
Increased Incidence of Premenstrual Syndrome in Females with Palmar Hyperhidrosis

 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
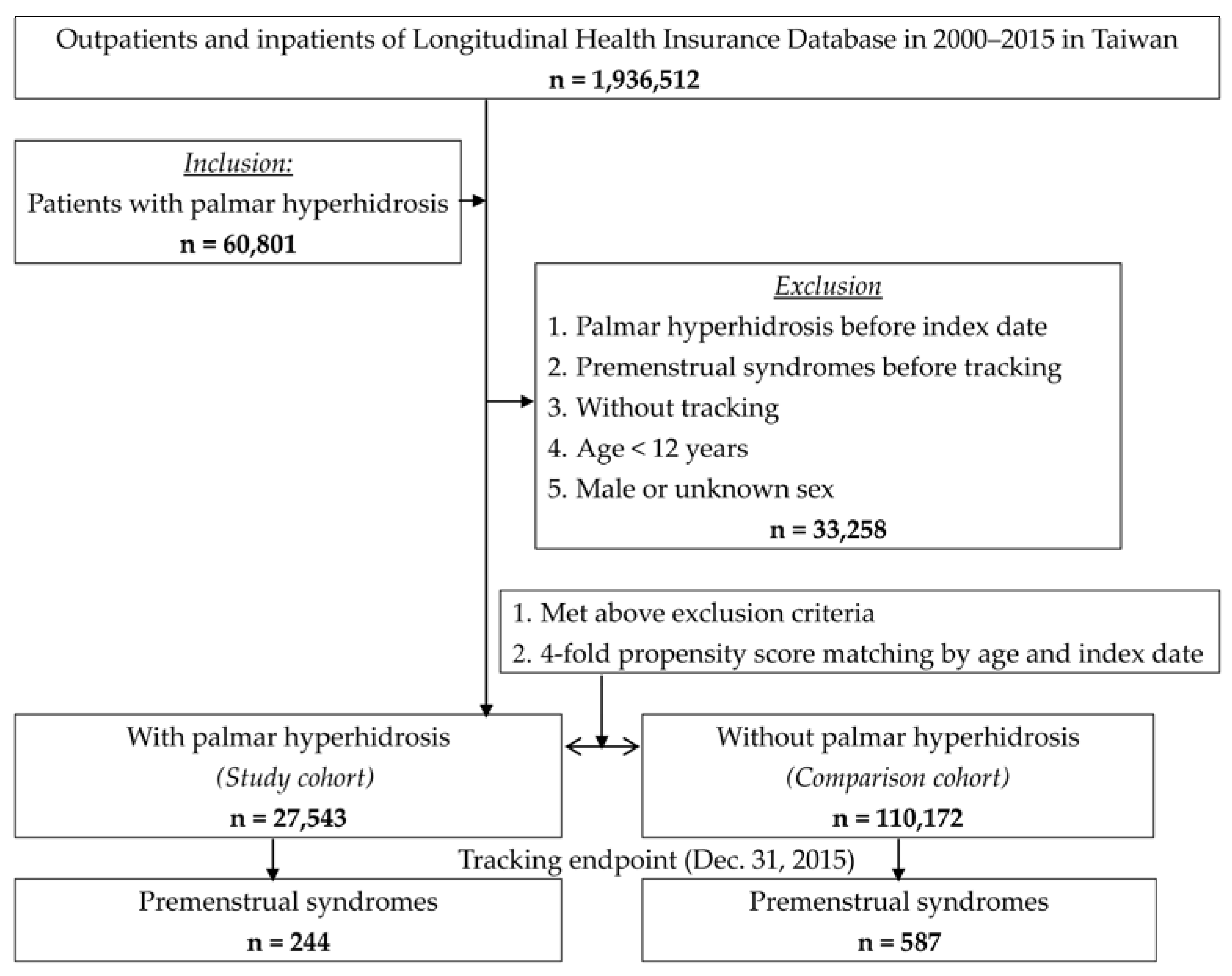
2.1. Database
2.2. Design
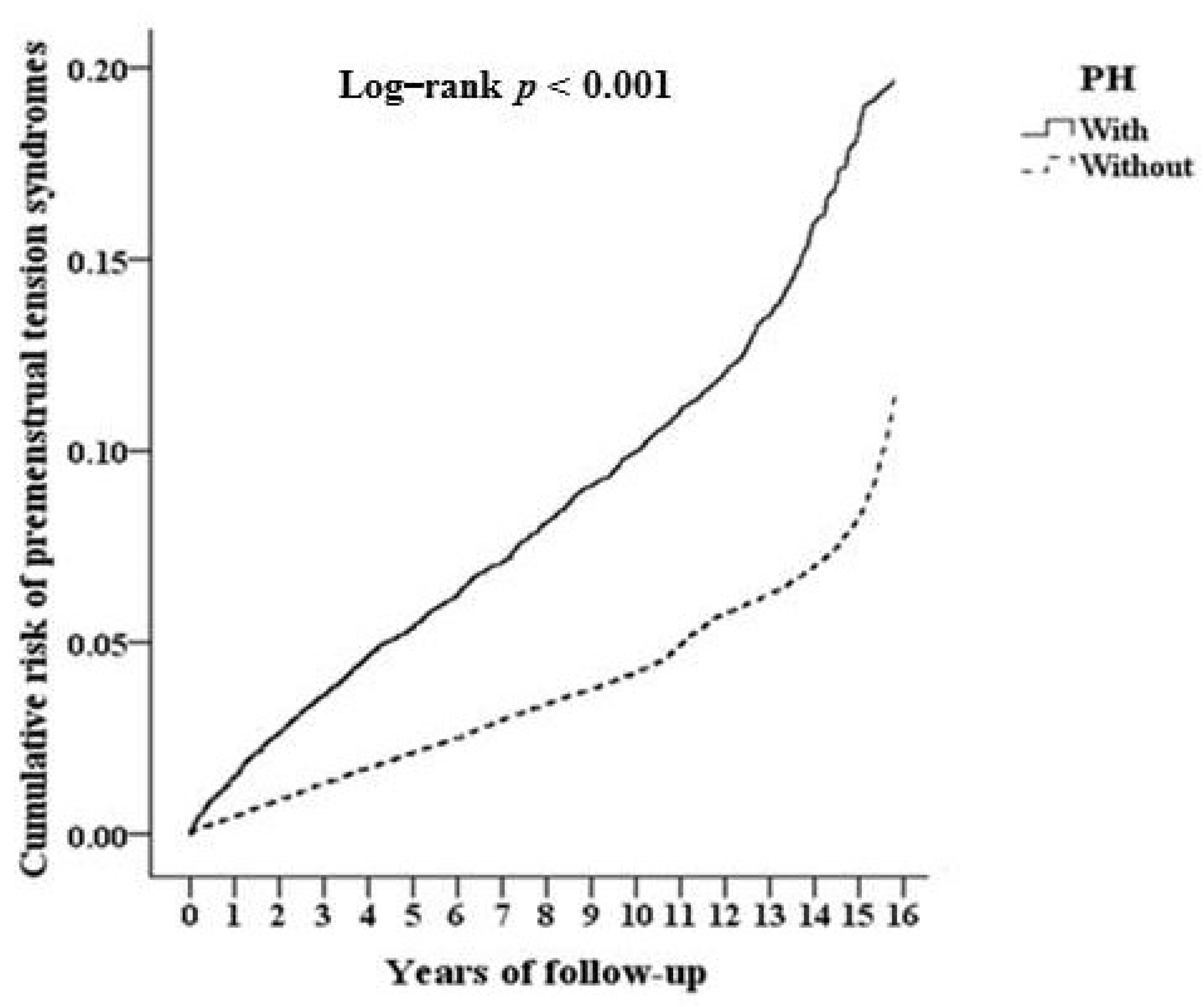
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hofmeister, S.; Bodden, S. Premenstrual syndrome and premenstrual dysphoric disorder. Am. Fam. Physician 2016, 94, 236–240. [Google Scholar]
- Matsumoto, T.; Ushiroyama, T.; Kimura, T.; Hayashi, T.; Moritani, T. Altered autonomic nervous system activity as a potential etiological factor of premenstrual syndrome and premenstrual dysphoric disorder. Biopsychosoc. Med. 2007, 1, 24. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.A.; Bisdorff, A.; Bronstein, A.M.; Lempert, T.; Rossi-Izquierdo, M.; Staab, J.P.; Strupp, M.; Kim, J.S. Hemodynamic orthostatic dizzi-ness/vertigo: Diagnostic criteria. J. Vestib. Res. 2019, 29, 45–56. [Google Scholar] [CrossRef] [Green Version]
- Alvares, G.A.; Quintana, D.S.; Hickie, I.B.; Guastella, A.J. Autonomic nervous system dysfunction in psychiatric disorders and the impact of psychotropic medications: A systematic review and meta-analysis. J. Psychiatry Neurosci. 2016, 41, 89–104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martínez-Martínez, L.-A.; Mora, T.; Vargas, A.; Fuentes-Iniestra, M.; Martínez-Lavín, M. Sympathetic nervous system dysfunction in fibromyalgia, chronic fatigue syndrome, irritable bowel syndrome, and interstitial cystitis: A review of case-control studies. J. Clin. Rheumatol. 2014, 20, 146–150. [Google Scholar] [CrossRef] [PubMed]
