
The Effect of Chair-Based Exercise on Physical Function in Older Adults: A Systematic Review and Meta-Analysis

 ,
,  , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Quality Assessment
2.2. Data Synthesis
3. Results
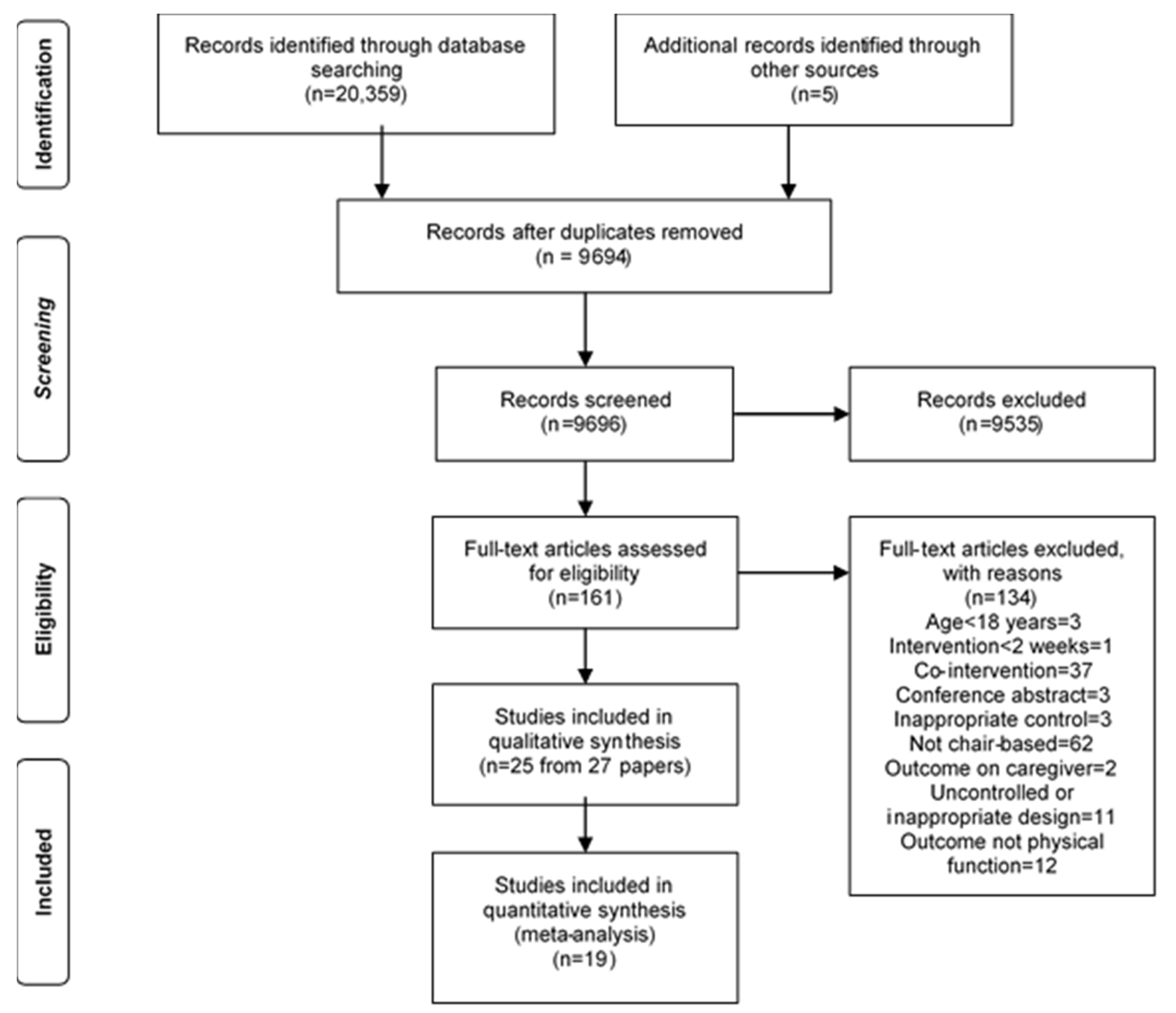
3.1. Search Results
3.2. Characteristics of Included Studies
3.3. Intervention Characteristics
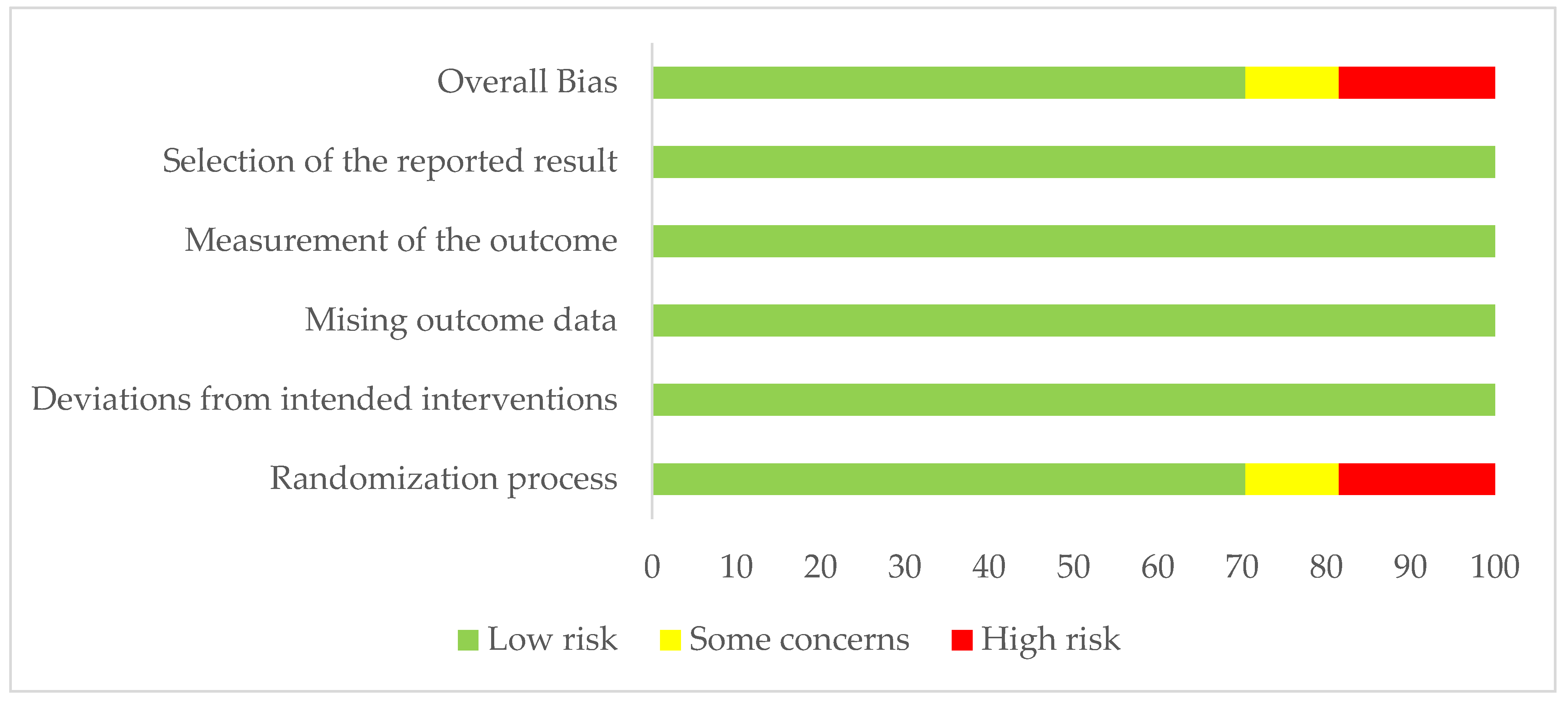
3.4. Risk of Bias
3.5. Effects on Physical Function
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cunningham, C.; O’Sullivan, R.; Caserotti, P.; Tully, M.A. Consequences of physical inactivity in older adults: A systematic review of reviews and meta-analyses. Scand. J. Med. Sci. Sports 2020, 30, 816–827. [Google Scholar] [CrossRef] [PubMed]
- Bangsbo, J.; Blackwell, J.; Boraxbekk, C.J.; Caserotti, P.; Dela, F.; Evans, A.B.; Jespersen, A.P.; Gliemann, L.; Kramer, A.F.; Lundbye-Jensen, J.; et al. Copenhagen Consensus statement 2019: Physical activity and ageing. Br. J. Sports Med. 2019, 53, 856–858. [Google Scholar] [CrossRef] [Green Version]
- Sexton, B.P.; Taylor, N.F. To sit or not to sit? A systematic review and meta-analysis of seated exercise for older adults. Australas. J. Ageing 2018, 38, 15–27. [Google Scholar] [CrossRef] [Green Version]
- Ikai, S.; Uchida, H.; Mizuno, Y.; Tani, H.; Nagaoka, M.; Tsunoda, K.; Mimura, M.; Suzuki, T. Effects of chair yoga therapy on physical fitness in patients with psychiatric disorders: A 12-week single-blind randomized controlled trial. J. Psychiatr. Res. 2017, 94, 194–201. [Google Scholar] [CrossRef]
- Stubbs, B.; Brefka, S.; Denkinger, M.D. What works to prevent falls in community-dwelling older Adults? Umbrella review of meta-analyses of randomized controlled trials. Phys. Ther. 2015, 95, 1095–1110. [Google Scholar] [CrossRef] [Green Version]
- Walston, J.D. Sarcopenia in older adults. Curr. Opin. Rheumatol. 2014, 24, 623–627. [Google Scholar] [CrossRef] [Green Version]
- Kortebein, P.; Ferrando, A.; Lombeida, J.; Wolfe, R.; Evans, W.J. Effect of 10 days of bed rest on skeletal muscle in healthy older adults. JAMA 2007, 297, 1772–1774. [Google Scholar] [CrossRef]
- Hvid, L.; Aagaard, P.; Justesen, L.; Bayer, M.L.; Andersen, J.L.; Ørtenblad, N.; Kjaer, M.; Suetta, C. Effects of aging on muscle mechanical function and muscle fiber morphology during short-term immobilization and subsequent retraining. J. Appl. Physiol. 2010, 109, 1628–1634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suetta, C.; Hvid, L.G.; Justesen, L.; Christensen, U.; Neergaard, K.; Simonsen, L.; Ortenblad, N.; Magnusson, S.P.; Kjaer, M.; Aagaard, P. Effects of aging on human skeletal muscle after immobilization and retraining. J. Appl. Physiol. 2009, 107, 1172–1180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Public Health England. Active at Home. Available online: https://campaignresources.phe.gov.uk/resources/campaigns/50-resource-ordering/resources/5118 (accessed on 15 February 2021).
