1. Introduction
Adolescent mental health problems are a growing concern [
1]. Depression, anxiety, and stress are important indicators of common mental health problems [
2,
3]. In past decades, an upward trend of psychological distress has been reported, with an increasing number of young people suffering from mental health problems all around the world [
4,
5,
6,
7]. In a meta-analysis of 24 studies, Regehr [
8] reported that around half of university students displayed moderate levels of mental health problems such as depression, anxiety, and stress. In the United States [
5], researchers found that 33% of university students exhibited depressive symptoms, 40% exhibited anxiety symptoms, and 38% showed symptoms of stress. In mainland China, Gao [
6] found that 32%, 45%, and 26% of university students exhibited depression, anxiety, and stress, respectively. The high prevalence of psychological morbidity among university students is alarming and deserves further investigation and intervention.
Hong Kong is a highly competitive city where young people face huge stress such as academic/career challenges, high property prices, and low income [
1], with a significant number of young locals displaying psychological distress [
9]. A 10-year longitudinal cohort study indicated that the percentage of the Hong Kong adult population with depression increased from 1.9% between 2009 and 2014 to 11.2% in 2019 [
10]. Moreover, many studies have found that mental health problems and psychological morbidity are quite common among university students [
5,
7,
8,
9,
11]. In a study of 7915 freshmen in Hong Kong, Wong et al. [
9] found that 21%, 41%, and 27% of students displayed moderately severe or above-average levels of depression, anxiety, and stress levels, respectively. Similarly, in a survey involving 1200 university students in Hong Kong, 68.5% of participants reported mild to severe depression symptoms, and 54.4% reported mild to severe symptoms of anxiety [
11]. Due to the high lifetime prevalence of psychological distress and the great suffering of patients and society, it is urgent to have a deeper understanding of university students’ mental health.
There are two demographic correlates of the psychological morbidity of university students which deserve attention. First, gender differences in psychological morbidity have long been a focus of researchers, but the findings are mixed. Although many traditional viewpoints have supposed that females are more vulnerable to negative events and have more mental health problems than males in general [
12,
13], an increasing number of studies have argued that males suffer from more burnout and psychological distress than females in the contemporary world (e.g., [
14,
15]). Specifically, although some scholars found that females are more depressed than males (e.g., [
16,
17,
18,
19]), a comparable number of research findings discovered that males reported higher scores on depression scales than females (e.g., [
6,
9,
15,
19,
20]). In regard to anxiety, most of the existing studies have revealed a higher level of anxiety in females (e.g., [
4,
6,
9,
17,
21]), while very few studies have found that males were more anxious than females in response to controllable events (e.g., [
12]). Concerning stress, some studies have reported that females showed a higher level of stress than males (e.g., [
4,
9,
18,
21]), whereas a limited number of studies have indicated that males are more stressed than females (e.g., [
15]). In short, the gender difference in mental health is unclear.
Secondly, the occurrence of political events is another correlate of the mental health of young people. Obviously, the occurrence of political events, such as protests, riots, revolutions, or political instability, would also constitute risk factors for adolescent development [
22,
23]. Thus, different cohorts of young people may display different levels of psychological morbidity in response to the political events they experience. Unfortunately, few studies have examined how political factors may influence adolescent development [
24].
Besides gender and political event correlates, there are well-being correlates of psychological morbidity. Conceptually speaking, there are two domains of well-being [
25], including eudaimonic well-being (i.e., self-realization and fully functioning) and hedonic well-being (i.e., pleasure-seeking and avoidance of pain). Although some research has shown a relationship between negative events and mental health problems, very few studies have investigated psychological morbidity and well-being indexed by positive youth development (PYD) attributes and life satisfaction. PYD can be regarded as eudaimonic well-being [
26], which refers to individuals’ psychosocial competence and positive functioning, which can protect against negative emotions and behaviors [
27,
28]. Lerner et al. [
29] stated that young people with positive development are less likely to experience mental health problems such as depression. Zhou et al. [
30] uncovered that PYD attributes could protect young people from depression. Although the benefits of PYD have been widely studied among adolescents, they have seldom been explored in university students [
28,
31].
Life satisfaction can be regarded as hedonic well-being [
26,
32], and the impact of life satisfaction on depression, anxiety, and stress has been reported (e.g., [
33,
34]). For instance, Gilman and Huebner [
35] and Tsitsas et al. [
36] revealed that life satisfaction had negative impacts on depression, anxiety, and stress. However, most of the existing studies are based on Western people [
35,
36].
