
Effect of Different Software Programs on the Accuracy of Dental Scanner Using Three-Dimensional Analysis



Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
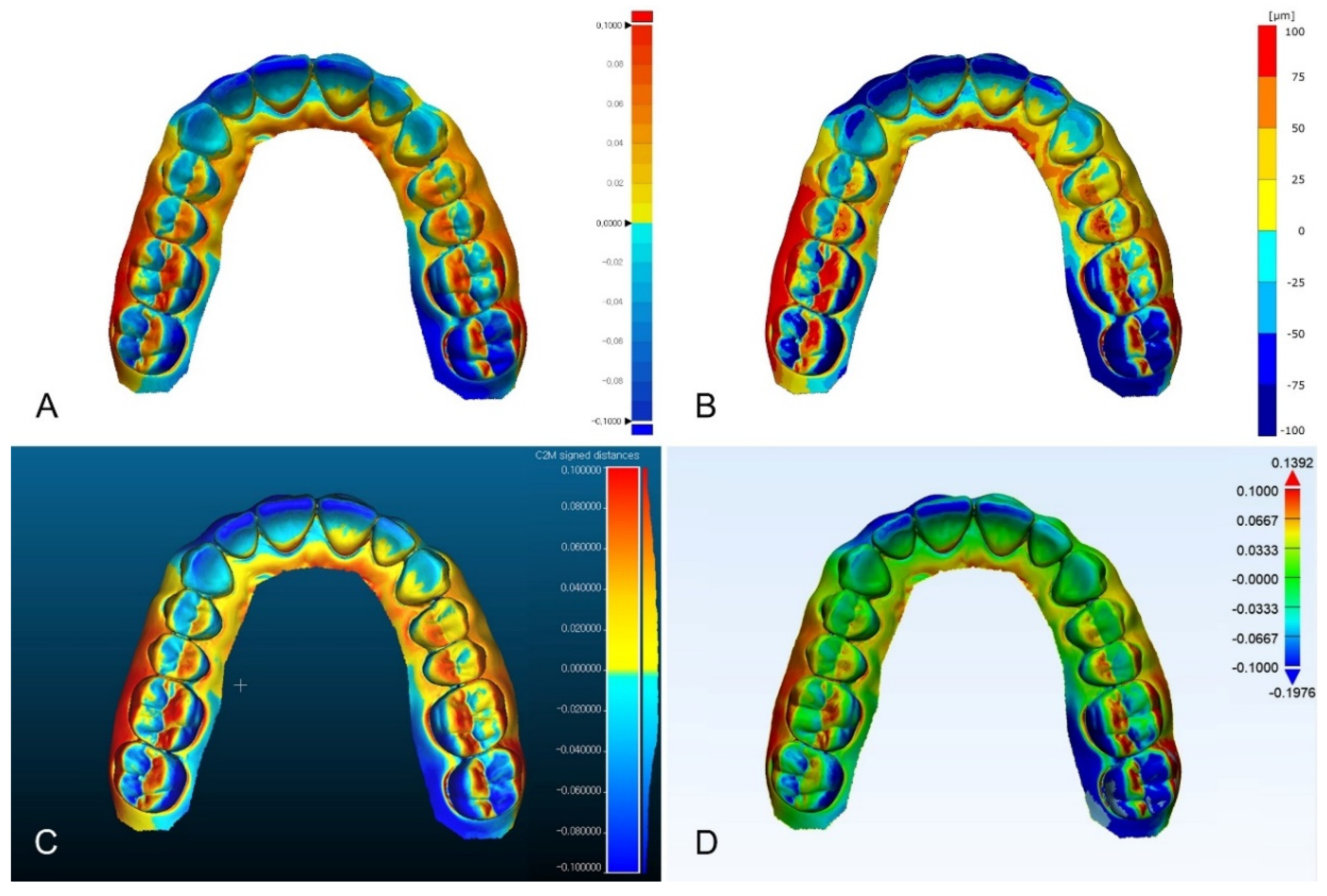
- As the area of the virtual model for 3D analysis becomes smaller, a difference in results occurs depending on the software program used.
- The difference in results among software programs is not considered in the 3D analysis for the complete-arch region.
