
The Effect of a Brief, Web-Based Animated Video for Improving Comprehension and Implementation Feasibility for Reducing Anterior Cruciate Ligament Injury: A Three-Arm Randomized Controlled Trial

Abstract
:1. Introduction
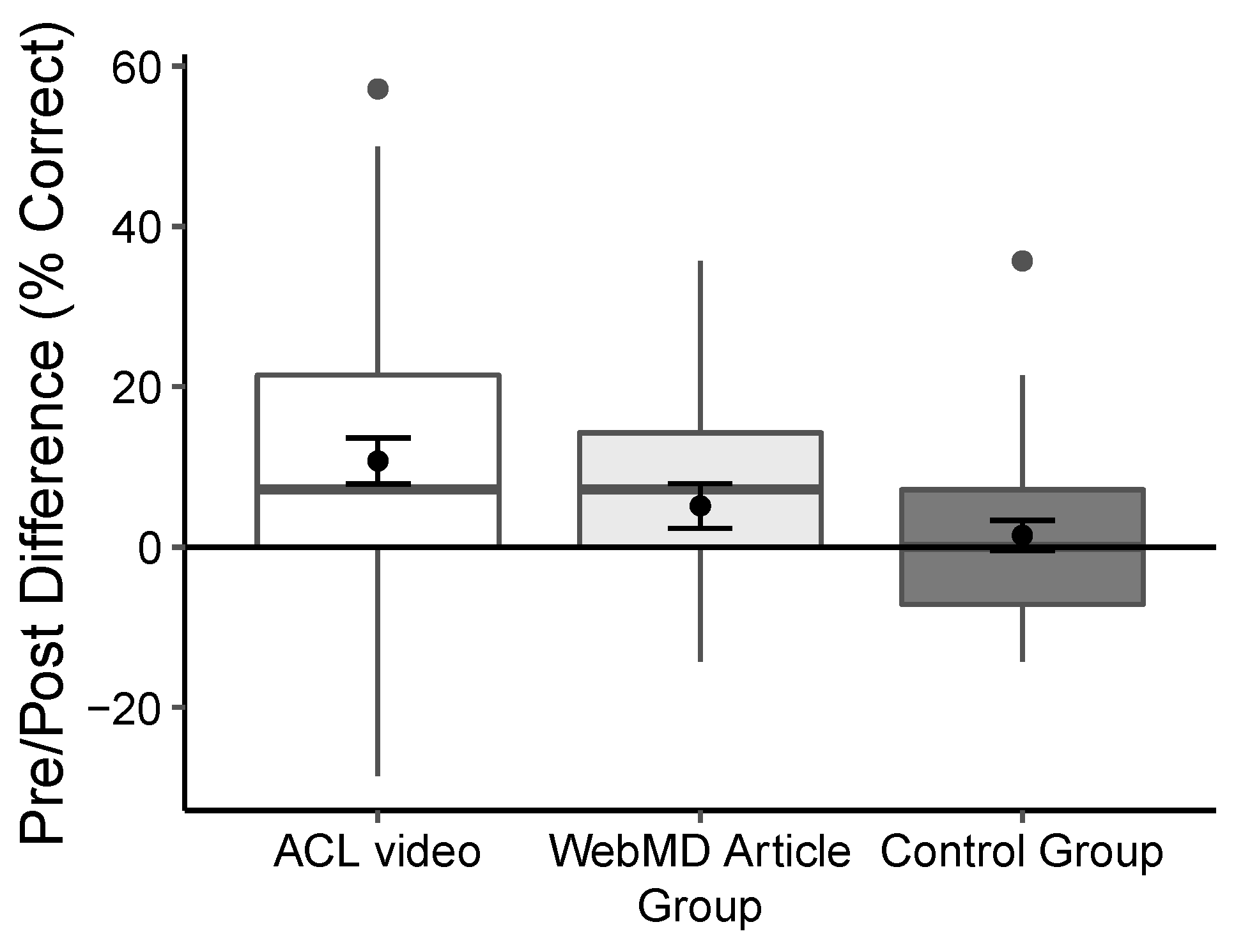
- Overall comprehension of ACL injury risk and mitigation: placebo control group < active control group < intervention group.
