
Association of Body Composition with Type 2 Diabetes: A Retrospective Chart Review Study

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Measures and Instruments
2.3. Definitions of Variables
2.4. Statistical Analyses
3. Results
3.1. Demographics of Participants
3.2. Prevalence of Low Muscle Mass and Sarcopenic Obesity in Different Age and Sex Groups
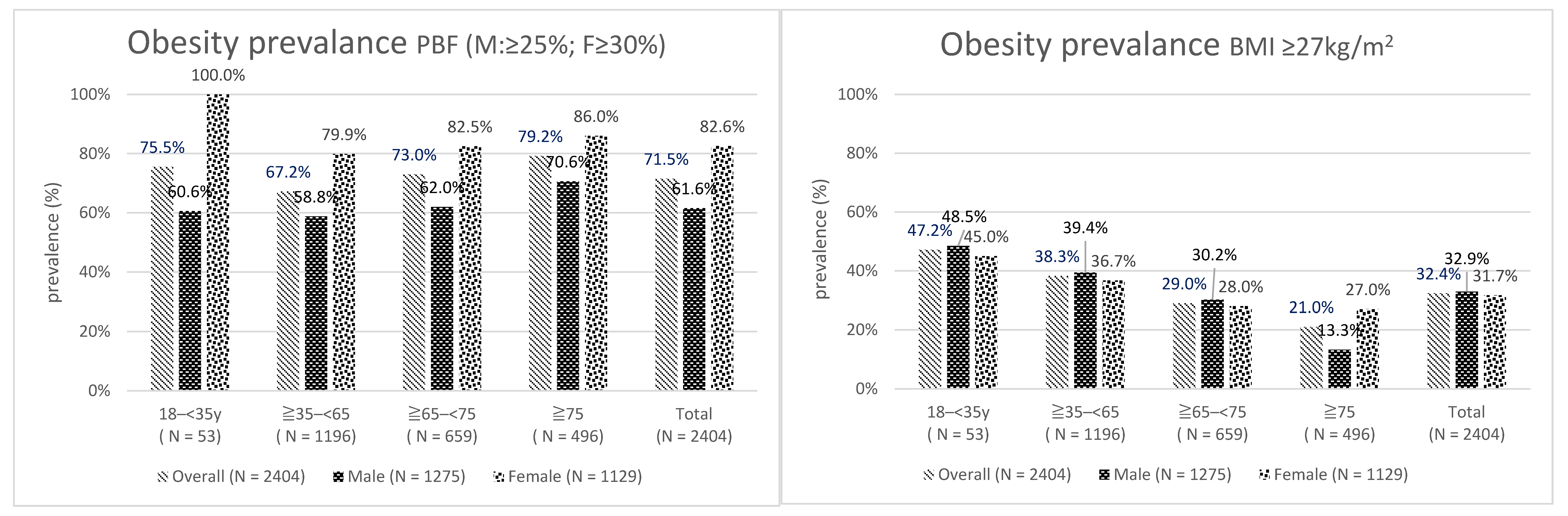
3.3. Obesity Prevalence
3.4. Prevalence of Body Composition Anomalies in Different BMI Groups
3.5. Body Composition by Age and Sex
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Saeedi, P.; Petersohn, I.; Salpea, P.; Malanda, B.; Karuranga, S.; Unwin, N.; Colagiuri, S.; Guariguata, L.; Motala, A.A.; Ogurtsova, K.; et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the In-ternational Diabetes Federation Diabetes Atlas. Diabetes Res. Clin. Pract. 2019, 157, 107843. [Google Scholar] [CrossRef] [Green Version]
- International Diabetes Federation. IDF Diabetes Atlas, 8th ed.; International Diabetes Federation: Brussels, Belgium, 2017. [Google Scholar]
- Han, T.S.; Al-Gindan, Y.Y.; Govan, L.; Hankey, C.R.; Lean, M.E.J. Associations of BMI, waist circumference, body fat, and skeletal muscle with type 2 diabetes in adults. Acta Diabetol. 2019, 56, 947–954. [Google Scholar] [CrossRef] [Green Version]
- Kurioka, S.; Murakami, Y.; Nishiki, M.; Sohmiya, M.; Koshimura, K.; Kato, Y. Relationship between Visceral Fat Accumulation and Anti-Lipolytic Action of Insulin in Patients with Type 2 Diabetes Mellitus. Endocr. J. 2002, 49, 459–464. [Google Scholar] [CrossRef] [Green Version]
- He, X.; Li, Z.; Tang, X.; Zhang, L.; Wang, L.; He, Y.; Jin, T.; Yuan, D. Age- and sex-related differences in body composition in healthy subjects aged 18 to 82 years. Medicine 2018, 97, e11152. [Google Scholar] [CrossRef]
- Wells, J.; Fewtrell, M. Measuring body composition. Arch. Dis. Child 2006, 91, 612–617. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borga, M.; West, J.; Bell, J.D.; Harvey, N.C.; Romu, T.; Heymsfield, S.B.; Leinhard, O.D. Advanced body composition assessment: From body mass index to body composition profiling. J. Investig. Med. 2018, 66, 1–9. [Google Scholar] [CrossRef]
- Santanasto, A.J.; Goodpaster, B.H.; Kritchevsky, S.B.; Miljkovic, I.; Satterfield, S.; Schwartz, A.V.; Cummings, S.R.; Boudreau, R.M.; Harris, T.B.; Newman, A.B. Body Composition Remodeling and Mortality: The Health Aging and Body Composition Study. J. Gerontol. Ser. A Boil. Sci. Med. Sci. 2016, 72, 513–519. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chuang, S.-Y.; Chang, H.-Y.; Lee, M.-S.; Chen, R.C.-Y.; Pan, W.-H. Skeletal muscle mass and risk of death in an elderly population. Nutr. Metab. Cardiovasc. Dis. 2014, 24, 784–791. [Google Scholar] [CrossRef] [PubMed]