- Robinson, K.R.; Leighton, P.; Logan, P.; Gordon, A.L.; Anthony, K.; Harwood, R.H.; Gladman, J.R.; Masud, T. Developing the principles of chair based exercise for older people: A modified Delphi study. BMC Geriatr. 2014, 14, 65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yao, C.-T.; Tseng, C.-H. Effectiveness of Chair Yoga for Improving the Functional Fitness and Well-being of Female Community-Dwelling Older Adults with Low Physical Activities. Top. Geriatr. Rehabilit. 2019, 35, 248–254. [Google Scholar] [CrossRef]
- Noradechanunt, C.; Worsley, A.; Groeller, H. Thai Yoga improves physical function and well-being in older adults: A randomised controlled trial. J. Sci. Med. Sport 2017, 20, 494–501. [Google Scholar] [CrossRef] [PubMed]
- Sallis, J.F.; Adlakha, D.; Oyeyemi, A.; Salvo, D. An international physical activity and public health research agenda to inform coronavirus disease-2019 policies and practices. J. Sport Health Sci. 2020, 9, 328–334. [Google Scholar] [CrossRef]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Hoffmann, T.C.; Glasziou, P.P.; Boutron, I.; Milne, R.; Perera, R.; Moher, D.; Altman, D.G.; Barbour, V.; Macdonald, H.; Johnston, M.; et al. Better reporting of interventions: Template for intervention description and replication (TIDieR) checklist and guide. BMJ 2014, 348, g1687. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baum, E.E.; Jarjoura, D.; Polen, A.E.; Faur, D.; Rutecki, G. Effectiveness of a group exercise program in a long-term care facility: A randomized pilot trial. J. Am. Med. Dir. Assoc. 2003, 4, 74–80. [Google Scholar] [CrossRef]
- Daniel, K. Wii-hab for pre-frail older adults. Rehabilit. Nurs. 2012, 37, 195–201. [Google Scholar] [CrossRef]
- Dean, C.M.; Channon, E.F.; Hall, J.M. Sitting training early after stroke improves sitting ability and quality and carries over to standing up but not to walking: A randomised trial. Aust. J. Physiother. 2007, 53, 97–102. [Google Scholar] [CrossRef]
- Furtado, G.E.; Uba-Chupel, M.; Carvalho, H.M.; Souza, N.R.; Ferreira, J.P.; Teixeira, A.M. Effects of a chair-yoga exercises on stress hormone levels, daily life activities, falls and physical fitness in institutionalized older adults. Complement. Ther. Clin. Pract. 2016, 24, 123–129. [Google Scholar] [CrossRef]
- Furtado, G.E.; Carvalho, H.M.; Loureiro, M.; Patrício, M.; Uba-Chupel, M.; Colado, J.C.; Hogervorst, E.; Ferreira, J.P.; Teixeira, A.M. Chair-based exercise programs in institutionalized older women: Salivary steroid hormones, disabilities and frailty changes. Exp. Gerontol. 2020, 130, 110790. [Google Scholar] [CrossRef]
- Kertapati, Y.; Sahar, J.; Nursasi, A.Y. The effects of chair yoga with spiritual intervention on the functional status of older adults. Enferm. Clin. 2018, 28 (Suppl. 1), 70–73. [Google Scholar] [CrossRef]
- Kim, S.G.; Goo, M.; Park, J.H. Comparison of the effectiveness of balance training using a reaching task between a sitting position and a standing position in the elderly. J. Phys. Ther. Sci. 2015, 27, 2337–2339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kujawski, S.; Kujawska, A.; Gajos, M.; Klawe, J.J.; Tafil-Klawe, M.; Mądra-Gackowska, K.; Stankiewicz, B.; Newton, J.L.; Kędziora-Kornatowska, K.; Zalewski, P. Effects of 3-months sitting callisthenic balance and resistance exercise on aerobic capacity, aortic stiffness and body composition in healthy older participants. Randomized Controlled Trial. Exp. Gerontol. 2018, 108, 125–130. [Google Scholar] [CrossRef] [PubMed]
