
Prioritising Risk Factors for Prescription Drug Overdose among Older Adults in South Korea: A Multi-Method Study


Abstract
:1. Introduction
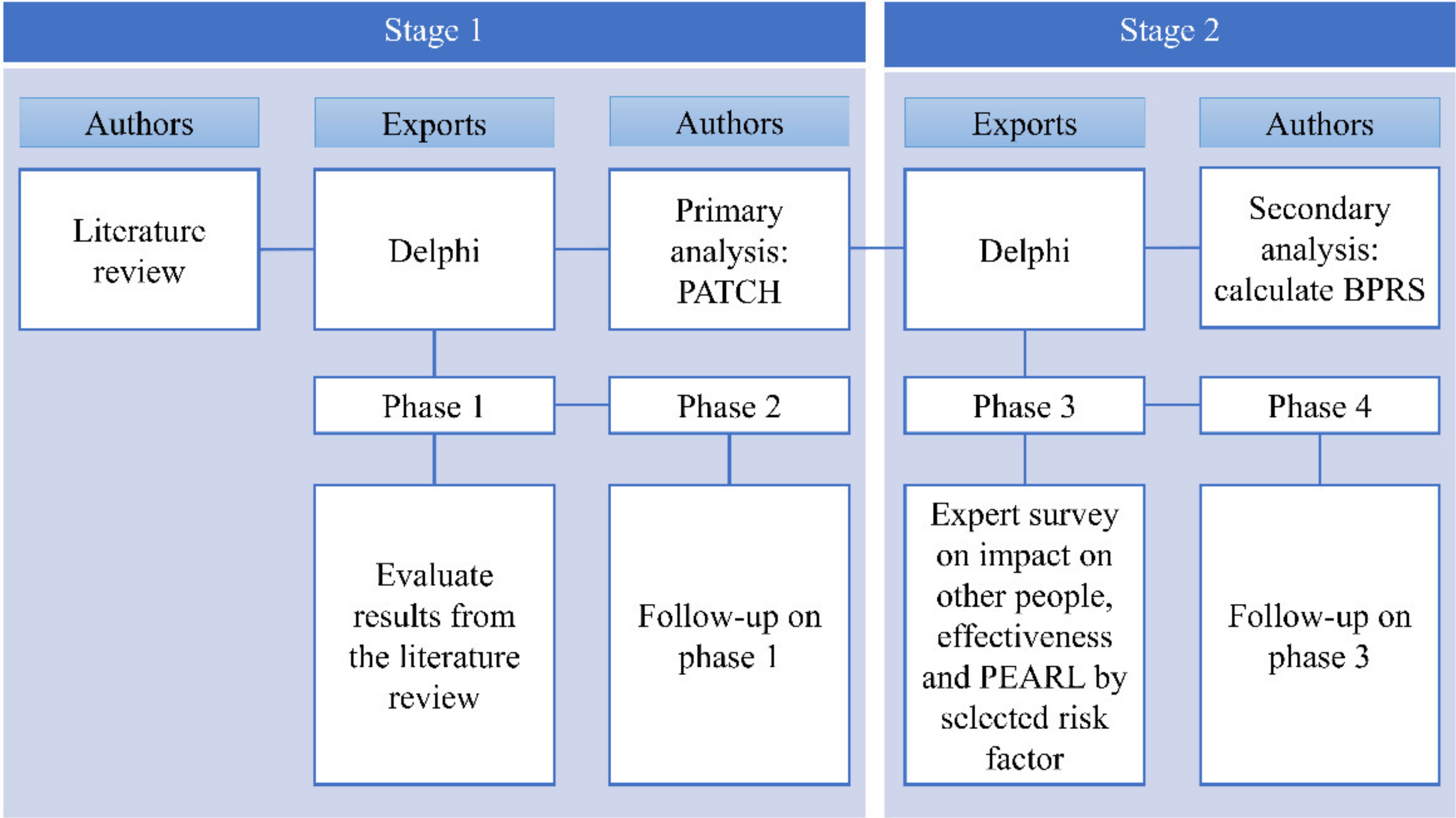
2. Materials and Methods
2.1. Stage 1: Primary Selection of Target Risk Factors for Prioritising
2.1.1. Expert Panel
2.1.2. Definition of Agreement on Delphi
2.2. Stage 2: Prioritisation by the BPRS
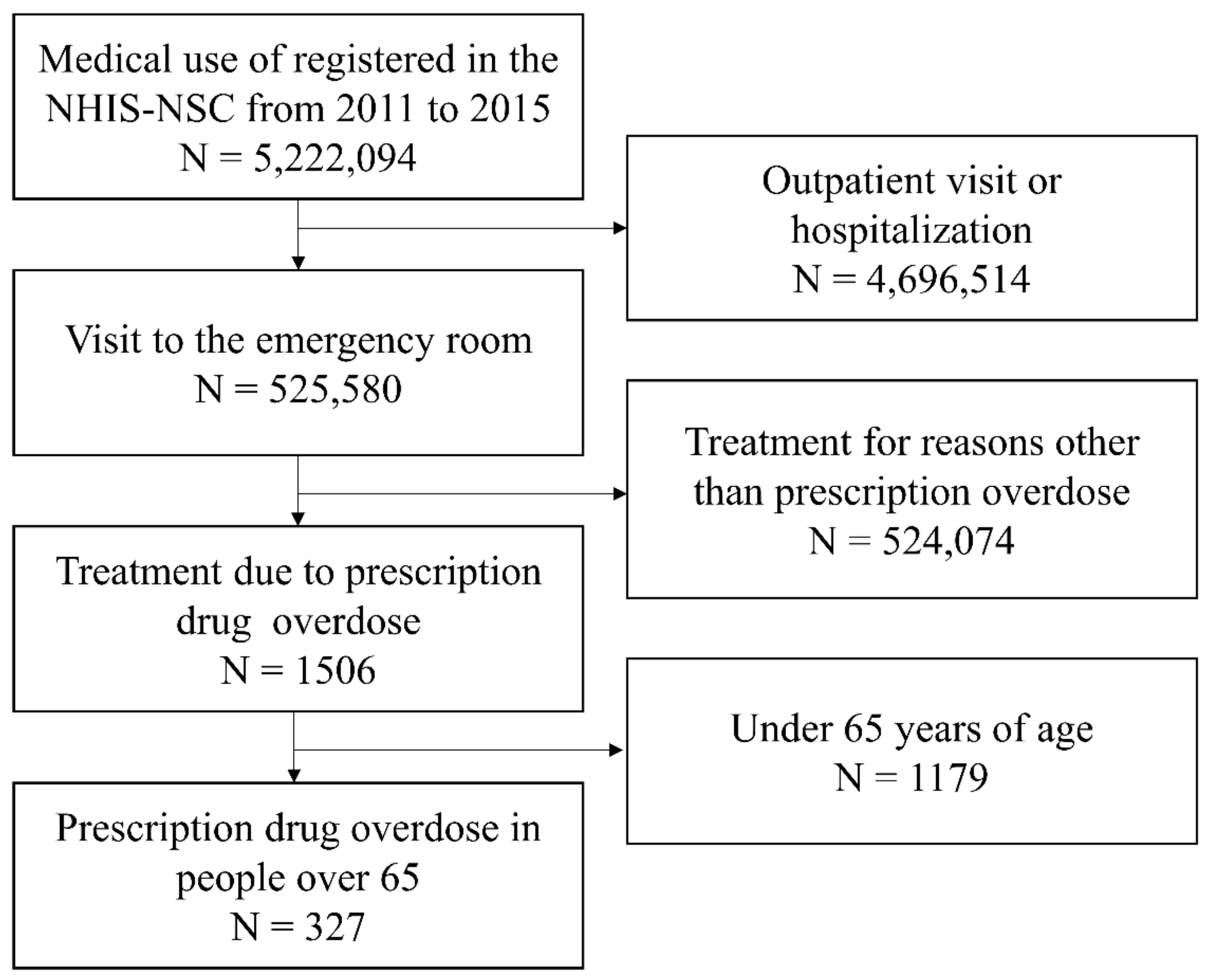
2.2.1. Data Sources
2.2.2. Variable
2.2.3. Definition of Criterion and Scores
2.3. Ethics
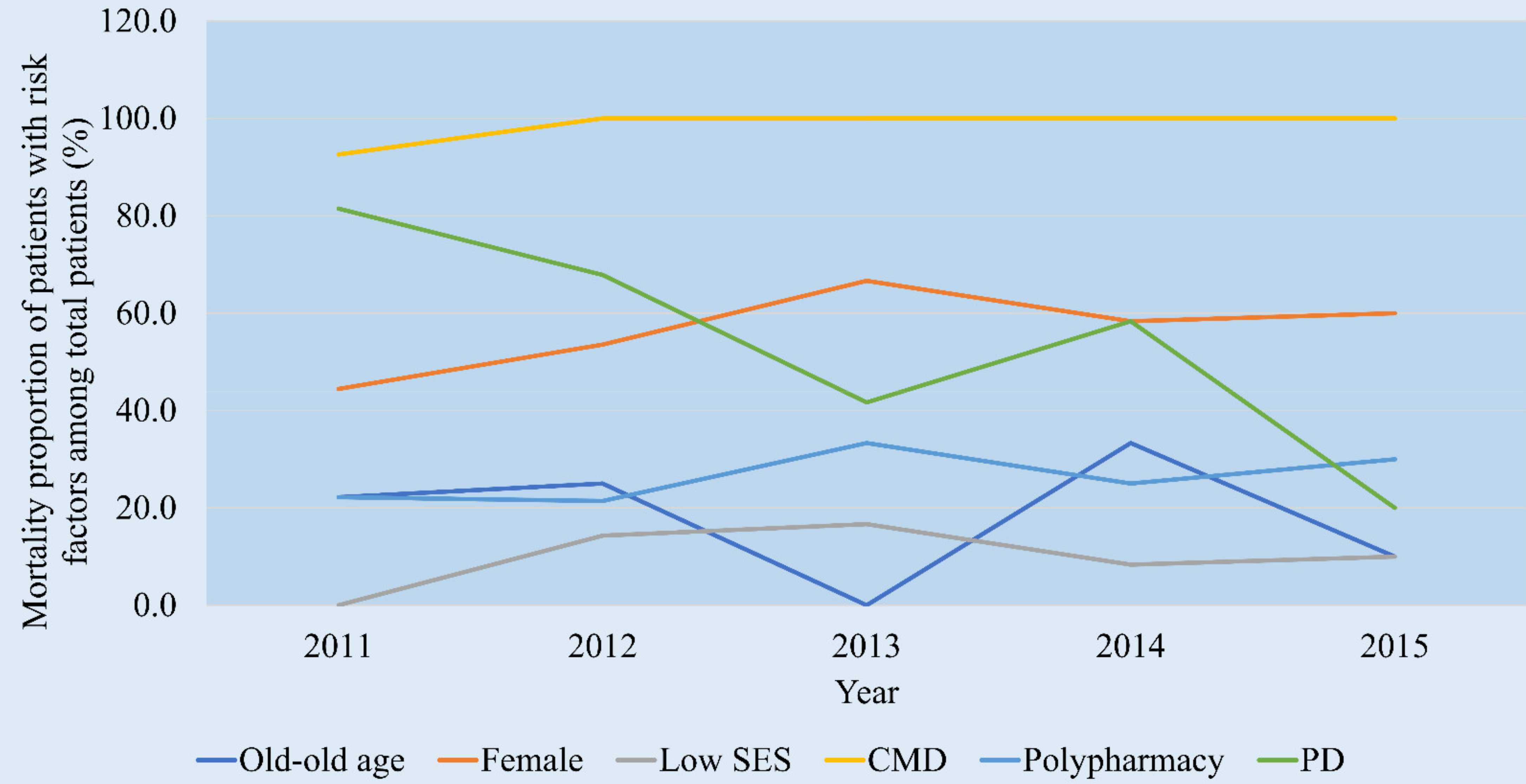
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hedegaard, H.; Miniño, A.M.; Warner, M. Urban-rural differences in drug overdose death rates, by sex, age, and type of drugs involved, 2017. NCHS Data Brief. 2019, 345, 1–8. [Google Scholar]
- Hedegaard, H.; Miniño, A.M.; Warner, M. Drug overdose deaths in the United States, 1999–2017. NCHS Data Brief. 2018, 329, 1–8. [Google Scholar]
