
Effectiveness of National Residential Smoking Cessation Program

 , , ,
, , ,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
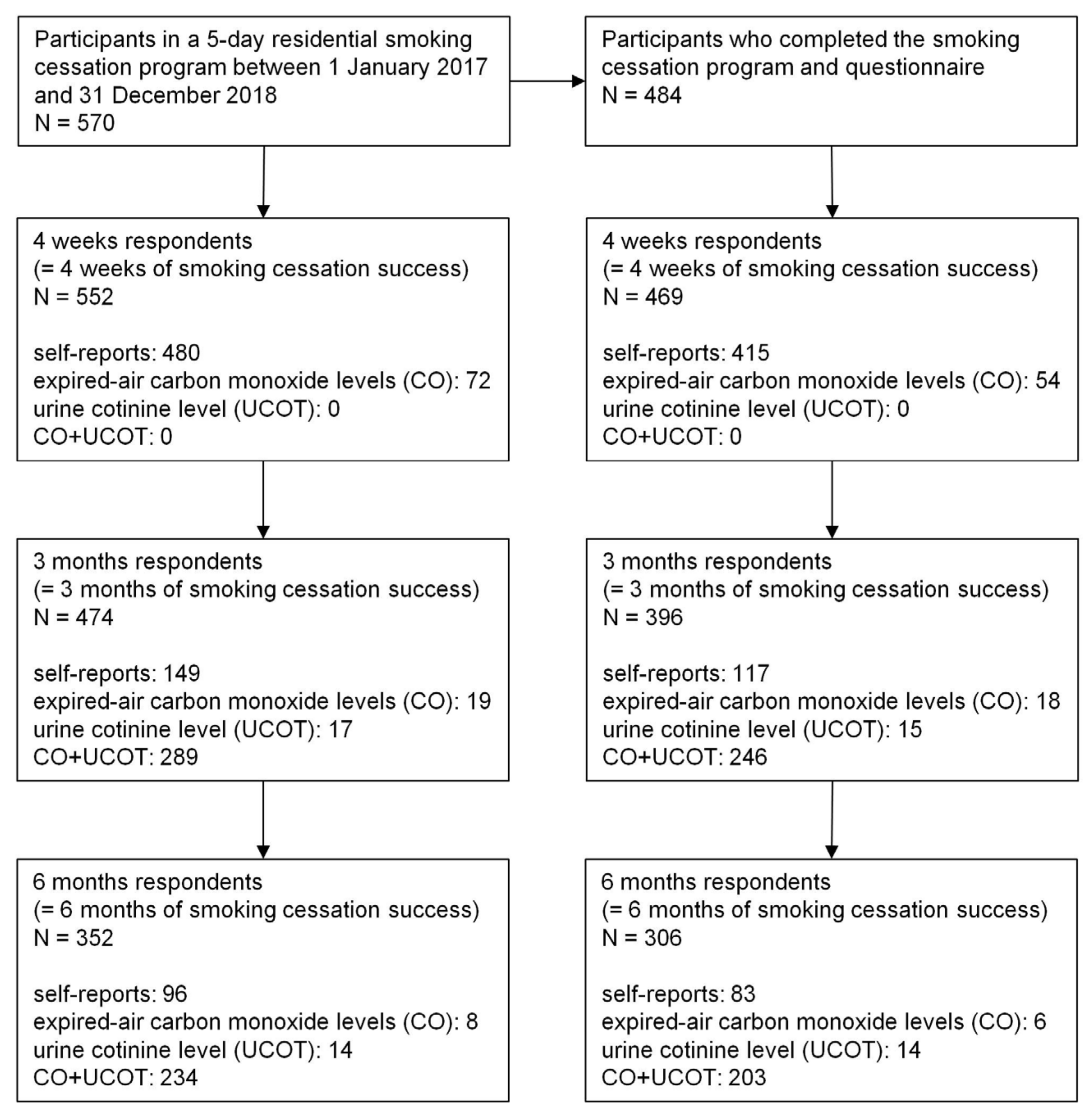
2.1. Study Design and Participants
2.2. Measurements
2.3. Intervention
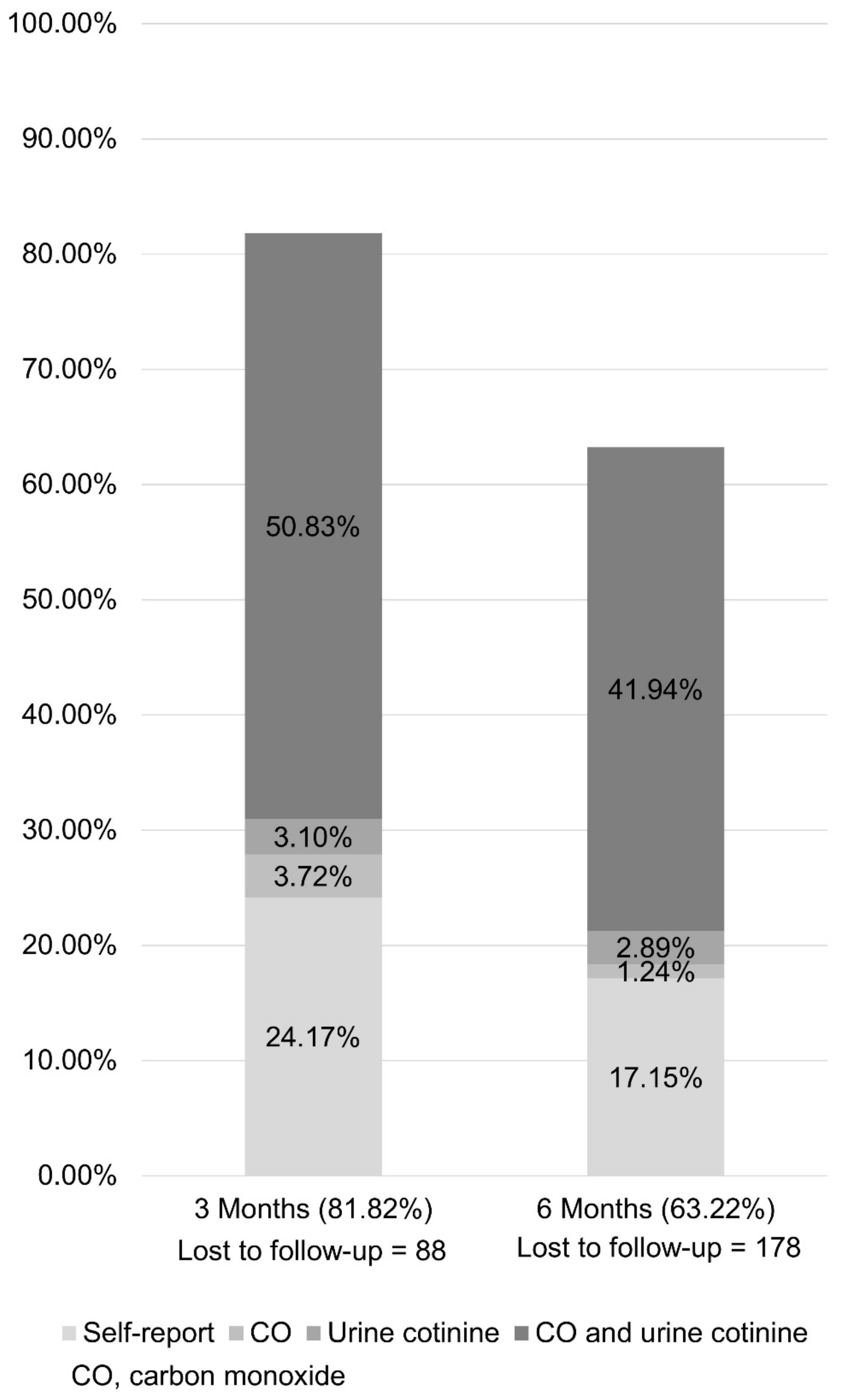
2.4. Follow-Up
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Patanavanich, R.; Glantz, S.A. Smoking Is Associated with COVID-19 Progression: A Meta-analysis. Nicotine Tob. Res. 2020, 22, 1653–1656. [Google Scholar] [CrossRef] [PubMed]
- Besaratinia, A. COVID-19: A pandemic converged with global tobacco epidemic and widespread vaping-state of the evidence. Carcinogenesis 2021, 42, 1009–1022. [Google Scholar] [CrossRef]
- National Center for Chronic Disease Prevention and Health Promotion (US) Office on Smoking and Health. The Health Consequences of Smoking—50 Years of Progress: A Report of the Surgeon General; Centers for Disease Control and Prevention (US): Atlanta, GA, USA, 2014. [Google Scholar]
- Carter, B.D.; Abnet, C.C.; Feskanich, D.; Freedman, N.D.; Hartge, P.; Lewis, C.E.; Ockene, J.K.; Prentice, R.L.; Speizer, F.E.; Thun, M.J.; et al. Smoking and mortality--beyond established causes. N. Engl. J. Med. 2015, 372, 631–640. [Google Scholar] [CrossRef] [Green Version]
- WHO Global Report on Trends in Prevalence of Tobacco Use 2000–2025, 3rd ed.; World Health Organization: Geneva, Switzerland, 2019; Available online: https://apps.who.int/iris/rest/bitstreams/1263754/retrieve (accessed on 1 August 2021).