- Latham, N.K.; Anderson, C.S.; Lee, A.; Bennett, D.A.; Moseley, A.; Cameron, I.D.; Fitness Collaborative Group. A randomized, controlled trial of quadriceps resistance exercise and vitamin D in frail older people: The Frailty Interventions Trial in Elderly Subjects (FITNESS). J. Am. Geriatr. Soc. 2003, 51, 291–299. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.Y.; Hui-Chan, C.W.; Tsang, W.W. The effects of practicing sitting Tai Chi on balance control and eye-hand coordination in the older adults: A randomized controlled trial. Disabil. Rehabilit. 2015, 37, 790–794. [Google Scholar] [CrossRef]
- McMurdo, M.E.; Rennie, L. A controlled trial of exercise by residents of old people’s homes. Age Ageing 1993, 22, 11–15. [Google Scholar] [CrossRef] [PubMed]
- McMurdo, M.E.; Rennie, L.M. Improvements in quadriceps strength with regular seated exercise in the institutionalized elderly. Arch. Phys. Med. Rehabilit. 1994, 75, 600–603. [Google Scholar]
- Netz, Y.; Axelrad, S.; Argov, E. Group physical activity for demented older adults feasibility and effectiveness. Clin. Rehabilit. 2007, 21, 977–986. [Google Scholar] [CrossRef]
- Nicholson, C.M.; Czernwicz, S.; Mandilas, G.; Rudolph, I.; Greyling, M.J. The role of chair exercises for older adults following hip fracture. South Afr. Med. J. 1997, 87, 1131–1138. [Google Scholar]
- Niemelä, K.; Väänänen, I.; Leinonen, R.; Laukkanen, P. Benefits of home-based rocking-chair exercise for physical performance in community-dwelling elderly women: A randomized controlled trial. Aging Clin. Exp. Res. 2011, 23, 279–287. [Google Scholar] [CrossRef]
- Park, J.; McCaffrey, R.; Newman, D.; Cheung, C.; Hagen, D. The effect of Sit ‘n’ Fit Chair Yoga among community-dwelling older adults with osteoarthritis. Holist. Nurs. Pract. 2014, 28, 247–257. [Google Scholar] [CrossRef]
- Park, J.; McCaffrey, R.; Newman, D.; Liehr, P.; Ouslander, J.G. A Pilot Randomized Controlled Trial of the Effects of Chair Yoga on Pain and Physical Function Among Community-Dwelling Older Adults with Lower Extremity Osteoarthritis. J. Am. Geriatr. Soc. 2017, 65, 592–597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, J.; Newman, D.; McCaffrey, R.; Garrido, J.J.; Riccio, M.L.; Liehr, P. The Effect of Chair Yoga on Biopsychosocial Changes in English- and Spanish-Speaking Community-Dwelling Older Adults with Lower-Extremity Osteoarthritis. J. Gerontol. Soc. Work 2016, 59, 604–626. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, J.; Gong, J.; Yim, J. Effects of a sitting boxing program on upper limb function, balance, gait, and quality of life in stroke patients. NeuroRehabilitation 2017, 40, 77–86. [Google Scholar] [CrossRef] [PubMed]
