
Instruments to Assess Physical Activity in Primary Education Students with Autism Spectrum Disorder: A Systematic Review

 , , and
, , and
Abstract
:1. Introduction
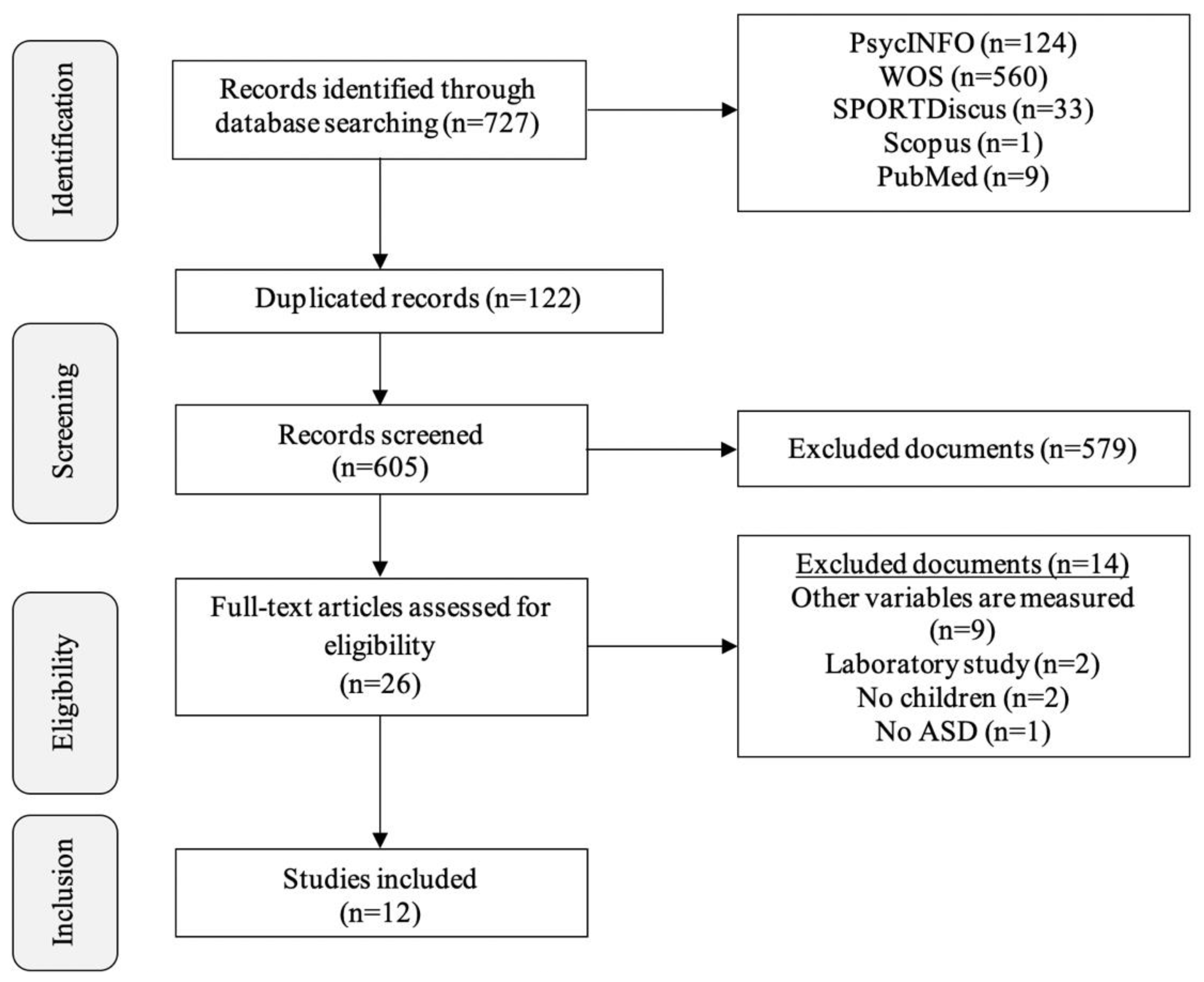
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion Criteria
3. Results
3.1. Summary of the Studies Included
3.2. Objective Measurement Instruments
3.3. Subjective Measurement Instruments
4. Discussion
4.1. Accelerometer
4.2. Questionnaire
4.3. Physical Activity Levels
4.4. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rissardi, G.G.; Cipullo, J.P.; Moreira, G.; Ciorlia, L.A.; Cesarino, C.; Giollo-Junior, L.T.; Zanesco, A.; Vilela-Martin, J.F. Prevalence of Physical Inactivity and its effects on blood pressure and metabolic parameters in a Brazilian urban population. Int. J. Cardiovasc. Sci. 2018, 31, 594–602. [Google Scholar] [CrossRef]
- World Health Organization. Physical Activity. Available online: https://www.who.int/es/news-room/fact-sheets/detail/physical-activity (accessed on 2 April 2020).
