
Follow-Up Survey of the Impact of COVID-19 on People Living with HIV during the Second Semester of the Pandemic

 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Study Setting and Procedures
2.2. Statistical Analysis
2.3. Ethical Considerations
3. Results
3.1. Participants’ Characteristics
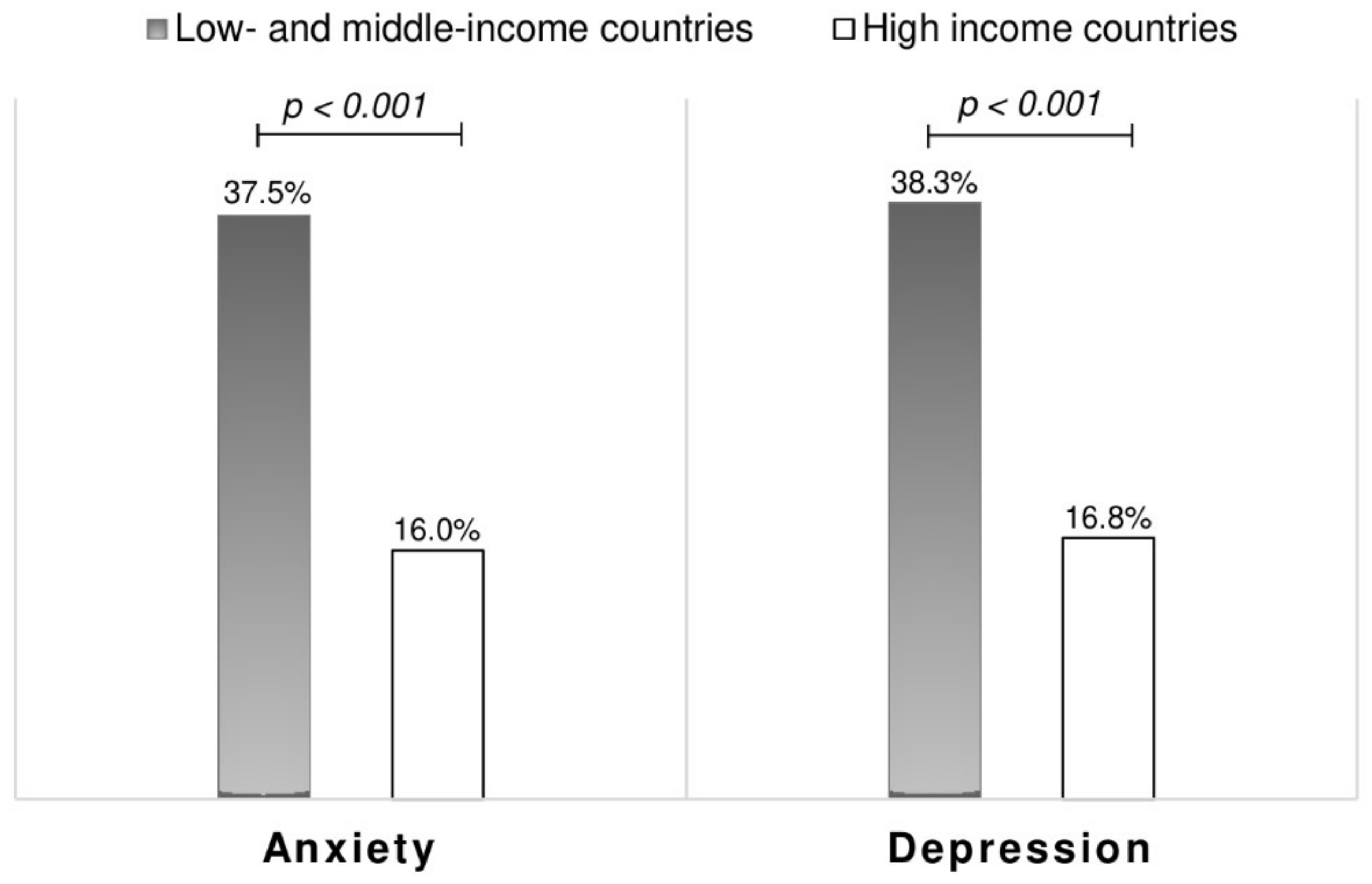
3.2. Psychosocial Well-Being
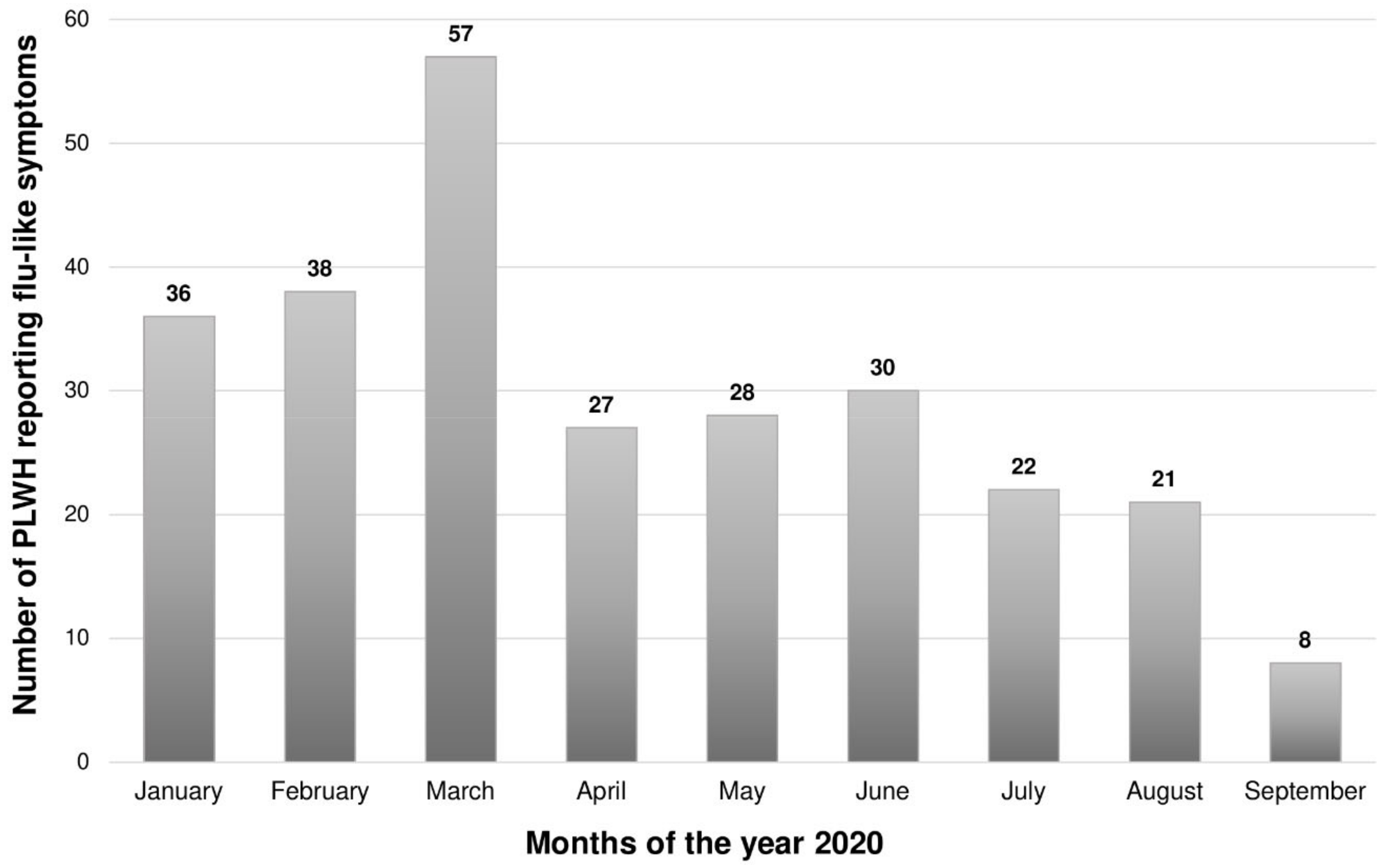
3.3. Flu-Like Symptoms
3.4. COVID-19 Preventive Measures and Impact on Respondents
3.5. Factors Associated with Visiting a Health Facility for HIV Follow-Up
3.6. Cohort of PLWH Who Were Identifiable in Previous (April 2020) and Current (July 2020) Surveys
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. WHO Coronavirus Disease (COVID-19) Dashboard. 2020. Available online: https://covid19.who.int/ (accessed on 3 March 2021).