- Park, J.; Tolea, M.I.; Sherman, D.; Rosenfeld, A.; Arcay, V.; Lopes, Y.; Galvin, J.E. Feasibility of Conducting Nonpharmacological Interventions to Manage Dementia Symptoms in Community-Dwelling Older Adults: A Cluster Randomized Controlled Trial. Am. J. Alzheimers Dis. Other Dement. 2020, 35, 1533317519872635. [Google Scholar] [CrossRef] [PubMed]
- Rieping, T.; Furtado, G.E.; Letieri, R.V.; Chupel, M.U.; Colado, J.C.; Hogervorst, E.; Filaire, E.; Teixeira, A.M.M.B.; Ferreira, J.P. Effects of Different Chair-Based Exercises on Salivary Biomarkers and Functional Autonomy in Institutionalized Older Women. Res. Q. Exerc. Sport 2019, 90, 36–45. [Google Scholar] [CrossRef]
- Venturelli, M.; Lanza, M.; Muti, E.; Schena, F. Positive effects of physical training in activity of daily living-dependent older adults. Exp. Aging Res. 2010, 36, 190–205. [Google Scholar] [CrossRef]
- Vogler, C.M.; Sherrington, C.; Ogle, S.J.; Lord, S.R. Reducing risk of falling in older people discharged from hospital: A randomized controlled trial comparing seated exercises, weight-bearing exercises, and social visits. Arch. Phys. Med. Rehabilit. 2009, 90, 1317–1324. [Google Scholar] [CrossRef]
- Vogler, C.M.; Menant, J.C.; Sherrington, C.; Ogle, S.J.; Lord, S.R. Evidence of detraining after 12-week home-based exercise programs designed to reduce fall-risk factors in older people recently discharged from hospital. Arch. Phys. Med. Rehabilit. 2012, 93, 1685–1691. [Google Scholar] [CrossRef] [PubMed]
- Soysal, P.; Hurst, C.; Demurtas, J.; Firth, J.; Howden, R.; Yang, L.; Tully, M.A.; Koyanagi, A.; Ilie, P.C.; López-Sánchez, G.F.; et al. Handgrip strength and health outcomes: Umbrella review of systematic reviews with meta-analyses of observational studies. J. Sport Health Sci. 2020. online ahead of print. [Google Scholar] [CrossRef]
- Simpkin, A.J.; Cooper, R.; Howe, L.D.; Relton, C.L.; Davey Smith, G.; Teschendorff, A.; Widschwendter, M.; Wong, A.; Kuh, D.; Hardy, R. Are objective measures of physical capability related to accelerated epigenetic age? Findings from a British birth cohort. BMJ Open 2017, 7, e016708. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bobos, P.; Nazari, G.; Lu, Z.; MacDermid, J.C. Measurement Properties of the Hand Grip Strength Assessment: A Systematic Review with Meta-analysis. Arch. Phys. Med. Rehabilit. 2020, 101, 553–565. [Google Scholar] [CrossRef] [PubMed]
- Jones, C.J.; Rikli, R.E.; Beam, W.C. A 30-s chair-stand test as a measure of lower body strength in community-residing older adults. Res. Q. Exerc. Sport 1999, 70, 113–119. [Google Scholar] [CrossRef]
- McMullan, I.I.; Bunting, B.P.; McDonough, S.M.; Tully, M.A.; Casson, K. Changes in physical activity predict changes in a comprehensive model of balance in older community-dwelling adults. A longitudinal analysis of the TILDA study. J. Frailty Sarcopenia Falls 2019, 4, 102–110. [Google Scholar] [CrossRef]
- Cunningham, C.; O’Sullivan, R. Why physical activity matters for older adults in a time of pandemic. Eur. Rev. Aging Phys. Act. 2020, 17, 16. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Author (Year) | Sample Size | Country | Age Mean (SD) | Gender | Study Design | Control Group | Participants’ Characteristics | Physical Function Outcomes |
