
Effects of Mirror Therapy Combined with EMG-Triggered Functional Electrical Stimulation to Improve on Standing Balance and Gait Ability in Patient with Chronic Stroke

Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Protocol
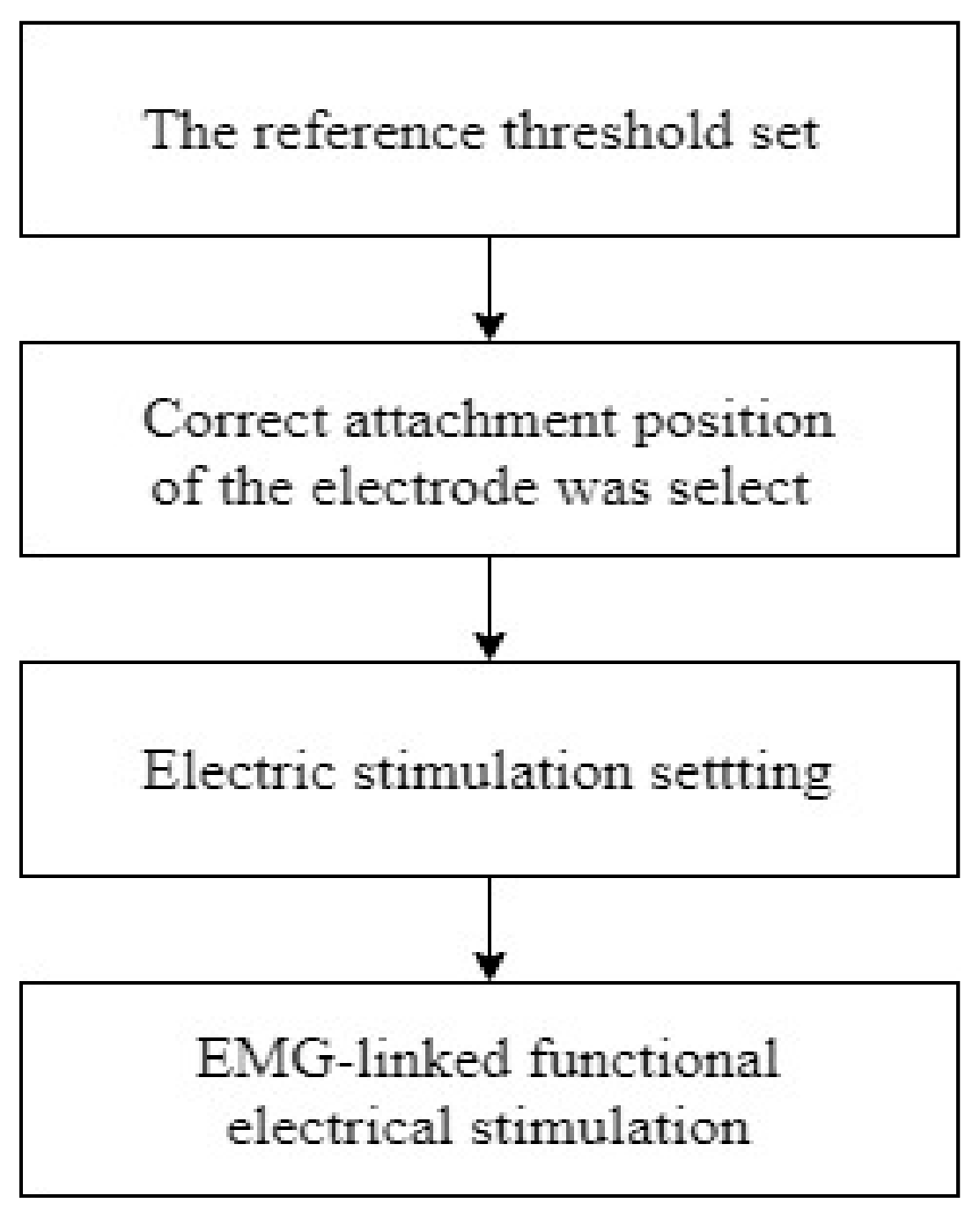
2.2.1. MT-FE Group
2.2.2. MT Group
2.2.3. Conservative Treatment Group (CON)
2.3. Measurement
2.3.1. Biorscue (COP, LOS)
2.3.2. Berg Balance Scale (BBS)
2.3.3. Functional Reach Test (FRT)
2.3.4. 10 m Walk Test (10 m WT)
2.4. Statistical Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Darcy, A.U. Neurological Rehabilitation, 5th ed.; Mosby Elsevier: St. Louis, MO, USA, 2006; pp. 857–858. [Google Scholar]
- Mayo, N.E.; Wood-Dauphinee, S.; Côté, R.; Durcan, L.; Carlton, J. Activity, participation, and quality of life 6 months poststroke. Arch. Phys. Med. Rehabil. 2002, 83, 1035–1042. [Google Scholar] [CrossRef]
- Tyson, S.F.; Hanley, M.; Chillala, J.; Selley, A.; Tallis, R.C. Balance disability after stroke. Phys. Ther. 2006, 86, 30–38. [Google Scholar] [CrossRef] [Green Version]
- Srivastava, A.; Taly, A.B.; Gupta, A.; Kumar, S.; Murali, T. Post-stroke balance training: Role of force platform with visual feedback technique. J. Neurol. Sci. 2009, 287, 89–93. [Google Scholar] [CrossRef]
- Brown, L.A.; Sleik, R.J.; Winder, T.R. Attentional demands for static postural control after stroke. Arch. Phys. Med. Rehabil. 2002, 83, 1732–1735. [Google Scholar] [CrossRef]
- Walker, C.; Brouwer, B.J.; Culham, E.G. Use of visual feedback in retraining balance following acute stroke. Phys. Ther. 2000, 80, 886–895. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonan, I.V.; Yelnik, A.P.; Colle, F.M.; Michaud, E.; Panigot, B.; Roth, P.; Guichard, J.P.; Vicaut, E. Reliance on visual information after stroke. Part II: Effectiveness of a balance rehabilitation program with visual cue deprivation after stroke: A randomized controlled trial. Arch. Phys. Med. Rehabil. 2004, 85, 274–278. [Google Scholar] [CrossRef] [PubMed]
- Ring, H.; Rosenthal, N. Contralled study of neuroprosthetic functional electrical stimulation in sub-acute post-stroke rehabilitation. J. Rehabil. Med. 2005, 37, 32–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, D.H.; Kim, K.H.; Lee, S.M. Effects of visual restriction and unstable base dual-task training on balance and concentration ability in persons with stroke. Phys. Ther. Rehabil. Sci. 2016, 5, 193–197. [Google Scholar] [CrossRef] [Green Version]