- Hojyo, S.; Uchida, M.; Tanaka, K.; Hasebe, R.; Tanaka, Y.; Murakami, M.; Hirano, T. How COVID-19 induces cytokine storm with high mortality. Inflamm. Regen. 2020, 40, 1–7. [Google Scholar] [CrossRef]
- Laurence, J. Why Aren’t People Living with HIV at Higher Risk for Developing Severe Coronavirus Disease 2019 (COVID-19)? AIDS Patient Care STDS 2020, 34, 247–248. [Google Scholar] [CrossRef] [PubMed]
- Xu, Z.; Zhang, C.; Wang, F.-S. COVID-19 in people with HIV. Lancet HIV 2020, 7, e524–e526. [Google Scholar] [CrossRef]
- Cooper, T.J.; Woodward, B.L.; Alom, S.; Harky, A. Coronavirus disease 2019 (COVID-19) outcomes in HIV/AIDS patients: A systematic review. HIV Med. 2020, 21, 567–577. [Google Scholar] [CrossRef] [PubMed]
- Laracy, J.; Zucker, J.; Castor, D.; McMahon, D.J.; Guo, T.W.; Yan, M.; Shalev, N.; Scherer, M.; Gordon, P.; Sobieszczyk, M.; et al. HIV-1 Infection Does Not Change Disease Course or Inflammatory Pattern of SARS-CoV-2-Infected Patients Presenting at a Large Urban Medical Center in New York City. Open Forum Infect. Dis. 2021, 8, ofab029. [Google Scholar] [CrossRef] [PubMed]
- Boulle, A.; Davies, M.-A.; Hussey, H.; Ismail, M.; Morden, E.; Vundle, Z.; Zweigenthal, V.; Mahomed, H.; Paleker, M.; Pienaar, D.; et al. Risk factors for COVID-19 death in a population cohort study from the Western Cape Province, South Africa. Clin. Infect. Dis. 2020, ciaa1198. [Google Scholar] [CrossRef]
- Dandachi, D.; Geiger, G.; Montgomery, M.W.; Karmen-Tuohy, S.; Golzy, M.; Antar, A.A.R.; Llibre, J.M.; Camazine, M.; Díaz-De Santiago, A.; Carlucci, P.; et al. Characteristics, Comorbidities, and Outcomes in a Multicenter Registry of Patients with Human Immunodeficiency Virus and Coronavirus Disease 2019. Clin. Infect. Dis. 2020, ciaa1339. [Google Scholar] [CrossRef]
- Mellor, M.M.; Bast, A.C.; Jones, N.R.; Roberts, N.W.; Ordóñez-Mena, J.M.; Reith, A.J.M.; Butler, C.C.; Matthews, P.C.; Dorward, J. Risk of Adverse COVID-19 Outcomes for People Living with HIV: A Rapid Review and Meta-Analysis. MedRxiv 2020. Available online: https://journals.lww.com/10.1097/QAD.0000000000002836 (accessed on 16 March 2021).