|---|---|---|---|---|---|---|---|---|
| Baum (2003) [19] | 20 | USA | 88 (NR) | NR | RCT | Art therapy | Frail elderly | Timed up and go, physical performance test, Berg balance |
| Daniel (2012) [20] | 15 | USA | 77 (5.3) | M = 39%, F = 61% | RCT | Non-intervention control | Pre-frail older adults | Chair stands, timed up and go, timed arm curls, sit and reach, step 2 test, 6-min walk test, senior fitness test, fear of falling, LLFDI-function |
| Dean (2017) [21] | 12 | Australia | 67 (11.9) | M = 64%, F = 36% | RCT | Seated cognitive-manipulative tasks | Stroke survivors | Sitting ability, sitting quality, 10-m walk test |
| Furtado (2016) [22] | 35 | Portugal | 83.81 (6.6) | M = 0%, F = 100% | CBA | Non-intervention control | Institutionalised older adults | Lawton Instrumental Activities of Daily Living, Tinetti Falls Efficacy Scale, senior fitness test, 30 s chair sit to stand, 30 s arm-curl test, chair sit-and-reach test, timed up and go |
| Furtado (2020) [23] | 40 | Portugal | 81.62 (7.91) | M = 0%, F = 100% | RCT | Non-intervention control | Institutionalised older women | Physical frailty, Falls Efficacy Scale, Katz Index of Independence in ADL |
| Ikai (2017) [4] | 56 | Japan | 55.3 (13.7) | M = 64%, F = 36% | RCT | Instructed to spend group time in activities of their choice (e.g., walking, reading or chatting) | Inpatients with chronic psychiatric disorders | Anteflexion in sitting, handgrip, modified falls efficacy scale, postural sway |
| Kertapati (2018) [24] | 84 | Indonesia | 66 (NR) | M = 19%, F = 81% | CBA | Non-intervention control | Older adults living in in Depok City, Indonesia | Functional Independence Measure |
| Kim (2015) [25] | 30 | Korea | 73.2 (3.1) | M = 0%, F = 100% | CBA | Standing balance training | Community-dwelling women aged ≥65 years | Short-form berg balance, 10-m walk test, timed up and go, falls efficacy scale |
| Kujasski (2018) [26] | 55 | Poland | 65 (NR) | M = 9%, F = 91% | RCT | Resistance exercise programme | Community-dwelling older adults aged ≥55 years | 6-min walk test |
| Latham (2003) [27] | 242 | New Zealand and Australia | 79.1 (6.9) | M = 47%, F = 53% | RCT | Offered general advice on problems encountered | Frail older adults after hospital discharge | ADL (Barthel index), modified falls efficacy scale, quadriceps strength, time taken to walk 4 m, timed up and go, berg balance |
| Lee (2015) [28] | 59 | Hong Kong | 85.8 (9.2) | M = 23.7%, F = 76.3% | RCT | Limb mobilization programme | Living in residential care facilities | Sequential weight shifting, forward reach, eye–hand coordination |
| McMurdo (1993) [29] | 41 | Scotland | 80.4 (6.5) | M = 89%, F = 11% | RCT | Reminiscence sessions without exercise | Older adults living in residential homes | Sway, handgrip strength, chair-to-stand, ADL (Barthel index) |
| McMurdo (1994) [30] | 65 | Scotland | 82.9 (6) | M = 83%, F = 17% | RCT | Reminiscence sessions without exercise | Older adults living in residential homes | Quadriceps strength, step test |