- Gaetano, A. Relationship between physical inactivity and effects on individual health status. J. Phys. Educ. Sport. 2016, 16, 1069–1074. [Google Scholar] [CrossRef]
- González, K.; Fuentes, J.; Márquez, J.L. Physical inactivity, sedentary behavior and chronic diseases. Korean J. Fam. Med. 2017, 38, 111–115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Obesity and Overweight. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 2 April 2020).
- Jones, R.A.; Downing, K.; Rinehart, N.J.; Barnett, L.M.; May, T.; McGillivray, J.A.; Hinkley, T. Physical activity, sedentary behavior and their correlates in children with autism spectrum disorder: A systematic review. PLoS ONE 2017, 12, e0172482. [Google Scholar] [CrossRef]
- American Psychiatric Association. Manual Diagnóstico y Estadístico de los Trastornos Mentales (DSM-V), 5th ed.; Editorial Médica Panamericana: Madrid, Spain, 2014. [Google Scholar]
- Baio, J.; Wiggins, L.; Christensen, D.L.; Menner, M.J.; Daniels, J.; Warren, Z.; Dowling, N.F. Prevalence of autism spectrum disorder among children aged 8 years- Autism and developmental disabilities monitoring network, 11 sites, United States, 2014. MMWR. Surveill. Summ. 2018, 67, 1–23. [Google Scholar] [CrossRef] [PubMed]
- Srinivasan, S.M.; Pescatello, L.S.; Bhat, A.N. Current perspectives on physical activity and exercise recommendations for children and adolescents with autism spectrum disorders. Phys. Ther. 2014, 94, 875–889. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, C.; Wong, S.; Lo, F.; So, R.; Chan, D. Study protocol: A randomized controlled trial study on the effect of a game-based exercise training program on promoting physical fitness and mental health in children with autism spectrum disorder. BMC Psychiatry 2018, 18, 56–65. [Google Scholar] [CrossRef] [Green Version]
- Hill, A.P.; Zuckerman, K.E.; Fombonne, E. Obesity and Autism. Pediatrics 2015, 136, 1051–1061. [Google Scholar] [CrossRef] [Green Version]
- Golden, D.; Getchell, N. Physical activity levels in children with and without autism spectrum disorder when playing active and sedentary Xbox Kinect videogames. Games Health J. 2017, 6, 97–103. [Google Scholar] [CrossRef]
- Memari, A.H.; Mirfazeli, F.S.; Kordi, R.; Shayestehfar, M.; Moshayedi, P.; Mansournia, M.A. Cognitive and social functioning are connected to physical activity behavior in children with autism spectrum disorder. Res. Autism Spectr. Disord. 2017, 33, 21–28. [Google Scholar] [CrossRef]
- Nalbant, S. Effects of participation in inclusive physical activity on social skills of individuals with autism spectrum disorder. J. Educ. Train Stud. 2018, 6, 255–261. [Google Scholar] [CrossRef] [Green Version]
- Liu, T.; Fedak, A.T.; Hamilton, M. Effect of physical activity on the stereotypic behaviors of children with autism spectrum disorder. Int. J. Sch. Health. 2016, 3, 17–22. [Google Scholar] [CrossRef]
- Bo, J.; Pang, Y.; Dong, L.; Xing, Y.; Xiang, Y.; Zhang, M.; Wright, M.; Shen, B. Brief report: Does social functioning moderate the motor outcomes of a physical activity program for children with autism spectrum disorders—A pilot study. J. Autism Dev. Disord. 2019, 49, 415–421. [Google Scholar] [CrossRef] [PubMed]
- Pan, C.Y.; Chu, C.H.; Tsai, C.L.; Sung, M.C.; Huang, C.Y.; Ma, W.Y. The impacts of physical activity intervention on physical and cognitive outcomes in children with autism spectrum disorder. Autism 2016, 21, 190–202. [Google Scholar] [CrossRef]
- Godard, C.; Carlín, L.; Torres, J.; Rodríguez, M.P.; Leyton, B.; Salazar, G. Nivel de intensidad de las principales actividades físicas de escolares chilenos: Determinación por acelerometría. Rev. Chil. Nut. 2016, 43, 247–254. [Google Scholar] [CrossRef] [Green Version]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, F.P.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- Pan, C.Y. Objectively measured physical activity between children with Autism Spectrum Disorders and children without disabilities during inclusive recess setting in Taiwan. J. Autism Dev. Disord. 2008, 38, 1292–1301. [Google Scholar] [CrossRef]
- Memari, A.H.; Ghaheri, B.; Ziaee, V.; Kordi, R.; Hafizi, S.; Moshayedi, P. Physical activity in children and adolescents with autism assessed by triaxial accelerometry. Pediatric Obes. 2012, 8, 150–158. [Google Scholar] [CrossRef]
- Hinckson, E.A.; Dickinson, A.M.; Water, T.; Sands, M.; Penman, L. Physical activity, dietary habits and overall health in overweight and obese children and youth with intellectual disability or autism. Res. Dev. Disabil. 2013, 34, 1170–1178. [Google Scholar] [CrossRef]
- Tyler, K.; MacDonald, M.; Menear, K. Physical activity and physical fitness of school-aged children and youth with autism spectrum disorders. Autism Res. Treat. 2014, 2014, 312163. [Google Scholar] [CrossRef]