- The Lancet. The lethal burden of drug overdose. Lancet 2013, 382, 833. [Google Scholar] [CrossRef]
- Mahase, E. Drug deaths: England and Wales see highest number since records began. BMJ 2020, 371, m3988. [Google Scholar] [CrossRef]
- Kim, W.; Kim, K.H.; Shin, D.W.; Park, J.; Kim, H. Characteristics of Korean poisoning patients: Retrospective analysis by national emergency department information system. J. Korean Soc. Clin. Toxicol. 2019, 17, 108–117. [Google Scholar]
- Koh, J.; Jeon, W.; Kang, H.; Kim, Y.W.; Kim, H. Analysis of poisoning patients using 2017-based injury in-depth surveillance data. J. Korean Soc. Clin. Toxicol. 2019, 18, 85–93. [Google Scholar]
- Anatharaju, A.; Feller, A.; Chedid, A. Aging liver. A review. Gerontology 2002, 48, 343–353. [Google Scholar] [CrossRef]
- Mangoni, A.A.; Jackson, S.H.D. Age-related changes in pharmacokinetics and pharmacodynamics: Basic principles and practical applications. Br. J. Clin. Pharmacol. 2004, 57, 6–14. [Google Scholar] [CrossRef] [Green Version]
- Sönnerstam, E.; Sjölander, M.; Gustafsson, M. Inappropriate prescription and renal function among older patients with cognitive impairment. Drugs Aging 2016, 33, 889–899. [Google Scholar] [CrossRef] [Green Version]
- Bories, M.; Bouzillé, G.; Cuggia, M.; Le Corre, P. Drug-drug interactions in elderly patients with potentially inappropriate medications in primary care, nursing home and hospital settings: A systematic review and a preliminary study. Pharmaceutics 2021, 13, 266. [Google Scholar] [CrossRef]
- Terwindt, F.; Rajan, D.; Soucat, A. Priority-Setting for National Health Policies, Strategies and Plans, Strategizing National Health in the 21st Century: A Handbook; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- Hesse-Biber, S.N.; Johnson, R.B. (Eds.) The Oxford Handbook of Multimethod and Mixed Methods Research Inquiry; Oxford University Press: Oxford, UK, 2015. [Google Scholar] [CrossRef]
- Woodcock, T.; Adeleke, Y.; Goeschel, C.; Pronovost, P.; Dixon-Woods, M. A modified Delphi study to identify the features of high quality measurement plans for healthcare improvement projects. BMC Med. Res. Methodol. 2020, 20, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neiger, B.L.; Thackeray, R.; Fagen, M.C. Basic priority rating model 2.0: Current applications for priority setting in health promotion practice. Health Promot. Pract. 2011, 12, 166–171. [Google Scholar] [CrossRef]
- Green, L.W.; Kreuter, M.W. CDC’s Planned Approach to Community Health as an application of PRECEED and an inspiration for PROCEED. J. Health Educ. 1992, 23, 140–147. [Google Scholar] [CrossRef]
- World Health Organization. Strategizing National Health in the 21st Century: A Handbook; World Health Organization: Geneva, Switzerland, 2016; Available online: https://apps.who.int/iris/handle/10665/250221 (accessed on 18 March 2021).