| Netz (2007) [31] | 26 | Israel | 76.9 (6.72) | M = 48%, F = 52% | RCT | Social activity including conversations, social games, viewing pictures and reading newspaper articles | Older adults with dementia | Timed up and go, sit to stand, functional reach |
| Nicholson (1997) [32] | 30 | South Africa | 79.8 (6.6) | M = 0%, F = 100% | CBA | Non-intervention control | Patients discharged from an orthopaedic ward 8–10 days after hip surgery | Handgrip strength, Falls Efficacy Scale |
| Niemela (2011) [33] | 51 | Finland | 80.2 (3.6) | M = 0%, F = 100% | RCT | Non-intervention control | War veterans, spouse, or widow of war veterans | Max walking speed, handgrip, chair rising, standing on one leg, Berg balance scale |
| Park (2014) [34] | 25 | USA | 79 (6.42) | M = 23.5%, F = 76.5% | RCT | Health Education programme | Osteoarthritis | Gait speed, 6-min walk test, Berg balance scale |
| Park (2016 and 2017a) [35,36] | 112 | USA | 75.3 (7.5) | M = 24.1%, F = 75.9% | RCT | Health Education programme | Lower Extremity Osteoarthritis | Gait speed, Berg balance scale |
| Park (2017b) [37] | 26 | Korea | NR | NR | RCT | Conventional physiotherapy | Stroke patients | Manual Function Test, handgrip strength, berg balance scale, postural sway, time taken to walk 10 m |
| Park (2019) [38] | 31 | USA | 84.3 (7.7) | M = 58.1%, F = 41.9% | Cluster RCT | Music therapy groups | Individuals living with dementia | Timed up and go, physical performance test, SPPB, handgrip |
| Rieping (2019) [39] | 32 | Portugal | 80 (8.04) | M = 0%, F = 100% | CBA | Non-intervention control | Institutionalised Older Women | 30-s arm-curl test, 30-s chair seat and stand test, 8ft up and go test, Falls Efficacy Scale, Lawton Scale of Instrumental ADL, Katz Index of Independence in ADL |
| Venturelli (2010) [40] | 30 | Italy | 84 (6) | M = 0%, F = 100% | RCT | Usual care | Frail women | Arm curl strength test, ADL (Barthel index), performance-oriented mobility assessment index |
| Vogler (2009) [41] | 120 | Australia | 80 (7) | M = 21%, F = 79% | RCT | Social visit by a research assistant at the same frequency as the exercise group | Inpatients in a care and rehabilitation facility | Physical Performance and Mobility Examination, maximal balance range tests |
| Vogler (2012) [42] | 120 | Australia | 80 (7) | M = 21%, F = 79% | RCT | Social visit by a research assistant at the same frequency as the exercise group | Older people recently discharged from hospital | Physiological Profile Assessment, maximal balance range tests |
| Yao (2019) [12] | 31 | Taiwan | 77.5 (6.2) | M = 0%, F = 100% | CBA | Maintained regular daily activities | Community dwelling older females | Handgrip strength, lower limb muscle strength, upper limb muscle strength, static balance, agility, dynamic balance, lower limb flexibility, upper limb flexibility |
| Author (Year) | Brief Description of Intervention | Who Delivered the Intervention | Mode of Delivery | Where Exercise Took Place | Length of Intervention (Weeks) | Total Number of Sessions | Frequency of Sessions (Per Week) | Duration of Sessions (mins) | How Adherence Was Assessed | Adherence |
