
Health Education Intervention on Hearing Health Risk Behaviors in College Students


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
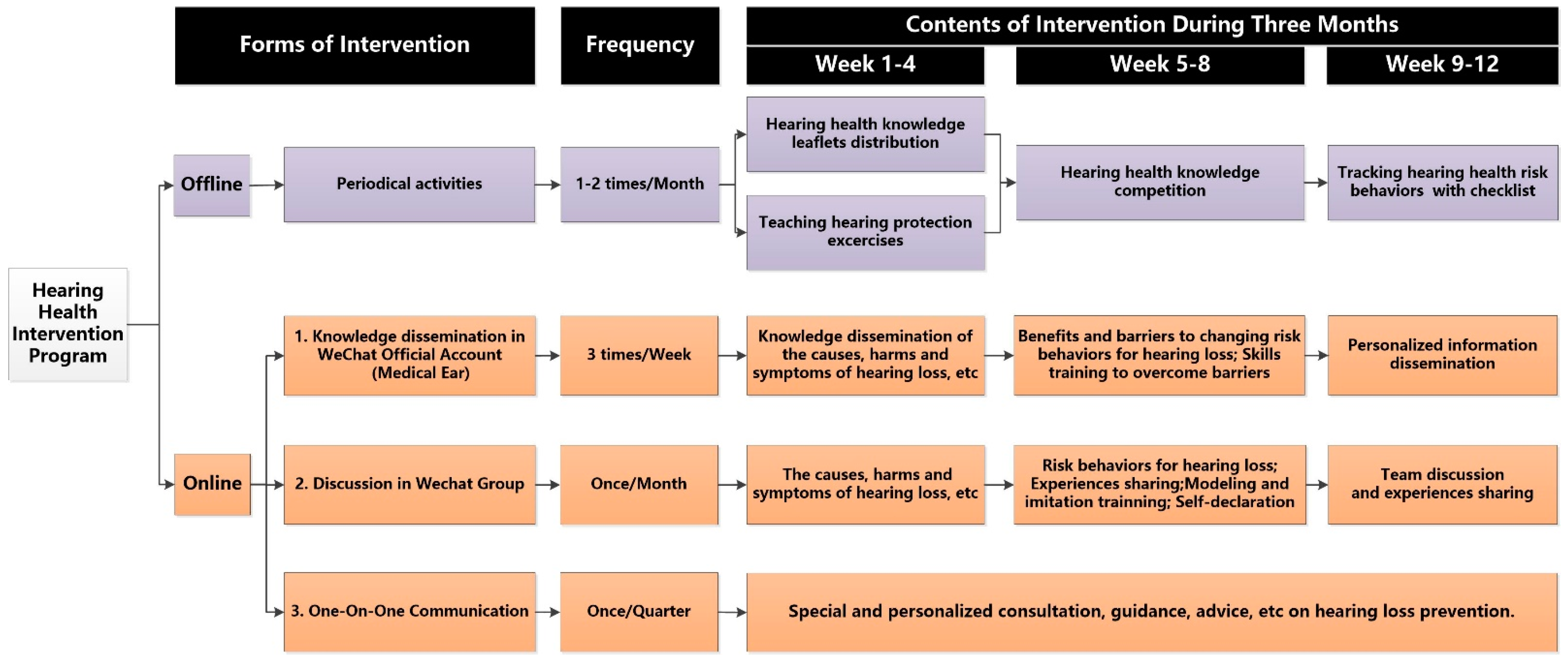
2.2. Hearing Health Intervention
2.3. Questionnaire Survey
2.4. Statistical Analysis
3. Results
3.1. Basic Characteristics of the Participants
3.2. Baseline Comparison and the Effects of Intervention on Hearing Health Knowledge and Belief
3.3. Baseline Comparison and the Effects of Intervention on Hearing Health Related Behaviors
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

References
- Disease, G.B.D.; Injury, I.; Prevalence, C. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1545–1602. [Google Scholar]
- World Health Organization (WHO). New WHO-ITU Standard Aims to Prevent Hearing Loss among 1.1 Billion Young People. Available online: https://www.who.int/zh/news-room/fact-sheets/detail/deafness-and-hearing-loss (accessed on 20 August 2020).
- Tung, C.Y.; Chao, K.P. Effect of recreational noise exposure on hearing impairment among teenage students. Res. Dev. Disabil. 2013, 34, 126–132. [Google Scholar] [CrossRef]
- Balanay, J.A.; Kearney, G.D. Attitudes toward noise, perceived hearing symptoms, and reported use of hearing protection among college students: Influence of youth culture. Noise Health 2015, 17, 394–405. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Hearing Loss due to Recreational Exposure to Loud Sounds: A Review 2015. Available online: https://apps.who.int/iris/bitstream/handle/10665/154589/9789241508513_eng.pdf.PublishedMarch2015 (accessed on 18 August 2020).