In view of the growing mental health problems in university students, the development of objective assessment tools is indispensable. In the scientific literature, some scales have been commonly used to measure mental health problems, but only the DASS can measure depression, anxiety, and stress using a single instrument. The DASS has been translated into at least 44 different languages and has been validated across different age groups, different countries, different regions, and clinical and non-clinical populations [
37]. Although some researchers have argued that either the one-factor model [
19], the bi-factor model [
17], or the second-order model/hierarchical factor model [
38] is more suitable than the original three-factor model [
39], most studies have supported the three-factor model (e.g., [
40,
41,
42,
43]).
Although the DASS has been validated in mainland China [
20,
42], it has not been validated in other Chinese communities, including Singapore, Taiwan, Macau, and Hong Kong. Among the existing Chinese studies using the DASS, Wong et al. [
9] revealed that male university students displayed more depression and less anxiety and stress than their female counterparts in Hong Kong. Gao et al. [
6] found that female mainland Chinese university students were significantly more anxious than males, with no gender differences in terms of depression and stress. In short, Chinese findings concerning gender differences in mental health are equivocal. Furthermore, very limited research has examined the role of political events in adolescent psychological morbidity. Due to the de-emphasis of holistic development in Chinese communities [
1], only very limited Chinese studies investigated the role of PYD and life satisfaction in reducing psychological distress, although PYD has been demonstrated to positively prevent psychological and social problems [
30,
44]. Finally, no study has to date examined the relationship between well-being (indexed by PYD and life satisfaction) and psychological morbidity (indexed by the DASS).
To fill these research gaps, this study examined the factor structure of the DASS in Hong Kong and also examined the gender, political event, and well-being (PYD and life satisfaction) correlates and psychological morbidity indexed by the DASS measures. We attempted to address the following research questions.
Research Question 1: What is the mental health status of university students in Hong Kong? With reference to the findings that mental health symptoms are widespread in university students in Hong Kong [
7,
9,
10,
11], we expected that prevalence rates based on the DASS would be comparable to the existing findings.
Research Question 2: What are the psychometric properties of the DASS in university students in Hong Kong?