- Pandian, S.; Arya, K.N.; Davidson, E.W. Comparison of Brunnstrom movement therapy and Motor Relearning Program in rehabilitation of post-stroke hemiparetic hand: A randomized trial. J. Bodyw. Mov. Ther. 2012, 16, 330–337. [Google Scholar] [CrossRef]
- Kim, D.H.; Kim, K.H.; Lee, S.M. The effects of virtual reality training with upper limb sensory exercise stimulation on the arom of upper limb joints, function, and concentration on chronic stroke patients. Phys. Med. Rehabil. Kurortmed. 2019, 30, 86–94. [Google Scholar] [CrossRef]
- Kim, D.H.; Kim, K.H. A Convergence Study on the Effects of functional electrical stimulation with mirror therapy on balance and gait ability in chronic stroke patients. J. Korea Converg. Soc. 2018, 9, 109–120. [Google Scholar] [CrossRef]
- Sutbeyaz, S.; Yavuzer, G.; Sezer, N.; Koseoglu, B.F. Mirror therapy enhances lower-extremity motor recovery and motor functioning after stroke: A randomized controlled trial. Am. J. Phys. Med. Rehabil. 2007, 88, 555–559. [Google Scholar] [CrossRef] [PubMed]
- Steven, L.W.; Pamela, A.C.; Michael, E.; Audrey, L.A.; Bryn, M.; Aimee, P. Assessing Wolf Motor Function Test as outcome measure for research in patients after stroke. J. Am. Heart Assoc. 2001, 32, 1635–1639. [Google Scholar]
- Garry, M.I.; Loftus, A.; Summers, J.J. Mirror, mirror on the wall: Viewing a mirror reflection of unilateral hand movements facilitates ipsilateral M1 excitability. Exp. Brain Res. 2005, 163, 118–122. [Google Scholar] [CrossRef] [PubMed]
- Kapadia, N.M.; Nagai, M.K.; Ziavanovic, V.; Bernstein, J.; Woodhouse, J.; Rumney, P.; Popovic, M.R. Functional Electrical Stimulation Therapy for Recovery of Reaching and Grasping in severe Chronic Pediatric Stroke Patient. J. Child. Neurol. 2013, 29, 493–502. [Google Scholar] [CrossRef]
- Kowalczewski, J.; Gritsenko, V.; Ashworth, N.; Ellaway, P.; Prochazka, A. Upper-extremity functional electric stimulation–assisted exercises on a workstation in the subacute phase of stroke recovery. Arch. Phys. Med. Rehabil. 2007, 88, 833–839. [Google Scholar] [CrossRef]
- De Kroon, J.R.; IJzerman, M.J. Electrical stimulation of the upper extremity in stroke: Cyclic versus EMG-triggered stimulation. Clin. Rehabil. 2008, 22, 690–697. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.H.; Han, E.Y.; Kim, T.H.; Jumg, H.Y. Comparison of Cortical Excitability Between the EMG-triggered Functional Electrical Stimulation (FES) and FES in Hemiplegic Stroke. Korean J. Stroke 2005, 7, 159–164. [Google Scholar]