- Memari, A.H.; Panahi, N.; Ranjbar, N.; Moshayedi, P.; Shafiei, M.; Kordi, R.; Ziaee, V. Children with autism spectrum disorder and patterns of participation in daily physical and play activities. Neurol. Res. Int. 2015, 531906. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Must, A.; Phillips, S.M.; Carol, C.; Bandini, L.G. Barriers to physical activity in children with autism spectrum disorders: Relationship to physical activity and screen time. J. Phys. Act. Health 2015, 12, 529–534. [Google Scholar] [CrossRef] [Green Version]
- Haegele, J.A.; Zhu, X.; Kirk, T.N. Weekday physical activity and health-related fitness of youths with Visual Impairments and those with Autism Spectrum Disorder and Visual Impairments. J. Vis. Impair. Blind. 2018, 112, 372–384. [Google Scholar] [CrossRef]
- Bricout, V.A.; Pace, M.; Dumortier, L.; Baillieul, F.; Favre-Juvin, A.; Guinot, M. Reduced cardiorespiratory capacity in children with Autism Spectrum Disorders. J. Clin. Med. 2018, 7, 361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Healy, S.; García, J.M. Psychosocial correlates of physical activity participation and screen-time in typically developing children and children on the autism spectrum. J. Dev. Phys. Disabil. 2018, 31, 313–328. [Google Scholar] [CrossRef]
- Woodman, A.C.; Breviglia, E.; Mori, Y.; Golden, R.; Maina, J.; Wisniewski, H. The effect of music on exercise intensity among children with Autism Spectrum Disorder: A pilot study. J. Clin. Med. 2018, 7, 38. [Google Scholar] [CrossRef] [Green Version]
- Garcia, J.M.; Leahy, N.; Rivera, P.; Renziehausen, J.; Samuels, J.; Fukuda, D.H.; Stout, J.R. Brief report: Preliminary efficacy of a judo program to promote participation in physical activity in youth with Autism Spectrum Disorder. J. Autism. Dev. Disord. 2019, 50, 1418–1424. [Google Scholar] [CrossRef]
- Garcia, J.M.; Leahy, N.; Rivera, P.; Brazendale, K.; Rice, D.J. The association among demographic factors, health behaviors and sleep quality in youth with Autism Spectrum Disorder. Disabil. Health J. 2019, 13, 100885. [Google Scholar] [CrossRef]
- Vanhelst, J.; Béghin, L.; Duhamel, A.; Bergman, P.; Sjöström, M.; Gottrand, F. Comparison of uniaxial and triaxial accelerometry in the assessment of physical activity among adolescents under free-living conditions: The HELENA study. BMC Med. Res. Metodol. 2012, 12, 26. [Google Scholar] [CrossRef]
- Plasqui, G.; Westerterp, K.R. Physical activity assessment with accelerometers: An evaluation against doubly labeled water. Obesity 2007, 15, 2371–2379. [Google Scholar] [CrossRef]
- Montoye, A.H.; Moore, R.W.; Bowles, H.R.; Horycinski, R.; Pfeiffer, K.A. Reporting accelerometer methods in physical intervention studies: A systematic review and recommendations for authors. Br. J. Sports Med. 2018, 52, 1507–1516. [Google Scholar] [CrossRef] [PubMed]
- Duncan, M.J.; Roscoe, C.M.; Faghy, M.; Tallis, J.; Eyre, E.L. Estimating physical activity in children aged 8–11 years using accelerometry: Contributions from fundamental movement skills and different accelerometer placements. Front. Physiol. 2019, 10, 242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hauck, J.L.; Ketcheson, L.R.; Ulrich, D.A. Methodology to promote physical activity monitoring adherence in youth with Autism Spectrum Disorder. Front. Public Health 2016, 4, 206. [Google Scholar] [CrossRef] [Green Version]
- Oreskovic, N.M.; Neumeyer, A.M.; Duggan, M.P.; Kuhlthau, K.A. Assessment of walking routes as a possible approach for promoting physical activity in children with Autism Spectrum Disorder: Brief Report. Dev. Neurorehabilit. 2019, 23, 59–63. [Google Scholar] [CrossRef] [PubMed]
- Bender, J.M.; Brownson, R.C.; Elliott, M.B.; Haire-Joshu, D.L. Children´s physical activity: Using accelerometers to validate a parent proxy record. Med. Sci. Sports Exerc. 2005, 37, 1409–1413. [Google Scholar] [CrossRef] [PubMed]
- Jurado-Castro, J.M.; Llorente-Cantarero, F.J.; Gil-Campos, M. Evaluación de la actividad física en niños. Acta Pediatrica Esp. 2019, 77, 94–99. [Google Scholar]
- Cancela-Carral, J.M.; Lago-Ballesteros, J.; Ayán-Pérez, C.; Mosquera-Morono, M.B. Análisis de fiabilidad y validez de tres cuestionarios de autoinforme para valorar la actividad física realizada por adolescentes españoles. Gac. Sanit. 2016, 30, 333–338. [Google Scholar] [CrossRef] [Green Version]
- Voss, C.; Dean, P.H.; Gardner, R.F.; Duncombe, S.L.; Harris, K.C. Validity and reliability of the physical activity questionnaire for children (PAQ-C) and adolescents (PAQ-A) in individuals with congenital heart disease. PLoS ONE 2017, 12, e0175806. [Google Scholar] [CrossRef]