With reference to the literature, we put forward the following two hypotheses:
Hypothesis 1. It was expected that three factors (depression, anxiety, and stress) would emerge from the data based on the DASS.
Hypothesis 2. It was expected that the DASS would show stable factor structure across gender and time (five cohorts from 2014/15 to 2018/19 academic years) (Hypothesis 2a and Hypothesis 2b, respectively).
Research Question 3: Is gender related to the psychological morbidity of university students in Hong Kong? Based on the existing research findings [
9], it was expected that male students would show more symptoms of depression, anxiety, and stress than their female counterparts (Hypothesis 3).
Research Question 4: Do different cohorts of students show different levels of psychological morbidity?
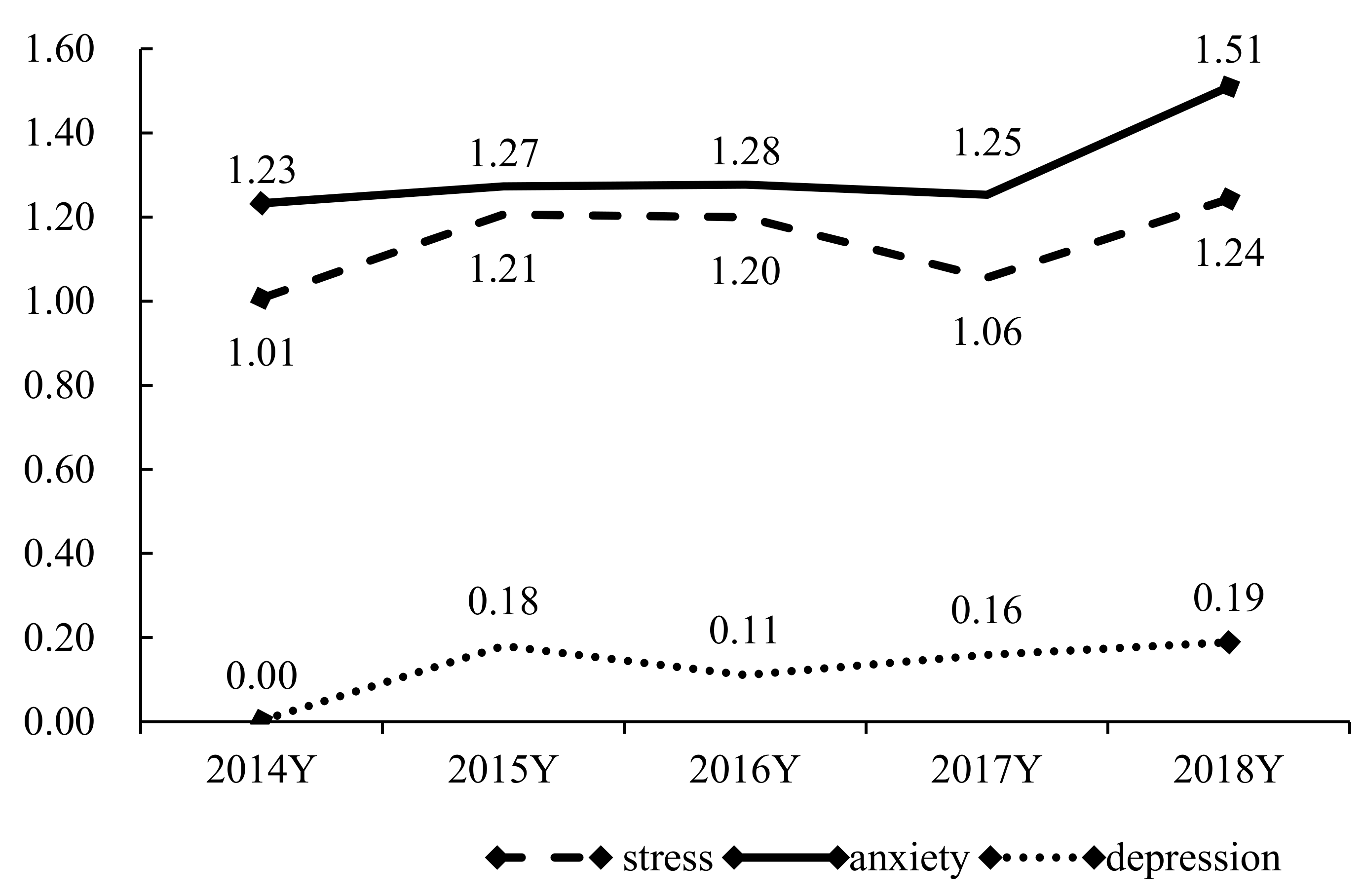
As the political situation in Hong Kong became stressful after 2014 (i.e., Umbrella Movement), we expected that the depression, anxiety, and stress symptoms would increase in the cohorts in 2015/16 to 2018/19 academic year (Hypothesis 4).
Research Question 5: Is psychological morbidity related to different aspects of well-being?
Based on the literature [
44,
45,
46], it was expected that a higher level of eudaimonic well-being (indexed by PYD) and a higher level of hedonic well-being (indexed by life satisfaction) would be negatively related to depression, anxiety, and stress (Hypothesis 5a and Hypothesis 5b, respectively).
4. Discussion
Mental health problems appeared to be more serious in Hong Kong university students than 15 years ago [
9]. The mean depression has moved from “normal” to “mild”, the mean anxiety has moved from “mild” to “moderate”, and only the mean of stress stayed within a “normal” level among university students. Meanwhile, more young students showed at least moderate levels of depression (32.7% vs. 21%) and anxiety (44.7% vs. 41%). These prevalence rates suggest that the mental health scores of university students under the current study are worse than those reported previously. This implies that the psychological distress of young university students in Hong Kong deserves notable attention and relevant and adequate mental health services should be provided.
Consistent with the findings of a systematic review covering 45 studies [
37], the three-factor DASS model exhibited the best fit and provided a better model fit than other proposed models, hence supporting Hypothesis 1. This implies that among Chinese young people, the construct of psychological morbidity can be well distinguished by three dimensions: depression, anxiety, and stress. The good psychometric properties of the DASS demonstrate that this scale can measure psychological morbidity in an objective manner in a Chinese context.