- Chung, J.-Y.; Kang, H.-T.; Lee, D.-C.; Lee, H.-R.; Lee, Y.-J. Body composition and its association with cardiometabolic risk factors in the elderly: A focus on sarcopenic obesity. Arch. Gerontol. Geriatr. 2013, 56, 270–278. [Google Scholar] [CrossRef] [PubMed]
- Schorr, M.; Dichtel, L.E.; Gerweck, A.V.; Valera, R.D.; Torriani, M.; Miller, K.K.; Bredella, M.A. Sex differences in body composition and association with cardiometabolic risk. Biol. Sex Differ. 2018, 9, 28. [Google Scholar] [CrossRef] [PubMed]
- Ebbert, J.O.; Jensen, M.D. Fat Depots, Free Fatty Acids, and Dyslipidemia. Nutrients 2013, 5, 498–508. [Google Scholar] [CrossRef] [Green Version]
- Lee, Y.-C.; Chuang, P.-N.; Kuo, C.-S.; Lu, C.-W.; Yang, K.-C. The utility of visceral fat level measured by bioelectrical impedance analysis in predicting metabolic syndrome. Obes. Res. Clin. Pract. 2020, 14, 519–523. [Google Scholar] [CrossRef] [PubMed]
- Kannel, W.B.; Cupples, L.A.; Ramaswami, R.; Stokes, J.; Kreger, B.E.; Higgins, M. Regional obesity and risk of cardiovascular disease; the Framingham study. J. Clin. Epidemiol. 1991, 44, 183–190. [Google Scholar] [CrossRef]
- Tournadre, A.; Pereira, B.; Dutheil, F.; Giraud, C.; Courteix, D.; Sapin, V.; Frayssac, T.; Mathieu, S.; Malochet-Guinamand, S.; Soubrier, M. Changes in body composition and metabolic profile during interleukin 6 inhibition in rheumatoid arthritis. J. Cachexia Sarcopenia Muscle 2017, 8, 639–646. [Google Scholar] [CrossRef]
- Liu, X.Z.; Chen, D.S.; Xu, X.; Li, H.H.; Liu, L.Y.; Zhou, L.; Fan, J. Longitudinal associations between metabolic score for visceral fat and hyperuricemia in non-obese adults. Nutr. Metab. Cardiovasc. Dis. 2020, 30, 1751–1757. [Google Scholar] [CrossRef]
- Srikanthan, P.; Hevener, A.L.; Karlamangla, A.S. Sarcopenia Exacerbates Obesity-Associated Insulin Resistance and Dysglycemia: Findings from the National Health and Nutrition Examination Survey III. PLoS ONE 2010, 5, e10805. [Google Scholar] [CrossRef]
- Wang, T.; Feng, X.; Zhou, J.; Gong, H.; Xia, S.; Wei, Q.; Hu, X.; Tao, R.; Li, L.; Qian, F.; et al. Type 2 diabetes mellitus is associated with increased risks of sarcopenia and pre-sarcopenia in Chinese elderly. Sci. Rep. 2016, 6, 38937. [Google Scholar] [CrossRef] [Green Version]
- Mesinovic, J.; Zengin, A.; De Courten, B.; Ebeling, P.R.; Scott, D. Sarcopenia and type 2 diabetes mellitus: A bidirectional relationship. Diabetes Metab. Syndr. Obesity: Targets Ther. 2019, 12, 1057–1072. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, M.; Tan, Y.; Shi, Y.; Wang, X.; Liao, Z.; Wei, P. Diabetes and Sarcopenic Obesity: Pathogenesis, Diagnosis, and Treatments. Front. Endocrinol. 2020, 11, 568. [Google Scholar] [CrossRef] [PubMed]
