou, S.; Sutton, S.; Gardner, C.D. Effect of a mobile app intervention on vegetable consumption in overweight adults: A randomized controlled trial. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Otu, A.; Ebenso, B.; Okuzu, O.; Osifo-Dawodu, E. Using a mHealth tutorial application to change knowledge and attitude of frontline health workers to Ebola virus disease in Nigeria: A before-and-after study. Hum. Resour. Health 2016, 14, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Fralick, M.; Haj, R.; Hirpara, D.; Wong, K.; Muller, M.; Matukas, L.; Taggart, L. Can a smartphone app improve medical trainees’ knowledge of antibiotics? Int. J. Med. Educ. 2017, 8, 416–420. [Google Scholar] [CrossRef] [Green Version]
- Bamgboje-Ayodele, A.; Ellis, L.; Turner, P. Safe food management and smartphone technology: Investigating the impact of an app on consumer knowledge retention. Online J. Public Health Inform. 2018, 10, 1–15. [Google Scholar] [CrossRef]
- Idris, N.A.; Zakaria, R.; Muhamad, R.; Husain, N.R.N.; Ishak, A.; Wan Mohammad, W.M.Z. The effectiveness of tuberculosis education programme in Kelantan, Malaysia on knowledge, attitude, practice and stigma towards tuberculosis among adolescents. Malays. J. Med. Sci. 2020, 27, 102–114. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Socio-Demographic Profile | Groups | |||
|---|---|---|---|---|
| Intervention (n = 50) | Control (n = 50) | |||
| n | % | n | % | |
| Gender | ||||
| Male | 21 | 42.0 | 15 | 30.0 |
| Female | 29 | 58.0 | 35 | 70.0 |
| Age group | ||||
| 18–20 years | 7 | 14.0 | 2 | 4.0 |
| 21–30 years | 17 | 34.0 | 10 | 20.0 |
| 31–40 years | 11 | 22.0 | 8 | 16.0 |
| 41–50 years | 3 | 6.0 | 17 | 34.0 |
| >50 years | 12 | 24.0 | 13 | 26.0 |
| Ethnicity | ||||
| Malay | 50 | 100.0 | 50 | 100.0 |
| Marital status | ||||
| Single | 18 | 36.0 | 7 | 14.0 |
| Married | 29 | 58.0 | 41 | 82.0 |
| Separated/divorced/widowed | 3 | 6.0 | 2 | 4.0 |
| Academic qualification | ||||
| Informal education | 0 | 0.0 | 1 | 2.0 |
| Primary school | 4 | 8.0 | 0 | 0.0 |
| Secondary school | 20 | 40.0 | 28 | 56.0 |
| Certificate/STPM/A level/GCE/ Foundation/matriculation/ diploma | 18 | 36.0 | 12 | 24.0 |
| Tertiary education (degree/master’s/ PhD) | 8 | 16.0 | 9 | 18.0 |
| Job sector | ||||
| Self-employed | 15 | 30.0 | 7 | 14.0 |
| Government sector | 10 | 20.0 | 2 | 4.0 |
| Private sector | 11 | 22.0 | 9 | 18.0 |
| Unemployed | 14 | 28.0 | 32 | 64.0 |
| Income level | ||||
| RM0–RM500 | 21 | 42.0 | 30 | 60.0 |
| RM501–RM1000 | 11 | 22.0 | 6 | 12.0 |
| RM1001–RM1500 | 10 | 20.0 | 5 | 10.0 |
| RM1501–RM2000 | 3 | 6.0 | 2 | 4.0 |
| >RM2000 | 5 | 10.0 | 7 | 14.0 |
| Variables | Intervention Group (n = 50) | Control Group (n = 50) | Z Statistics | p-Value |
|---|---|---|---|---|
| Median Score (IQR) | Median Score (IQR) | |||
| Knowledge | ||||
| Pre | 27.5 (10.0) | 30.0 (7.0) | −3.565 | 0.000 * |
| Post | 30.0 (8.0) | 31.0 (6.0) | −1.274 | 0.203 |
| Attitude | ||||
| Pre | 43.0 (7.0) | 46.0 (5.0) | −2.671 | 0.008 * |
| Post | 46.5 (6.0) | 46.0 (6.0) | −0.410 | 0.682 |
| Practice | ||||