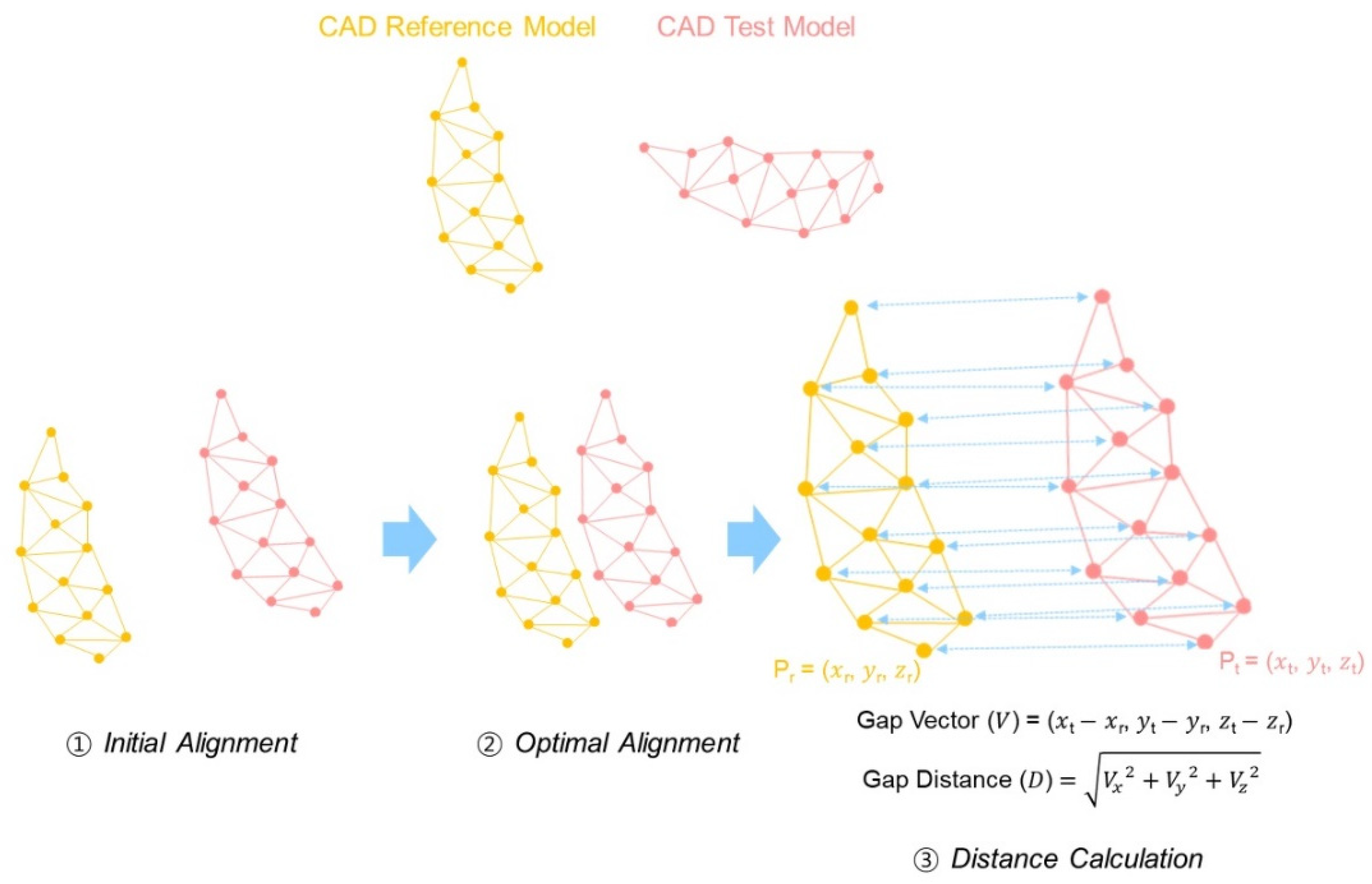
- Differences in the results are due to the heterogeneity of RMS calculation algorithms rather than on the different alignment algorithms of the software program used.
- Therefore, in light of these conclusions, the accuracy analysis of the intraoral scanner for complete arch can be evaluated without considering the software program.