- Kyle, U.G.; Bosaeus, I.; De Lorenzo, A.D.; Deurenberg, P.; Elia, M.; Gómez, J.M.; Heitmann, B.L.; Kent-Smith, L.; Melchior, J.-C.; Pirlich, M.; et al. Bioelectrical impedance analysis—Part II: Utilization in clinical practice. Clin. Nutr. 2004, 23, 1430–1453. [Google Scholar] [CrossRef]
- Jeon, K.C.; Kim, S.-Y.; Jiang, F.L.; Chung, S.; Ambegaonkar, J.P.; Park, J.-H.; Kim, Y.-J.; Kim, C.-H. Prediction Equations of the Multifrequency Standing and Supine Bioimpedance for Appendicular Skeletal Muscle Mass in Korean Older People. Int. J. Environ. Res. Public Health 2020, 17, 5847. [Google Scholar] [CrossRef]
- Antonio, J.; Kenyon, M.; Ellerbroek, A.; Carson, C.; Burgess, V.; Tyler-Palmer, D.; Mike, J.; Roberts, J.; Angeli, G.; Peacock, C. Comparison of Dual-Energy X-Ray Absorptiometry (DXA) versus a Multi-frequency Bioelectrical Impedance (InBody 770) Device for Body Composition Assessment after a 4-Week Hypoenergetic Diet. J. Funct. Morphol. Kinesiol. 2019, 4, 23. [Google Scholar] [CrossRef] [Green Version]
- Lemos, T.; Gallagher, D. Current body composition measurement techniques. Curr. Opin. Endocrinol. Diabetes Obes. 2017, 24, 310–314. [Google Scholar] [CrossRef]
- Pietrobelli, A.; Rubiano, F.; St-Onge, M.-P.; Heymsfield, S.B. New bioimpedance analysis system: Improved phenotyping with whole-body analysis. Eur. J. Clin. Nutr. 2004, 58, 1479–1484. [Google Scholar] [CrossRef] [Green Version]
- Examination Committee of Criteria for ‘Obesity Disease’ in Japan. New criteria for’obesity disease’in Japan. Circ. J. 2002, 66, 987–992. [Google Scholar] [CrossRef] [Green Version]
- Chen, L.-K.; Liu, L.-K.; Woo, J.; Assantachai, P.; Auyeung, T.-W.; Bahyah, K.S.; Chou, M.-Y.; Hsu, P.-S.; Krairit, O.; Lee, J.S.; et al. Sarcopenia in Asia: Consensus Report of the Asian Working Group for Sarcopenia. J. Am. Med Dir. Assoc. 2014, 15, 95–101. [Google Scholar] [CrossRef]
- Kim, T.N.; Yang, S.J.; Yoo, H.J.; Lim, K.I.; Kang, H.J.; Song, W.; Seo, J.A.; Kim, S.G.; Kim, N.H.; Baik, S.H.; et al. Prevalence of sarcopenia and sarcopenic obesity in Korean adults: The Korean sarcopenic obesity study. Int. J. Obes. 2009, 33, 885–892. [Google Scholar] [CrossRef] [Green Version]
- Yang, R.; Zhang, Y.; Shen, X.; Yan, S. Sarcopenia associated with renal function in the patients with type 2 diabetes. Diabetes Res. Clin. Pract. 2016, 118, 121–129. [Google Scholar] [CrossRef]
- Kohara, K. Sarcopenic obesity in aging population: Current status and future directions for research. Endocrine 2014, 45, 15–25. [Google Scholar] [CrossRef]
- Atlantis, E.; Martin, S.A.; Haren, M.T.; Taylor, A.W.; Wittert, G.A. Inverse associations between muscle mass, strength, and the metabolic syndrome. Metab. Clin. Exp. 2009, 58, 1013–1022. [Google Scholar] [CrossRef]