- Feasibility of utilizing ACL injury prevention strategies: placebo control group < active control group < intervention group.
2. Materials and Methods
2.1. Trial Design
2.2. Procedure
2.3. Participants
2.4. Intervention
2.5. Outcome Measures
2.6. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
Appendix B
- Shoulder
- Pelvis
- Ankle
- Hip
- Knee
- Anterior Condyle Ligament
- Anterior Cruciate Ligament
- Anatomical Cruciate Ligament
- Anterior Collateral Ligament
- Anatomical Collateral Ligament
- Hockey
- Soccer
- Weightlifting
- Running
- Volleyball
- 1 in 2 (50%)
- 1 in 10 (10%)
- 1 in 20 (5%)
- 1 in 100 (1%)
- 1 in 300 (0.33%)
- 1 in 500 (0.2%)
- Lower
- Higher
- Equal
- Walking lunge
- Jump and hold
- Nordic hamstring
- Hip flexor stretch
- Landing stabilization exercises
- Lower body strength
- Endurance training
- Stretching
- Upper body strength
- Olympic weightlifting
- Once a month during sport season
- Twice a week before sport season and none during season
- Before each practice and game (2–3x a week)
- Once a week prior to and during season
- Neurocognitive Training
- Dynamic Stretching
- Endurance Training
- Balance Training
- Neuromuscular Training
- FIFA SuperFit program
- Neuromotor Plus Injury Prevention program (NIP)
- ReduceKnee program
- Prevent Injury and Enhance Performance program (PEP)
- 10%
- 25%
- 50%
- 80%
- 95%
- Keeping knees in line with toes (avoiding knocked knee position)
- Keeping trunk or upper body vertical (minimize hip flexion)
- Pointing toes outward
- Landing stiff or hard
- Landing softly
- 1 month
- 3 months
- 6 months
- Over 9 months
- They cannot return to sport following an ACL injury
- True
- False
- Rheumatoid Arthritis
- ACL injury on non-injured leg
- Duchenne Muscular Dystrophy
- ACL re-tear
- Osteoarthritis
- Lateral epicondylitis
References
- Herzog, M.M.; Marshall, S.W.; Lund, J.L.; Pate, V.; Mack, C.D.; Spang, J.T. Incidence of anterior cruciate ligament reconstruction among adolescent females in the United States, 2002 through 2014. JAMA Pediatr. 2017, 171, 808–810. [Google Scholar] [CrossRef] [PubMed]
- Sugimoto, D.; Myer, G.D.; Bush, H.M.; Klugman, M.F.; Medina McKeon, J.M.; Hewett, T.E. Compliance with neuromuscular training and anterior cruciate ligament injury risk reduction in female athletes: A meta-analysis. J. Athl. Train. 2012, 47, 714–723. [Google Scholar] [CrossRef] [Green Version]
- Petushek, E.J.; Sugimoto, D.; Stoolmiller, M.; Smith, G.; Myer, G.D. Evidence-based best-practice guidelines for preventing anterior cruciate ligament injuries in young female athletes: A systematic review and meta-analysis. Am. J. Sports Med. 2018, 47, 1744–1753. [Google Scholar] [CrossRef]
- Soomro, N.; Sanders, R.; Hackett, D.; Hubka, T.; Ebrahimi, S.; Freeston, J.; Cobley, S. The efficacy of injury prevention programs in adolescent team sports: A meta-analysis. Am. J. Sports Med. 2016, 44, 2415–2424. [Google Scholar] [CrossRef]
- Sugimoto, D.; Myer, G.D.; Foss, K.D.B.; Hewett, T.E. Specific exercise effects of preventive neuromuscular training intervention on anterior cruciate ligament injury risk reduction in young females: Meta-analysis and subgroup analysis. Br. J. Sports Med. 2015, 49, 282–289. [Google Scholar] [CrossRef] [Green Version]