- Danhauer, J.L.; Johnson, C.E.; Byrd, A.; Degood, L.; Meuel, C.; Pecile, A.; Koch, L.L. Survey of college students on iPod use and hearing health. J. Am. Acad. Audiol. 2009, 20, 5–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- You, S.; Kwak, C.; Han, W. Use of Personal Listening Devices and Knowledge/Attitude for Greater Hearing Conservation in College Students: Data Analysis and Regression Model Based on 1009 Respondents. Int. J. Environ. Res. Public Health 2020, 17, 1–26. [Google Scholar]
- Liang, M.; Zhao, F.; French, D.; Zheng, Y. Characteristics of noise-canceling headphones to reduce the hearing hazard for MP3 users. J. Acoust. Soc. Am. 2012, 131, 4526–4534. [Google Scholar] [CrossRef] [PubMed]
- Hutchinson Marron, K.; Marchiondo, K.; Stephenson, S.; Wagner, S.; Cramer, I.; Wharton, T.; Hughes, M.; Sproat, B.; Alessio, H. College students’ personal listening device usage and knowledge. Int. J. Audiol. 2015, 54, 384–390. [Google Scholar] [CrossRef]
- Rahnavard, Z.; Mohammadi, M.; Rajabi, F.; Zolfaghari, M. An Educational Intervention Using Health Belief Model on Smoking Preventive Behavior Among Female Teenagers. Hayat J. Fac. Nurs. Midwifery 2011, 17, 15–26. [Google Scholar]
- Khan, K.M.; Bielko, S.L.; McCullagh, M.C. Efficacy of hearing conservation education programs for youth and young adults: A systematic review. BMC Public Health 2018, 18, 1286. [Google Scholar] [CrossRef] [PubMed]
- Knobel, K.A.; Lima, M.C. Effectiveness of the Brazilian version of the Dangerous Decibels(®) educational program. Int. J. Audiol. 2014, 53, S35–S42. [Google Scholar] [CrossRef]
- Keppler, H.; Ingeborg, D.; Sofie, D.; Bart, D. The effects of a hearing education program on recreational noise exposure, attitudes and beliefs toward noise, hearing loss, and hearing protector devices in young adults. Noise Health 2015, 17, 253–262. [Google Scholar] [CrossRef] [Green Version]
- Wang, D.H.; Zhuang, Y.Z.; Wu, Y.Y.; Ma, H.Y.; Xu, L.W. Analysis of influential factors of self-reported hearing loss deviation in young adults. J. Public Health (Bangk.) 2020, 28, 455–461. [Google Scholar] [CrossRef] [Green Version]
- Zak-Place, J.; Stern, M. Health belief factors and dispositional optimism as predictors of STD and HIV preventive behavior. J. Am. Coll. Health 2004, 52, 229–236. [Google Scholar] [CrossRef]
- Saunders, G.H.; Frederick, M.T.; Silverman, S.C.; Nielsen, C.; Laplante-Lévesque, A. Description of Adults Seeking Hearing Help for the First Time According to Two Health Behavior Change Approaches: Transtheoretical Model (Stages of Change) and Health Belief Model. Ear Hear. 2016, 37, 324–333. [Google Scholar] [CrossRef]
- Khan, K.M.; Evans, S.S.; Bielko, S.L.; Rohlman, D.S. Efficacy of technology-based interventions to increase the use of hearing protections among adolescent farm workers. Int. J. Audiol. 2018, 57, 124–134. [Google Scholar] [CrossRef]
- Matei, R.; Broad, S.; Goldbart, J.; Ginsborg, J. Health Education for Musicians. Front. Psychol. 2018, 9, 1137. [Google Scholar] [CrossRef]
- Imam, L.; Hannan, S.A. Noise-induced hearing loss: A modern epidemic? Br. J. Hosp. Med. (Lond.) 2017, 78, 286–290. [Google Scholar] [CrossRef] [PubMed]