- Morrison, S.; Nakamura, K. Central Mechanisms for Thermoregulation. Annu. Rev. Physiol. 2019, 81, 285–308. [Google Scholar] [CrossRef] [PubMed]
- Macefield, V.G.; James, C.; Henderson, L.A. Identification of sites of sympathetic outflow at rest and during emotional arousal: Concurrent recordings of sympathetic nerve activity and fMRI of the brain. Int. J. Psychophysiol. 2013, 89, 451–459. [Google Scholar] [CrossRef]
- Hohenschurz-Schmidt, D.J.; Calcagnini, G.; DiPasquale, O.; Jackson, J.B.; Medina, S.; O’Daly, O.; O’Muircheartaigh, J.; Rubio, A.D.L.; Williams, S.C.R.; McMahon, S.B.; et al. Linking Pain Sensation to the Autonomic Nervous System: The Role of the Anterior Cingulate and Periaqueductal Gray Resting-State Networks. Front. Neurosci. 2020, 14. [Google Scholar] [CrossRef]
- Coon, E.A.; Cheshire, W.P., Jr. Sweating disorders. CONTINUUM Lifelong Learn. Neurol. 2020, 26, 116–137. [Google Scholar] [CrossRef]
- Lenefsky, M.; Rice, Z.P. Hyperhidrosis and its impact on those living with it. Am. J. Manag. Care 2018, 24, S491–S495. [Google Scholar]
- Birner, P.; Heinzl, H.; Schindl, M.; Pumprla, J.; Schnider, P. Cardiac autonomic function in patients suffering from primary focal hyperhidrosis. Eur. Neurol. 2000, 44, 112–116. [Google Scholar] [CrossRef] [PubMed]
