
The Relationship between Emotional Intelligence, Obesity and Eating Disorder in Children and Adolescents: A Systematic Mapping Review

 , , ,
, , ,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
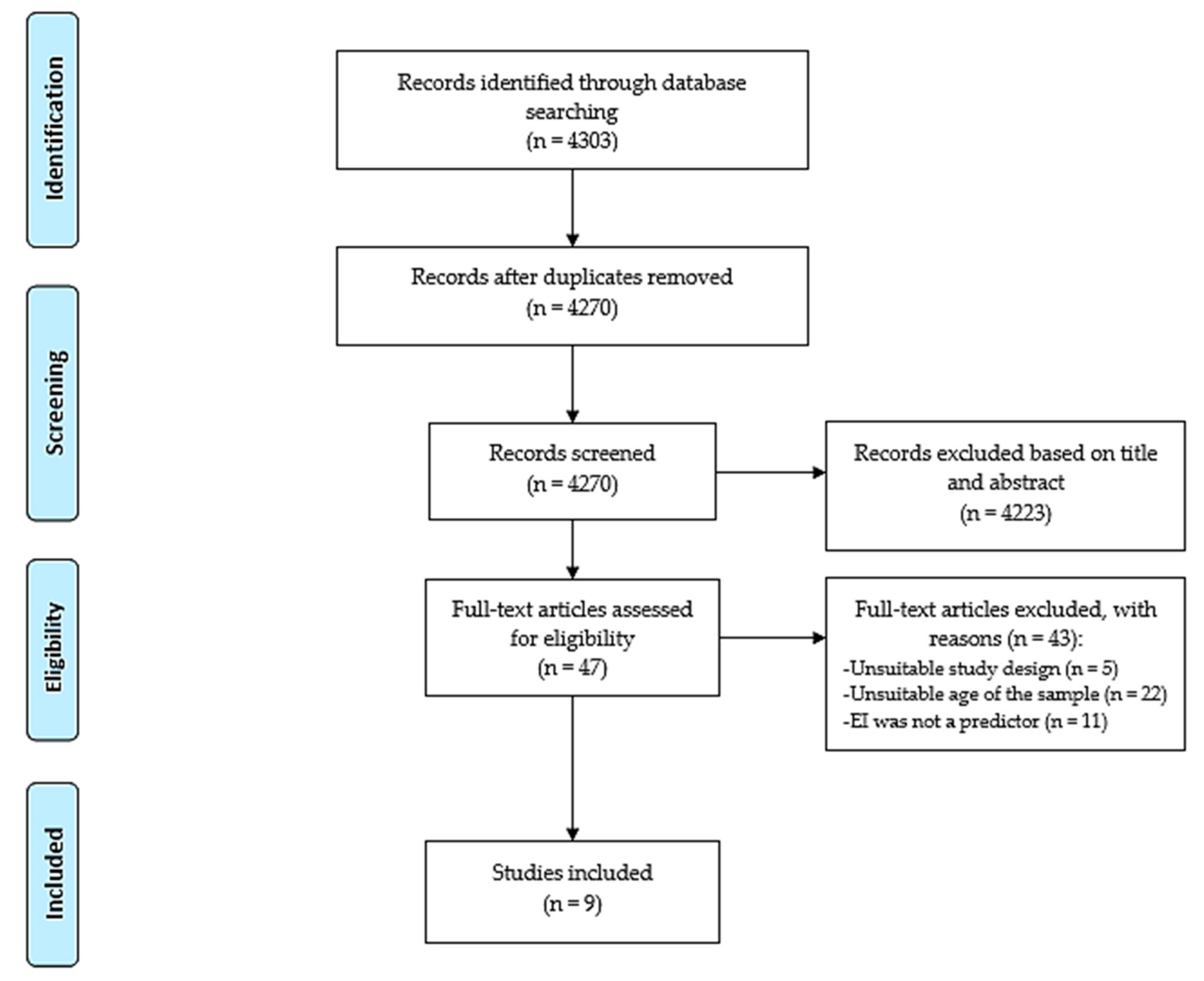
2.3. Study Selection
2.4. Assessment of Risk of Bias
2.5. Data Extraction and Synthesis
3. Results
3.1. Characteristics of Selected Articles
3.2. Methodological Quality of Included Studies
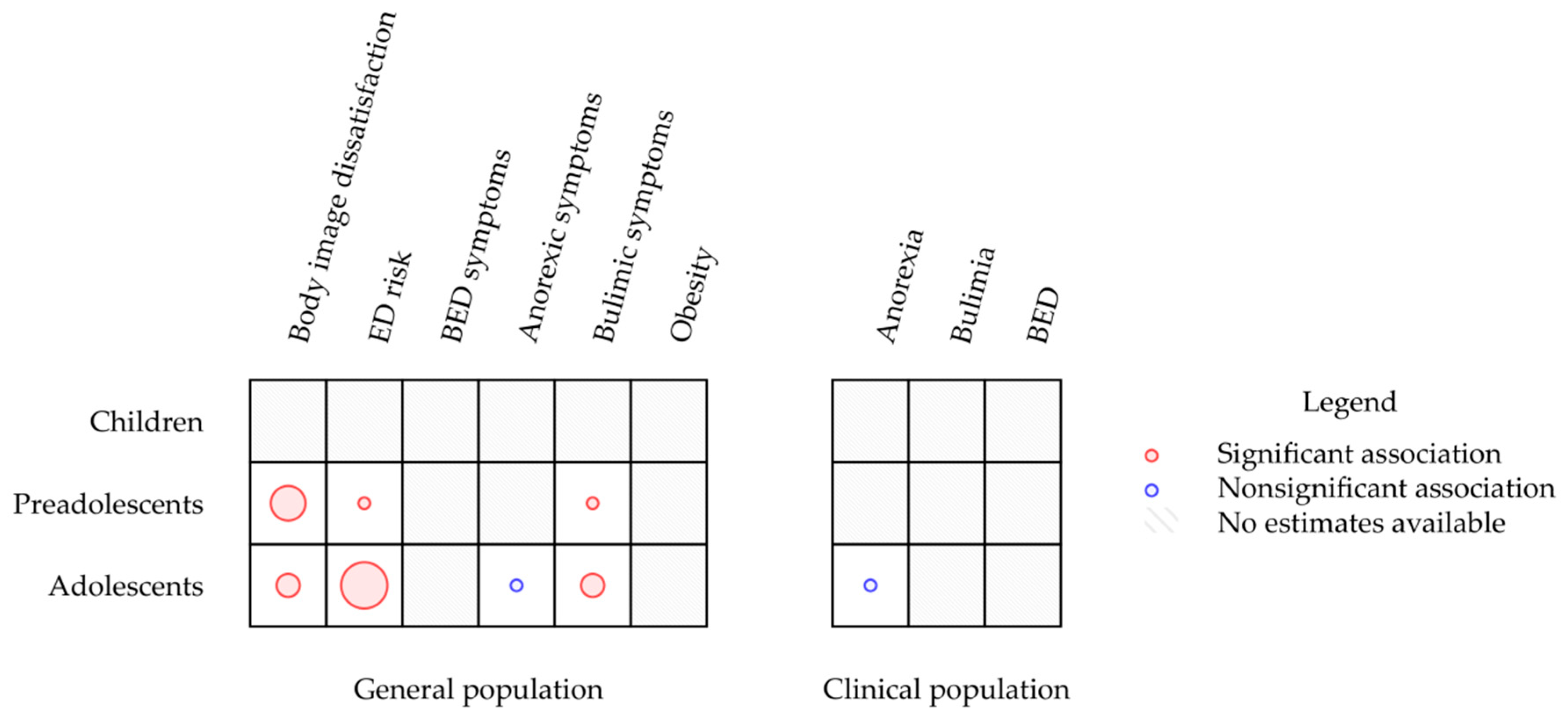
3.3. Emotional Intelligence and Eating Disorders
4. Discussion
4.1. Strengths and Limitations
4.2. Future Research and Practical Directions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Borrello, M.; Pietrabissa, G.; Ceccarini, M.; Manzoni, G.M.; Castelnuovo, G. Motivational Interviewing in Childhood Obesity Treatment. Front. Psychol. 2015, 6. [Google Scholar] [CrossRef] [Green Version]
- Karnik, S.; Kanekar, A. Childhood Obesity: A Global Public Health Crisis. Int. J. Prev. Med. 2012, 3, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pietrabissa, G.; Rossi, A.; Borrello, M.; Manzoni, G.M.; Mannarini, S.; Castelnuovo, G.; Molinari, E. Development and Validation of a Self-Determination Theory-Based Measure of Motivation to Exercise and Diet in Children. Front. Psychol. 2020, 11, 1299. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®); American Psychiatric Pub: Washington, DC, USA, 2013; ISBN 0-89042-557-4. [Google Scholar]
- Hayes, J.F.; Fitzsimmons-Craft, E.E.; Karam, A.M.; Jakubiak, J.; Brown, M.L.; Wilfley, D.E. Disordered Eating Attitudes and Behaviors in Youth with Overweight and Obesity: Implications for Treatment. Curr. Obes. Rep. 2018, 7, 235–246. [Google Scholar] [CrossRef] [PubMed]
- Nicholls, D.; Viner, R. Eating Disorders and Weight Problems. BMJ 2005, 330, 950–953. [Google Scholar] [CrossRef] [Green Version]
- Aimé, A.; Fuller-Tyszkiewicz, M.; Dion, J.; Markey, C.H.; Strodl, E.; McCabe, M.; Mellor, D.; Gallegos, A.G.; Pietrabissa, G.; Alcaraz-Ibánez, M. Assessing Positive Body Image, Body Satisfaction, Weight Bias, and Appearance Comparison in Emerging Adults: A Cross-Validation Study across Eight Countries. Body Image 2020, 35, 320–332. [Google Scholar] [CrossRef]
- McCabe, M.; Tatangelo, G.; Watson, B.; Fuller-Tyszkiewicz, M.; Rodgers, R.F.; Aimé, A.; Mellor, D.; Granero-Gallegos, A.; Strodl, E.; Caltabiano, M.; et al. Development and Testing of a Model for Risk and Protective Factors for Eating Disorders and Higher Weight among Emerging Adults: A Study Protocol. Body Image 2019, 31, 139–149. [Google Scholar] [CrossRef]
- Strodl, E.; Markey, C.; Aimé, A.; Rodgers, R.F.; Dion, J.; Coco, G.L.; Gullo, S.; McCabe, M.; Mellor, D.; Granero-Gallegos, A.; et al. A Cross-Country Examination of Emotional Eating, Restrained Eating and Intuitive Eating: Measurement Invariance across Eight Countries. Body Image 2020, 35, 245–254. [Google Scholar] [CrossRef]
- Tylka, T.L.; Subich, L.M. Examining a Multidimensional Model of Eating Disorder Symptomatology among College Women. J. Couns. Psychol. 2004, 51, 314. [Google Scholar] [CrossRef] [Green Version]