- Hidding, L.M.; Chinapaw, M.J.; Van Poppel, M.N.; Mokkink, L.B.; Altenburg, T.M. An updated systematic review of childhood physical activity questionnaires. Sports Med. 2018, 48, 2797–2842. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Category | Keywords |
|---|---|
| Autism Spectrum Disorder | Ti (ASD OR autism OR autism spectrum disorder) OR Ab (ASD OR autism OR autism spectrum disorder) |
| Physical Activity | Ti (physical activity OR physical exercise OR physical fitness OR physical condition) OR Ab (physical activity OR physical exercise OR physical fitness OR physical condition) |
| Measurement | Ti (assess* OR evaluat* OR measure* OR test* OR instrument assess*) OR Ab (assess* OR evaluat* OR measure* OR test* OR instrument assess*) |
| Population | Ti (primary educat* OR primary school OR elementar* school OR child*) OR Ab (primary educat* OR primary school OR elementar* school OR child*) |
| First Author and Year | Country | Participants | Design, Intervention | Objective | |
|---|---|---|---|---|---|
| Sample | ASD Diagnosis | ||||
| Pan, 2008 [20] | Taiwan | 48 schoolchildren: ASD (23 boys and 1 girl) and Non-ASD (23 boys and 1 girl) aged 7–12 years old (14 schools). | Autism (mild or high functioning, n = 12; moderate, n = 9) and Asperger’s syndrome (n = 3). All without ID or severe behavioural problems. Manifest comorbidities: yes. | Follow-up during the regular school day (5 consecutive days). Periods of interest: school breaks (morning and afternoon). No specific intervention space was needed; the study was carried out in the participants’ environment. | To compare the percentage of time spent by children with and without ASD in moderate-to-high intensity PA during their inclusive school break time. |
| Memari et al., 2012 [21] | Tehran (Iran) | 80 schoolchildren with ASD (52 boys and 28 girls) aged 7 to 14 years old (special schools). Exclusion of 10 students (malfunctioning device, n = 4; invalid data, n = 6). | High-functioning autism (CI > 70) without concomitant ID. Exclusion criteria: orthopaedic dysfunctions, inability to use/accept accelerometers and serious behavioural problems. Manifest comorbidities: yes. | Follow-up during 1 full week (7 days and 7 nights). Two comparisons of special interest: weekend; school day–extracurricular activity hours. | To analyse the patterns of PA in students with ASD, as well as their correlation with factors which may influence their activity levels. |
| Hinckson et al., 2013 [22] | New Zealand | 17 schoolchildren: ASD (6 boys and 1 girl) and ID (4 boys and 6 girls) between 7 and 20 years old (2 special needs centres). All were obese or overweight. | Formal diagnosis of ASD. The degree of severity was not specified. Manifest comorbidities: yes. | School programme of 10 weeks dedicated to PA, nutrition and motivational skills. Data collection before and after the programme and 24 weeks after the interventionPresence and participation of families. | To determine the effectiveness of a PA and nutrition-based programme for weight control in obese schoolchildren with ID or autism. |
| Tyler et al., 2014 [23] | USA | 29 schoolchildren: ASD (9 boys and 8 girls) and Non-ASD (6 boys and 6 girls) between 9 and 17 years old. | Formal diagnosis of ASD. The degree of severity was not specified. Manifest comorbidities: no. | Laboratory environment (diagnostic assessment, anthropometric measurements and assessment of physical fitness) and natural environment of students to measure PA (7 days). | To analyse the physical fitness and PA of schoolchildren with ASD, in comparison with their normotypically developing peers. |
| Memari et al., 2015 [24] | Tehran (Iran) | 83 schoolchildren with ASD (52 boys and 31 girls) between 6 and 15 years old (4 specific schools for autism). | High-functioning autism (IQ > 70). Manifest comorbidities: no. | Family-based intervention aimed at finding out levels of PA practice in leisure time (7 days). | To assess the participation of children with ASD in daily physical activities, and their relationship to a range of factors. |
| Must et al., 2015 [25] | USA | 111 schoolchildren: ASD (53, 83% children) and Non-ASD (58, 78% children) between 3 and 11 years old. | Formal diagnosis of ASD. The degree of severity was not specified. Manifest comorbidities: no. | Cross-sectional study carried out between January 2007 and December 2008. | To compare the prevalence of barriers towards PA among schoolchildren with and without ASD, as well as to assess the association between barriers, PA practice and screen time in children with ASD. |