- U.S. Department of Health and Human Services. How Tobacco Smoke Causes Disease: The Biology and Behavioral Basis for Smoking-Attributable Disease: A Report of the Surgeon General; U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health: Atlanta, GA, USA, 2010. [Google Scholar]
- Hughes, J.R.; Keely, J.; Naud, S. Shape of the relapse curve and long-term abstinence among untreated smokers. Addiction 2004, 99, 29–38. [Google Scholar] [CrossRef]
- Cahill, K.; Stevens, S.; Perera, R.; Lancaster, T. Pharmacological interventions for smoking cessation: An overview and network meta-analysis. Cochrane Database Syst Rev. 2013, 2013, CD009329. [Google Scholar] [CrossRef] [PubMed]
- Lancaster, T.; Stead, L.F. Individual behavioural counselling for smoking cessation. Cochrane Database Syst. Rev. 2017, 3, CD001292. [Google Scholar] [CrossRef] [PubMed]
- Stead, L.F.; Bergson, G.; Lancaster, T. Physician advice for smoking cessation. Cochrane Database Syst. Rev. 2008, 2, CD000165. [Google Scholar] [CrossRef] [Green Version]
- Lancaster, T.; Hajek, P.; Stead, L.F.; West, R.; Jarvis, M.J. Prevention of relapse after quitting smoking: A systematic review of trials. Arch. Intern. Med. 2006, 166, 828–835. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hurt, R.D.; Dale, L.C.; Offord, K.P.; Bruce, B.K.; McCLAIN, F.L.; Eberman, K.M. Inpatient treatment of severe nicotine dependence. Mayo Clin. Proc. 1992, 67, 823–828. [Google Scholar] [CrossRef]
- Hays, J.T.; Croghan, I.T.; Schroeder, D.R.; Burke, M.V.; Ebbert, J.O.; McFadden, D.D.; Hurt, R.D. Residential treatment compared with outpatient treatment for tobacco use and dependence. Mayo Clin. Proc. 2011, 86, 203–209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Korea Disease Control and Prevention Agency. Korea National Health and Nutrition Examination Survey: Current Smoking Rate Trend, 1998–2019. Available online: https://kosis.kr/statHtml/statHtml.do?orgId=177&tblId=DT_11702_N001&conn_path=I2 (accessed on 1 August 2021).
- OECD. Health at a Glance 2019: OECD Indicators; OECD Publishing: Paris, France, 2019. [Google Scholar]
- Cho, M.J.; Kim, K.H. Use of the Center for Epidemiologic Studies Depression (CES-D) Scale in Korea. J. Nerv. Ment. Dis. 1998, 186, 304–310. [Google Scholar] [CrossRef] [PubMed]
- Cho, M.J.; Kim, K.H. Diagnostic validity of the CES-D(Korean version) in the assessment of DSM-III-R major depression. J. Korean Neuropsychiatr. Assoc. 1993, 32, 381–399. [Google Scholar]
- Williams, G.C.; Gagné, M.; Ryan, R.M.; Deci, E.L. Facilitating autonomous motivation for smoking cessation. Health Psychol. 2002, 21, 40–50. [Google Scholar] [CrossRef]
- Velicer, W.F.; Diclemente, C.C.; Rossi, J.S.; Prochaska, J.O. Relapse situations and self-efficacy: An integrative model. Addict. Behav. 1990, 15, 271–283. [Google Scholar] [CrossRef]
- Kim, M.S.; Kwon, J.H. The Outcome study of cognitive behavioral and behavioral smoking abstinence program for Korean nicotine dependent adolescents. Korean J. Clin. Psychol. 2006, 25, 1–23. [Google Scholar]