|---|---|---|---|---|---|---|---|---|---|---|
| Baum (2003) [19] | Chair-based exercise with weights | Exercise physiologist | Group exercise | Long term care facility | 26 | 78 | 3 | 60 | NR | NR |
| Daniel (2012) [20] | Seated aerobic exercises | Certified fitness professional | Group exercise | Study site | 15 | 45 | 3 | 45 | Attendance at sessions | 86% |
| Dean (2017) [21] | Seated reaching tasks | NR | NR | Hospital rehabilitation facility | 2 | 10 | 5 | 30 | NR | NR |
| Furtado (2016) [22] | Chair yoga based on hatha yoga, focusing on flexibility | Expert technicians | NR | Social and health care support centres | 14 | 28 | 2 | NR | Attendance at sessions | NR |
| Furtado (2020) [23] | Chair exercises with TheraBand | Instructor | Group exercise | Gym | 28 | 84 | 3 | 45 | Attendance at sessions | 72% |
| Ikai (2017) [4] | Chair yoga | Yoga instructor and occupational health staff support | Group exercise | Hospital | 12 | 24 | 2 | 20 | NR | NR |
| Kertapati (2018) [24] | Chair yoga with spiritual intervention | Instructor | Group exercise | NR | 4 | 12 | 3 | 60 | NR | NR |
| Kim (2015) [25] | Seated stretching | NR | NR | NR | 8 | 24 | 3 | 20 | NR | NR |
| Kujasski (2018) [26] | Seated stretching and mobility exercises | NR | NR | University campus | 12 | 24 | 2 | 45–50 | Technician recorded attendance | 71% |
| Latham (2003) [27] | Quadriceps exercises using adjustable ankle cuff weights | Physical therapists | Group and individual exercise | Hospitals/home | 10 | 30 | 3 | NR | NR | NR |
| Lee (2015) [28] | Seated tai chi | Researchers who developed the exercise | Group exercise | Residential care facilities | 12 | 36 | 3 | 60 | NR | NR |
| McMurdo (1993) [29] | Upper and lower limb flexibility and strengthening exercises while seated | NR | Group exercise | Local authority residential homes | 28 | 56 | 2 | 45 | Attendance at sessions | 91% |
| McMurdo (1994) [30] | Isometric exercises to music designed to strengthen major muscle groups and improve joint flexibility and muscle tone | Physiotherapist | Group exercise | Local authority residential homes | 24 | 48 | 2 | 45 | Attendance at sessions | 72% |
| Netz (2007) [31] | Seated exercises to promote range of motion, strength and coordination of upper and lower limbs | Physical activity leader | Instructor-patient interaction | Day centre | 12 | 24 | 2 | 45 | NR | NR |
| Nicholson (1997) [32] | Seated exercise with simple objects to help patients’ full range of motion | Physiotherapist | Group exercise | Geriatric hospital | 72 | 24 | NR | 50 | NR | NR |
| Niemela (2011) [33] | Rocking chair exercises | Physiotherapist | Individual exercises at home | Rehab centre and home | 6 | 84 | 14 | 15 | Adherence rates obtained from diaries | 96% |
| Park (2014) [34] | The Sit ‘N’ Fit Chair Yoga programme | Yoga instructor | Instructor | Senior centre | 8 | 16 | 2 | 45 | NR | NR |
| Park (2016 and 2017a) [35,36] | Chair yoga | Certified yoga instructor | Group exercise and instruction manual with photos | Senior housing development | 8 | 16 | 2 | 45 | Daily logs | Logs were not completed |