- Joy, E.A.; Taylor, J.R.; Novak, M.A.; Chen, M.; Fink, B.P.; Porucznik, C.A. Factors Influencing the implementation of anterior cruciate ligament injury prevention strategies by girls soccer coaches. J. Strength Cond. Res. 2013, 27, 2263–2269. [Google Scholar] [CrossRef]
- Norcross, M.F.; Johnson, S.T.; Bovbjerg, V.E.; Koester, M.C.; Hoffman, M.A. Factors influencing high school coaches’ adoption of injury prevention programs. J. Sci. Med. Sport 2016, 19, 299–304. [Google Scholar] [CrossRef]
- Sugimoto, D.; Myer, G.D.; Barber Foss, K.D.; Pepin, M.J.; Micheli, L.J.; Hewett, T.E. Critical components of neuromuscular training to reduce ACL injury risk in female athletes: Meta-regression analysis. Br. J. Sports Med. 2016, 50, 1259–1266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pryor, J.L.; Root, H.J.; Vandermark, L.W.; Pryor, R.R.; Martinez, J.C.; Trojian, T.H.; Denegar, C.R.; DiStefano, L.J. Coach-led preventive training program in youth soccer players improves movement technique. J. Sci. Med. Sport 2017, 20, 861–866. [Google Scholar] [CrossRef] [PubMed]
- Iversen, M.D.; Friden, C. Pilot study of female high school basketball players’ anterior cruciate ligament injury knowledge, attitudes, and practices. Scand. J. Med. Sci. Sports 2009, 19, 595–602. [Google Scholar] [CrossRef] [PubMed]
- Pollard, C.D.; Sigward, S.M.; Ota, S.; Langford, K.; Powers, C.M. The influence of in-season injury prevention training on lower-extremity kinematics during landing in female soccer players. Clin. J. Sport Med. 2006, 16, 223–227. [Google Scholar] [CrossRef]
- O’Brien, J.; Finch, C.F. Injury prevention exercise programmes in professional youth soccer: Understanding the perceptions of programme deliverers. BMJ Open Sport Exerc. Med. 2016, 2, e000075. [Google Scholar] [CrossRef] [Green Version]
- McKay, C.D.; Steffen, K.; Romiti, M.; Finch, C.F.; Emery, C.A. The effect of coach and player injury knowledge, attitudes and beliefs on adherence to the FIFA 11+ programme in female youth soccer. Br. J. Sports Med. 2014, 48, 1281–1286. [Google Scholar] [CrossRef] [Green Version]
- Orr, B.; Brown, C.; Hemsing, J.; McCormick, T.; Pound, S.; Otto, D.; Emery, C.A.; Beaupre, L.A. Female soccer knee injury: Observed knowledge gaps in injury prevention among players/parents/coaches and current evidence (the KNOW study). Scand. J. Med. Sci. Sports 2013, 23, 271–280. [Google Scholar] [CrossRef]
- Donaldson, A.; Callaghan, A.; Bizzini, M.; Jowett, A.; Keyzer, P.; Nicholson, M. A concept mapping approach to identifying the barriers to implementing an evidence-based sports injury prevention programme. Inj. Prev. 2019, 25, 244–251. [Google Scholar] [CrossRef] [PubMed]
- Pfile, K.R.; Curioz, B. Coach-led prevention programs are effective in reducing anterior cruciate ligament injury risk in female athletes: A number-needed-to-treat analysis. Scand. J. Med. Sci. Sports 2017, 27, 1950–1958. [Google Scholar] [CrossRef] [PubMed]
- Petushek, E.J.; Ward, P.; Cokely, E.T.; Myer, G.D. Injury risk estimation expertise: Interdisciplinary differences in performance on the ACL injury risk estimation quiz. Orthop. J. Sports Med. 2015, 3, 2325967115614799. [Google Scholar] [CrossRef]