- The use of software programs for 3D analysis should be determined according to the clinical situation.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CAD/CAM | computer-aided design and computer-aided manufacturing |
| 3D | three-dimensional |
| CRM | computer-aided design reference model |
| CTM | computer-aided design test model |
| ICP | iterative closest point |
| RMS | root mean square |
| ANOVA | analysis of variance |
| HSD | honestly significant difference |
References
- Rekow, E.D. Digital dentistry: The new state of the art—Is it disruptive or destructive? Dent. Mater. 2020, 36, 9–24. [Google Scholar] [CrossRef]
- Baghani, M.T.; Shayegh, S.S.; Johnston, W.M.; Shidfar, S.; Hakimaneh, S.M.R. In vitro evaluation of the accuracy and precision of intraoral and extraoral complete-arch scans. J. Prosthet. Dent. 2020. [Google Scholar] [CrossRef] [PubMed]
- Persson, A.S.; Odén, A.; Andersson, M.; Sandborgh-Englund, G. Digitization of simulated clinical dental impressions: Virtual three-dimensional analysis of exactness. Dent. Mater. 2009, 25, 929–936. [Google Scholar] [CrossRef] [PubMed]
- Revilla-León, M.; Subramanian, S.G.; Özcan, M.; Krishnamurthy, V.R. Clinical study of the influence of ambient light scanning conditions on the accuracy (trueness and precision) of an intraoral scanner. J. Prosthodont. 2020, 29, 107–113. [Google Scholar] [CrossRef]
- Sim, J.Y.; Jang, Y.; Kim, W.C.; Kim, H.Y.; Lee, D.H.; Kim, J.H. Comparing the accuracy (trueness and precision) of models of fixed dental prostheses fabricated by digital and conventional workflows. J. Prosthodont. Res. 2019, 63, 25–30. [Google Scholar] [CrossRef] [PubMed]
- Piedra-Cascón, W.; Methani, M.M.; Quesada-Olmo, N.; Jiménez-Martínez, M.J.; Revilla-León, M. Scanning accuracy of nondental structured light extraoral scanners compared with that of a dental-specific scanner. J. Prosthet. Dent. 2020. [Google Scholar] [CrossRef] [PubMed]
- Son, K.; Lee, K.B. Effect of tooth types on the accuracy of dental 3d scanners: An in vitro study. Materials 2020, 13, 1744. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vecsei, B.; Joós-Kovács, G.; Borbély, J.; Hermann, P. Comparison of the accuracy of direct and indirect three-dimensional digitizing processes for CAD/CAM systems—An in vitro study. J. Prosthodont. Res. 2017, 61, 177–184. [Google Scholar] [CrossRef]
- Zhang, F.; Suh, K.J.; Lee, K.M. Validity of intraoral scans compared with plaster models: An in-vivo comparison of dental measurements and 3D surface analysis. PLoS ONE 2016, 11, e0157713. [Google Scholar] [CrossRef]
- Kim, R.J.Y.; Park, J.M.; Shim, J.S. Accuracy of 9 intraoral scanners for complete-arch image acquisition: A qualitative and quantitative evaluation. J. Prosthet. Dent. 2018, 120, 895–903.e1. [Google Scholar] [CrossRef]
- Park, G.H.; Son, K.; Lee, K.B. Feasibility of using an intraoral scanner for a complete-arch digital scan. J. Prosthet. Dent. 2019, 121, 803–810. [Google Scholar] [CrossRef]
- Peng, P.W.; Hsu, C.Y.; Huang, H.Y.; Chao, J.C.; Lee, W.F. Trueness of removable partial denture frameworks additively manufactured with selective laser melting. J. Prosthet. Dent. 2020. [Google Scholar] [CrossRef]
- Yu, B.Y.; Son, K.; Lee, K.B. Evaluation of intaglio surface trueness and margin quality of interim crowns in accordance with the build angle of stereolithography apparatus 3-dimensional printing. J. Prosthet. Dent. 2020. [Google Scholar] [CrossRef]
- Ammoun, R.; Suprono, M.S.; Goodacre, C.J.; Oyoyo, U.; Carrico, C.K.; Kattadiyil, M.T. Influence of tooth preparation design and scan angulations on the accuracy of two intraoral digital scanners: An in vitro study based on 3-dimensional comparisons. J. Prosthodont. 2020, 29, 201–206. [Google Scholar] [CrossRef]