- Danner, U.N.; Sternheim, L.; Evers, C. The Importance of Distinguishing between the Different Eating Disorders (Sub) Types When Assessing Emotion Regulation Strategies. Psychiatry Res. 2014, 215, 727–732. [Google Scholar] [CrossRef] [PubMed]
- Hayaki, J.; Friedman, M.A.; Brownell, K.D. Emotional Expression and Body Dissatisfaction. Int. J. Eat. Disord. 2002, 31, 57–62. [Google Scholar] [CrossRef] [PubMed]
- O’Dea, J.A.; Abraham, S. Improving the Body Image, Eating Attitudes, and Behaviors of Young Male and Female Adolescents: A New Educational Approach That Focuses on Self-esteem. Int. J. Eat. Disord. 2000, 28, 43–57. [Google Scholar] [CrossRef]
- Sarrionandia, A.; Mikolajczak, M. A Meta-Analysis of the Possible Behavioural and Biological Variables Linking Trait Emotional Intelligence to Health. Health Psychol. Rev. 2020, 14, 220–244. [Google Scholar] [CrossRef]
- Barchard, K.A.; Brackett, M.A.; Mestre, J.M. Taking Stock and Moving Forward: 25 Years of Emotional Intelligence Research. Emot. Rev. 2016, 8, 289. [Google Scholar] [CrossRef]
- Goldenberg, I.; Matheson, K.; Mantler, J. The Assessment of Emotional Intelligence: A Comparison of Performance-Based and Self-Report Methodologies. J. Pers. Assess. 2006, 86, 33–45. [Google Scholar] [CrossRef] [PubMed]
- Petrides, K.V. Ability and trait emotional intelligence. In The Wiley-Blackwell Handbooks of Personality and Individual Differences; Wiley Blackwell: Hoboken, NJ, USA, 2011; pp. 656–678. [Google Scholar]
- Siegling, A.B.; Saklofske, D.H.; Petrides, K. Measures of ability and trait emotional intelligence. In Measures of Personality and Social Psychological Constructs; Elsevier: Amsterdam, The Netherlands, 2015; pp. 381–414. [Google Scholar]
- Mestre, J.M.; MacCann, C.; Guil, R.; Roberts, R.D. Models of Cognitive Ability and Emotion Can Better Inform Contemporary Emotional Intelligence Frameworks. Emot. Rev. 2016, 8, 322–330. [Google Scholar] [CrossRef]
- Foye, U.; Hazlett, D.E.; Irving, P. Exploring the Role of Emotional Intelligence on Disorder Eating Psychopathology. Eat. Weight Disord. Stud. Anorex. Bulim. Obes. 2019, 24, 299–306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mayer, J.D.; Caruso, D.R.; Salovey, P. The Ability Model of Emotional Intelligence: Principles and Updates. Emot. Rev. 2016, 8, 290–300. [Google Scholar] [CrossRef]
- Petrides, K.V.; Mikolajczak, M.; Mavroveli, S.; Sanchez-Ruiz, M.-J.; Furnham, A.; Pérez-González, J.-C. Developments in Trait Emotional Intelligence Research. Emot. Rev. 2016, 8, 335–341. [Google Scholar] [CrossRef]
- Costarelli, V.; Demerzi, M.; Stamou, D. Disordered Eating Attitudes in Relation to Body Image and Emotional Intelligence in Young Women. J. Hum. Nutr. Diet. 2009, 22, 239–245. [Google Scholar] [CrossRef]
- Gardner, K.J.; Quinton, S.; Qualter, P. The Role of Trait and Ability Emotional Intelligence in Bulimic Symptoms. Eat. Behav. 2014, 15, 237–240. [Google Scholar] [CrossRef] [PubMed]