- Green, A.; Yancy, W.S.; Braxton, L.; Westman, E.C. Residential smoking therapy. J. Gen. Intern. Med. 2003, 18, 275–280. [Google Scholar] [CrossRef] [Green Version]
- Ho, R.K.S.; Fok, P.W.Y.; Chan, H.C.H. Pilot study of a 3-day residential treatment for smoking cessation in Hong Kong. Tob. Prev. Cessat. 2018, 4, 40. [Google Scholar] [CrossRef]
- Seo, Y.G.; Paek, Y.J.; Jo, M.W.; Choi, J. Predictors of long-term abstinence rate by income level in the Korean smoking cessation programme. Addiction 2019, 114, 2056–2064. [Google Scholar] [CrossRef]
- Benowitz, N.L. Nicotine addiction. N. Engl. J. Med. 2010, 362, 2295–2303. [Google Scholar] [CrossRef]
- Caponnetto, P.; Polosa, R. Common predictors of smoking cessation in clinical practice. Respir. Med. 2008, 102, 1182–1192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fagerström, K.; Russ, C.; Yu, C.R.; Yunis, C.; Foulds, J. he Fagerström Test for Nicotine Dependence as a predictor of smoking abstinence: A pooled analysis of varenicline clinical trial data. Nicotine Tob. Res. 2012, 14, 1467–1473. [Google Scholar] [CrossRef]
- Gwaltney, C.J.; Metrik, J.; Kahler, C.W.; Shiffman, S. Self-efficacy and smoking cessation: A meta-analysis. Psychol. Addict. Behav. 2009, 23, 56–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gwaltney, C.J.; Shiffman, S.; Balabanis, M.H.; Paty, J.A. Dynamic self-efficacy and outcome expectancies: Prediction of smoking lapse and relapse. J. Abnorm. Psychol. 2005, 114, 661–675. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Fang, L.; Zhou, Y.; Pan, L.; Yang, X.; Li, H.; Wang, Q.; Jiang, F.; Zhang, N.; Han, M.; et al. Mediation of smoking abstinence self-efficacy on the association of nicotine dependence with smoking cessation. Eur. J. Public Health 2015, 25, 200–204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taniguchi, C.; Tanaka, H.; Saka, H.; Oze, I.; Tachibana, K.; Nozaki, Y.; Suzuki, Y.; Sakakibara, H. Changes in self-efficacy associated with success in quitting smoking in participants in Japanese smoking cessation therapy. Int. J. Nurs Pract. 2018, 24, e12647. [Google Scholar] [CrossRef]
- Chang, P.-H.; Chiang, C.-H.; Ho, W.-C.; Wu, P.-Z.; Tsai, J.-S.; Guo, F.-R. Combination therapy of varenicline with nicotine replacement therapy is better than varenicline alone: A systematic review and meta-analysis of randomized controlled trials. BMC Public Health 2015, 15, 689. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holm, M.; Schiöler, L.; Andersson, E.; Forsberg, B.; Gislason, T.; Janson, C.; Jogi, R.; Schlunssen, V.; Svanes, C.; Torén, K. Predictors of smoking cessation: A longitudinal study in a large cohort of smokers. Respir. Med. 2017, 132, 164–169. [Google Scholar] [CrossRef] [Green Version]
- Lynch, K.L.; Twesten, J.E.; Stern, A.; Augustson, E.M. Level of Alcohol Consumption and Successful Smoking Cessation. Nicotine Tob. Res. 2019, 21, 1058–1064. [Google Scholar] [CrossRef] [PubMed]
- Rice, V.H.; Templin, T.; Fox, D.H.; Jarosz, P.; Mullin, M.; Seiggreen, M.; Lepczyk, M. Social context variables as predictors of smoking cessation. Tob. Control. 1996, 5, 280–285. [Google Scholar] [CrossRef]