| Pre | 33.0 (6.0) | 34.0 (3.0) | −2.571 | 0.010 * |
| Post | 35.0 (5.0) | 36.0 (8.0) | −0.964 | 0.335 |
| Perceived barrier | ||||
| Pre | 9.0 (3.0) | 9.5 (3.0) | −0.805 | 0.421 |
| Post | 10.0 (6.0) | 10.0 (4.0) | −0.076 | 0.939 |
| Perceived susceptibility | ||||
| Pre | 8.0 (2.0) | 8.0 (2.0) | −0.056 | 0.955 |
| Post | 10.0 (2.0) | 10.0 (2.0) | −0.294 | 0.768 |
| Variables | Intervention Group (n = 50) | Control Group (n = 50) | ||||
|---|---|---|---|---|---|---|
| Pre | Post | p-Value | Pre | Post | p-Value | |
| Median Score (IQR) | Median Score (IQR) | Median Score (IQR) | Median Score (IQR) | |||
| Knowledge | 27.5 (10.0) | 30.0 (8.0) | 0.000 * | 30.0 (7.0) | 31.0 (6.0) | 0.324 |
| Variables | Intervention Group (n = 50) | Control Group (n = 50) | ||||
|---|---|---|---|---|---|---|
| Pre | Post | p-Value | Pre | Post | p-Value | |
| Median Score (IQR) | Median Score (IQR) | Median Score (IQR) | Median Score (IQR) | |||
| Attitude | 43.0 (7.0) | 46.5 (6.0) | 0.001 * | 46.0 (5.0) | 46.0 (6.0) | 0.490 |
| Variables | Intervention Group (n = 50) | Control Group (n = 50) | ||||
|---|---|---|---|---|---|---|
| Pre | Post | p-Value | Pre | Post | p-Value | |
| Median Score (IQR) | Median Score (IQR) | Median Score (IQR) | Median Score (IQR) | |||
| Practice | 33.0 (6.0) | 35.0 (5.0) | 0.000 * | 34.0 (3.0) | 36.0 (8.0) | 0.131 |
| Variables | Intervention Group (n = 50) | Control Group (n = 50) | ||||
|---|---|---|---|---|---|---|
| Pre | Post | p-Value | Pre | Post | p-Value | |
| Median Score (IQR) | Median Score (IQR) | Median Score (IQR) | Median Score (IQR) | |||
| Perceived barrier | 9.0 (3.0) | 10.0 (6.0) | 0.129 | 9.50 (3.0) | 10.0 (4.0) | 0.422 |
| Perceived susceptibility | 8.0 (2.0) | 10.0 (2.0) | 0.069 | 8.0 (2.0) | 10.0 (2.0) | 0.012 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zaujan, N.A.M.; Ali, A.; Osman, M.; Chee, H.Y.; Ithnin, N.R.; Misni, N.; Sukeri, S.; Chin, C.P.-Y. Effect of Smartphone App’s Intervention on Consumers’ Knowledge, Attitude, Practice, and Perception of Food Poisoning Prevention When Dining Out at Selected Rural Areas in Terengganu. Int. J. Environ. Res. Public Health 2021, 18, 10294. https://doi.org/10.3390/ijerph181910294
Zaujan NAM, Ali A, Osman M, Chee HY, Ithnin NR, Misni N, Sukeri S, Chin CP-Y. Effect of Smartphone App’s Intervention on Consumers’ Knowledge, Attitude, Practice, and Perception of Food Poisoning Prevention When Dining Out at Selected Rural Areas in Terengganu. International Journal of Environmental Research and Public Health. 2021; 18(19):10294. https://doi.org/10.3390/ijerph181910294
Chicago/Turabian StyleZaujan, Nur Afifah Mursyida, Asma’ Ali, Malina Osman, Hui Yee Chee, Nur Raihana Ithnin, Norashiqin Misni, Surianti Sukeri, and Christie Pei-Yee Chin. 2021. "Effect of Smartphone App’s Intervention on Consumers’ Knowledge, Attitude, Practice, and Perception of Food Poisoning Prevention When Dining Out at Selected Rural Areas in Terengganu" International Journal of Environmental Research and Public Health 18, no. 19: 10294. https://doi.org/10.3390/ijerph181910294