- Lee, J.; Lee, J.S.; Park, S.-H.; Shin, S.A.; Kim, K. Cohort profile: The National Health Insurance Service-National Sample Cohort (NHIS-NSC), South Korea. Int. J. Epidemiol. 2017, 46, e15. [Google Scholar] [CrossRef] [PubMed]
- Seong, S.C.; Kim, Y.-Y.; Park, S.K.; Khang, Y.H.; Kim, H.C.; Park, J.H.; Kang, H.J.; Do, C.H.; Song, J.S.; Lee, E.J.; et al. Cohort profile: The National Health Insurance Service-National Health Screening Cohort (NHIS-HEALS) in Korea. BMJ Open 2017, 7, e016640. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen-Mansfield, J.; Shmotkin, D.; Blumstein, Z.; Shorek, A.; Eyal, N.; Hazan, H. The old, old-old, and the oldest old: Continuation or distinct categories? An examination of the relationship between age and changes in health, function, and wellbeing. Int. J. Aging Hum. Dev. 2013, 77, 37–57. [Google Scholar] [CrossRef] [PubMed]
- Tang, Y.; Zhang, L.; Pan, J.; Zhang, Q.; He, T.; Wu, Z.; Zhan, J.; Li, Q. Unintentional poisoning in china, 1990 to 2015: The Global Burden of Disease Study 2015. Am. J. Public Health 2017, 107, 1311–1315. [Google Scholar] [CrossRef]
- Klein-Schwartz, W.; Oderda, G.M. Poisoning in the elderly. Epidemiological, clinical and management considerations. Drugs Aging 1991, 1, 67–89. [Google Scholar] [CrossRef]
- Gurwitz, J.H.; Field, T.S.; Judge, J.; Rochon, P.; Harrold, L.R.; Cadoret, C.; Lee, M.; White, K.; LaPrino, J.; Erramuspe-Mainard, J.; et al. The incidence of adverse drug events in two large academic long-term care facilities. Am. J. Med. 2005, 118, 251–258. [Google Scholar] [CrossRef]
- Rawle, M.J.; Cooper, R.; Kuh, D.; Richards, M. Associations between polypharmacy and cognitive and physical capability: A British birth cohort study. J. Am. Geriatr. Soc. 2018, 66, 916–923. [Google Scholar] [CrossRef] [Green Version]
- Atkin, P.A.; Veitch, P.C.; Veitch, E.M.; Ogle, S. The epidemiology of serious adverse drug reactions among the elderly. Drugs Aging 1999, 14, 141–152. [Google Scholar] [CrossRef]
- Creswell, J.W.; Plano Clark, V.L. Designing and conducting mixed methods research. Aust. N. Z. J. Public Health 2007, 31, 388. [Google Scholar] [CrossRef]
- Tashakkori, A.; Teddlie, C. Quality of inferences in mixed methods research: Calling for an integrative framework. In Advances in Mixed Methods Research; Bergman, M.M., Ed.; SAGE: London, UK, 2008. [Google Scholar]
- Hilmer, S.N.; Gnjidic, D.; Le Couteur, D.G. Thinking through the medication list—Appropriate prescribing and deprescribing in robust and frail older patients. Aust. Fam. Physician 2012, 41, 924–928. [Google Scholar]
- Oscanoa, T.J.; Lizaraso, F.; Carvajal, A. Hospital admissions due to adverse drug reactions in the elderly. A meta-analysis. Eur. J. Clin. Pharmacol. 2017, 73, 759–770. [Google Scholar] [CrossRef]
- Zanaty, A.W.; Elagamy, S.E. Retrospective study of acute poisoning in elderly cases admitted to menoufia poisoning control center (mpcc), menoufia university hospitals from 2012 to 2014. Egypt J. Forensic Sci. Appl. Toxicol. 2016, 16, 113–140. [Google Scholar] [CrossRef] [Green Version]