- Jiang, W.; Zhao, F.; Guderley, N.; Manchaiah, V. Daily music exposure dose and hearing problems using personal listening devices in adolescents and young adults: A systematic review. Int. J. Audiol. 2016, 55, 197–205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clercq, C.M.P.L.; Ingen, G.V.; Ruytjens, L.; Schroeff, M.P.V.D. Music-induced Hearing Loss in Children, Adolescents, and Young Adults: A Systematic Review and Meta-analysis. Otol. Neurotol. 2016, 37, 1208–1216. [Google Scholar] [CrossRef] [PubMed]
- Sunny, O.D.; Asoegwu, C.N.; Abayomi, S.O. Subjective tinnitus and its association with use of ear phones among students of the College of Medicine, University of Lagos, Nigeria. Int. Tinnitus. J. 2012, 17, 169–172. [Google Scholar] [CrossRef] [PubMed]
- Seedat, R.Y.; Ehlers, R.; Lee, Y.; Mung’omba, C.; Plaatjies, K.; Prins, M.; Randeree, M.; Zakhura, M.; Joubert, G. Knowledge of the audiological effects, symptoms and practices related to personal listening devices of health sciences students at a South African university. J. Laryngol. Otol. 2020, 134, 20–23. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.; Han, X.; Fang, H.; Xu, C.; Lin, X.; Xia, S.; Yu, W.; He, J.; Jiang, S.; Tao, H. Impact of Health Education on Knowledge and Behaviors toward Infectious Diseases among Students in Gansu Province, China. Biomed. Res. Int. 2018, 2018, 6397340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marlenga, B.; Linneman, J.G.; Pickett, W.; Wood, D.J.; Kirkhorn, S.R.; Broste, S.K.; Knobloch, M.J.; Berg, R.L. Randomized trial of a hearing conservation intervention for rural students: Long-term outcomes. Pediatrics 2011, 128, e1139–e1146. [Google Scholar] [CrossRef] [PubMed]
- Martin, W.H.; Sobel, J.L.; Griest, S.E.; Howarth, L.C.; Becker, T.M. Program Sustainability: Hearing Loss and Tinnitus Prevention in American Indian Communities. Am. J. Prev. Med. 2017, 52, S268–S270. [Google Scholar] [CrossRef] [Green Version]
- Klein, B.A.; Weintraub, J.A.; Brame, J.L.; Kowlowitz, V.; McKenna, N.M.; Ciarrocca, K. Audiology and oral health professional students: An interprofessional education collaboration. J. Dent. Educ. 2020, 84, 983–990. [Google Scholar] [CrossRef]

{kind=link}
| Characteristic | Total (n = 830) | Male | p | Female | p | ||
|---|---|---|---|---|---|---|---|
| Intervention Group (n = 61) | Control Group (n = 180) | Intervention Group (n = 358) | Control Group (n = 231) | ||||
| Age, years | 19.57 ± 0.85 | 19.62 ± 0.637 | 19.70 ± 0.838 a | 0.512 | 19.42 ± 0.759 | 19.66 ± 0.991 | 0.002 |
| Grade | <0.001 | <0.001 | |||||
| Sophomore | 416 (50.1) | 45 (73.8) | 58 (32.2) b | 220 (40.3) | 93 (61.5) | ||
| Junior | 414 (49.9) | 16 (26.2) | 122 (67.8) | 138 (59.7) | 138 (38.5) | ||
| Tinnitus | 0.734 | 0.179 | |||||
| No | 402 (48.4) | 30 (49.2) | 84 (46.7) | 183 (51.1) | 105 (45.5) | ||
| Yes | 428 (51.6) | 31 (50.8) | 96 (53.3) | 175 (48.9) | 126 (54.5) | ||
| Earache | 0.996 | 0.359 | |||||
| No | 569 (68.6) | 42 (68.9) | 124 (68.9) | 250 (69.8) | 153 (66.2) | ||
| Yes | 261 (31.4) | 19 (31.1) | 56 (31.1) | 108 (30.2) | 78 (33.8) | ||
| Ear tightness | 0.461 | 0.359 | |||||
| No | 595 (71.7) | 47 (77.0) | 130 (72.2) | 259 (72.3) | 159 (68.8) | ||