- Latham, J.; Ludlow, M.; Mennito, A.; Kelly, A.; Evans, Z.; Renne, W. Effect of scan pattern on complete-arch scans with 4 digital scanners. J. Prosthet. Dent. 2020, 123, 85–95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Treesh, J.C.; Liacouras, P.C.; Taft, R.M.; Brooks, D.I.; Raiciulescu, S.; Ellert, D.O.; Ye, L. Complete-arch accuracy of intraoral scanners. J. Prosthet. Dent. 2018, 120, 382–388. [Google Scholar] [CrossRef] [PubMed]
- Sousa, M.V.S.; Vasconcelos, E.C.; Janson, G.; Garib, D.; Pinzan, A. Accuracy and reproducibility of 3-dimensional digital model measurements. Am. J. Orthod. Dentofac. Orthop. 2012, 142, 269–273. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z. Iterative point matching for registration of free-form curves and surfaces. Int. J Comput. Vis. 1994, 13, 119–152. [Google Scholar] [CrossRef]
- Sharp, G.C.; Lee, S.W.; Wehe, D.K. ICP registration using invariant features. IEEE Trans. Pattern Anal. Mach. Intell. 2002, 24, 90–102. [Google Scholar] [CrossRef] [Green Version]
- Pérez, L.; Diez, E.; Usamentiaga, R.; García, D.F. Industrial robot control and operator training using virtual reality interfaces. Comput. Ind. 2019, 109, 114–120. [Google Scholar] [CrossRef]
- O’Toole, S.; Osnes, C.; Bartlett, D.; Keeling, A. Investigation into the accuracy and measurement methods of sequential 3D dental scan alignment. Dent. Mater. 2019, 35, 495–500. [Google Scholar] [CrossRef]
- Jeong, Y.G.; Lee, W.S.; Lee, K.B. Accuracy evaluation of dental models manufactured by CAD/CAM milling method and 3D printing method. J. Adv. Prosthodont. 2018, 10, 245. [Google Scholar] [CrossRef] [Green Version]
- Park, J.M.; Jeon, J.; Koak, J.Y.; Kim, S.K.; Heo, S.J. Dimensional accuracy and surface characteristics of 3D-printed dental casts. J. Prosthet. Dent. 2020. [Google Scholar] [CrossRef]
- Lee, D.; Lee, S.Y.; Kim, H.; Park, C. A Hybrid Dental Model Concept Utilizing Fused Deposition Modeling and Digital Light Processing 3D Printing. Int. J. Prosthodont. 2020, 33, 229–231. [Google Scholar] [CrossRef]
- Deja, M.; Dobrzyński, M.; Rymkiewicz, M. Application of reverse engineering technology in part design for shipbuilding industry. Pol. Marit. Res. 2019, 26, 126–133. [Google Scholar] [CrossRef] [Green Version]
- Chen, L.; Lin, W.S.; Polido, W.D.; Eckert, G.J.; Morton, D. Accuracy, reproducibility, and dimensional stability of additively manufactured surgical templates. J. Prosthet. Dent. 2019, 122, 309–314. [Google Scholar] [CrossRef]
- Lin, C.C.; Ishikawa, M.; Huang, B.H.; Huang, M.S.; Cheng, H.C.; Maida, T.; Endo, K. In vitro accuracy of static guided implant surgery measured by optical scan: Examining the impact of operator experience. Appl. Sci. 2020, 10, 2718. [Google Scholar] [CrossRef] [Green Version]
- Cheng, S.; Marras, I.; Zafeiriou, S.; Pantic, M. Statistical non-rigid ICP algorithm and its application to 3D face alignment. Image Vis. Comput. 2017, 58, 3–12. [Google Scholar] [CrossRef]
- Marcel, R.; Reinhard, H.; Andreas, K. Accuracy of CAD/CAM-fabricated bite splints: Milling vs 3D printing. Clin. Oral Investig. 2020, 24, 4607–4615. [Google Scholar] [CrossRef] [PubMed]
- Li, P.; Wang, R.; Wang, Y.; Tao, W. Evaluation of the ICP Algorithm in 3D Point Cloud Registration. IEEE Access 2020, 8, 68030–68048. [Google Scholar] [CrossRef]
- Holz, D.; Ichim, A.E.; Tombari, F.; Rusu, R.B.; Behnke, S. Registration with the point cloud library: A modular framework for aligning in 3-D. IEEE Robot Autom. Mag. 2015, 22, 110–124. [Google Scholar] [CrossRef]
- Winkler, J.; Gkantidis, N. Trueness and precision of intraoral scanners in the maxillary dental arch: An in vivo analysis. Sci. Rep. 2020, 10, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kernen, F.; Schlager, S.; Alvarez, V.S.; Mehrhof, J.; Vach, K.; Kohal, R.; Flügge, T. Accuracy of intraoral scans: An in vivo study of different scanning devices. J. Prosthet. Dent. 2021, in press. [Google Scholar] [CrossRef] [PubMed]