- Galeazzi, G.M.; Monzani, D.; Gherpelli, C.; Covezzi, R.; Guaraldi, G.P. Posturographic stabilisation of healthy participants exposed to full-length mirror image is inversely related to body-image preoccupations. Neurosci. Lett. 2006, 410, 71–75. [Google Scholar] [CrossRef]
- Lee, D.; Lee, G.; Jeong, J. Mirror Therapy with Neuromuscular Electrical Stimulation for improving motor function of stroke survivors: A pilot randomized clinical study. Technol. Health Care 2016, 27, 503–511. [Google Scholar] [CrossRef]
- Kojima, K.; Ikuno, K.; Morii, Y.; Tokuhisa, K.; Morimoto, S.; Shomoto, K. Feasibility study of a combined treatment of electromyography-triggered neuromuscular stimulation and mirror therpy in stroke patient: A randomized crossover trial. NeuroRehabilitation 2014, 34, 235–244. [Google Scholar] [CrossRef] [PubMed]
- Ji, S.G.; Kim, M.K. The effects of mirror therapy on the gait of subacute stroke patient; a randomized controlled trial. Clin. Rehabil. 2014, 29, 348–354. [Google Scholar] [CrossRef]
- Cauraugh, J.; Light, K.; Kim, S.; Thigpen, M.; Behrman, A. Chronic motor dysfunction after stroke: Recovering wrist and finger extension by electromyography-trigered neuromuscular stimulation. Stroke 2000, 31, 1360–1364. [Google Scholar] [CrossRef] [PubMed]
- Bolton, D.A.; Cauraugh, J.H.; Hausenblas, H.A. Electromyogram triggered neuromuscular stimulation and stroke motor recovery of arm/hand functions: A meta analysis. J. Neurol. Sci. 2004, 223, 121–127. [Google Scholar] [CrossRef]
- Latash, M.L.; Ferreira, S.S.; Wieczorek, S.A.; Duarte, M. Movement sway: Changes in postural sway during voluntary shifts of the center of pressure. Exp. Brain Res. 2003, 150, 314–324. [Google Scholar] [CrossRef] [PubMed]
- Berg, K.; Wood-Dauphinee, S.; Williams, J.I.; Gayton, D. Measuring balance in the elderly: Preliminary development of an instrument. Physiother. Can. 1989, 41, 304–311. [Google Scholar] [CrossRef]
- Bogle Thorbahn, L.D.; Newton, R. A Use of the Berg Balance test to predict falls in elderly persons. Phys. Ther. 1996, 76, 576–585. [Google Scholar] [CrossRef]
- Duncan, P.W.; Weiner, D.K.; Chandler, J.; Studenski, S. Functional reach: A new clinical measure of balance. J. Gerontol. 1990, 45, M192–M197. [Google Scholar] [CrossRef]
- Lamb, S.E.; Ferrucci, L.; Volapto, S.; Fried, L.P.; Guralnik, J.M. Risk factors for falling in home-dwelling older women with stroke: The Women’ s Health and Aging Study. Stroke 2003, 34, 494–501. [Google Scholar] [CrossRef] [Green Version]