| Haegele et al., 2018 [26] | USA | 12 schoolchildren: ASD + VI (4 boys and 2 girls) and VI (4 boys and 2 girls) between 8 and 16 years old (school for visually impaired children). | Formal diagnosis of ASD. The degree of severity was not specified. The lack of accuracy when establishing the diagnosis may have prevented learning about additional limitations. Manifest comorbidities: no. | Intervention lasting 1 school week (5 days). PA level was measured during 4 days (Monday to Thursday, 8 h minimum). A physical fitness test was conducted on Friday during the physical education session. | To compare PA and physical fitness among schoolchildren with ASD+VI and those with only VI. |
| Bricout et al., 2018 [27] | France | 40 schoolchildren (all children): ASD (20) and Non-ASD (20) between 8 and 13 years old. | High-functioning autism (CI > 70) without concomitant ID. Exclusion criteria: Contraindication for physical exercise, psychiatric or medical disorders, respiratory disorders and medical treatment. Manifest comorbidities: no. | Laboratory environment (respiratory capacity and physical fitness) and natural environment of students in order to measure PA (7 days). | To examine the cardiorespiratory fitness of children with ASD and compare it with that of normotypically developing schoolchildren. |
| Healy et al., 2018 [28] | Ireland | 110 schoolchildren: ASD (55) and Non-ASD (55) aged 9. Girls represented 15% (n = 8) of both groups. | Formal diagnosis of ASD. The degree of severity was not specified.Manifest comorbidities: no. | Data from a nationally representative cohort study. | To compare the psychosocial factors associated with ASD and screen time between children with and without ASD. |
| Woodman et al., 2018 [29] | USA | 13 schoolchildren with ASD (11 boys and 2 girls) between 5 and 13 years old (public school for students with ASD). | Formal diagnosis of ASD, with concomitant diagnosis of ID. Manifest comorbidities: no. | Jogging programme during 6 consecutive school days. The intensity of PA was analysed in a structured (from 9:50 to 10:25) and unstructured (from 10:25 to 10:45) jogging period, subject to different musical conditions. | To examine the influence of music on exercise intensity in children with ASD by means of a jogging programme. |
| Garcia et al., 2019 [30] | USA | 14 schoolchildren with ASD (12 boys and 2 girls) aged 8 to 17 years old. Exclusion criteria: serious physical limitations and violent behaviour. | Formal diagnosis of ASD. The degree of severity was not specified. Manifest comorbidities: yes. | 8-week Judo Programme to promote PA (summer; 1 session of 45 min per week). | To examine the effectiveness of a judo programme aimed at promoting moderate-to-high intensity PA and reducing sedentary behaviours in children with ASD. |
| Garcia et al., 2019 [31] | USA | 49 ASD schoolchildren (36 boys and 13 girls) aged 8 to 17 (public school for ASD students). Exclusion of 1 student (non-compliance with accelerometer time criteria). | High-functioning autism (IQ > 70). Manifest comorbidities: no. | Follow-up during 1 week (7 days and 7 nights) to analyse the quality and duration of sleep and regular levels of PA. | To compare demographic and lifestyle factors with duration and quality of sleep in children with ASD. |
| First Author and Year | Measurement Instruments | ||||
|---|---|---|---|---|---|
| Main Instruments | Complementary Instruments | Other Instruments | Description | ||
| Objective | Subjective | ||||
| Pan, 2008 [20] | x | - | - | - | Objective instrument: GT1M ActiGraph (uniaxial accelerometer) programmed to collect data at 1-min intervals; tied on the right side of the hip (using an elastic belt). Its use was discontinued at the end of the school day; the data were downloaded immediately and it was restarted the following day. |
| Memari et al., 2012 [21] | x | - | x | - | Objective instrument: GT3X ActiGraph (triaxial accelerometer) programmed to collect data at 1-min intervals; tied on the right side of the hip (using an elastic belt). Complementary instruments: A logbook/log sheet (families and teachers) to record the hours when the device was not used. Questionnaire (families) to measure sedentary behaviour. |
| Hinckson et al., 2013 [22] | - | x | - | x | Subjective instrument: PA questionnaire (MEND) completed by the families. Selection of 2 out of the 4 questions on the MEND: time dedicated to activity/inactivity and time dedicated to moderate-to-high intensity PA. Other instruments: Nutrition questionnaire (14 items) on the frequency of having breakfast, carbonated drinks, white bread, wholemeal cereals, pastries and fresh food. 6-min walk test (6MWT) to assess physical fitness. |