- Swami, V.; Begum, S.; Petrides, K. Associations between Trait Emotional Intelligence, Actual–Ideal Weight Discrepancy, and Positive Body Image. Pers. Individ. Differ. 2010, 49, 485–489. [Google Scholar] [CrossRef]
- Zysberg, L.; Rubanov, A. Emotional Intelligence and Emotional Eating Patterns: A New Insight into the Antecedents of Eating Disorders? J. Nutr. Educ. Behav. 2010, 42, 345–348. [Google Scholar] [CrossRef]
- Zysberg, L.; Tell, E. Emotional Intelligence, Perceived Control, and Eating Disorders. SAGE Open 2013, 3, 2158244013500285. [Google Scholar] [CrossRef] [Green Version]
- Mikolajczak, M.; Van Bellegem, S. Increasing Emotional Intelligence to Decrease Healthcare Expenditures: How Profitable Would It Be? Pers. Individ. Differ. 2017, 116, 343–347. [Google Scholar] [CrossRef]
- Yau, Y.H.C.; Potenza, M.N. Stress and Eating Behaviors. Minerva Endocrinol. 2013, 38, 255–267. [Google Scholar] [PubMed]
- Higgins, J.P.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Hoboken, NJ, USA, 2019; ISBN 1-119-53661-8. [Google Scholar]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A Web and Mobile App for Systematic Reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, S.H.; Augustin, C.; Bethel, A.; Gill, D.; Anzaroot, S.; Brun, J.; DeWilde, B.; Minnich, R.C.; Garside, R.; Masuda, Y.J.; et al. Using Machine Learning to Advance Synthesis and Use of Conservation and Environmental Evidence: Letter. Conserv. Biol. 2018, 32, 762–764. [Google Scholar] [CrossRef] [Green Version]
- Downes, M.J.; Brennan, M.L.; Williams, H.C.; Dean, R.S. Development of a Critical Appraisal Tool to Assess the Quality of Cross-Sectional Studies (AXIS). BMJ Open 2016, 6, e011458. [Google Scholar] [CrossRef] [Green Version]
- Amado Alonso, D.; León-del-Barco, B.; Mendo-Lázaro, S.; Iglesias Gallego, D. Examining Body Satisfaction and Emotional–Social Intelligence among School Children: Educational Implications. Int. J. Environ. Res. Public Health 2020, 17, 2120. [Google Scholar] [CrossRef] [Green Version]
- Markey, M.A.; Vander Wal, J.S. The Role of Emotional Intelligence and Negative Affect in Bulimic Symptomatology. Compr. Psychiatry 2007, 48, 458–464. [Google Scholar] [CrossRef]
- Peres, V.; Corcos, M.; Robin, M.; Pham-Scottez, A. Emotional Intelligence, Empathy and Alexithymia in Anorexia Nervosa during Adolescence. Eat. Weight Disord. Stud. Anorex. Bulim. Obes. 2018, 25, 1–8. [Google Scholar] [CrossRef]
- Wong, Y.; Lin, J.-S.; Chang, Y.-J. Body Satisfaction, Emotional Intelligence, and the Development of Disturbed Eating: A Survey of Taiwanese Students. Asia Pac. J. Clin. Nutr. 2014, 23, 651. [Google Scholar]
- Pollatos, O.; Georgiou, E.; Kobel, S.; Schreiber, A.; Dreyhaupt, J. Trait-Based Emotional Intelligence, Body Image Dissatisfaction, and HRQoL in Children. Front. Psychiatry 2020, 10, 7. [Google Scholar] [CrossRef]
- Li, Y. Social Anxiety and Eating Disorder Risk Among Chinese Adolescents: The Role of Emotional Intelligence. School Ment. Health 2018, 10, 264–274. [Google Scholar] [CrossRef]