- Seidell, J.C.; Visscher, T. Body weight and weight change and their health implications for the elderly. Eur. J. Clin. Nutr. 2000, 54, S33–S39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okorodudu, D.; Jumean, M.F.; Montori, V.M.; Romero-Corral, A.; Somers, V.K.; Erwin, P.J.; Lopez-Jimenez, F. Diagnostic performance of body mass index to identify obesity as defined by body adiposity: A systematic review and meta-analysis. Int. J. Obes. 2010, 34, 791–799. [Google Scholar] [CrossRef] [Green Version]
- Molarius, A.; Seidell, J.C.; Visscher, T.L.; Hofman, A. Misclassification of high-risk older subjects using waist action levels established for young and middle-aged adults—results from the Rotterdam Study. J. Am. Geriatr. Soc. 2000, 48, 1638–1645. [Google Scholar] [CrossRef]
- Chang, C.-J.; Wu, C.-H.; Yao, W.-J.; Yang, Y.-C.; Wu, J.-S.; Lu, F.-H. Low body mass index but high percent body fat in Taiwanese subjects: Implications of obesity cutoffs. Int. J. Obes. 2003, 27, 253–259. [Google Scholar] [CrossRef] [Green Version]
- Chodzko-Zajko, W.J.; Proctor, D.N.; Singh, M.A.F.; Minson, C.T.; Nigg, C.R.; Salem, G.J.; Skinner, J.S. Exercise and Physical Activity for Older Adults. Med. Sci. Sports Exerc. 2009, 41, 1510–1530. [Google Scholar] [CrossRef] [PubMed]
- Janssen, I.; Heymsfield, S.B.; Wang, Z.; Ross, R. Skeletal muscle mass and distribution in 468 men and women aged 18–88 yr. J. Appl. Physiol. 2000, 89, 81–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hong, S.; Chang, Y.; Jung, H.-S.; Yun, K.E.; Shin, H.; Ryu, S. Relative muscle mass and the risk of incident type 2 diabetes: A cohort study. PLoS ONE 2017, 12, e0188650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mizgier, M.L.; Casas, M.; Contreras-Ferrat, A.; Llanos, P.; Galgani, J.E. Potential role of skeletal muscle glucose metabolism on the regulation of insulin secretion. Obes. Rev. 2014, 15, 587–597. [Google Scholar] [CrossRef] [PubMed]
- Marinou, K.; Hodson, L.; Vasan, S.K.; Fielding, B.A.; Banerjee, R.; Brismar, K.; Koutsilieris, M.; Clark, A.; Neville, M.J.; Karpe, F. Structural and Functional Properties of Deep Abdominal Subcutaneous Adipose Tissue Explain Its Association With Insulin Resistance and Cardiovascular Risk in Men. Diabetes Care 2014, 37, 821–829. [Google Scholar] [CrossRef] [Green Version]
- Kuwahara, K.; Honda, T.; Nakagawa, T.; Yamamoto, S.; Hayashi, T.; Mizoue, T. Body mass index trajectory patterns and changes in visceral fat and glucose metabolism before the onset of type 2 diabetes. Sci. Rep. 2017, 7, srep43521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lahav, Y.; Goldstein, N.; Gepner, Y. Comparison of body composition assessment across body mass index categories by two mul-tifrequency bioelectrical impedance analysis devices and dual-energy X-ray absorptiometry in clinical settings. Eur. J. Clin. Nutr. 2021, 1–8. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Overall N = 2404 N (%)/Mean ± SD | Male N = 1275 (53.0%) N (%)/Mean ± SD | Female N = 1129 (47.0%) N (%)/Mean ± SD |