- Hughes, J.R.; Keely, J.P.; Niaura, R.S.; Ossip-Klein, D.J.; Richmond, R.L.; Swan, G.E. Measures of abstinence in clinical trials: Issues and recommendations. Nicotine Tob. Res. 2003, 5, 13–25. [Google Scholar] [CrossRef]
- Shie, H.G.; Pan, S.W.; Yu, W.K.; Chen, W.C.; Ho, L.I.; Ko, H.K. Levels of exhaled carbon monoxide measured during an intervention program predict 1-year smoking cessation: A retrospective observational cohort study. NPJ Prim. Care Respir. Med. 2017, 27, 59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stepankova, L.; Kralikova, E.; Zvolská, K.; Pánková, A.; Ovesna, P.; Blaha, M.; Brose, L.S. Depression and Smoking Cessation: Evidence from a Smoking Cessation Clinic with 1-Year Follow-Up. Ann. Behav. Med. 2017, 51, 454–463. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, D.; Lee, Y.R.; Oh, I.H. Cost-effectiveness of smoking cessation programs for hospitalized patients: A systematic review. Eur. J. Health Econ. 2019, 20, 1409–1424. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Day 1 | Day 2 | Day 3 | Day 4 | Day 5 | |
|---|---|---|---|---|---|
| 08:00 | CO a testing | Breakfast and CO testing | |||
| 09:00 | Health Check-up (Lab, Chest CT b, Carotid Sono, PFT c, UA d) | Individual counseling <Psychological counseling> | Individual counseling <The result of Health Check-up> | Final individual counseling | |
| 10:30 | Group Exercise | Recreational session | Closing ceremony | ||
| 12:00 | Lunch | ||||
| 13:30 | Group session <Mindfulness> | Group session <Psychological counseling> | Group Exercise | ||
| 14:00 | Welcoming Ceremony | ||||
| 15:00 | Psychological assessment | Group session <Behavioral therapy> | Group Exercise | Group session <Behavioral therapy> | |
| 16:00 | Group session <Pharmacotherapy> | ||||
| 17:00 | Physician Rounding (Medical counseling and prescription of medications) | ||||
| 18:00 | Dinner | ||||
| 19:00 | Group session <Psychological counseling> | Lecture <Cardiovascular disease and Smoking> | Nutrition management after smoking cessation | Drama therapy | |
| Follow-Up | 4 Weeks | 3 Months | 6 Months | |||
|---|---|---|---|---|---|---|
| Success | Fail | Success | Fail | Success | Fail | |
| Number (%) | 552 (96.84) | 18 (3.16) | 474 (83.16) | 96 (16.84) | 352 (61.75) | 218 (38.25) |
| Follow-Up | 4 Weeks | 3 Months | 6 Months | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Success | Fail | Success | Fail | Success | Fail | ||||
| 469 (96.90) | 15 (3.10) | p-Value | 396 (81.82) | 88 (18.18) | p-value | 306 (63.22) | 178 (36.78) | p-Value | |
| Age (yr, mean ± SD) | 55.41 ± 10.63 | 52.53 ± 13.75 | 0.31 | 55.85 ± 10.49 | 52.91 ± 11.56 | 0.02 | 55.89 ± 10.20 | 54.34 ± 11.56 | 0.13 |
| Gender | 0.40 | 0.03 | 0.26 | ||||||
| M | 414 (88.27) | 15 (100.00) | 357 (90.15) | 72 (81.82) | 275 (89.87) | 154 (86.52) | |||
| F | 55 (11.73) | 0 (0.00) | 39 (9.85) | 16 (18.18) | 31 (10.13) | 24 (13.48) | |||
| Education level (9 data missing) | 0.39 | 0.30 | 0.17 | ||||||
| Middle school or less | 51 (11.09) | 3 (20.00) | 40 (10.31) | 14 (16.09) | 28 (9.30) | 26 (14.94) | |||