- Qato, D.M.; Wilder, J.; Schumm, L.P.; Gillet, V.; Alexander, G.C. Changes in prescription and over-the-counter medication and dietary supplement use among older adults in the United States, 2005 vs 2011. JAMA Intern. Med. 2016, 176, 473–482. [Google Scholar] [CrossRef]
- Tinetti, M.E.; Bogardus, S.T.; Agostini, J.V. Potential pitfalls of disease-specific guidelines for patients with multiple conditions. N. Engl. J. Med. 2004, 351, 2870–2874. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nightingale, G.; Hajjar, E.; Swartz, K.; Andrel-Sendecki, J.; Chapman, A. Evaluation of a pharmacist-led medication assessment used to identify prevalence of and associations with polypharmacy and potentially inappropriate medication use among ambulatory senior adults with cancer. J. Clin. Oncol. 2015, 33, 1453–1459. [Google Scholar] [CrossRef] [PubMed]
- Cadogan, C.A.; Ryan, C.; Hughes, C.M. Appropriate polypharmacy and medicine safety: When many is not too many. Drug Saf. 2016, 39, 109–116. [Google Scholar] [CrossRef] [Green Version]
- Campanelli, C.M. By the American Geriatrics Society 2015 Beers Criteria Update Expert Panel. American Geriatrics Society 2015 updated Beers Criteria for potentially inappropriate medication use in older adults. J. Am. Geriatr. Soc. 2015, 63, 2227–2246. [Google Scholar]
- Patterson, S.M.; Hughes, C.; Kerse, N.; Cardwell, C.R.; Bradley, M.C. Interventions to improve the appropriate use of polypharmacy for older people. Cochrane Database Syst. Rev. 2012, 5, CD008165. [Google Scholar] [CrossRef] [Green Version]
- Bohnert, A.S.B.; Ilgen, M.A.; Ignacio, R.V.; McCarthy, J.F.; Valenstein, M.; Blow, F.C. Risk of death from accidental overdose associated with psychiatric and substance use disorders. Am. J. Psychiatry 2012, 169, 64–70. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, R.J.; Harvey, L.A.; Brodaty, H.; Draper, B.; Close, J.C. Dementia and intentional and unintentional poisoning in older people: A 10-year review of hospitalization records in New South Wales, Australia. Int. Psychogeriatr. 2015, 27, 1757–1768. [Google Scholar] [CrossRef]
- Balmert, L.C.; Buchanich, J.M.; Pringle, J.L.; Williams, K.E.; Burke, D.S.; Marsh, G.M. Patterns and trends in accidental poisoning deaths: Pennsylvania’s experience 1979–2014. PLoS ONE 2016, 11, e0151655. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Size | Seriousness | Effectiveness of Intervention | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Urgency | Severity | Economic Cost | Impact on Others | |||||||||
| Indicator | Proportion of patients with drug overdose who have the relevant risk factors (%) | Trend of 5-year mortality in patients with risk factors | Admission rate to the intensive care unit for patients with this risk factor (%) | Medical expenses owing to drug overdose in patients with the relevant risk factors (1000 won) | Expert opinion (Likert 5 scale) | Expert opinion (score out of 10) | ||||||
| Score range | 1–10 | 1–5 | 1–5 | 1–5 | 1–5 | 1–10 | ||||||