|---|---|---|---|
| Age | 63.2 ± 12.9 | 60.6 ± 12.4 | 69.9 ± 11.6 |
| 18–<35 | 53 (2.2%) | 33 (2.6%) | 20 (1.8%) |
| ≧35–<65 | 1196 (49.8%) | 719 (56.4%) | 477 (42.2%) |
| ≧65–<75 | 659 (27.4%) | 305 (23.9%) | 354 (31.4%) |
| ≧75 | 496 (20.6%) | 218 (17.1%) | 278 (24.6%) |
| Disease duration | 12.5 ± 7.9 | 12.1 ± 7.9 | 12.9 ± 7.9 |
| A1C | 7.3 ± 1.1 | 7.3 ± 1.1 | 7.1 ± 1.1 |
| Height (m) | 1.60 ± 0.09 | 1.66 ± 0.07 | 1.53 ± 0.06 |
| BW (kg) | 65.8 ± 14.0 | 71.4 ± 13.7 | 59.6 ± 11.6 |
| BMI (kg/m2) | 26.9 ± 4.1 | 25.7 ± 4.2 | 25.4 ± 4.4 |
| <18.5 | 44 (1.8%) | 23 (1.8%) | 21 (1.9%) |
| ≧18.5–<24 | 890 (37.0%) | 426 (33.4%) | 464 (41.1%) |
| ≧24–<27 | 692 (28.8%) | 406 (31.8%) | 286 (25.3%) |
| ≧27 | 778 (32.4%) | 420 (32.9%) | 358 (31.7%) |
| BFM (kg) | 20.9 ± 8.0 | 19.8 ± 8.0 | 22.2 ± 7.8 |
| FFM (kg) | 44.9 ± 9.7 | 51.6 ± 7.8 | 37.4 ± 5.2 |
| PBF (%) | 31.4 ± 8.1 | 27.0 ± 6.6 | 36.3 ± 6.6 |
| VFA | 102.3 ± 42.6 | 91.0 ± 38.2 | 115.1 ± 43.7 |
| ASM (kg) | 18.2 ± 4.8 | 21.5 ± 3.7 | 14.5 ± 2.7 |
| SMI (kg/m2) | 7.0 ± 1.2 | 7.7 ± 0.9 | 6.1 ± 0.9 |
| Variable | Overall (N = 2404) | Male (N = 1275) | Female (N = 1129) | |||
|---|---|---|---|---|---|---|
| Low Muscle Mass | Sarcopenic Obesity | Low Muscle Mass | Sarcopenic Obesity | Low Muscle Mass | Sarcopenic Obesity | |
| Age | ||||||
| 18<35 | 5 (9.4%) | 3 (5.7%) | 2 (6.1%) | 0 (0.0%) | 3 (15.0%) | 3 (15.0%) |
| ≧35–<65 | 195 (16.3%) | 112 (9.4%) | 88 (12.2%) | 36 (5.0%) | 107 (22.4%) | 76 (15.9%) |
| ≧65–<75 | 204 (31.0%) | 133 (20.2%) | 81 (26.6%) | 39 (12.8%) | 123 (34.7%) | 94 (26.6%) |
| ≧75 | 269 (54.2%) | 201 (40.5%) | 118 (54.1%) | 81 (37.2%) | 151 (54.3%) | 120 (43.2%) |
| Total | 673 (28.0%) | 449 (18.7%) | 289 (22.7%) | 156 (12.2%) | 384 (34.0%) | 293 (26.0%) |
| Category | Low Muscle Mass | Sarcopenic Obesity | Obesity | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| BMI | Overall (N = 2404) | Male (N = 1275) | Female (N = 1129) | Overall (N = 2404) | Male (N = 1275) | Female (N = 1129) | Overall (N = 2404) | Male (N = 1275) | Female (N = 1129) | |
| <18.5 | 42 (95.5%) | 22 (95.7%) | 20 (95.2%) | 3 (6.8%) | 0 (0.0%) | 3 (14.3%) | 3 (6.8%) | 0 (0.0%) | 3 (14.3%) | |
| ≧18.5–<24 | 495 (55.6%) | 216 (50.7%) | 279 (60.1%) | 310 (34.8%) | 105 (24.6%) | 205 (44.2%) | 425 (47.8%) | 129 (30.3%) | 296 (63.8%) | |
| ≧24–<27 | 114 (16.5%) | 43 (10.6%) | 71 (24.8%) | 114 (16.5%) | 43 (10.6%) | 71 (24.8%) | 537 (77.6%) | 262 (64.5%) | 275 (96.2%) | |