- Li, Y. Linking Body Esteem to Eating Disorders among Adolescents: A Moderated Mediation Model. J. Health Psychol. 2019, 25, 1755–1770. [Google Scholar] [CrossRef]
- Alicia Zavala, M.; Lopez, I. Adolescents at Risks: What Is the Role of Emotional Intelligence? Behav. Psychol. Psicol. Conduct. 2012, 20, 59–75. [Google Scholar]
- Cuesta-Zamora, C.; González-Martí, I.; García-López, L.M. The Role of Trait Emotional Intelligence in Body Dissatisfaction and Eating Disorder Symptoms in Preadolescents and Adolescents. Pers. Individ. Differ. 2018, 126, 1–6. [Google Scholar] [CrossRef]
- Maxwell, S.E.; Cole, D.A.; Mitchell, M.A. Bias in Cross-Sectional Analyses of Longitudinal Mediation: Partial and Complete Mediation Under an Autoregressive Model. Multivar. Behav. Res. 2011, 46, 816–841. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Resurrección, D.; Salguero, J.; Ruiz-Aranda, D. Emotional Intelligence and Psychological Maladjustment in Adolescence: A Systematic Review. J. Adolesc. 2014, 37, 461–472. [Google Scholar] [CrossRef]
- Romero-Mesa, J.; Pelaez-Fernandez, M.A.; Extremera, N. Emotional Intelligence and Eating Disorders: A Systematic Review. Eat. Weight Disord. 2020, 7, 1–15. [Google Scholar] [CrossRef]
- Foye, U.; Hazlett, D.E.; Irving, P. ‘The Body Is a Battleground for Unwanted and Unexpressed Emotions’: Exploring Eating Disorders and the Role of Emotional Intelligence. Eat. Disord. 2019, 27, 321–342. [Google Scholar] [CrossRef] [PubMed]
- Hambrook, D.; Oldershaw, A.; Rimes, K.; Schmidt, U.; Tchanturia, K.; Treasure, J.; Richards, S.; Chalder, T. Emotional Expression, Self-silencing, and Distress Tolerance in Anorexia Nervosa and Chronic Fatigue Syndrome. Br. J. Clin. Psychol. 2011, 50, 310–325. [Google Scholar] [CrossRef] [Green Version]
- Kun, B.; Demetrovics, Z. Emotional Intelligence and Addictions: A Systematic Review. Subst. Use Misuse 2010, 45, 1131–1160. [Google Scholar] [CrossRef]
- Martins, A.; Ramalho, N.; Morin, E. A Comprehensive Meta-Analysis of the Relationship between Emotional Intelligence and Health. Pers. Individ. Differ. 2010, 49, 554–564. [Google Scholar] [CrossRef]
- Schutte, N.S.; Malouff, J.M.; Thorsteinsson, E.B.; Bhullar, N.; Rooke, S.E. A Meta-Analytic Investigation of the Relationship between Emotional Intelligence and Health. Pers. Individ. Differ. 2007, 42, 921–933. [Google Scholar] [CrossRef]
- Stice, E. Risk and Maintenance Factors for Eating Pathology: A Meta-Analytic Review. Psychol. Bull. 2002, 128, 825. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodgers, R.F.; Fuller-Tyszkiewicz, M.; Markey, C.; Granero-Gallegos, A.; Sicilia, A.; Caltabiano, M.; Blackburns, M.-E.; Hayami-Chisuwa, N.; Strodl, E.; Aimé, A.; et al. Psychometric Properties of Measures of Sociocultural Influence and Internalization of Appearance Ideals across Eight Countries. Body Image 2020, 35, 300–315. [Google Scholar] [CrossRef]
- Oldershaw, A.; DeJong, H.; Hambrook, D.; Broadbent, H.; Tchanturia, K.; Treasure, J.; Schmidt, U. Emotional Processing Following Recovery from Anorexia Nervosa. Eur. Eat. Disord. Rev. 2012, 20, 502–509. [Google Scholar] [CrossRef] [PubMed]