| Tyler et al., 2014 [23] | x | - | x | x | Objective instrument: GTX3 + ActiGraph (triaxial accelerometer, valid for children with ID) tied on the right side of the hip (using an elastic belt). It was used at all times (except under the water and at night). The data collected were reduced to 4 categories (sedentary, low, moderate and moderate-to-high intensity). Complementary instruments: A logbook/log sheet (families) to record the hours when the device was not used. Other instruments: Fitness tests on aerobic capacity, muscle strength and flexibility. |
| Memari et al., 2015 [24] | - | x | x | - | Subjective instrument: PA questionnaire (adapted from GLTEQ) completed by families and teachers Two key topics: intensity and frequency of PA. Complementary instruments: List of barriers (families) against the practice of PA in leisure time. Daily activity journal (families) to know the type of game (individual or social). |
| Must et al., 2015 [25] | - | x | x | - | Subjective instrument: PA questionnaire (CHAMPS) completed by families in order to determine participation in structured and unstructured physical activities (type of activity and frequency). Complementary instruments: Screen time questionnaire (families) to determine the number of hours schoolchildren spent sitting or lying down (TV, video games, computer). Questionnaire on barriers (families) against PA practice (of the person, the family, social, community). |
| Haegele et al., 2018 [26] | x | - | - | x | Objective instrument: GT3X ActiGraph (triaxial accelerometer) that counts the accelerations at a sampling frequency of 30 HZ, tied on the right side of the hip (using an elastic belt). It was used only during the waking state hours and the data were classified into 4 categories (sedentary, low, moderate and high intensity). Other instruments: Fitness test (based on the Brockport test) to measure aerobic resistance, upper body muscle strength, abdominal muscle strength and flexibility. |
| Bricout et al., 2018 [27] | x | x | x | x | Objective instrument: Pro-3 SenseWear (triaxial accelerometer) placed on the triceps with an elastic belt to measure PA. It was used 24 h a day (except when showering or swimming). Subjective instrument: PA Questionnaire (PAQ-C) completed by families and schoolchildren (9 items). PA periods: week–weekend; with or without a teacher. Complementary instruments: A logbook/log sheet (families) to record the hours when the device was not used. Other instruments: EUROFIT battery to measure physical fitness. |
| Healy et al., 2018 [28] | - | x | x | - | Subjective instrument: PA questionnaire (GLTEQ) completed by families (based on the last 14 days; frequency, moderate-to-high or low intensity) and by students (based on the last 7 days; PA practice). Complementary instruments: Screen time questionnaire (families) with 3 variables (TV, computers and video games). |
| Woodman et al., 2018 [29] | x | - | - | - | Objective instrument: Omron activity device (Model HJA-750C; triaxial accelerometer) to measure METs (metabolic equivalent of task) and the percentage of 10-s intervals in high-intensity activity. It was placed on the back of the elastic waistband of school uniforms (so that when swinging the arms did not touch the accelerometer). It was used for 6 days (from 09:15 to 10:45). |
| Garcia et al., 2019 [30] | x | - | - | - | Objective instrument: GT9X ActiGraph (triaxial accelerometer which filters out high-frequency vibrations in order to artificially increase the data) programmed to collect data at 1-min intervals; placed on the non-dominant wrist (7 days). Data collected on the initial day were excluded from the analysis (possible artificial increase in PA). |
| Garcia et al., 2019 [31] | x | - | x | - | Objective instrument: GT9X ActiGraph (triaxial accelerometer) placed on the non-dominant wrist. It was used on a 24-h basis (except during water activities) to measure the quality and duration of sleep and the levels of PA. Complementary instruments: Screen time questionnaire (families) to determine the number of hours schoolchildren spent in sedentary activities (TV, computers, video games; 7-point scale). |
| First Author and Year | Results | Limitations | Conclusions |
|---|---|---|---|
| Pan, 2008 [20] | PA is stable, no group was moderately active for more than 50% of the break time. Schoolchildren without ID spent more time in moderate-to-high intensity PA when compared to students with ASD (36.15% vs. 27.2%). Subgroup ASD/Early primary (1st, 2nd and 3rd) more active than the group ASD/Late primary (4th, 5th and 6th). | Cross-sectional design of the studio. Reduced sample size. Presence of the accelerometer (possible rejection by the students). Data collection in 1-min intervals (possible underestimation of PA in free play). Absence of social, behavioural, cognitive and motor skills assessment (possible biases in the findings). | The lower level of PA in schoolchildren with ASD during breaks suggests that unstructured time during the school day may need to be redesigned for structuring. In order to improve the PA of students with ASD during the breaks, several types of strategies or interventions should be developed. |