- Son, K.; Lee, S.; Kang, S.H.; Park, J.; Lee, K.B.; Jeon, M.; Yun, B.J. A comparison study of marginal and internal fit assessment methods for fixed dental prostheses. J. Clin. Med. 2019, 8, 785. [Google Scholar] [CrossRef] [Green Version]
- Huang, M.Y.; Son, K.; Lee, K.B. Effect of distance between the abutment and the adjacent teeth on intraoral scanning: An in vitro study. J. Prosthet. Dent. 2021, 125, 911–917. [Google Scholar] [CrossRef] [PubMed]
- Son, K.; Lee, K.B. Effect of finish line locations of tooth preparation on the accuracy of intraoral scanners. Int. J. Comput. Dent. 2021, 24, 29–40. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 3D Analysis Software Programs | Function | Version | Payment | |||||
|---|---|---|---|---|---|---|---|---|
| Alignment | 3D Analysis | |||||||
| Initial Alignment | Optimal Alignment | Align Algorithm | 3D Comparison | Calculation Principle | ||||
| Geomagic control X | Initial alignment | Best-fit alignment | Iterative closest point | 3D compare | Root mean square | v2019.0.1 | Paid | |
| GOM Inspect | Pre alignment | Local best-fit | Iterative closest point | Surface comparison | Root mean square | v2.0.1 | Free (Partially paid) | |
| Cloudcompare | Point pairs picking | Fine registration | Iterative closest point | Mesh distance | Root mean square | v2.12 | Free | |
| Materialise 3-matic | N points registration | Global registration | Iterative closest point | Part comparison analysis | Root mean square | v13.0 | Paid | |
| Analysis Region | Descriptive Statistics | 3D Analysis Software Program | F | p * | ||||
|---|---|---|---|---|---|---|---|---|
| Geomagic Control X | GOM Inspect | Cloudcompare | Materialise 3-Matic | |||||
| Complete arch | Mean ± SD | 49.6 ± 13.0 | 58.7 ± 12.6 | 50.3 ± 12.1 | 52.4 ± 15.1 | 1.888 | 0.139 | |
| 95% CI | Lower | 43.5 | 52.7 | 44.8 | 45.3 | |||
| Upper | 55.7 | 64.6 | 56.2 | 59.5 | ||||
| Half arch | Mean ± SD | 37.0 ± 5.1 a | 44.3 ± 5.4 b | 40.8 ± 4.8 b | 40.0 ± 4.8 b | 6.893 | <0.001 | |
| 95% CI | Lower | 34.7 | 41.7 | 38.5 | 37.8 | |||
| Upper | 39.4 | 46.9 | 43.0 | 42.3 | ||||
| Tooth preparation | Mean ± SD | 24.1 ± 2.5 a | 21.2 ± 2.2 b | 23.6 ± 2.2 a,b | 25.4 ± 2.8 b | 10.211 | <0.001 | |
| 95% CI | Lower | 22.9 | 20.1 | 22.5 | 24.1 | |||
| Upper | 25.1 | 22.2 | 24.6 | 26.7 | ||||
| Descriptive Statistics | 3D Analysis Software Program | F | p * | |||||
|---|---|---|---|---|---|---|---|---|
| Geomagic Control X | GOM Inspect | Cloudcompare | Materialise 3-Matic | |||||
| Different RMS calculation methods | Mean ± SD | 24.1 ± 2.5 a,b | 23.1 ± 1.9 a | 24.6 ± 1.9 a,b | 25.5 ± 2.2 b | 4.291 | 0.007 | |
| 95% CI | Lower | 17.9 | 19.0 | 20.3 | 20.7 | |||
| Upper | 28.7 | 26.0 | 28.4 | 28.9 | ||||
| Different alignment procedure | Mean ± SD | 24.1 ± 2.5 | 24.2 ± 2.5 | 24.2 ± 2.5 | 25.0 ± 3.1 | 0.475 | 0.701 | |
| 95% CI | Lower | 17.9 | 17.9 | 18.0 | 18.0 | |||
| Upper | 28.7 | 28.7 | 28.8 | 30.2 | ||||
| Source | F | p |
|---|---|---|
| 3D analysis software program | 3.022 | 0.031 * |
| Analysis region | 247.564 | <0.001 * |
| 3D analysis software program x Analysis region | 2.621 | 0.018 ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Son, K.; Lee, W.-S.; Lee, K.-B. Effect of Different Software Programs on the Accuracy of Dental Scanner Using Three-Dimensional Analysis. Int. J. Environ. Res. Public Health 2021, 18, 8449. https://doi.org/10.3390/ijerph18168449
Son K, Lee W-S, Lee K-B. Effect of Different Software Programs on the Accuracy of Dental Scanner Using Three-Dimensional Analysis. International Journal of Environmental Research and Public Health. 2021; 18(16):8449. https://doi.org/10.3390/ijerph18168449
Chicago/Turabian StyleSon, Keunbada, Wan-Sun Lee, and Kyu-Bok Lee. 2021. "Effect of Different Software Programs on the Accuracy of Dental Scanner Using Three-Dimensional Analysis" International Journal of Environmental Research and Public Health 18, no. 16: 8449. https://doi.org/10.3390/ijerph18168449