- Cheng, C.-A.; Cheng, C.-G.; Chu, H.; Lin, H.-C.; Chung, C.-H.; Chiu, H.-W.; Chien, W.C. Risk reduction of long-term major adverse cardio-vascular events after endoscopic thoracic sympathectomy in palmar hyperhidrosis. Clin. Auton. Res. 2017, 27, 393–400. [Google Scholar] [CrossRef] [PubMed]
- Park, J.-M.; Moon, D.H.; Lee, H.S.; Park, J.-y.; Lee, J.-W.; Lee, S. Hyperhidrosis, Endoscopic Thoracic Sympathectomy, and Cardiovas-cular Outcomes: A Cohort Study Based on the Korean Health Insurance Review and Assessment Service Database. Int. J. Environ. Res. Public Health 2019, 16, 3925. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, C.-G.; Cheng, C.-A.; Chien, W.-C.; Chung, C.-H.; Lee, J.-T. Associated with Ischemic Stroke Risk Reduction after Endoscopic Thoracic Sympathectomy for Palmar Sweating. J. Stroke Cerebrovasc. Dis. 2018, 27, 2235–2242. [Google Scholar] [CrossRef]
- Cheng, C.-G.; Chien, W.-C.; Yu, C.-P.; Chung, C.-H.; Cheng, C.-A. Association between Reflux Esophagitis Incidence and Palmar Hyperhidrosis. Int. J. Environ. Res. Public Health 2020, 17, 4502. [Google Scholar] [CrossRef]
- Charkoudian, N.; Stachenfeld, N.S. Sex hormone effects on autonomic mechanisms of thermoregulation in humans. Auton. Neurosci. 2016, 196, 75–80. [Google Scholar] [CrossRef]
- National Health Insurance Research Database Taipei 2021. Available online: http://nhird.nhri.org.tw/en/index.html (accessed on 31 January 2021).