- Fodjo, J.N.S.; de Moura, V.E.F.M.; Van Hees, S.; dos Santos, T.T.; Vanholder, P.; Reyntiens, P.; Van den Bergh, R.; Colebunders, R. Impact of the COVID-19 Pandemic on the Medical Follow-up and Psychosocial Well-Being of People Living With HIV: A Cross-Sectional Survey. Jaids J. Acquir. Immune Defic. Syndr. 2020, 85, 257–262. [Google Scholar] [CrossRef]
- Bulstra, C.A.; Reddy, C.L.; Atun, R.; Bärnighausen, T.; Hontelez, J.A.C. Impact of the COVID-19-Related Global Recession on the Financing of the Global HIV Response. AIDS 2021. Available online: https://journals.lww.com/10.1097/QAD.0000000000002872 (accessed on 16 March 2021). [CrossRef]
- WHO: Access to HIV Medicines Severely Impacted by COVID-19 as AIDS Response Stalls. Available online: https://www.who.int/news/item/06-07-2020-who-access-to-hiv-medicines-severely-impacted-by-covid-19-as-aids-response-stalls (accessed on 20 November 2020).
- Wong, L.E.; Hawkins, J.E.; Langness, S.; Murrell, K.L.; Iris, P.; Sammann, A. Where Are All the Patients? Addressing Covid-19 Fear to Encourage Sick Patients to Seek Emergency Care. NEJM Catal. Innov. Care Deliv. 2020. Available online: https://catalyst.nejm.org/doi/full/10.1056/CAT.20.0193 (accessed on 12 February 2021).
- ICPCovid Research Group. International Citizen Project Covid-19. 2020. Available online: https://www.icpcovid.com/ (accessed on 11 May 2020).
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W. The Patient Health Questionnaire-2: Validity of a Two-Item Depression Screener. Med. Care 2003, 41, 1284–1292. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W.; Monahan, P.O.; Löwe, B. Anxiety Disorders in Primary Care: Prevalence, Impairment, Comorbidity, and Detection. Ann. Intern. Med. 2007, 146, 317–325. [Google Scholar] [CrossRef]
- Teymoori, A.; Real, R.; Gorbunova, A.; Haghish, E.F.; Andelic, N.; Wilson, L.; Asendorf, T.; Menon, D.; Steinbüchel, N. Measurement invariance of assessments of depression (PHQ-9) and anxiety (GAD-7) across sex, strata and linguistic backgrounds in a European-wide sample of patients after Traumatic Brain Injury. J. Affect. Disord. 2020, 262, 278–285. [Google Scholar] [CrossRef]
- Public Health Surveillance for COVID-19: Interim Guidance. Available online: https://www.who.int/publications-detail-redirect/who-2019-nCoV-surveillanceguidance-2020.7 (accessed on 19 August 2020).
- World Bank Country and Lending Groups–World Bank Data Help Desk. Available online: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups (accessed on 24 May 2020).
- Lam, P. Logit GEE (Zelig Package). 2017. Available online: http://docs.zeligproject.org/articles/zelig_logitgee.html (accessed on 21 November 2020).
- Rezaei, S.; Ahmadi, S.; Rahmati, J.; Hosseinifard, H.; Dehnad, A.; Aryankhesal, A.; Shabaninejad, H.; Ghasemyani, S.; Alihosseini, S.; Bragazzi, N.L.; et al. Global prevalence of depression in HIV/AIDS: A systematic review and meta-analysis. BMJ Support. Palliat. Care 2019, 9, 404–412. [Google Scholar] [CrossRef]
- Brandt, C.; Zvolensky, M.J.; Woods, S.P.; Gonzalez, A.; Safren, S.A.; O’Cleirigh, C.M. Anxiety symptoms and disorders among adults living with HIV and AIDS: A critical review and integrative synthesis of the empirical literature. Clin. Psychol. Rev. 2017, 51, 164–184. [Google Scholar] [CrossRef] [Green Version]
- Government of Belgium. COVID-19 Impact on Mental Health. For a Healthy Belgium. 2021. Available online: https://www.healthybelgium.be/en/health-status/covid-19-crisis/covid-19-impact (accessed on 7 April 2021).