In line with previous studies (e.g., [
60]), both the measurement and structural invariance across gender were established in this study. This study demonstrates the configural, metric, scalar, error variance, and factor variance invariance across gender in a Chinese sample, suggesting that the DASS-21 is an appropriate instrument to measure the same constructs of depression, anxiety, and stress across gender. Hypothesis 2a was supported. Male and female university students conceptualize and interpret the three dimensions of psychological distress in a similar way. The findings suggest that the DASS-21 will not be affected by gender in a non-clinical setting, and gender differences are due to a true difference in the construct of psychological distress rather than different psychometric responses to the scale items [
57]. Furthermore, the structural invariance of the DASS across the five different cohorts was also established in this study, suggesting that the factor structure does not change across time. These findings support Hypothesis 2b. Taken as a whole, the present study provides good support for the psychometric properties of the DASS in university students in Hong Kong. It is noteworthy that the analyses used in this study are consistent with those reported in the field [
41,
42,
43,
61,
62].
Regarding the socio-demographic correlates of the DASS, we found that male university students displayed significantly more depression, anxiety, and stress symptoms than did female university students which provides support for Hypothesis 3. These findings are in line with the existing literature [
9]. As social norms discourage males from openly expressing negative internal emotions and psychological distress [
63], this may explain the relatively higher psychological morbidity in male students. A meta-analysis with 205 studies [
64] indicated that, compared with females, males seem to feel more obliged to hide their inner thoughts and experiences and therefore tend to do so. The low level of emotional disclosure and the lower level of support-seeking among males may also explain why males are more depressed than females.
In contrast to most existing studies (e.g., [
6]) but consistent with very few studies (e.g., [
65]), male students were found to have a higher level of anxiety than their female counterparts. Males are found to be more anxious than females when it comes to learning and examinations [
65]. This may explain why males would feel more anxious than females in a university context where learning and taking examinations are the most important and major duties for students.
Finally, we also found that the male university students exhibited a higher level of stress than their female counterparts. In Hong Kong, there are more males (67.5%) than females (55%) in the labor market [
66] because males are expected to take more responsibility for earning money and supporting their families in Chinese society [
67]. Thus, male university students may worry more about their future careers after graduation and suffer more stress than their female peers. Although males have shown significantly more depression, anxiety, and stress than females, evidence has shown that compared with females, males tend to solve their emotional problems themselves and to use fewer mental health services [
6,
7,
68,
69]. Therefore, we should pay more attention to promoting the mental health of male university students.
Consistent with Hypothesis 4, we found that psychological morbidity escalated after 2014 (i.e., occurrence of a political event). Although we found no significant changes in psychological morbidity between the 2015/16 and 2018/19 academic years, the depression, anxiety, and stress of university students increased year by year, and psychological morbidity reported by students in 2018 was significantly higher than that reported in 2014. This trend of increasing levels of psychological morbidity among university students may reflect the social instability in Hong Kong during the past few years. An important turning point in Hong Kong’s social life was the civil disobedience campaign “Umbrella Movement”, which took place in 2014. In an investigation based on a population-representative sample of 1,208 Hong Kong people in 2015 [
16], Hou et al. revealed that in 2015, Hong Kong citizens experienced significantly higher levels of depression and anxiety than they did in 2003 [
70] and 2011 [
71]. Ni et al. [
72] also found that major depression increased by 7% in Hong Kong adults after the Umbrella Movement. This suggests that young people in Hong Kong have been suffering more and more psychological distress since 2014. Existing studies (e.g., [
18,
73]) found that stressful life events, such as social movements, make people depressed, and politics may have become a regular and persistent risk factor that negatively affects mental health [
74]. Therefore, timely intervention on the psychological morbidity of university students in connection with political events in Hong Kong is required. In view of the paucity of research on the experience of political events and psychological morbidity in university students in Hong Kong, this study is a valuable contribution to the limited literature.