- Indusekhar, R.; Usman, S.B.; O’Brien, S. Psychological aspects of premenstrual syndrome. Best Pr. Res. Clin. Obstet. Gynaecol. 2007, 21, 207–220. [Google Scholar] [CrossRef]
- Koifman, R.; Dayan, L.; Ablin, J.N.; Jacob, G. Cardiovascular Autonomic Profile in Women with Premenstrual Syndrome. Front. Physiol. 2018, 9. [Google Scholar] [CrossRef]
- Smith, S.M.; Vale, W.W. The role of the hypothalamic-pituitary-adrenal axis in neuroendocrine responses to stress. Dialog. Clin. Neurosci. 2006, 8, 383–395. [Google Scholar]
- Shah, A.S.; Alonso, A.; Whitsel, E.A.; Soliman, E.Z.; Vaccarino, V.; Shah, A.J. Association of Psychosocial Factors with Short-Term Resting Heart Rate Variability: The Atherosclerosis Risk in Communities Study. J. Am. Hear. Assoc. 2021, 10, e017172. [Google Scholar] [CrossRef]
- Armbruster, D.; Grage, T.; Kirschbaum, C.; Strobel, A. Processing emotions: Effects of menstrual cycle phase and premenstrual symptoms on the startle reflex, facial EMG and heart rate. Behav. Brain Res. 2018, 351, 178–187. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, T.; Egawa, M.; Kimura, T.; Hayashi, T. A potential relation between premenstrual symptoms and subjective percep-tion of health and stress among college students: A cross-sectional study. Biopsychosoc. Med. 2019, 13, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Guarino, D.; Nannipieri, M.; Iervasi, G.; Taddei, S.; Bruno, R.M. The Role of the Autonomic Nervous System in the Pathophysiology of Obesity. Front. Physiol. 2017, 8, 665. [Google Scholar] [CrossRef] [Green Version]
- Hashim, M.S.; Obaideen, A.A.; Jahrami, H.A.; Radwan, H.; Hamad, H.J.; Owais, A.A.; Alardah, L.G.; Qiblawi, S.; Al-Yateem, N.; Faris, M.A.-I.E. Premenstrual Syndrome Is Associated with Dietary and Lifestyle Behaviors among University Students: A Cross-Sectional Study from Sharjah, UAE. Nutritions 2019, 11, 1939. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pal, G.K.; Adithan, C.; Ananthanarayanan, P.H.; Pal, P.; Nanda, N.; Thiyagarajan, D.; Syamsunderkiran, A.N.; Lalitha, V.; Dutta, T.K. Association of Sympathovagal Imbalance With Cardiovascular Risks in Young Prehypertensives. Am. J. Cardiol. 2013, 112, 1757–1762. [Google Scholar] [CrossRef] [PubMed]
- Okeahialam, B.N. The Role of Premenstrual Syndrome in the Causation of Arterial Hypertension in Women. Open J. Obstet. Gynecol. 2014, 4, 817–821. [Google Scholar] [CrossRef] [Green Version]
- Shah, A.S.; Vajravelu, M.E.; Bacha, F.; Farrell, R.M.; Gidding, S.S.; Katz, L.E.L.; Tryggestad, J.B.; White, N.H.; Urbina, E.M. Heart rate variability and cardiac autonomic dys-function: Prevalence, risk factors, and relationship to arterial stiffness in the treatment options for type 2 diabetes in adoles-cents and youth (TODAY) study. Diabetes Care 2019, 42, 2143–2150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeong, J.H.; Fonkoue, I.T.; Quyyumi, A.A.; DaCosta, D.; Park, J. Nocturnal blood pressure is associated with sympathetic nerve ac-tivity in patients with chronic kidney disease. Physiol. Rep. 2020, 8, e14602. [Google Scholar] [CrossRef] [PubMed]
- Ngassam, E.; Azabji-Kenfack, M.; Tankeu, A.T.; Mfeukeu-Kuate, L.; Nganou-Gnindjio, C.-N.; Mba, C.; Katte, J.C.; Dehayem, M.Y.; Mbanya, J.C.; Sobngwi, E. Heart rate variability in hyperthyroidism on sub Saharan African patients: A case–control study. BMC Res. Notes 2018, 11, 814. [Google Scholar] [CrossRef] [Green Version]