| High school | 155 (33.70) | 3 (20.00) | 130 (33.51) | 28 (32.18) | 101 (33.55) | 57 (32.76) | |||
| College or beyond | 254 (55.22) | 9 (60.00) | 218 (56.19) | 45 (51.72) | 172 (57.14) | 91 (52.30) | |||
| Alcohol | 0.98 | 0.56 | 0.31 | ||||||
| Yes | 158 (33.69) | 5 (33.33) | 131 (33.08) | 32 (36.36) | 98 (32.03) | 65 (36.52) | |||
| Regular exercise | 0.40 | 0.24 | 0.11 | ||||||
| Yes | 140 (29.85) | 6 (40.00) | 124 (31.31) | 22 (25.00) | 100 (32.68) | 46 (25.84) | |||
| Hypertension | 138 (29.42) | 1 (6.67) | 0.08 | 111 (28.03) | 28 (31.82) | 0.48 | 86 (28.10) | 53 (29.78) | 0.70 |
| Diabetes | 89 (18.98) | 3 (20.00) | 0.92 | 77 (19.44) | 15 (17.05) | 0.60 | 63 (20.59) | 29 (16.29) | 0.25 |
| Dyslipidemia | 73 (15.57) | 4 (26.67) | 0.25 | 61 (15.40) | 16 (18.18) | 0.52 | 50 (16.34) | 27 (15.17) | 0.73 |
| Any supporters | 0.19 | 0.20 | 0.23 | ||||||
| Yes | 401 (85.50) | 11 (73.33) | 341 (86.11) | 71 (80.68) | 265 (86.60) | 147 (82.58) | |||
| Smoking | |||||||||
| Age of smoking initiation (yr, mean ± SD) | 20.61 ± 4.77 | 18.53 ± 3.25 | 0.10 | 20.68 ± 4.65 | 19.93 ± 5.12 | 0.18 | 20.73 ± 4.66 | 20.23 ± 4.89 | 0.27 |
| Smoking duration (yr, mean ± SD) | 36.20 ± 10.31 | 35.40 ± 12.74 | 0.77 | 36.57 ± 10.28 | 34.40 ± 10.69 | 0.08 | 36.58 ± 9.97 | 35.48 ± 11.05 | 0.26 |
| Cigarettes per day (N, mean ± SD) | 20.69 ± 8.15 | 25.33 ± 10.93 | 0.03 | 20.33 ± 7.46 | 23.07 ± 11.00 | 0.005 | 20.05 ± 7.52 | 22.17 ± 9.30 | 0.006 |
| FTND a score | 0.03 | <0.001 | <0.001 | ||||||
| Mild (1–3) | 154 (32.84) | 2 (13.33) | 140 (35.35) | 16 (18.18) | 118 (38.56) | 38 (21.35) | |||
| Moderate (4–6) | 202 (43.07) | 5 (33.33) | 171 (43.18) | 36 (40.91) | 121 (39.54) | 86 (48.31) | |||
| Severe (7–10) | 113 (24.09) | 8 (53.33) | 85 (21.46) | 36 (40.91) | 67 (21.90) | 54 (30.34) | |||
| Quit attempt in the past year | 0.28 | 0.35 | 0.51 | ||||||
| Yes | 172 (36.67) | 3 (20.00) | 147 (37.12) | 28 (31.82) | 114 (37.25) | 61 (34.27) | |||
| Pharmacotherapy | <0.001 | <0.001 | 0.12 | ||||||
| No | 12 (2.56) | 1 (6.67) | 9 (2.27) | 4 (4.55) | 8 (2.61) | 5 (2.81) | |||
| NRT b | 158 (33.69) | 8 (53.33) | 126 (31.82) | 40 (45.45) | 96 (31.37) | 70 (39.33) | |||
| Varenicline | 11 (2.35) | 4 (26.67) | 8 (2.02) | 7 (7.95) | 7 (2.29) | 8 (4.49) | |||
| Varenicline + short-term NRT | 288 (61.41) | 2 (13.33) | 253 (63.89) | 37 (42.05) | 195 (63.73) | 95 (53.37) | |||
| Psychological | |||||||||
| IRC c rulers (mean ± SD) | |||||||||
| Importance | 9.04 ± 1.60 | 9.13 ± 1.25 | 0.82 | 9.03 ± 1.63 | 9.10 ± 1.41 | 0.68 | 9.04 ± 1.60 | 9.03 ± 1.58 | 0.95 |
| Readiness | 8.26 ± 2.09 | 7.53 ± 1.96 | 0.18 | 8.31 ± 2.05 | 7.93 ± 2.24 | 0.12 | 8.25 ± 2.13 | 8.23 ± 2.01 | 0.93 |
| Confidence | 7.67 ± 2.17 | 7.07 ± 2.15 | 0.29 | 7.75 ± 2.13 | 7.17 ± 2.27 | 0.02 | 7.80 ± 2.10 | 7.38 ± 2.27 | 0.04 |
| Depression scale (CES-D d, 3 data missing) | 0.08 | 0.002 | 0.37 | ||||||
| Normal and Mild depressive symptoms (≤15) | 246 (52.79) | 5 (33.33) | 219 (55.58) | 32 (36.78) | 166 (54.61) | 85 (48.02) | |||