| Park (2017b) [37] | Sitting boxing | NR | Group exercise | Rehabilitation care hospital | 6 | 18 | 3 | 30 | NR | NR |
| Park (2019) [38] | Chair yoga | Certified yoga instructor, music therapist, fitness instructor | Group exercise | College of medicine and centre for comprehensive brain health, community-based day centres for AD/dementia | 12 | 24 | 2 | 45 | NR | NR |
| Rieping (2019) [39] | Chair-based exercises: aerobic or with TheraBand | NR | NR | NR | 14 | 28 | 2 | 45 | NR | NR |
| Venturelli (2010) [40] | Circuit-based upper body exercise | Kinesiologist | Group exercise | Residents from a geriatric institute | 12 | 36 | 3 | 45 | Attendance at sessions | 75% |
| Vogler (2009) [41] | Seated exercises targeted hip flexion, extension, abduction, knee flexion and extension, and ankle plantar and dorsiflexion | Physical therapists | Delivered at participants’ home | Aged care and rehabilitation centre- Hospital/home | 12 | 36 | 3 | NR | Attendance at sessions | 70% |
| Vogler (2012) [42] | Home-based seated exercises: weight bearing or resistance | Physiotherapists | Group exercise | Home | 12 | 36 | 3 | NR | Self-reported completion of exercise sessions | 70% |
| Yao (2019) [12] | Chair yoga | Instructor | Group exercise | 2 communities | 12 | 24 | 2 | 110 | NR | NR |
| Outcome | Effect Size | 95% CI | No. of Participants | No. of Studies | I2 (%) |
|---|---|---|---|---|---|
| Objective Physical Function | |||||
| Berg Balance Scale | MD 0.66 | −1.01, 2.33 | 359 | 5 | 20% |
| Handgrip | MD 2.10 * | 0.76, 3.43 | 266 | 7 | 42% |
| Timed up and go test | MD 0.95 | −1.12, 3.01 | 394 | 7 | 39% |
| Gait Speed | MD −0.03 | −0.21, 0.16 | 450 | 6 | 77% |
| 30 s arm curl test | MD 2.82 * | 1.34, 4.31 | 97 | 3 | 71% |
| 30 s chair stand test | MD 2.25 * | 0.64, 3.86 | 97 | 3 | 62% |
| Subjective Physical Function | |||||
| Activities of daily living | SMD 0.32 | −0.4, 1.04 | 126 | 4 | 74% |
| Falls Efficacy | SMD −0.06 | −0.46, 0.34 | 208 | 5 | 49% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Klempel, N.; Blackburn, N.E.; McMullan, I.L.; Wilson, J.J.; Smith, L.; Cunningham, C.; O’Sullivan, R.; Caserotti, P.; Tully, M.A. The Effect of Chair-Based Exercise on Physical Function in Older Adults: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 1902. https://doi.org/10.3390/ijerph18041902
Klempel N, Blackburn NE, McMullan IL, Wilson JJ, Smith L, Cunningham C, O’Sullivan R, Caserotti P, Tully MA. The Effect of Chair-Based Exercise on Physical Function in Older Adults: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2021; 18(4):1902. https://doi.org/10.3390/ijerph18041902
Chicago/Turabian StyleKlempel, Natalie, Nicole E. Blackburn, Ilona L. McMullan, Jason J. Wilson, Lee Smith, Conor Cunningham, Roger O’Sullivan, Paolo Caserotti, and Mark A. Tully. 2021. "The Effect of Chair-Based Exercise on Physical Function in Older Adults: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 18, no. 4: 1902. https://doi.org/10.3390/ijerph18041902