- Mitchell, A.J.; Yadegarfar, M.; Gill, J.; Stubbs, B. Case finding and screening clinical utility of the Patient Health Questionnaire (PHQ-9 and PHQ-2) for depression in primary care: A diagnostic meta-analysis of 40 studies. Bjpsych. Open 2016, 2, 127–138. [Google Scholar] [CrossRef] [Green Version]
- Skapinakis, P. The 2-item Generalized Anxiety Disorder scale had high sensitivity and specificity for detecting GAD in primary care. Evid. Based Med. 2007, 12, 149. [Google Scholar] [CrossRef] [Green Version]
- Puccinelli, P.J.; da Costa, T.S.; Seffrin, A.; de Lira, C.A.B.; Vancini, R.L.; Nikolaidis, P.T.; Knechtle, B.; Rosemann, T.; Hill, L.; Andrade, M.S. Reduced level of physical activity during COVID-19 pandemic is associated with depression and anxiety levels: An internet-based survey. BMC Public Health 2021, 21, 425. [Google Scholar]
- Ramiz, L.; Contrand, B.; Rojas Castro, M.Y.; Dupuy, M.; Lu, L.; Sztal-Kutas, C.; Lagarde, E. A longitudinal study of mental health before and during COVID-19 lockdown in the French population. Glob. Health 2021, 17, 29. [Google Scholar] [CrossRef] [PubMed]
- Al Maqbali, M.; Al Sinani, M.; Al-Lenjawi, B. Prevalence of stress, depression, anxiety and sleep disturbance among nurses during the COVID-19 pandemic: A systematic review and meta-analysis. J. Psychosom. Res. 2021, 141, 110343. [Google Scholar] [CrossRef] [PubMed]
- Hogan, A.B.; Jewell, B.L.; Sherrard-Smith, E.; Vesga, J.F.; Watson, O.J.; Whittaker, C.; Knechtle, B.; Rosemann, T.; Hill, L.; Andrade, M.S. Potential impact of the COVID-19 pandemic on HIV, tuberculosis, and malaria in low-income and middle-income countries: A modelling study. Lancet Glob. Health 2020, 8, e1132–e1141. [Google Scholar] [CrossRef]
- Jiang, H.; Zhou, Y.; Tang, W. Maintaining HIV care during the COVID-19 pandemic. Lancet HIV 2020, 7, e308–e309. [Google Scholar] [CrossRef]
- Mandel, A.; Veetil, V. The Economic Cost of COVID Lockdowns: An Out-of-Equilibrium Analysis. Econ. Dis. Clim. Chang. 2020, 4, 431–451. [Google Scholar]
- Budak, J.Z.; Scott, J.D.; Dhanireddy, S.; Wood, B.R. The Impact of COVID-19 on HIV Care Provided via Telemedicine—Past, Present, and Future. Curr. HIV/AIDS Rep. 2021. Available online: http://link.springer.com/10.1007/s11904-021-00543-4 (accessed on 16 March 2021). [CrossRef]
- Bell, N.; Bracchi, M.; Dalla Pria, A.; Nelson, M.; Boffito, M. Indirect HIV morbidity and mortality due to COVID-19. Clin. Infect. Dis. 2021, ciab128. [Google Scholar] [CrossRef]
- Bhatt, M.; Soneja, M.; Gupta, N. COVID-19 in patients living with human immunodeficiency virus (HIV) infection: Challenges and way-forward. Drug Discov. 2020, 15, 42–43. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Observed |
|---|---|
| Age, years: mean (SD) | 44.5 (13.2) |
| Sex: n (%) | |
| Male | 182 (73.7%) |
| Female | 61 (24.7%) |
| Other | 4 (1.6%) |
| Classification of country of residence: n (%) | |
| Low and Middle income country (LMIC) | 128 (51.8%) |
| High income country (HIC) | 119 (48.2%) |
| Highest education level: n (%) | |
| Primary | 19 (7.7%) |
| Secondary | 73 (29.6%) |
| Undergraduate | 75 (30.4%) |
| Post-graduate | 80 (32.4%) |
| Religion: n (%) | |
| Christian | 123 (49.8%) |
| Muslim | 6 (2.4%) |
| Other | 31 (12.6%) |
| None | 87 (35.2%) |
| Marital status: n (%) | |