| Moderate depressive symptoms (16~24) | 117 (25.11) | 3 (20.00) | 96 (24.37) | 24 (27.59) | 73 (24.01) | 47 (26.55) | |||
| Severe depressive symptoms (≥25) | 103 (22.10) | 7 (46.67) | 79 (20.05) | 31 (35.63) | 65 (21.38) | 45 (25.42) | |||
| Craving score (TCQ e, mean ± SD) | 140.18 ± 40.80 | 169.14 ± 49.99 | 0.01 | 138.99 ± 40.92 | 150.52 ± 42.26 | 0.02 | 140.27 ± 41.73 | 142.54 ± 40.80 | 0.58 |
| Self-efficacy scale (mean ± SD) | 26.04 ± 6.71 | 25.07 ± 7.54 | 0.58 | 26.34 ± 6.68 | 24.55 ± 6.81 | 0.02 | 26.88 ± 6.63 | 24.52 ± 6.67 | <0.001 |
| Model 1 a | Model 2 b | Model 3 c | ||||
|---|---|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| Age (yr, mean ± SD) | 1.03s (1.00–1.05) | 0.02 | 1.03 (1.00–1.05) | 0.02 | 1.03 (1.00–1.06) | 0.02 |
| Gender | ||||||
| M | 1 | 1 | 1 | |||
| F | 0.49 (0.26–0.93) | 0.03 | 0.49 (0.26–0.93) | 0.03 | 0.61 (0.30–1.24) | 0.17 |
| Education level (9 data missing) | ||||||
| Middle school or less | 1 | 1 | 1 | |||
| High school | 1.63 (0.78–3.38) | 0.19 | 2.24 (0.97–5.15) | 0.06 | 1.44 (0.60–3.43) | 0.41 |
| College or beyond | 1.70 (0.85–3.37) | 0.13 | 2.49 (1.09–5.68) | 0.03 | 1.53 (0.64–3.62) | 0.34 |
| FTND d score | ||||||
| Mild (1–3) | 1 | 1 | 1 | |||
| Moderate (4–6) | 0.54 (0.29–1.02) | 0.06 | 0.56 (0.30–1.07) | 0.08 | 0.52 (0.26–1.02) | 0.06 |
| Severe (7–10) | 0.27 (0.14–0.52) | <0.001 | 0.29 (0.15–0.57) | <0.001 | 0.28 (0.14–0.59) | 0.001 |
| Pharmacotherapy | ||||||
| NRT e | 1 | 1 | 1 | |||
| No | 0.71 (0.21–2.44) | 0.59 | 0.67 (0.19–2.31) | 0.52 | 0.80 (0.19–3.36) | 0.76 |
| Varenicline | 0.36 (0.12–1.06) | 0.07 | 0.36 (0.12–1.07) | 0.07 | 0.39 (0.23–1.26) | 0.12 |
| Varenicline + short-term NRT | 2.17 (1.32–3.56) | 0.002 | 2.18 (1.32–3.61) | 0.002 | 2.13 (1.25–3.63) | 0.006 |
| Depression scale (CES-D f) | ||||||
| Normal and Mild depressive symptoms (≤15) | 1 | 1 | 1 | |||
| Moderate depressive symptoms (16~24) | 0.58 (0.33–1.05) | 0.07 | 0.54 (0.30–0.98) | 0.04 | 0.60 (0.32–1.13) | 0.12 |
| Severe depressive symptoms (≥25) | 0.37 (0.21–0.65) | 0.001 | 0.36 (0.20–0.65) | 0.001 | 0.48 (0.25–0.91) | 0.03 |
| Self-efficacy scale (tertile) | ||||||
| low | 1 | 1 | 1 | |||
| moderate | 1.17 (0.69–1.99) | 0.57 | 0.98 (0.56–1.70) | 0.93 | 0.80 (0.43–1.50) | 0.48 |
| high | 1.61 (0.89–2.91) | 0.12 | 1.38 (0.75–2.53) | 0.30 | 0.92 (0.46–1.85) | 0.82 |
| Model 1 a | Model 2 b | Model 3 c | ||||
|---|---|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| Age (yr, mean ± SD) | 1.01 (1.00–1.03) | 0.13 | 1.01 (1.00–1.03) | 0.13 | 1.01 (0.99–1.03) | 0.26 |
| Gender | ||||||
| M | 1 | 1 | 1 | |||
| F | 0.72 (0.41–1.28) | 0.26 | 0.72 (0.41–1.28) | 0.27 | 0.85 (0.46–1.59) | 0.61 |
| Education level (9 data missing) | ||||||
| Middle school or less | 1 | 1 | 1 | |||
| High school | 1.65 (0.88–3.07) | 0.12 | 2.04 (1.03–4.04) | 0.04 | 1.89 (0.91–3.89) | 0.09 |
| College or beyond | 1.76 (0.97–3.17) | 0.06 | 2.27 (1.15–4.46) | 0.02 | 1.90 (0.93–3.89) | 0.08 |
| FTND d score | ||||||
| Mild (1–3) | 1 | 1 | 1 | |||
| Moderate (4–6) | 0.45 (0.29–0.72) | 0.001 | 0.46 (0.29–0.73) | 0.001 | 0.46 (0.28–0.75) | 0.002 |