- Treasure, J.; Corfield, F.; Cardi, V. A Three-Phase Model of the Social Emotional Functioning in Eating Disorders. Eur. Eat. Disord. Rev. 2012, 20, 431–438. [Google Scholar] [CrossRef]
- Harrison, A.; Sullivan, S.; Tchanturia, K.; Treasure, J. Emotion Recognition and Regulation in Anorexia Nervosa. Clin. Psychol. Psychother. 2009, 16, 348–356. [Google Scholar] [CrossRef]
- Kucharska-Pietura, K.; Nikolaou, V.; Masiak, M.; Treasure, J. The Recognition of Emotion in the Faces and Voice of Anorexia Nervosa. Int. J. Eat. Disord. 2004, 35, 42–47. [Google Scholar] [CrossRef] [PubMed]
- Zonnevylle-Bender, M.J.; Van Goozen, S.H.; Cohen-Kettenis, P.T.; Van Elburg, A.; De Wildt, M.; Stevelmans, E.; Van Engeland, H. Emotional Functioning in Anorexia Nervosa Patients: Adolescents Compared to Adults. Depress. Anxiety 2004, 19, 35–42. [Google Scholar] [CrossRef]
- Pollatos, O.; Herbert, B.M.; Schandry, R.; Gramann, K. Impaired Central Processing of Emotional Faces in Anorexia Nervosa. Psychosom. Med. 2008, 70, 701–708. [Google Scholar] [CrossRef] [Green Version]
- Hambrook, D.; Brown, G.; Tchanturia, K. Emotional Intelligence in Anorexia Nervosa: Is Anxiety a Missing Piece of the Puzzle? Psychiatry Res. 2012, 200, 12–19. [Google Scholar] [CrossRef]
- Tchanturia, K.; Davies, H.; Roberts, M.; Harrison, A.; Nakazato, M.; Schmidt, U.; Treasure, J.; Morris, R. Poor Cognitive Flexibility in Eating Disorders: Examining the Evidence Using the Wisconsin Card Sorting Task. PLoS ONE 2012, 7, e28331. [Google Scholar] [CrossRef] [PubMed]
- Gramaglia, C.; Ressico, F.; Gambaro, E.; Palazzolo, A.; Mazzarino, M.; Bert, F.; Siliquini, R.; Zeppegno, P. Alexithymia, Empathy, Emotion Identification and Social Inference in Anorexia Nervosa: A Case-Control Study. Eat. Behav. 2016, 22, 46–50. [Google Scholar] [CrossRef]
- Wildes, J.E.; Ringham, R.M.; Marcus, M.D. Emotion Avoidance in Patients with Anorexia Nervosa: Initial Test of a Functional Model. Int. J. Eat. Disord. 2010, 43, 398–404. [Google Scholar] [CrossRef] [Green Version]
- Pietrabissa, G.; Gullo, S.; Aimé, A.; Mellor, D.; McCabe, M.; Alcaraz-Ibánez, M.; Begin, C.; Blackburn, M.-E.; Caltabiano, M.; Sicilia, A. Measuring Perfectionism, Impulsivity, Self-Esteem and Social Anxiety: Cross-National Study in Emerging Adults from Eight Countries. Body Image 2020, 35, 265–278. [Google Scholar] [CrossRef] [PubMed]
- Lupyan, G. Linguistically Modulated Perception and Cognition: The Label-Feedback Hypothesis. Front. Psychol. 2012, 3, 54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Voelker, D.K.; Reel, J.J.; Greenleaf, C. Weight Status and Body Image Perceptions in Adolescents: Current Perspectives. Adolesc. Health Med. Ther. 2015, 6, 149. [Google Scholar] [CrossRef] [Green Version]
- Mussell, M.P.; Mitchell, J.E.; Weller, C.L.; Raymond, N.C.; Crow, S.J.; Crosby, R.D. Onset of Binge Eating, Dieting, Obesity, and Mood Disorders among Subjects Seeking Treatment for Binge Eating Disorder. Int. J. Eat. Disord. 1995, 17, 395–401. [Google Scholar] [CrossRef]