- Patterson, S.L.; Forrester, L.W.; Rodgers, M.M.; Ryan, A.S.; Ivey, F.M.; Sorkin, J.D.; Macko, R.F. Determinants of walking function after stroke: Differences by deficit severity. Arch. Phys. Med. Rehabil. 2007, 88, 115–119. [Google Scholar] [CrossRef] [PubMed]
- Van Vliet, P.M.; Wulf, G. Extrinsic feedback for motor learning after stroke: What is the evidence? Disabil. Rehabil. 2006, 28, 831–840. [Google Scholar] [CrossRef]
- Rizzolatti, G.; Craighero, L. The mirror-neuron system. Annu. Rev. Neurosci. 2004, 27, 169–192. [Google Scholar] [CrossRef] [Green Version]
- Maeda, F.; Mazziotta, J.; Iacoboni, M. Transcranial magnetic stimulation studies of the human mirror neuron system. Int. Congr. Ser. 2002, 1232, 889–894. [Google Scholar] [CrossRef]
- Pinsault, N.; Vuillerme, N. The effects of scale display of visual feedback on postural control during quiet standing in healthy elderly subjects. Arch. Phys. Med. Rehabil. 2008, 89, 1772–1774. [Google Scholar] [CrossRef] [PubMed]
- Robertson, J.A.; Eng, J.J.; Hung, C. The effect of functional electrical stimulation on balance function and balance confidence in community-dwelling individuals with stroke. Physiother. Can. 2010, 62, 114–119. [Google Scholar] [CrossRef] [Green Version]
- Francisco, G.; Chae, J.; Chawla, H.; Kirshblum, S.; Zorowitz, R.; Lewis, G.; Pang, S. Electromyogram-triggered neuromuscular stimulation for improving the arm function of acute stroke survivors: A randomized pilot study. Arch. Phys. Med. Rehabil. 1998, 79, 570–575. [Google Scholar] [CrossRef]
- Celnik, P.; Stefan, K.; Hummel, F.; Duque, J.; Classen, J.; Cohen, L.G. Encoding a motor memory in the older adult by action observation. Neuroimage 2006, 29, 677–684. [Google Scholar] [CrossRef]
- Choi, J.; Park, S. The effect of weight shifting and motor imagery training on the ability of weight shifting task and functional activity in stroke patients. J. Spec. Educ. Rehabil. Sci. 2009, 48, 169–182. [Google Scholar]
- Kim, J.H.; Chung, Y.; Kim, Y.; Hwang, S. Functional electrical stimulation applied to gluteus medius and tibialis anterior corresponding gait cycle for stroke. Gait Posture 2012, 36, 65–67. [Google Scholar] [CrossRef]
- Yavuzer, G.; Eser, F.; Karakus, D.; Karaoglan, B.; Stam, H.J. The effects of balance training on gait late after stroke: A randomized controlled trial. Clin. Rehabil. 2006, 20, 960–969. [Google Scholar] [CrossRef]
- Bradley, L.; Hart, B.B.; Mandana, S.; Flowers, K.; Riches, M.; Sanderson, P. Electromyographic biofeedback for gait training after stroke. Clin. Rehabil. 1998, 12, 11–22. [Google Scholar] [CrossRef] [PubMed]