- Hazra, S.; Venkataraman, S.; Handa, G.; Yadav, S.L.; Wadhwa, S.; Singh, U.; Kochhar, K.P.; Deepak, K.K.; Sarkar, K. A Cross-Sectional Study on Central Sensitization and Autonomic Changes in Fibromyalgia. Front. Neurosci. 2020, 14, 788. [Google Scholar] [CrossRef]
- Franco, O.S.; Bs, A.O.S.J.; Signori, L.U.; Prietsch, S.O.M.; Zhang, L. Cardiac autonomic modulation assessed by heart rate variability in children with asthma. Pediatr. Pulmonol. 2020, 55, 1334–1339. [Google Scholar] [CrossRef]
- Van Gestel, A.J.; Kohler, M.; Steier, J.; Sommerwerck, U.; Teschler, S.; Russi, E.W.; Teschler, H. Cardiac autonomic function and cardiovascu-lar response to exercise in patients with chronic obstructive pulmonary disease. COPD 2012, 9, 160–165. [Google Scholar] [CrossRef]
- Danel, D.; Kozak, K.; Szala, A.; Kunert-Keil, C.; Dziedzic-Danel, A.; Siennicka, A. The Relationship between the Premenstrual Syn-drome and Resting Cardiac Vagal Tone in Young Healthy Females: Role of Hormonal Contraception. Neurophysiology 2019, 51, 447–454. [Google Scholar] [CrossRef]
- Abdi, F.; Ozgoli, G.; Rahnemaie, F.S. A systematic review of the role of vitamin D and calcium in premenstrual syndrome. Obstet. Gynecol. Sci. 2019, 62, 73–86. [Google Scholar] [CrossRef]
- Gepshtein, Y.; Plotnikoff, G.A.; Watanabe, K. Kampo in women’s health: Japan’s traditional approach to premenstrual symptoms. J. Altern. Complement Med. 2008, 14, 427–435. [Google Scholar] [CrossRef] [PubMed]
- Kamalifard, M.; Yavari, A.; Asghari-Jafarabadi, M.; Ghaffarilaleh, G.; Kasb-Khah, A. The Effect of Yoga on Women’s Premenstrual Syndrome: A Randomized Controlled Clinical Trial. Int. J. Women’s Health Reprod. Sci. 2017, 5, 205–211. [Google Scholar] [CrossRef] [Green Version]
- Bygstad, E.; Terkelsen, A.J.; Pilegaard, H.K.; Hansen, J.; Mølgaard, H.; Hjortdal, V.E. Thoracoscopic sympathectomy increases effer-ent cardiac vagal activity and baroreceptor sensitivity. Eur. J. Cardiothorac. Surg. 2013, 44, e193–e199. [Google Scholar] [CrossRef]
- Staunton, E.; Smid, S.D.; Dent, J.; Blackshaw, L.A. Triggering of transient LES relaxations in ferrets: Role of sympathetic pathways and effects of baclofen. Am. J. Physiol. Liver Physiol. 2000, 279, G157–G162. [Google Scholar] [CrossRef] [Green Version]
- Horslen, L.C.; Wilshire, C.L.; Louie, B.E.; Vallières, E. Long-term impact of endoscopic thoracic sympathectomy for primary pal-mar hyperhidrosis. Ann. Thorac. Surg. 2018, 106, 1008–1012. [Google Scholar] [CrossRef]
- Kingsley, J.D.; Figueroa, A. Acute and training effects of resistance exercise on heart rate variability. Clin. Physiol. Funct. Imaging 2016, 36, 179–187. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Palmar Hyperhidrosis (27543) | Control (110172) | p | |
|---|---|---|---|
| Age (years) | 28.30 ± 13.23 | 28.32 ± 13.25 | 0.823 |
| Obesity | 246 (0.89%) | 1014 (0.92%) | 0.697 |
| Depression | 5344 (19.4%) | 19187 (17.42%) | <0.001 * |
| Anxiety | 5672 (20.59%) | 20013 (18.17%) | <0.001 * |
| Thyrotoxicosis | 39 (0.14%) | 168 (0.15%) | 0.676 |
| Fibromyalgia | 42 (0.15%) | 180 (0.16%) | 0.687 |
| Hyperlipidemia | 4752 (17.25%) | 18245 (16.56%) | 0.006 * |