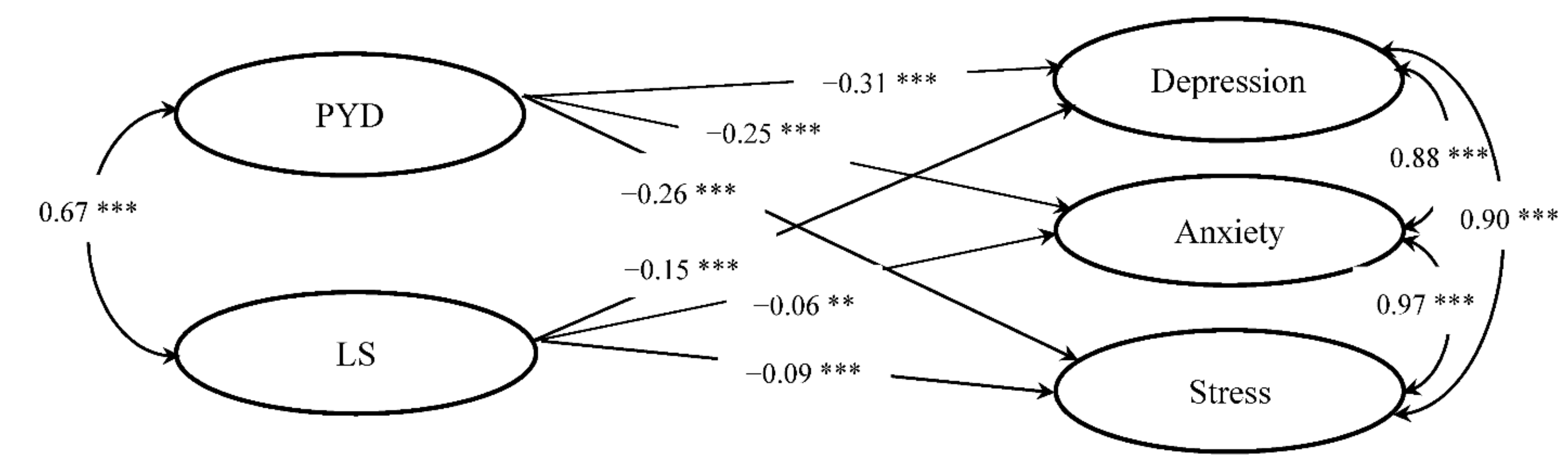
As expected, PYD as an indicator of eudaimonic well-being, Martela and Sheldon [
32] showed significant and negative impacts on the three factors of psychological distress in our samples. This finding can be supported by existing studies that have demonstrated that good PYD can relieve individuals’ psychological distress (e.g., [
44,
45,
75,
76]). PYD is able to nurture youth mental health and encourage young people to make positive changes in multiple domains of their life to prevent behavioral and emotional problems [
77]. Consistent with previous studies (e.g., [
46,
78]), we also found that life satisfaction as an indicator of hedonic well-being has significant negative impacts on depression, anxiety, and stress. As people with higher levels of life satisfaction may have positive values and are more resistant to mental health disorders, life satisfaction is an important factor in protecting individuals’ mental health [
33]. Life satisfaction can help people to maintain positive mental functioning by enhancing internal motivation in stressful situations, while a low level of life satisfaction is a major risk factor for mental health problems, such as depression [
79]. In short, the findings provide support for Hypotheses 5a and 5b that both eudaimonic and hedonic well-being are important correlates of psychological morbidity in young people. Promoting PYD and increasing life satisfaction deserve the attention of researchers and should be taken into account when combating mental health problems in young people.
Five limitations should be acknowledged and addressed in future work. First, although the sample size in the present study was large, all respondents were from the same university. The findings cannot be generalized to all university students in Hong Kong, and need to be replicated in other universities in Hong Kong to avoid sampling bias. Moreover, one should be careful not to generalize the findings in this study to Western society, due to potential significant language effects when measuring psychological distress [
80]. Second, multiple variables could be related to mental health problems, such as psychological factors, environmental factors, temperamental characteristics, and coping strategies [
81]. However, we only tested gender, political event, and well-being correlates with mental health problems in this study. The association between different factors and mental health problems should be examined in the future. Third, we did not have data for other age groups (e.g., children and elders) and clinical samples. In the future, furthe exploration of psychological morbidity across different age groups and different populations is necessary. Fourth, although we recruited five cohorts of university students in this study, this study is essentially a cross-sectional investigation, which only allows us to understand associations, not causality, between well-being correlates and psychological mobility. A longitudinal study would be helpful to reveal the causal relationships amongst the variables under investigation. Last but not least, we did not test psychological distress in the 2019/20 academic year that could reflect the mental health of young people after the social unrest in Hong Kong. Future work would benefit from examining students’ mental health after the social unrest in 2019 as many young students were involved in this unrest and social dysfunction would influence young people [
82]. With the emergence of COVID-19 in 2020, systematic studies on the quality of life of university students are also indispensable [
83,
84].






{kind=link}
{kind=link}