- Frank, B.S.; Register-Mihalik, J.; Padua, D.A. High levels of coach intent to integrate a ACL injury prevention program into training does not translate to effective implementation. J. Sci. Med. Sport 2015, 18, 400–406. [Google Scholar] [CrossRef] [PubMed]
- Petushek, E.J.; Cokely, E.T.; Ward, P.; Myer, G.D. Injury risk estimation expertise: Cognitive-perceptual mechanisms of ACL-IQ. J. Sport Exerc. Psychol. 2015, 37, 291–304. [Google Scholar] [CrossRef]
- Shams, L.; Seitz, A.R. Benefits of multisensory learning. Trends Cogn. Sci. 2008, 12, 411–417. [Google Scholar] [CrossRef]
- Mayer, R.E.; Moreno, R. Nine ways to reduce cognitive load in multimedia learning. Educ. Psychol. 2003, 38, 43–52. [Google Scholar] [CrossRef] [Green Version]
- Bravo, E.; Amante, B.; Simo, P.; Enache, M.; Fernandez, V. Video as a new teaching tool to increase student motivation. In Proceedings of the 2011 IEEE Global Engineering Education Conference (EDUCON), Amman, Jordan, 4–6 April 2011; pp. 638–642. [Google Scholar] [CrossRef] [Green Version]
- Azevedo, R.F.; Morrow, D.; Hasegawa-Johnson, M.; Gu, K.; Soberal, D.; Huang, T.; Schuh, W.; Garcia-Retamero, R. Improving patient comprehension of numeric health information. In Proceedings of the Human Factors and Ergonomics Society Annual Meeting, San Francisco, CA, USA, 27 October 2015; Volume 59, pp. 488–492. [Google Scholar]
- Volandes, A.E.; Barry, M.J.; Chang, Y.; Paasche-Orlow, M.K. Improving decision making at the end of life with video images. Med. Decis. Mak. 2010, 30, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Winston, K.; Grendarova, P.; Rabi, D. Video-based patient decision aids: A scoping review. Patient Educ. Couns. 2018, 101, 558–578. [Google Scholar] [CrossRef] [PubMed]
- Kay, R.; Kletskin, I. Evaluating the use of problem-based video podcasts to teach mathematics in higher education. Comput. Educ. 2012, 59, 619–627. [Google Scholar] [CrossRef]
- Allen Moore, W.; Russell Smith, A. Effects of video podcasting on psychomotor and cognitive performance, attitudes and study behaviour of student physical therapists. Innov. Educ. Teach. Int. 2012, 49, 401–414. [Google Scholar] [CrossRef]
- Austin, C.A.; Mohottige, D.; Sudore, R.L.; Smith, A.K.; Hanson, L.C. Tools to promote shared decision making in serious illness: A systematic review. JAMA Intern. Med. 2015, 175, 1213–1221. [Google Scholar] [CrossRef] [Green Version]
- Goldfarb, M.J.; Bibas, L.; Bartlett, V.; Jones, H.; Khan, N. Outcomes of patient-and family-centered care interventions in the ICU: A systematic review and meta-analysis. Crit. Care Med. 2017, 45, 1751–1761. [Google Scholar] [CrossRef] [PubMed]
- Stockwell, B.R.; Stockwell, M.S.; Cennamo, M.; Jiang, E. Blended learning improves science education. Cell 2015, 162, 933–936. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lim, S.L.; Yang, J.-C.; Ehrisman, J.; Havrilesky, L.J.; Reed, S.D. Are videos or text better for describing attributes in stated-preference surveys? Patient 2020, 13, 401–408. [Google Scholar] [CrossRef]
- Silva, A.F.; Ramirez-Campillo, R.; Sarmento, H.; Afonso, J.; Clemente, F.M. Effects of training programs on decision-making in youth team sports players: A systematic review and meta-analysis. Front. Psychol. 2021, 12, 1687. [Google Scholar] [CrossRef]