| Hypertension | 5711 (20.73%) | 21159 (19.21%) | <0.001 * |
| Diabetes mellitus | 5523 (20.05%) | 19887 (18.05%) | <0.001 * |
| Chronic kidney disease | 2975 (10.8%) | 12797 (11.62%) | <0.001 * |
| Asthma | 2480 (9%) | 9899 (8.99%) | 0.921 |
| Chronic obstructive pulmonary disease | 3016 (10.95%) | 12007 (10.9%) | 0.805 |
| Abortion | 42 (0.15%) | 1782 (1.62%) | <0.001 * |
| Pregnancy | 1678 (6.09%) | 16782 (15.23%) | <0.001 * |
| Irregular menstruation | 1588 (5.77%) | 6725 (6.1%) | 0.035 * |
| Drinking | 1604 (5.82%) | 6781 (6.15%) | 0.04 * |
| Season | 0.999 | ||
| Spring (March–May) | 5022 (18.23%) | 20088 (18.23%) | |
| Summer (June–August) | 6731 (24.44%) | 26924 (24.4%) | |
| Autumn (September–November) | 7782 (28.25%) | 31128 (28.25%) | |
| Winter (December–February) | 8008 (29.07%) | 32032 (29.07%) | |
| Location | <0.001 * | ||
| Northern Taiwan | 9215 (33.46%) | 28561 (25.92%) | |
| Middle Taiwan | 7203 (26.15%) | 26184 (23.77%) | |
| Southern Taiwan | 7675 (27.87%) | 27354 (24.83%) | |
| Eastern Taiwan | 3429 (12.45%) | 19446 (17.65%) | |
| Outlets islands | 21 (0.08%) | 8627 (7.83%) | |
| Urbanization level | <0.001 * | ||
| 1 (The highest) | 8216 (29.83%) | 28901 (26.23%) | |
| 2 | 9034 (32.8%) | 35121 (31.88%) | |
| 3 | 4125 (14.98%) | 21443 (19.46%) | |
| 4 (The lowest) | 6168 (22.39%) | 24707 (22.43%) | |
| Levels of healthcare | <0.001 * | ||
| Medical center | 13309 (48.32%) | 33452 (30.36%) | |
| Regional hospital | 8245 (29.94%) | 40267 (36.55%) | |
| Local hospital | 5989 (21.74%) | 36453 (33.09%) |
| Variables | Crude Hazard Ratio (95% Confidence Interval) | p | Adjusted Hazard Ratio (95% Confidence Interval) | p |
|---|---|---|---|---|
| Palmar hyperhidrosis | 1.389 (1.186–1.673) | <0.001 * | 1.276 (1.05–1.488) | 0.002 * |
| Age | 1.065 (0.864–1.372) | 0.786 | 0.975 (0.725–1.211) | 0.894 |
| Obesity | 1.599 (1.182–1.87) | <0.001 * | 1.386 (1.052–1.764) | <0.001 * |
| Depression | 2.586 (1.875–3.783) | <0.001 * | 2.01 (1.726–3.348) | <0.001 * |
| Anxiety | 2.677 (1.894–3.86) | <0.001 * | 2.154 (1.705–3.492) | <0.001 * |
| Hyperlipidemia | 1.798 (1.482–2.403) | <0.001 * | 1.529 (1.284–2.03) | <0.001 * |
| Hypertension | 1.701 (1.385–2.311) | <0.001 * | 1.443 (1.156–1.911) | <0.001 * |
| Diabetes mellitus | 1.725 (1.406–2.375) | <0.001 * | 1.486 (1.209–1.976) | <0.001 * |
| Chronic kidney disease | 1.286 (1.095–1.422) | <0.001 * | 1.197 (1.01–1.359) | 0.039 * |
| Irregular menstruation | 2.989 (1.762–7.264) | <0.001 * | 2.121 (1.573–4.009) | <0.001 * |
| Abortion | 1.623 (1.024–2.765) | 0.025 * | 1.307 (0.862–1.872) | 0.184 |
| Thyrotoxicosis | 2.289 (0.278–5.24) | 0.909 | 2.001 (0.185–2.701) | 0.928 |
| Fibromyalgia | 3.454 (0.425–6.187) | 0.918 | 2.271 (0.193–4.229) | 0.937 |
| Asthma | 1.451 (0.896–1.782) | 0.286 | 1.186 (0.715–1.607) | 0.38 |
| Chronic obstructive pulmonary disease | 1.209 (0.776–1.509) | 0.335 | 1.078 (0.622–1.403) | 0.478 |
| Drinking | 1.592 (0.751–2.248) | 0.375 | 1.57 (0.724–2.188) | 0.392 |
| Season | ||||
| Spring | Reference | Reference | ||
| Summer | 1.185 (0.789–1.506) | 0.289 | 1.086 (0.725–1.348) | 0.31 |
| Autumn | 1.209 (0.813–1.584) | 0.178 | 1.113 (0.774–1.387) | 0.287 |
| Winter | 1.288 (0.856–1.617) | 0.144 | 1.187 (0.798–1.401) | 0.209 |