| Memari et al., 2012 [21] | Significant differences between age groups and sex for PA (minimum level of PA among 13–14-year-olds and girls). More PA in out-of-school hours than during school No significant changes were found in PA levels comparing weekdays and weekends. | Cross-sectional design of the studio. Absence of a control group with which to compare the results. Homogeneity of the sample (difficulty to generalise the results to the ASD variety). Possible biases in the accelerometer results due to their incompatibility with aquatic activities and to the presence of stereotyped behaviours in schoolchildren with ASD. | The lower level of PA in schoolchildren with ASD during the school day underlines the need to revise school programmes for adapted PA. For a higher level of PA in children with ASD, they should be given PA opportunities according to their socio-demographic profile. |
| Hinckson et al., 2013 [22] | Unclear data, with trivial effects. Children more active after the implementation of the programme. | Reduced sample size. No control group with which to compare the results. Non-validated PA questionnaire for schoolchildren with ID. Winter and summer assessments (possible influence of the climate on PA levels). Absence of quantitative measurements. | A programme specifically designed for the needs of schoolchildren with ID and their families is needed. The programme should focus on healthy living rather than on managing overweight. The school may be the appropriate place to deliver such a programme. Appropriate tools need to be developed to accurately determine PA in young people with ID. |
| Tyler et al., 2014 [23] | Children with ASD are less physically active than their normotypically developing peers (less time in moderate-to-high intensity PA and higher rates of sedentary behaviour). | Uneven sample sizes and unmatched controls. Reduced sample size. Introduction of individual adaptations in the evaluations. | Children with ASD face well-known health disparities, so efforts to promote PA in schools, and through public health initiatives, must include this group. |
| Memari et al., 2015 [24] | Only 10 (12%) schoolchildren were physically active. Only 6% “often” participated in PA, whereas the majority, 85.5%, opted for the “never/rarely” response. Boys were more active than girls and the older they were, the more inactive they became. Preference for playing alone. | Cross-sectional design of the studio. Absence of a control group with which to compare the results. Measures based only on information from families or teachers (possible biases due to subjectivity). | Only a small percentage of children with ASD are physically active, and the financial concerns, lack of opportunities and socio-demographic factors are major constraints on their ASD. |
| Must et al., 2015 [25] | More barriers against PA in schoolchildren with ASD. The total number of barriers was inversely correlated with the number of hours and types of PA, but was directly related to total screen time. | Homogeneous sample (predominantly white and well educated). Exclusive use of qualitative assessment tests (possible subjectivity bias). | PA programmes designed to meet the special requirements of the ASD population and conducted by adults with specialised training are urgently needed. Systematic assessment of such programmes will contribute to the development of best practices regarding PA programming for children with ASD. |
| Haegele et al., 2018 [26] | Sedentary activities are predominant during the week. Non-compliance with the recommendation of 60 daily minutes of moderate-high intensity PA. The ASD/VI group was significantly less active than the VI group. | Reduced sample size. The severity of ASD and associated comorbidities were not recorded, so the presence of additional limitations which could influence PA is unknown. Biases may appear in accelerometer results as they do not record upper body PA. Intervention in a school with many opportunities for PA practice (possible overestimation of results and difficulty to generalise findings). | This study identifies a substantial need for health promotion among young people with ASD and visual impairment, and the results show the need to encourage intervention programmes to help improve these health-related variables. |