- Pietrabissa, G.; Castelnuovo, G.; Jackson, J.B.; Rossi, A.; Manzoni, G.M.; Gibson, P. Brief Strategic Therapy for Bulimia Nervosa and Binge Eating Disorder: A Clinical and Research Protocol. Front. Psychol. 2019, 10, 373. [Google Scholar] [CrossRef]
- Jackson, J.B.; Pietrabissa, G.; Rossi, A.; Manzoni, G.M.; Castelnuovo, G. Brief Strategic Therapy and Cognitive Behavioral Therapy for Women with Binge Eating Disorder and Comorbid Obesity: A Randomized Clinical Trial One-Year Follow-Up. J. Consult. Clin. Psychol. 2018, 86, 688. [Google Scholar] [CrossRef]
- Grilo, C.; Masheb, R. Onset of Dieting vs Binge Eating in Outpatients with Binge Eating Disorder. Int. J. Obes. 2000, 24, 404–409. [Google Scholar] [CrossRef] [Green Version]
- Marcus, M.D.; Kalarchian, M.A. Binge Eating in Children and Adolescents. Int. J. Eat. Disord. 2003, 34, S47–S57. [Google Scholar] [CrossRef] [PubMed]
- Haiman, C.; Devlin, M.J. Binge Eating before the Onset of Dieting: A Distinct Subgroup of Bulimia Nervosa? Int. J. Eat. Disord. 1999, 25, 151–157. [Google Scholar] [CrossRef]
- Bulik, C.M.; Sullivan, P.F.; Carter, F.A.; Joyce, P.R. Initial Manifestations of Disordered Eating Behavior: Dieting versus Binging. Int. J. Eat. Disord. 1997, 22, 195–201. [Google Scholar] [CrossRef]
- Johnson, J.G.; Cohen, P.; Kotler, L.; Kasen, S.; Brook, J.S. Psychiatric Disorders Associated with Risk for the Development of Eating Disorders during Adolescence and Early Ad ulthood. J. Consult. Clin. Psychol. 2002, 70, 1119. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Orientation Programme on Adolescent Health for Health Care Providers; WHO: Geneva, Switzerland, 2006. [Google Scholar]
- Grogan, S. Body Image: Understanding Body Dissatisfaction in Men, Women and Children; Taylor & Francis: Milton Park, UK, 2016; ISBN 1-317-40043-7. [Google Scholar]
- Pantelis, D. The Role of Emotions in Eating Behavior and Impact on Obesity and Weight Management. Adv. Obes. Weight Manag. Control 2018, 8, 175–176. [Google Scholar] [CrossRef] [Green Version]
- Casagrande, M.; Boncompagni, I.; Forte, G.; Guarino, A.; Favieri, F. Emotion and Overeating Behavior: Effects of Alexithymia and Emotional Regulation on Overweight and Obesity. Eat. Weight Disord. Stud. Anorex. Bulim. Obes. 2020, 25, 1333–1345. [Google Scholar] [CrossRef] [PubMed]
- Harrison, A.; Sullivan, S.; Tchanturia, K.; Treasure, J. Emotional Functioning in Eating Disorders: Attentional Bias, Emotion Recognition and Emotion Regulation. Psychol. Med. 2010, 40, 1887. [Google Scholar] [CrossRef] [PubMed]
- Liverpool, S.; Mota, C.P.; Sales, C.M.; Čuš, A.; Carletto, S.; Hancheva, C.; Sousa, S.; Cerón, S.C.; Moreno-Peral, P.; Pietrabissa, G. Engaging Children and Young People in Digital Mental Health Interventions: Systematic Review of Modes of Delivery, Facilitators, and Barriers. J. Med. Internet Res. 2020, 22, e16317. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Author, Year | Country | EI Measure | Study Aim | Primary Outcome | Outcome Measure | Population | Sample Size | Female % | Mean Age (SD) | Age Range | Mean BMI (SD) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Amado Alonso, 2020 [34] | ES | EQI-YV | To explore how body image satisfaction and gender act as modulators of EI | Body image satisfaction | Stunkard Figure Rating Scale | Preadolescents (non-clinical) | 944 | 42 | 10.76 (1.11) | 9–12 | N/A |