| Location | ||||
| Northern Taiwan | Reference | Multicollinearity with urbanization level | ||
| Middle Taiwan | 0.903 (0.397–1.713) | 0.629 | ||
| Southern Taiwan | 0.984 (0.441–1.786) | 0.583 | ||
| Eastern Taiwan | 0.845 (0.342–1.684) | 0.675 | ||
| Outlets islands | 5.254 (0.013–278.901) | 0.996 | ||
| Urbanization level | ||||
| 1 (The highest) | 1.986 (1.5–2.976) | <0.001 * | 1.875 (1.357–2.78) | <0.001 * |
| 2 | 1.624 (1.184–2.773) | <0.001 * | 1.523 (1.01202.622) | 0.038 * |
| 3 | 1.301 (0.905–2.501) | 0.099 | 1.112 (0.787–2.403) | 0.248 |
| 4 (The lowest) | Reference | Reference | ||
| Levels of healthcare | ||||
| Medical center | 1.682 (1.249–2.187) | <0.001 * | 1.572 (1.172–2.08) | <0.001 * |
| Regional hospital | 1.603 (1.24–2.113) | <0.001 * | 1.533 (1.159–2.001) | <0.001 * |
| Local hospital | Reference | Reference |
| PH | with | without (Reference) | with vs. without (Reference) | |||||
|---|---|---|---|---|---|---|---|---|
| Stratified | Events | PYs | Rate (Per 105 PYs) | Events | PYs | Rate (Per 105 PYs) | Adjusted Hazard Ratio (95% Confidence Interval) | p |
| Total | 244 | 243,198.75 | 100.33 | 587 | 982,035.11 | 59.77 | 1.276 (1.05–1.488) | 0.002 * |
| Abortion | ||||||||
| Without | 231 | 242,677.79 | 95.19 | 406 | 965,437.89 | 42.05 | 1.221 (1.036–1.407) | 0.015 * |
| With | 13 | 520.96 | 2,495.41 | 181 | 16,597.22 | 1090.54 | 1.74 (1.431–2.029) | <0.001 * |
| Pregnancy | ||||||||
| Without | 244 | 228,338.22 | 106.86 | 587 | 806,427.21 | 72.79 | 1.276 (1.05–1.488) | 0.002 * |
| With | 0 | 14,860.53 | 0.00 | 0 | 175,607.90 | 0.00 | – | - |
| Irregular menstruation | ||||||||
| Without | 114 | 228,973.97 | 49.79 | 303 | 921,235.07 | 32.89 | 1.152 (1.007–1.342) | 0.044 * |
| With | 130 | 14,224.78 | 913.90 | 284 | 60,800.04 | 467.10 | 1.487 (1.249–1.739) | <0.001 * |
| Obesity | ||||||||
| Without | 185 | 240,576.30 | 76.90 | 537 | 972,247.92 | 55.23 | 1.058 (0.876–1.239) | 0.176 |
| With | 59 | 2,622.45 | 2,249.81 | 50 | 9,787.19 | 510.87 | 3.321(2.735–3.918) | <0.001 * |
| Depression | ||||||||
| Without | 135 | 194,652.60 | 69.35 | 344 | 803,975.95 | 42.79 | 1.232 (1.036–1.433) | 0.015 * |
| With | 109 | 48,546.15 | 224.53 | 243 | 178,059.16 | 136.47 | 1.297 (1.145–1.598) | <0.001 * |
| Anxiety | ||||||||
| Without | 130 | 191,977.17 | 67.72 | 336 | 797,121.35 | 42.15 | 1.229 (1.024–1.428) | 0.025 * |
| With | 114 | 51,221.58 | 222.56 | 251 | 184,913.76 | 135.74 | 1.286 (1.067–1.577) | <0.001 * |
| Thyrotoxicosis | ||||||||
| Without | 239 | 242,810.24 | 98.43 | 585 | 980,519.79 | 59.66 | 1.254 (1.023–1.438) | 0.025 * |
| With | 5 | 388.51 | 1286.97 | 2 | 1515.32 | 131.99 | 7.411 (5.986–8.63) | <0.001 * |
| Fibromyalgia | ||||||||
| Without | 239 | 242,757.26 | 98.45 | 583 | 980,377.17 | 59.47 | 1.259 (1.038–1.482) | 0.011 * |
| With | 5 | 441.49 | 1132.53 | 4 | 1657.94 | 241.26 | 3.568 (2.937–4.161) | <0.001 * |
| Hyperlipidemia | ||||||||
| Without | 166 | 200,789.30 | 82.67 | 399 | 805,723.03 | 49.52 | 1.267 (1.048–1.48) | 0.003 * |
| With | 78 | 42,409.45 | 183.92 | 188 | 176,312.08 | 106.63 | 1.315 (1.079–1.529) | <0.001 * |
| Hypertension | ||||||||
| Without | 161 | 191,641.64 | 84.01 | 408 | 785,809.93 | 51.92 | 1.23 (1.021–1.431) | 0.028 * |