| Distribution of score | ~10 10~20 20~30 30~40 40~50 50~60 60~70 70~80 80~90 90~100 | 1 2 3 4 5 6 7 8 9 10 | Decreasing Stabilising Increasing | 1 3 5 | 20 20–40 40–60 60–80 80–100 | 1 2 3 4 5 | <1000 1000–1200 1200–1400 1400–1600 >1600 | 1 2 3 4 5 | No affect Minor affect Neutral Moderate affect Major affect | 1 2 3 4 5 | No effective Neutral Extremely effective | 1 2 3 4 5 6 7 8 9 10 |
| Data source | NHIS-NSC | NHIS-NSC | NHIS-NSC | NHIS-NSC | Delphi | Delphi | ||||||
| N (%) | |
|---|---|
| Sex | |
| Female | 4 (22.2) |
| Male | 14 (77.8) |
| Age (years), median (IQR) | 44.5 (38–57) |
| Professions | |
| Emergency physician | 15 (83.3) |
| Professor in the injury prevention research institute | 3 (16.7) |
| Career in injury surveillance and prevention (year), median (IQR) | 10 (5–25) |
| Setting Priorities | ||
|---|---|---|
| More Important | Less Important | |
| More changeable | Polypharmacy | |
| Less changeable | Old-old age Female Chronic medical disease Low SES Psychiatric disease | Social isolation Physical disabilities/reduced mobility Chronic pain History of alcohol problem Transitions in care/living situations |
| Size (%) | Seriousness | Effectiveness of Intervention (Median, IQR) | ||||
|---|---|---|---|---|---|---|
| Urgency | Severity (%) | Economic Cost (won) | Impact on Others (Median, IQR) | |||
| Old-old | 12.8 | Stabilising | 16.2 | 1,396,531 | 1 (1–3) | 7 (5–9) |
| Female | 56.6 | Stabilising | 51.5 | 1,384,519 | 3 (1–3) | 6 (3–6) |
| Low SES | 10.1 | Increasing | 4.0 | 1,647,413 | 5 (3–5) | 8 (3–9) |
| Chronic medical disease | 93.9 | Stabilising | 94.9 | 1,446,485 | 5 (1–5) | 9 (7–10) |
| Polypharmacy | 78.3 | Stabilising | 72.7 | 1,353,738 | 4 (3–5) | 10 (7–10) |
| Psychiatric disease | 76.1 | Decreasing | 70.7 | 1,135,366 | 3 (1–5) | 8 (6–10) |
| Risk Factor | Size | Seriousness | Effectiveness of Intervention | P | E | A | R | L | Total BPRS | Rank |
|---|---|---|---|---|---|---|---|---|---|---|
| Chronic medical disease | 9 | 3 + 5 + 4 + 5 = 17 | 9 | 1 | 1 | 1 | 1 | 1 | 78 | 1 |
| Polypharmacy | 7 | 3 + 4 + 3 + 4 = 14 | 10 | 1 | 1 | 1 | 1 | 1 | 70 | 2 |
| Psychiatric disease | 7 | 1 + 4 + 2 + 3 = 10 | 8 | 1 | 1 | 1 | 1 | 1 | 45 | 3 |
| Low SES | 1 | 5 + 1 + 5 + 5 = 16 | 8 | 1 | 1 | 1 | 1 | 1 | 45 | 3 |
| Female | 5 | 3 + 3 + 3 + 3 = 12 | 6 | 1 | 1 | 1 | 1 | 1 | 34 | 5 |
| Old-old age | 1 | 3 + 1 + 3 + 1 = 8 | 7 | 1 | 1 | 1 | 1 | 1 | 21 | 6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, E.-H.; Park, J.-O.; Cho, J.-P.; Lee, C.-A. Prioritising Risk Factors for Prescription Drug Overdose among Older Adults in South Korea: A Multi-Method Study. Int. J. Environ. Res. Public Health 2021, 18, 5948. https://doi.org/10.3390/ijerph18115948
Lee E-H, Park J-O, Cho J-P, Lee C-A. Prioritising Risk Factors for Prescription Drug Overdose among Older Adults in South Korea: A Multi-Method Study. International Journal of Environmental Research and Public Health. 2021; 18(11):5948. https://doi.org/10.3390/ijerph18115948
Chicago/Turabian StyleLee, Eun-Hae, Ju-Ok Park, Joon-Pil Cho, and Choung-Ah Lee. 2021. "Prioritising Risk Factors for Prescription Drug Overdose among Older Adults in South Korea: A Multi-Method Study" International Journal of Environmental Research and Public Health 18, no. 11: 5948. https://doi.org/10.3390/ijerph18115948