| Severe (7–10) | 0.40 (0.24–0.67) | <0.001 | 0.42 (0.25–0.70) | 0.001 | 0.46 (0.26–0.81) | 0.01 |
| Pharmacotherapy | ||||||
| NRT e | 1 | 1 | 1 | |||
| No | 1.17 (0.37–3.72) | 0.79 | 1.13 (0.35–3.63) | 0.83 | 1.09 (0.29–4.03) | 0.90 |
| Varenicline | 0.64 (0.22–1.84) | 0.41 | 0.65 (0.22–1.89) | 0.43 | 0.67 (0.22–2.03) | 0.48 |
| Varenicline + short-term NRT | 1.50 (1.01–2.22) | 0.05 | 1.49 (1.00–2.21) | 0.05 | 1.64 (1.07–2.51) | 0.02 |
| Depression scale (CES-D f) | ||||||
| Normal and Mild depressive symptoms (≤15) | 1 | 1 | 1 | |||
| Moderate depressive symptoms (16~24) | 0.80 (0.51–1.25) | 0.32 | 0.76 (0.48–1.20) | 0.24 | 0.86 (0.53–1.40) | 0.55 |
| Severe depressive symptoms (≥25) | 0.74 (0.47–1.17) | 0.20 | 0.73 (0.45–1.17) | 0.19 | 1.03 (0.61–1.76) | 0.90 |
| Self-efficacy scale (tertile) | ||||||
| low | 1 | 1 | 1 | |||
| moderate | 1.10 (0.72–1.69) | 0.66 | 1.03 (0.66–1.59) | 0.91 | 0.95 (0.59–1.54) | 0.85 |
| high | 2.38 (1.47–3.87) | <0.001 | 2.24 (1.37–3.68) | 0.001 | 1.97 (1.15–3.37) | 0.01 |
| 3 Months Model 3 a | 6 Months Model 3 a | |||
|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| Age (yr, mean ± SD) | 1.03 (1.00–1.06) | 0.04 | 1.01 (0.99–1.04) | 0.23 |
| Gender | ||||
| M | 1 | 1 | ||
| F | 0.57 (0.28–1.18) | 0.13 | 0.81 (0.43–1.52) | 0.51 |
| Education level (9 data missing) | ||||
| Middle school or less | 1 | 1 | ||
| High school | 1.54 (0.62–3.82) | 0.36 | 1.85 (0.88–3.91) | 0.11 |
| College or beyond | 1.49 (0.60–3.69) | 0.39 | 1.79 (0.85–3.74) | 0.12 |
| FTND b score | ||||
| Mild (1–3) | 1 | 1 | ||
| Moderate (4–6) | 0.50 (0.25–1.02) | 0.06 | 0.46 (0.28–0.76) | 0.002 |
| Severe (7–10) | 0.33 (0.15–0.71) | 0.005 | 0.52 (0.29–0.93) | 0.03 |
| Pharmacotherapy | ||||
| NRT c | 1 | 1 | ||
| Varenicline + short-term NRT | 2.12 (1.24–3.61) | 0.006 | 1.63 (1.07–2.49) | 0.02 |
| Depression scale (CES-D d) | ||||
| Normal and Mild depressive symptoms (≤15) | 1 | 1 | ||
| Moderate depressive symptoms (16~24) | 0.55 (0.29–1.06) | 0.07 | 0.80 (0.49–1.31) | 0.37 |
| Severe depressive symptoms (≥25) | 0.44 (0.23–0.88) | 0.02 | 0.97 (0.56–1.68) | 0.92 |
| Self-efficacy scale (tertile) | ||||
| low | 1 | 1 | ||
| moderate | 0.74 (0.39–1.42) | 0.37 | 0.93 (0.57–1.53) | 0.79 |
| high | 0.79 (0.39–1.62) | 0.53 | 1.75 (1.01–3.03) | 0.04 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, M.-J.; Seo, Y.-G.; Noh, H.-M.; Kim, Y.; Yoon, J.L.; Paek, Y.-J. Effectiveness of National Residential Smoking Cessation Program. Int. J. Environ. Res. Public Health 2021, 18, 9901. https://doi.org/10.3390/ijerph18189901
Park M-J, Seo Y-G, Noh H-M, Kim Y, Yoon JL, Paek Y-J. Effectiveness of National Residential Smoking Cessation Program. International Journal of Environmental Research and Public Health. 2021; 18(18):9901. https://doi.org/10.3390/ijerph18189901
Chicago/Turabian StylePark, Mi-Jeong, Young-Gyun Seo, Hye-Mi Noh, Yeol Kim, Jong Lull Yoon, and Yu-Jin Paek. 2021. "Effectiveness of National Residential Smoking Cessation Program" International Journal of Environmental Research and Public Health 18, no. 18: 9901. https://doi.org/10.3390/ijerph18189901