- Stevens, J.A.; Stoykov, M.E.P. Using motor imagery in the rehabilitation of hemiparesis. Arch. Phys. Med. Rehabil. 2003, 84, 1090–1092. [Google Scholar] [CrossRef]
- Ashford, D.; Bennett, S.J.; Davids, K. Observational modeling effects for movement dynamics and movement outcome measures across differing task constraints: A meta-analysis. J. Mot. Behav. 2006, 38, 185–205. [Google Scholar] [CrossRef]
- Thirumala, P.; Hier, D.B.; Patel, P. Motor recovery after stroke: Lessons from functional brain imaging. Neurol. Res. 2002, 24, 453–458. [Google Scholar] [CrossRef] [PubMed]
- Dursun, E.; Dursun, N.; Ural, C.E.; Çakci, A. Glenohumeral joint subluxation and reflex sympathetic dystrophy in hemiplegic patients. Arch. Phys. Med. Rehabil. 2000, 81, 944–946. [Google Scholar] [CrossRef] [PubMed]
- Boyaci, A.; Topuz, O.; Alkan, H.; Ozgen, M.; Sarsan, A.; Yildiz, N.; Ardic, F. Comparison of the effectiveness of active and passive neuromuscular electrical stimulation of hemiplegic upper extremities: A randomized, controlled trial. Int. J. Rehabil. Res. 2013, 36, 315–322. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y. The effects of EMG-triggered functional electrical stimulation on upper extremity function in stroke patients. Phys. Ther. Rehabil. Sci. 2013, 2, 1–6. [Google Scholar]


{kind=link}
| Variables | MT-EF Group (n = 20)/M ± SD | MT Group (n = 20)/M ± SD | CON Group (n = 20)/M ± SD | F | p |
|---|---|---|---|---|---|
| Age (year) | 56.05 ± 14.43 | 57.45 ± 5.27 | 59.70 ± 8.65 | 0.655 | 0.523 |
| Height (cm) | 163.91 ± 6.96 | 164.67 ± 8.69 | 161.09 ± 7.80 | 1.154 | 0.323 |
| Weight (kg) | 62.80 ± 7.59 | 64.52 ± 8.04 | 64.09 ± 9.71 | 0.222 | 0.802 |
| MMSE (score) | 27.05 ± 1.64 | 27.30 ± 1.45 | 27.70 ± 1.95 | 0.750 | 0.477 |
| Gender (male/famale) | 12/8 | 9/11 | 10/10 | 0.934 | 0.627 |
| Diagnosis (I/H) | 11/9 | 5/7 | 8/12 | 0.934 | 0.627 |
| Affected side (Left/Right) | 9/11 | 10/10 | 9/11 | 0.134 | 0.935 |
| COP Length (cm) | 31.65 ± 3.28 | 36.60 ± 6.82 | 33.15 ± 4.56 | 1.838 | 0.221 |
| LOS (cm2) | 5948.05 ± 2242.04 | 5691.00 ± 2075.61 | 5417.45 ± 2369.64 | 0.283 | 0.799 |
| BBS (score) | 39.50 ± 5.88 | 39.30 ± 6.12 | 38.40 ± 4.85 | 0.216 | 0.605 |
| FRT (cm) | 17.15 ± 7.73 | 16.35 ± 6.60 | 14.81 ± 7.68 | 0.523 | 0.605 |
| 10 m walk test (m/s) | 0.62 ± 0.27 | 0.74 ± 0.34 | 0.66 ± 0.31 | 0.783 | 0.605 |
| Variables | MT-EF Group (A) (n = 20)/M ± SD | MT Group (B) (n = 20)/M ± SD | CON Group (C) (n = 20)/M ± SD | F | p |
|---|---|---|---|---|---|
| COP Length (cm) | |||||