- Daneshvar, D.H.; Baugh, C.M.; Yutsis, M.; Pea, R.D.; Goldman, S.; Grant, G.A.; Cantu, R.C.; Sanders, L.M.; Chen, C.L.; Lama, R.D.; et al. Athlete enjoyment of prior education moderates change in concussion-reporting intention after interactive education. INQUIRY J. Health Care Organ. Provis. Financ. 2021, 58, 00469580211022641. [Google Scholar]
- Larkin, P.; Mesagno, C.; Berry, J.; Spittle, M.; Harvey, J. Video-based training to improve perceptual-cognitive decision-making performance of Australian football umpires. J. Sports Sci. 2018, 36, 239–246. [Google Scholar] [CrossRef]
- Mascarenhas, D.R.; Collins, D.; Mortimer, P.W.; Morris, B. Training accurate and coherent decision making in rugby union referees. Sport Psychol. 2005, 19, 131–147. [Google Scholar] [CrossRef] [Green Version]
- Glang, A.; Koester, M.C.; Beaver, S.; Clay, J.; McLaughlin, K. Online training in sports concussion for youth sports coaches. Int. J. Sports Sci. Coach. 2010, 5, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Mitchko, J.; Huitric, M.; Sarmiento, K.; Hayes, G.; Pruzan, M.; Sawyer, R. CDC’s approach to educating coaches about sports-related concussion. Am. J. Health Educ. 2007, 38, 99–103. [Google Scholar] [CrossRef]
- Mrazik, M.; Dennison, C.R.; Brooks, B.L.; Yeates, K.O.; Babul, S.; Naidu, D. A qualitative review of sports concussion education: Prime time for evidence-based knowledge translation. Br. J. Sports Med. 2015, 49, 1548–1553. [Google Scholar] [CrossRef]
- Feiss, R.; Lutz, M.; Reiche, E.; Moody, J.; Pangelinan, M. A Systematic review of the effectiveness of concussion education programs for coaches and parents of youth athletes. Int. J. Environ. Res. Public Health 2020, 17, 2665. [Google Scholar] [CrossRef]
- Anderson, S.F.; Maxwell, S.E. Addressing the “replication crisis”: Using original studies to design replication studies with appropriate statistical power. Multivar. Behav. Res. 2017, 52, 305–324. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, D.T.; King, G.; Pettigrew, S.; Wilson, T.D. Comment on “Estimating the reproducibility of psychological science”. Science 2016, 351, 1037. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maxwell, S.E.; Lau, M.Y.; Howard, G.S. Is psychology suffering from a replication crisis? What does “failure to replicate” really mean? Am. Psychol. 2015, 70, 487–498. [Google Scholar] [CrossRef] [PubMed]
- Shrout, P.E.; Rodgers, J.L. Psychology, science, and knowledge construction: Broadening perspectives from the replication crisis. Annu. Rev. Psychol. 2018, 69, 487–510. [Google Scholar] [CrossRef] [PubMed]
- Zack, E.S.; Kennedy, J.; Long, J.S. Can nonprobability samples be used for social science research? A cautionary tale. Surv. Res. Methods 2019, 13, 215–227. [Google Scholar] [CrossRef]
- Petushek, E.J.; Cokely, E.T.; Ward, P.; Durocher, J.J.; Wallace, S.J.; Myer, G.D. Injury risk estimation expertise: Assessing the ACL injury risk estimation quiz. Am. J. Sports Med. 2015, 43, 1640–1647. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Sultan, A.S.; AlYousef, M.Y.; Al Wtayyan, H.A.; Khamseen, M.A.B.; Alrasasi, M.N. Knowledge of community population in Al Ahsaa about the outcomes of ACL injury, 2017. Egypt. J. Hosp. Med. 2017, 69, 2935–2938. [Google Scholar] [CrossRef]
- McGorry, A. ACL Injuries. Available online: https://www.webmd.com/fitness-exercise/features/acl-injuries#1 (accessed on 1 September 2019).