| Bricout et al., 2018 [27] | The control group was more physically active than the ASD group (not significant results in any of the tests: accelerometer and questionnaire). | Reduced sample size. Very specific ASD group (CI > 70) and absence of girls in the study (difficulty to generalise results). | The results of the study suggest that children with ASD are in worse physical condition than their peers without ASD. Furthermore, since poor physical condition is a reliable indicator of poor health outcomes, this study provides an important argument for the systematic implementation of PA programmes aimed at young people with ASD. |
| Healy et al., 2018 [28] | The ASD group is less physically active and less involved in sports than the control group. Boys (both groups) are significantly more active and more involved in sports. | The severity of ASD was not recorded (difficulty to generalise results). Exclusive use of qualitative measures (possible biases due to subjectivity). | The association between negative social interactions and lower levels of PA in children with ASD should be examined as well as the social interventions developed among schoolchildren with ASD and their peers in PA settings. |
| Woodman et al., 2018 [29] | Average time spent on intense PA of 16 min/day. More PA levels in the structured period. In general, slower music produced greater PA benefits. The exception was found in schoolchildren with fewer maladaptive behaviours and mild or moderate symptoms of autism, who were more motivated by fast music. | Reduced sample size. Homogeneity of the sample (difficulty to generalise the results to the ASD variety).Unusual daily exercise in the school (possible overestimation of results). Schoolchildren did not participate in the selection of songs (children with ASD may be particularly sensitive to music). | Based on the results of the study, music should be incorporated into physical education programmes for schoolchildren with ASD, as it can motivate this group to participate in PA in order to prevent obesity and other health problems. Additionally, jogging is a low-cost, low-risk intervention which can be easily implemented in an educational setting. |
| Garcia et al., 2019 [30] | The daily time spent in moderate-to-high intensity PA increased significantly after the judo session. After the programme, the number of participants who complied with the recommendations of 60 min of daily PA was increased from 4 to 8 and sedentary behaviours were reduced. | Reduced sample size. Short duration of the intervention (8 weeks). Absence of a control condition (Judo condition was not compared to an inactive condition or to a general exercise class). | The study proved the preliminary effectiveness of the judo programme to promote PA among young people with ASD, finding that 50% of the sample continued to participate in judo or a similar martial arts training after the programme. Further studies are needed to support these findings, but judo programmes could be well received by this group. |
| Garcia et al., 2019 [31] | Children who met the criteria of duration and quality of sleep had more minutes of moderate-to-high intensity PA and less time in sedentary activities.Only 15% of the sample met the sleep criteria. | Cross-sectional design of the studio. Very specific group of ASD (IQ > 70) (difficulty to generalise results). The stereotyped behaviours of schoolchildren with ASD could artificially increase the data collected by the accelerometer. | The results of the study showed the association of healthy lifestyle factors (HF) with longer sleep among young people with ASD. Participants’ compliance with the accelerometer protocol was high (only one participant did not meet the criteria for minimum time of use), suggesting that this method of objectively assessing ASD may be feasible in the ASD population. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
López-Valverde, P.; Rico-Díaz, J.; Barcala-Furelos, M.; Martí-González, M.; Martín, J.L.; López-García, S. Instruments to Assess Physical Activity in Primary Education Students with Autism Spectrum Disorder: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 4913. https://doi.org/10.3390/ijerph18094913
López-Valverde P, Rico-Díaz J, Barcala-Furelos M, Martí-González M, Martín JL, López-García S. Instruments to Assess Physical Activity in Primary Education Students with Autism Spectrum Disorder: A Systematic Review. International Journal of Environmental Research and Public Health. 2021; 18(9):4913. https://doi.org/10.3390/ijerph18094913
Chicago/Turabian StyleLópez-Valverde, Paula, Javier Rico-Díaz, Martín Barcala-Furelos, Mariacarla Martí-González, Juan L. Martín, and Sergio López-García. 2021. "Instruments to Assess Physical Activity in Primary Education Students with Autism Spectrum Disorder: A Systematic Review" International Journal of Environmental Research and Public Health 18, no. 9: 4913. https://doi.org/10.3390/ijerph18094913