| Cuesta-Zamora, 2018 [42] | ES | TEIQue-ASF | To explore the relationship between EI and ED symptoms | Body dissatisfaction, bulimic symptoms, drive for thinness | EDI-3 subscales: DT-EDI-3, B-EDI-3, BD-EDI-3 | Preadolescents (sample 1) and adolescents (sample 2) (non-clinical) | 762 | Sample 1: 51.8; Sample 2: 47 | Sample 1: 10.55 (0.60); Sample 2: 13.53 (1.25) | Sample 1: 10–12; Sample 2: 12–17 | Female: 19.2 (3.9); Male: 19.1 (3.6) |
| Li, 2018 [39] | CN | WLEIS | To explore the relationship between EI, social anxiety and ED risk | ED risk | EAT-26 | Adolescents (non-clinical) | 784 | 51.3 | 17.12 (1.32) | 15–20 | 21.47 (2.39) |
| Li, 2019 [40] | CN | WLEIS | To explore the role of EI in moderating (1) the relationship between body esteem and ED and (2) the mediating effect of social appearance anxiety between body esteem and ED | ED risk | EAT-26 | Adolescents (non-clinical) | 2509 | 54.1 | 16.12 (1.45) | 15–20 | N/A |
| Markey, 2007 [35] | US | EQI-YV-SF | To explore the role of EI, alexithymia and coping strategies in moderating the relationship between a negative affect and ED symptoms | Bulimic symptoms | Bulimia test, revised | Adolescents (non-clinical) | 154 | 100 | 18.66 | 17–23 | 23.2 |
| Peres, 2017 [36] | FR | EQI-YV | To explore the differences in EI, empathy and alexithymia between adolescents with AN and healthy controls | AN | DSM-IV Mini-International Neuropsychiatric Interview | Adolescents (clinical vs. non-clinical) | 79 | 100 | AN: 16.2 (1.44); HC: 16.4 (1.73) | AN: 13.1–18.9; HC: 13.1–18.8 | N/A |
| Pollatos, 2020 [38] | DE | EQI-YV-SF | To explore the relationship between EI and body image | Body image perception | Body Silhouette Chart | Preadolescents (non-clinical) | 991 | 49.7 | 9.58 (0.62) | 8–11 | * 17.34 (2.6) |
| Wong, 2014 [37] | TW | AEIS | To explore the relationship between EI and ED risk | ED risk | EAT-26 | Adolescents (non-clinical) | 1028 | 24.4 | 16.1 (0.7) | 14–18 | N/A |
| Zavala, 2018 [41] | MX | EQI-YV | To explore the relationship between EI and ED symptoms | ED symptoms | Millon Adolescent Clinical Inventory (MACI), eating disorders subscale | Adolescents (non-clinical) | 829 | 52.5 | 13.6 (0.64) | 13–15 | N/A |
| Author, Year | Study Design | Selection | Measurement | Reporting | Confounding | Results |
|---|---|---|---|---|---|---|
| Amado Alonso, 2020 [34] | + | + | + | + | + | Body image satisfaction significantly correlates with interpersonal, stress management, adaptability, and mood components, but not with the intrapersonal component, of EI. The association between the stress management component of EI and body image satisfaction is significant only for boys. |