- Fleiss, J.L. Design and Analysis of Clinical Experiments; John Wiley & Sons: New York, NY, USA, 1999. [Google Scholar]
- Weiner, B.J.; Lewis, C.C.; Stanick, C.; Powell, B.J.; Dorsey, C.N.; Clary, A.S.; Boynton, M.H.; Halko, H. Psychometric assessment of three newly developed implementation outcome measures. Implement. Sci. 2017, 12, 108. [Google Scholar] [CrossRef]
- Benjamini, Y. Yekutieli, D. The control of the false discovery rate in multiple testing under dependency. Ann. Stat. 2001, 29, 1165–1188. [Google Scholar] [CrossRef]
- Allaire, J. RStudio: Integrated Development Environment for R; Version 1.2.1335; RStudio, PBC: Boston, MA, USA, 2018. [Google Scholar]
- Ghazal, S.; Cokely, E.; Garcia-Retamero, R.; Feltz, A. Decision Making Skill: From Intelligence to Numeracy and Expertise. In Cambridge Handbook of Expertise and Expert Performance; Cambridge University Press: New York, NY, USA, 2018. [Google Scholar]
- Mayer, R.; Mayer, R.E. The Cambridge Handbook of Multimedia Learning; Cambridge University Press: Cambridge, UK, 2014. [Google Scholar]
- Shaffer, V.A.; Focella, E.S.; Hathaway, A.; Scherer, L.D.; Zikmund-Fisher, B.J. On the usefulness of narratives: An interdisciplinary review and theoretical model. Ann. Behav. Med. 2018, 52, 429–442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Šimkovic, M.; Träuble, B. Robustness of statistical methods when measure is affected by ceiling and/or floor effect. PLoS ONE 2019, 14, e0220889. [Google Scholar] [CrossRef] [PubMed]
- Hilska, M.; Leppänen, M.; Vasankari, T.; Aaltonen, S.; Kannus, P.; Parkkari, J.; Steffen, K.; Kujala, U.M.; Konttinen, N.; Räisänen, A.M.; et al. Neuromuscular training warm-up prevents acute noncontact lower extremity injuries in children’s soccer: A cluster randomized controlled trial. Orthop. J. Sports Med. 2021, 9, 23259671211005770. [Google Scholar] [CrossRef]
- Austin, L.C.; Fischhoff, B. Injury prevention and risk communication: A mental models approach. Inj. Prev. 2012, 18, 124. [Google Scholar] [CrossRef] [Green Version]
- Donaldson, A.; Finch, C.F. Applying Implementation Science to Sports Injury Prevention. Br. J. Sports Med. 2013, 47, 473–475. [Google Scholar] [CrossRef] [PubMed]
- Michie, S.; van Stralen, M.M.; West, R. The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implement. Sci. 2011, 6, 42. [Google Scholar] [CrossRef] [Green Version]
- Wood, F.B.; Benson, D.; LaCroix, E.-M.; Siegel, E.R.; Fariss, S. Use of internet audience measurement data to gauge market share for online health information services. J. Med. Internet Res. 2005, 7, e31. [Google Scholar] [CrossRef] [PubMed]
- Petushek, E.; Mattioli, E.; Jepkema, R. Evaluation of online information quality, usability, and readability for anterior cruciate ligament injury prevention. In Proceedings of the International Symposium on Human Factors and Ergonomics in Health Care, 18–21 May 2020. Virtual Conference. [Google Scholar]