| pre | 31.65 ± 3.28 | 36.60 ± 6.82 | 33.15 ± 4.56 | 1.838 | 0.221 |
| post | 26.96 ± 3.29 | 33.54 ± 7.05 | 30.16 ± 4.05 | ||
| change | 4.69 ± 0.76 | 3.06 ± 0.85 | 2.30 ± 2.21 | 10.009 | 0.000 A|BC |
| t | 27.518163 | 16.087682 | 6.068127 | ||
| p | 0.000 | 0.000 | 0.000 | ||
| LOS (cm2) | |||||
| pre | 5948.05 ± 2242.04 | 5691.00 ± 2075.61 | 5417.45 ± 2369.64 | 0.283 | 0.799 |
| post | 7127.90 ± 2400.43 | 6218.75 ± 2082.27 | 5841.20 ± 2465.15 | ||
| change | −1179.85 ± 1036.26 | −527.75 ± 204.97 | −423.75 ± 237.93 | 8.601 | 0.001 A|BC |
| t | −5.091808 | −11.514431 | −7.964972 | ||
| p | 0.000 | 0.000 | 0.000 | ||
| BBS (score) | |||||
| pre | 39.50 ± 5.88 | 39.30 ± 6.12 | 38.40 ± 4.85 | 0.216 | 0.605 |
| post | 44.05 ± 5.87 | 42.45 ± 5.92 | 41.55 ± 4.83 | ||
| change | −4.55 ± 2.24 | −3.15 ± 1.42 | −3.15 ± 1.50 | 4.231 | 0.019 A|BC |
| t | −9.102396 | −9.889860 | −9.413531 | ||
| p | 0.000 | 0.000 | 0.000 | ||
| FRT (cm) | |||||
| pre | 17.15 ± 7.73 | 16.35 ± 6.60 | 14.81 ± 7.68 | 0.523 | 0.605 |
| post | 22.30 ± 8.07 | 18.15 ± 6.42 | 18.30 ± 7.78 | ||
| change | −5.15 ± 1.18 | −1.80 ± 2.65 | −3.49 ± 1.61 | 15.300 | 0.000 A|BC |
| t | −19.483491 | −3.040270 | −9.695429 | ||
| p | 0.000 | 0.007 | 0.000 | ||
| 10 m walk test (m/s) | |||||
| pre | 0.62 ± 0.27 | 0.74 ± 0.34 | 0.66 ± 0.31 | 0.783 | 0.605 |
| post | 0.82 ± 0.3 | 0.84 ± 0.38 | 0.72 ± 0.30 | ||
| change | −0.19 ± 0.13 | −0.10 ± 0.13 | −0.07 ± 0.06 | 6.909 | 0.002 A|BC |
| t | −6.840639 | −3.492978 | −5.285515 | ||
| p | 0.000 | 0.002 | 0.000 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, D.-H.; Jang, S.-H. Effects of Mirror Therapy Combined with EMG-Triggered Functional Electrical Stimulation to Improve on Standing Balance and Gait Ability in Patient with Chronic Stroke. Int. J. Environ. Res. Public Health 2021, 18, 3721. https://doi.org/10.3390/ijerph18073721
Kim D-H, Jang S-H. Effects of Mirror Therapy Combined with EMG-Triggered Functional Electrical Stimulation to Improve on Standing Balance and Gait Ability in Patient with Chronic Stroke. International Journal of Environmental Research and Public Health. 2021; 18(7):3721. https://doi.org/10.3390/ijerph18073721
Chicago/Turabian StyleKim, Dong-Hoon, and Sang-Hun Jang. 2021. "Effects of Mirror Therapy Combined with EMG-Triggered Functional Electrical Stimulation to Improve on Standing Balance and Gait Ability in Patient with Chronic Stroke" International Journal of Environmental Research and Public Health 18, no. 7: 3721. https://doi.org/10.3390/ijerph18073721