| Single | 101 (40.9%) |
| Stable relationship | 34 (13.8%) |
| Cohabitation | 33 (13.4%) |
| Married | 48 (19.4%) |
| Divorced | 23 (9.3%) |
| Other | 8 (3.2%) |
| Visited health facility or HIV clinic during the last month for routine HIV follow-up: n (%) | 132 (53.4%) |
| COVID-19 test results: n (%) | |
| Positive | 9/59 (15.3%) |
| Negative | 50/59 (84.7%) |
| Reported Changes during the Confinement Period: n (%) | ||||
|---|---|---|---|---|
| No Change | Better | Worse | Missing Data | |
| Financial situation (n = 175) | 97 (55.4%) | 13 (7.4%) | 65 (37.1%) | 72 |
| Sexual fulfilment (n = 160) | 73 (45.6%) | 11 (6.9%) | 76 (47.5%) | 87 |
| Family life (n = 166) | 82 (49.4%) | 21 (12.7%) | 63 (38.0%) | 81 |
| Social life outside family (n = 173) | 48 (27.7%) | 10 (5.8%) | 115 (66.5%) | 74 |
| Reported changes after relaxing confinement measures: n (%) | ||||
| Yes | No | Missing data | ||
| Difficulty to revert to normal social life (n = 183) | 91 (49.7%) | 92 (50.3%) | 64 | |
| Difficulty to revert to normal sexual life (n = 183) | 71 (38.8%) | 112 (61.2%) | 64 | |
| Covariates | Adjusted OR (95% CI) | p Value |
|---|---|---|
| Age (in years) | 0.984 (0.967–1.00) | 0.086 |
| Sex | ||
| Female | Reference | |
| Male | 0.915 (0.766–1.09) | 0.326 |
| Educational level | ||
| Primary | Reference | |
| Secondary | 0.532 (0.310–0.911) | 0.022 |
| Undergraduate | 0.856 (0.223–3.29) | 0.821 |
| Postgraduate | 0.247 (0.090–0.683) | 0.007 |
| Country classification | ||
| HIC | Reference | |
| LMIC | 0.368 (0.331–0.409) | <0.001 |
| PHQ-2 score | 0.907 (0.788–1.04) | 0.172 |
| GAD-2 score | 1.09 (0.856–1.39) | 0.479 |
| Fear of getting infected at hospital (Likert score) | 1.07 (0.948–1.22) | 0.261 |
| Availability of psychosocial support at HIV clinic | 0.837 (0.305–2.30) | 0.73 |
| Flu vaccination during the past 12 months | 1.10 (0.535–2.26) | 0.797 |
| History of lockdown in respondent’s locality | 1.20 (0.649–2.23) | 0.558 |
| Month of participation in online survey | ||
| July | Reference | |
| August | 2.11 (0.716–6.20) | 0.176 |
| September | 3.31 (1.47–7.43) | 0.004 |
| October | 0.636 (0.010–39.5) | 0.83 |
| November | 0.785 (0.437–1.41) | 0.419 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Siewe Fodjo, J.N.; Faria de Moura Villela, E.; Van Hees, S.; Vanholder, P.; Reyntiens, P.; Colebunders, R. Follow-Up Survey of the Impact of COVID-19 on People Living with HIV during the Second Semester of the Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 4635. https://doi.org/10.3390/ijerph18094635
Siewe Fodjo JN, Faria de Moura Villela E, Van Hees S, Vanholder P, Reyntiens P, Colebunders R. Follow-Up Survey of the Impact of COVID-19 on People Living with HIV during the Second Semester of the Pandemic. International Journal of Environmental Research and Public Health. 2021; 18(9):4635. https://doi.org/10.3390/ijerph18094635
Chicago/Turabian StyleSiewe Fodjo, Joseph Nelson, Edlaine Faria de Moura Villela, Stijn Van Hees, Pieter Vanholder, Patrick Reyntiens, and Robert Colebunders. 2021. "Follow-Up Survey of the Impact of COVID-19 on People Living with HIV during the Second Semester of the Pandemic" International Journal of Environmental Research and Public Health 18, no. 9: 4635. https://doi.org/10.3390/ijerph18094635