- Gosselin, M.M.; Mulcahey, M.K.; Feller, E.; Hulstyn, M.J. Examining internet resources on gender differences in ACL injuries: What patients are reading. Knee 2013, 20, 196–202. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Animated Video | Web-Based Article | Placebo Control | p Value for Group Difference | |
|---|---|---|---|---|
| N | 99 | 71 | 86 | |
| Gender (% female) | 30.3 | 25.4 | 29.1 | 0.77 |
| Age (%) | 0.26 | |||
| 18–24 | 11 | 8 | 20 | |
| 25–34 | 41 | 34 | 27 | |
| 35–44 | 26 | 35 | 37 | |
| 45–54 | 14 | 14 | 10 | |
| 55 and older | 7 | 8 | 6 | |
| Years of experience (mean (SD)) | 6.35 (4.6) | 7.93 (5.9) | 6.85 (4.6) | 0.13 |
| Number of athletes * (mean (SD)) | 33.6 (21.6) | 34.0 (20.8) | 38.0 (25.8) | 0.38 |
| Gender of athletes (%) | 0.23 | |||
| Boys | 48 | 58 | 52 | |
| Girls | 33 | 21 | 26 | |
| Both | 18 | 21 | 22 | |
| Sports (%) | 0.95 | |||
| Soccer | 22 | 15 | 19 | |
| Basketball | 17 | 16 | 15 | |
| Football | 14 | 13 | 12 | |
| Volleyball | 8 | 3 | 5 | |
| Lacrosse | 1 | 1 | 3 | |
| Gymnastics | 7 | 1 | 5 | |
| Multiple | 30 | 22 | 27 | |
| Level of sports (%) | 0.68 | |||
| Youth | 34 | 35 | 38 | |
| Middle School | 12 | 6 | 9 | |
| High School | 13 | 17 | 18 | |
| College | 3 | 7 | 2 | |
| Multiple | 37 | 35 | 31 | |
| Awareness of IPP ** (% yes) | 13 | 15 | 16 | 0.82 |
| Condition | Degrees of Freedom | F Statistic | p Value | Eta-Squared (Partial) | 95% CI |
|---|---|---|---|---|---|
| Overall Comprehension | |||||
| Pre and Post Test | 1 | 57.92 | <0.001 | 0.19 | 0.12–0.26 |
| Pre and Post Test × Condition | 2 | 14.14 | <0.001 | 0.10 | 0.05–0.16 |
| Basic ACL Knowledge | |||||
| Pre and Post Test | 1 | 31.57 | <0.001 | 0.11 | 0.06–0.18 |
| Pre and Post Test × Condition | 2 | 2.74 | 0.07 | 0.02 | 0–0.05 |
| Risk Knowledge | |||||
| Pre and Post Test | 1 | 31.19 | <0.001 | 0.11 | 0.06–0.17 |
| Pre and Post Test × Condition | 2 | 9.09 | <0.001 | 0.07 | 0.02–0.12 |
| Prevention Knowledge | |||||
| Pre and Post Test | 1 | 6.92 | <0.01 | 0.03 | 0–0.07 |
| Pre and Post Test × condition | 2 | 2.34 | 0.1 | 0–0.05 | |
| Severity Knowledge | |||||
| Pre and Post Test | 1 | 31.49 | <0.001 | 0.11 | 0.06–0.17 |
| Pre and Post Test × condition | 2 | 19.48 | <0.001 | 0.13 | 0.07–0.2 |
| Pre | Post | |||||
|---|---|---|---|---|---|---|
| M | SD | M | SD | Cohen’s d | 95% CI | |
| Overall Comprehension | ||||||
| Animated video | 32.77 | 11.47 | 43.65 | 13.65 | 0.86 | 0.57–1.16 |
| Web-based article | 31.99 | 13.16 | 37.12 | 12.93 | 0.39 | 0.06–0.73 |
| Control | 34.52 | 13.93 | 35.52 | 14.15 | 0.09 | −0.21–0.40 |
| Basic ACL Knowledge | ||||||
| Animated video | 66.84 | 35.13 | 79.29 | 31.95 | 0.37 | 0.09–0.65 |
| Web-based article | 66.2 | 33.36 | 79.58 | 33.36 | 0.38 | 0.04–0.71 |
| Control | 72.35 | 35.01 | 76.47 | 35.01 | 0.11 | −0.19–0.41 |
| Risk Knowledge | ||||||
| Animated video | 36.36 | 27.39 | 53.87 | 21.67 | 0.71 | 0.42–1.00 |
| Web-based article | 36.15 | 26.27 | 46 | 28.9 | 0.36 | 0.02–0.69 |
| Control | 37.98 | 27.13 | 38.76 | 27.47 | 0.03 | −0.27–0.33 |