| ≧27 | 22 (2.8%) | 8 (1.9%) | 14 (3.9%) | 22 (2.8%) | 8 (1.9%) | 14 (3.9%) | 753 (96.8%) | 395 (94.0%) | 358 (100.0%) | |
| Total | 673 (28.0%) | 289 (22.7%) | 384 (34.0%) | 449 (18.7%) | 156 (12.2%) | 293 (26.0%) | 1718 (71.5%) | 786 (61.6%) | 932 (82.6%) | |
| Variable | 18–<35 | ≧35–<65 | ≧65–<75 | ≧75 | ||||
|---|---|---|---|---|---|---|---|---|
| Male (N = 33) | Female (N = 20) | Male (N = 719) | Female (N = 477) | Male (N = 305) | Female (N = 354) | Male (N = 218) | Female (N = 278) | |
| Height (m) | 1.73 ± 0.06 | 1.60 ± 0.05 | 1.68 ± 0.06 *** | 1.55 ± 0.06 ** | 1.64 ± 0.05 *** | 1.52 ± 0.05 | 1.63 ± 0.06 *** | 1.50 ± 0.06 |
| BW (kg) | 85.8 ± 21.3 | 68.1 ± 13.3 | 74.6 ± 13.8 *** | 62.6 ± 12.7 | 68.2 ± 11.1 *** | 57.9 ± 9.7 *** | 63.2 ± 9.0 *** | 55.8 ± 10.0 *** |
| BMI (kg/m2) | 28.5 ± 6.7 | 26.6 ± 4.6 | 26.3 ± 4.3 * | 26.1 ± 4.9 | 25.3 ± 3.7 *** | 25.0 ± 3.9 | 23.9 ± 3.1 *** | 24.8 ± 3.9 |
| BFM (kg) | 25.4 ± 14.3 | 26.3 ± 8.5 | 20.4 ± 8.2 ** | 23.2 ± 8.7 | 19.0 ± 7.2 *** | 21.4 ± 7.0 * | 18.1 ± 5.9 *** | 21.1 ± 6.7 * |
| FFM (kg) | 60.4 ± 9.1 | 41.8 ± 6.1 | 54.1 ± 7.5 *** | 39.4 ± 5.5 | 49.2 ± 5.7 *** | 36.5 ± 4.1 *** | 45.1 ± 5.0 *** | 34.7 ± 4.5 *** |
| PBF (%) | 27.7 ± 9.3 | 37.9 ± 5.7 | 26.6 ± 6.6 | 36.0 ± 6.9 | 27.0 ± 6.6 | 36.1 ± 6.5 | 28.1 ± 6.1 | 37.0 ± 6.3 |
| VFA (cm2) | 108.2 ± 62.3 | 127.3 ± 43.4 | 91.8 ± 39.2 | 115.5 ± 46.1 | 88.3 ± 36.3 * | 112.4 ± 42.7 | 89.6 ± 31.8 * | 117.0 ± 40.7 |
| ASM (kg) | 25.4 ± 3.9 | 16.8 ± 2.8 | 22.7 ± 3.6 *** | 15.6 ± 2.7 | 20.4 ± 2.8 *** | 14.0 ± 2.1 *** | 18.5 ± 2.6 *** | 13.0 ± 2.4 *** |
| SMI (kg/m2) | 8.4 ± 1.0 | 6.5 ± 0.8 | 8.0 ± 0.9 * | 6.4 ± 0.9 | 7.6 ± 0.8 *** | 6.0 ± 0.7* | 7.0 ± 0.8 *** | 5.7 ± 0.8 *** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, C.-L.; Yu, N.-C.; Wu, H.-C.; Lee, Y.-Y.; Lin, W.-C.; Chiu, I.-Y.; Chien, W.-C.; Liu, Y.-C. Association of Body Composition with Type 2 Diabetes: A Retrospective Chart Review Study. Int. J. Environ. Res. Public Health 2021, 18, 4421. https://doi.org/10.3390/ijerph18094421
Lin C-L, Yu N-C, Wu H-C, Lee Y-Y, Lin W-C, Chiu I-Y, Chien W-C, Liu Y-C. Association of Body Composition with Type 2 Diabetes: A Retrospective Chart Review Study. International Journal of Environmental Research and Public Health. 2021; 18(9):4421. https://doi.org/10.3390/ijerph18094421
Chicago/Turabian StyleLin, Chia-Ling, Neng-Chun Yu, Hsueh-Ching Wu, Yung-Yen Lee, Wan-Chun Lin, I-Ying Chiu, Wu-Chien Chien, and Yuan-Ching Liu. 2021. "Association of Body Composition with Type 2 Diabetes: A Retrospective Chart Review Study" International Journal of Environmental Research and Public Health 18, no. 9: 4421. https://doi.org/10.3390/ijerph18094421