| Cuesta-Zamora, 2018 [42] | + | − | + | + | + | EI significantly and negatively correlates with ED scores in both samples. |
| Li, 2018 [39] | − | + | + | + | + | EI negatively correlates with social anxiety, which results in partially mediating the relationship between EI and ED risk. |
| Li, 2019 [40] | − | + | + | + | + | Social appearance anxiety partially mediates the relationship between body esteem and ED risk, whilst EI moderates the effects of body esteem on social appearance anxiety and ED. |
| Markey, 2007 [35] | − | − | + | + | + | EI significantly predicts bulimic symptoms. EI, alexithymia and coping strategies do not moderate the relationship between a negative affect and bulimic symptoms. |
| Peres, 2017 [36] | + | − | + | + | + | Samples (clinical vs. non-clinical) significantly differ for intrapersonal and general mood components of EI, while no differences in interpersonal, adaptability and stress management components of EI are found between groups. After controlling for anxiety and depression, no significant correlation is found between AN symptoms and the intrapersonal component of EI, whereas the relationship between the mood component of EI and AN remains significant. |
| Pollatos, 2020 [38] | + | + | + | + | + | Significant inverse associations are found in both the male and female subsamples between body image dissatisfaction and EI after controlling for the BMI. |
| Wong, 2014 [37] | + | + | + | + | − | ED symptoms positively correlate with emotional perception, emotional expression, and emotional application components, but not with the emotion regulation component, of EI. |
| Zavala, 2018 [41] | + | + | + | + | + | The intrapersonal, stress management and adaptability components of EI have a weak but significant inverse correlation with ED symptoms. In a multivariable model controlling for sex, only the stress management component of EI remained associated with ED risk. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Giusti, E.M.; Manna, C.; Scolari, A.; Mestre, J.M.; Prevendar, T.; Castelnuovo, G.; Pietrabissa, G. The Relationship between Emotional Intelligence, Obesity and Eating Disorder in Children and Adolescents: A Systematic Mapping Review. Int. J. Environ. Res. Public Health 2021, 18, 2054. https://doi.org/10.3390/ijerph18042054
Giusti EM, Manna C, Scolari A, Mestre JM, Prevendar T, Castelnuovo G, Pietrabissa G. The Relationship between Emotional Intelligence, Obesity and Eating Disorder in Children and Adolescents: A Systematic Mapping Review. International Journal of Environmental Research and Public Health. 2021; 18(4):2054. https://doi.org/10.3390/ijerph18042054
Chicago/Turabian StyleGiusti, Emanuele Maria, Chiara Manna, Anna Scolari, José M. Mestre, Tamara Prevendar, Gianluca Castelnuovo, and Giada Pietrabissa. 2021. "The Relationship between Emotional Intelligence, Obesity and Eating Disorder in Children and Adolescents: A Systematic Mapping Review" International Journal of Environmental Research and Public Health 18, no. 4: 2054. https://doi.org/10.3390/ijerph18042054