| Prevention Knowledge | ||||||
| Animated video | 30.44 | 14.36 | 36.7 | 18.59 | 0.38 | 0.09–0.66 |
| Web-based article | 27.93 | 14.85 | 30.05 | 15.33 | 0.14 | −0.19–0.47 |
| Control | 31.75 | 16.28 | 32.33 | 17.53 | 0.03 | −0.27–0.34 |
| Severity Knowledge | ||||||
| Animated video | 10.77 | 15.67 | 23.57 | 15.25 | 0.83 | 0.54–1.12 |
| Web-based article | 13.15 | 16.41 | 14.09 | 16.58 | 0.06 | −0.27–0.39 |
| Control | 12.79 | 16.3 | 14.34 | 16.6 | 0.09 | −0.21–0.40 |
| Condition | Variable Name | p Value * | Cohen’s d | 95% CI |
|---|---|---|---|---|
| Animated video vs. Control | ||||
| Overall Comprehension | <0.01 | 0.56 | 0.26–0.86 | |
| Basic ACL Knowledge | 1.0 | 0.08 | −0.21–0.37 | |
| Risk Knowledge | <0.01 | 0.62 | 0.31–0.91 | |
| Prevention Knowledge | 0.29 | 0.24 | −0.05–0.54 | |
| Severity Knowledge | <0.01 | 0.58 | 0.28–0.88 | |
| Web-based article vs. Control | ||||
| Overall Comprehension | 1.0 | 0.09 | −0.23–0.41 | |
| Basic ACL Knowledge | 1.0 | 0.09 | −0.23–0.41 | |
| Risk Knowledge | 0.21 | 0.26 | −0.06–0.58 | |
| Prevention Knowledge | 0.72 | −0.14 | −0.46–0.18 | |
| Severity Knowledge | 1.0 | −0.02 | −0.33–0.3 | |
| Animated video vs. Web-based article | ||||
| Overall Comprehension | <0.01 | 0.49 | 0.18–0.8 | |
| Basic ACL Knowledge | 1.0 | −0.01 | −0.32–0.3 | |
| Risk Knowledge | 0.15 | 0.32 | 0.01–0.62 | |
| Prevention Knowledge | 0.06 | 0.38 | 0.07–0.69 | |
| Severity Knowledge | <0.01 | 0.6 | 0.29–0.91 |
| Experiment Group | N | Mean | SD | Comparison Group | t-Test p Value * | Cohen’s d | 95% CI |
|---|---|---|---|---|---|---|---|
| Animated Video | 99 | 4.31 | 0.71 | Control | 0.03 | 0.38 | 0.09–0.68 |
| Control | 86 | 4.04 | 0.72 | Web-based article | 0.03 | 0.41 | 0.08–0.72 |
| Web-based article | 71 | 4.30 | 0.60 | Animated Video | 1.0 | 0.01 | −0.30–0.32 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Petushek, E.J.; Mørtvedt, A.I.; Nelson, B.L.; Hamati, M.C. The Effect of a Brief, Web-Based Animated Video for Improving Comprehension and Implementation Feasibility for Reducing Anterior Cruciate Ligament Injury: A Three-Arm Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2021, 18, 9092. https://doi.org/10.3390/ijerph18179092
Petushek EJ, Mørtvedt AI, Nelson BL, Hamati MC. The Effect of a Brief, Web-Based Animated Video for Improving Comprehension and Implementation Feasibility for Reducing Anterior Cruciate Ligament Injury: A Three-Arm Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2021; 18(17):9092. https://doi.org/10.3390/ijerph18179092
Chicago/Turabian StylePetushek, Erich J., Anne Inger Mørtvedt, Brittany L. Nelson, and Mary C. Hamati. 2021. "The Effect of a Brief, Web-Based Animated Video for Improving Comprehension and Implementation Feasibility for Reducing Anterior Cruciate Ligament Injury: A Three-Arm Randomized Controlled Trial" International Journal of Environmental Research and Public Health 18, no. 17: 9092. https://doi.org/10.3390/ijerph18179092