| With | 83 | 51,557.11 | 160.99 | 179 | 196,225.18 | 91.22 | 1.342 (1.104–1.568) | <0.001 * |
| Diabetes mellitus | ||||||||
| Without | 164 | 193,743.13 | 84.65 | 411 | 800,312.44 | 51.35 | 1.253 (1.033–1.468) | 0.016 * |
| With | 80 | 49,455.62 | 161.76 | 176 | 181,722.67 | 96.85 | 1.301 (1.069–1.512) | <0.001 * |
| Chronic kidney disease | ||||||||
| Without | 185 | 216,117.80 | 85.60 | 457 | 862,574.32 | 52.98 | 1.228 (1.012–1.432) | 0.036 * |
| With | 59 | 27,080.95 | 217.87 | 130 | 119,460.79 | 108.82 | 1.523 (1.297–1.804) | <0.001 * |
| Asthma | ||||||||
| Without | 177 | 220,364.93 | 80.32 | 445 | 893,005.53 | 49.83 | 1.251 (1.008–1.429) | 0.043 * |
| With | 67 | 22,833.82 | 293.42 | 142 | 89,029.58 | 159.50 | 1.403 (1.189–1.635) | <0.001 * |
| Chronic obstructive pulmonary disease | ||||||||
| Without | 181 | 215,499.72 | 83.99 | 449 | 871,425.58 | 51.52 | 1.239 (1.022–1.444) | 0.029 * |
| With | 63 | 27,699.03 | 227.44 | 138 | 110,609.53 | 124.76 | 1.389 (1.142–1.68) | <0.001 * |
| Drinking | ||||||||
| Without | 189 | 228,294.07 | 82.79 | 476 | 921,110.28 | 51.68 | 1.225 (1.006–1.429) | 0.043 * |
| With | 55 | 14,904.68 | 369.01 | 111 | 60,924.83 | 182.19 | 1.549 (1.278–1.893) | <0.001 * |
| Season | ||||||||
| Spring | 40 | 44,352.01 | 90.19 | 126 | 200,432.43 | 62.86 | 1.104 (0.893–1.278) | 0.204 |
| Summer | 58 | 59,292.00 | 97.82 | 131 | 229,883.14 | 56.99 | 1.305 (1.042–1.514) | 0.009 * |
| Autumn | 67 | 68,792.85 | 97.39 | 148 | 262,712.13 | 56.34 | 1.314 (1.082–1.539) | <0.001 * |
| Winter | 79 | 70,761.89 | 111.64 | 182 | 289,007.41 | 62.97 | 1.352 (1.109–1.586) | <0.001 * |
| Urbanization level | ||||||||
| 1 (The highest) | 72 | 72,713.27 | 99.02 | 103 | 264,744.44 | 38.91 | 1.935 (1.592–2.378) | <0.001 * |
| 2 | 63 | 79,441.57 | 79.30 | 130 | 305,515.50 | 42.55 | 1.416 (1.163–1.672) | <0.001 * |
| 3 | 47 | 37,447.12 | 125.51 | 164 | 190,805.68 | 85.95 | 1.111 (0.924–1.301) | 0.199 |
| 4 (The lowest) | 62 | 53,596.79 | 115.68 | 190 | 220,969.49 | 85.98 | 1.028 (0.84–1.194) | 0.286 |
| Level of healthcare | ||||||||
| Medical center | 92 | 116,906.34 | 78.70 | 116 | 298,357.83 | 38.88 | 1.542 (1.289–1.801) | <0.001 * |
| Regional hospital | 85 | 73,684.55 | 115.36 | 231 | 356,448.12 | 64.81 | 1.378 (1.136–1.587) | <0.001 * |
| Local hospital | 67 | 52,607.86 | 127.36 | 240 | 327,229.16 | 73.34 | 1.32 (1.089–1.542) | <0.001 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cheng, C.-A.; Liang, Y.-C.; Chang, Y.-H.; Cheng, C.-G.; Chung, C.-H.; Chien, W.-C. Increased Incidence of Premenstrual Syndrome in Females with Palmar Hyperhidrosis. Int. J. Environ. Res. Public Health 2021, 18, 4697. https://doi.org/10.3390/ijerph18094697
Cheng C-A, Liang Y-C, Chang Y-H, Cheng C-G, Chung C-H, Chien W-C. Increased Incidence of Premenstrual Syndrome in Females with Palmar Hyperhidrosis. International Journal of Environmental Research and Public Health. 2021; 18(9):4697. https://doi.org/10.3390/ijerph18094697
Chicago/Turabian StyleCheng, Chun-An, Yu-Cheng Liang, Yin-Han Chang, Chun-Gu Cheng, Chi-Hsiang Chung, and Wu-Chien Chien. 2021. "Increased Incidence of Premenstrual Syndrome in Females with Palmar Hyperhidrosis" International Journal of Environmental Research and Public Health 18, no. 9: 4697. https://doi.org/10.3390/ijerph18094697