| Yes | 235 (28.3) | 14 (23.0) | 50 (27.8) | 99 (27.7) | 72 (31.2) | ||
| Number of people with hearing loss in the family | 0.909 | 0.993 | |||||
| 0 | 322 (38.8) | 25 (41.0) | 73 (40.6) | 136 (38.0) | 88 (38.1) | ||
| 1 | 290 (34.9) | 23 (37.7) | 64 (35.6) | 124 (34.6) | 79 (34.2) | ||
| ≥2 | 218 (26.3) | 13 (21.3) | 43 (23.9) | 98 (27.4) | 64 (27.7) | ||
| Variable | Male | p | Female | p | ||
|---|---|---|---|---|---|---|
| Control | Intervention | Control | Intervention | |||
| (n = 180) | (n = 61) | (n = 231) | (n = 358) | |||
| Score of Hearing Health Knowledge | ||||||
| Baseline | 30.37 ± 6.24 | 29.33 ± 6.77 | 31.51 ± 5.17 | 31.01 ± 5.47 | - | |
| T2–T1 | 1.03 ± 9.09 | 3.48 ± 8.93 | 0.180 | 1.45 ± 7.21 | 3.23 ± 5.80 | 0.007 |
| T3–T1 | 1.20 ± 11.04 | 1.95 ± 12.29 | 0.887 | 1.95 ± 8.05 | 3.97 ± 8.04 | 0.014 |
| Score of Hearing Health Belief | ||||||
| Baseline | 164.57 ± 18.14 | 163.87 ± 16.13 | 171.08 ± 13.98 | 168.08 ± 14.67 | - | |
| T2–T1 | −1.56 ± 20.09 | 2.48 ± 18.73 | 0.368 | −2.68 ± 16.00 | −0.10 ± 16.54 | 0.183 |
| T3–T1 | −0.88 ± 21.70 | −2.28 ± 24.47 | 0.459 | −2.41 ± 15.98 | 1.32 ± 18.31 | 0.047 |
| Perceived Susceptibility | ||||||
| Baseline | 13.05 ± 3.50 | 13.77 ± 3.50 | 13.77 ± 3.30 | 13.41 ± 2.98 | - | |
| T2–T1 | −0.13 ± 4.23 | −0.49 ± 4.21 | 0.417 | −0.64 ± 4.04 | −0.54 ± 3.58 | 0.861 |
| T3–T1 | 0.56 ± 3.82 | 0.15 ± 4.55 | 0.290 | 0.26 ± 3.59 | 0.14 ± 3.86 | 0.734 |
| Perceived Severity | ||||||
| Baseline | 37.84 ± 4.86 | 37.67 ± 4.68 | 38.86 ± 4.42 | 38.11 ± 4.74 | - | |
| T2–T1 | −0.88 ± 7.88 | 0.43 ± 5.56 | 0.259 | −0.23 ± 6.49 | 1.15 ± 6.20 | 0.030 |
| T3–T1 | −1.04 ± 8.57 | −1.48 ± 10.08 | 0.777 | −0.11 ± 5.87 | 1.03 ± 6.47 | 0.065 |
| Perceived Benefits | ||||||
| Baseline | 30.81 ± 4.53 | 30.11 ± 3.96 | 31.06 ± 4.05 | 30.65 ± 4.15 | - | |
| T2–T1 | −0.22 ± 5.91 | 0.49 ± 4.14 | 0.724 | 0.06 ± 5.13 | 0.28 ± 5.02 | 0.677 |
| T3–T1 | −1.38 ± 6.99 | −1.67 ± 7.50 | 0.719 | −0.50 ± 5.22 | −0.21 ± 5.85 | 0.578 |
| Perceived Barriers | ||||||
| Baseline | 24.92 ± 6.83 | 23.93 ± 6.62 | - | 25.84 ± 5.97 | 24.73 ± 5.79 | - |
| T2–T1 | −0.73 ± 8.60 | 0.39 ± 8.33 | 0.442 | −0.87 ± 7.54 | −0.81 ± 7.36 | 0.841 |
| T3–T1 | −1.74 ± 8.91 | −1.67 ± 9.49 | 0.696 | −3.20 ± 7.25 | −1.48 ± 7.88 | 0.059 |
| Cues to Action | ||||||
| Baseline | 28.69 ± 6.03 | 28.56 ± 4.85 | - | 30.11 ± 4.54 | 30.48 ± 4.30 | - |
| T2–T1 | 0.24 ± 7.83 | 1.03 ± 5.48 | 0.759 | 0.15 ± 5.95 | −0.47 ± 6.17 | 0.227 |
| T3–T1 | 1.18 ± 7.06 | 1.39 ± 7.90 | 0.415 | 0.64 ± 5.94 | 0.36 ± 6.15 | 0.680 |
| Perceived Self-Efficacy | ||||||
| Baseline | 29.26 ± 5.34 | 29.82 ± 5.08 | 31.43 ± 4.63 | 30.70 ± 4.58 | - | |
| T2–T1 | 0.17 ± 5.49 | 0.62 ± 6.01 | 0.705 | −1.16 ± 5.42 | 0.28 ± 5.27 | 0.008 |
| T3–T1 | 1.54 ± 6.67 | 1.00 ± 6.97 | 0.467 | 0.51 ± 5.13 | 1.49 ± 5.36 | 0.074 |
| Behaviors | Males (n = 241) | Females (n = 589) | ||||||
|---|---|---|---|---|---|---|---|---|
| T2–T1 | T3–T1 | T2–T1 | T3–T1 | |||||
| OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p | |
| The average frequency of using headphones ≥3 times/day | 1.393 (0.654–2.964) | 0.39 | 1.387 (0.672–2.861) | 0.376 | 1.913 (1.148–3.189) | 0.013 | 1.612 (1.019–2.550) | 0.041 |
| Average duration of using headphones ≥30 min each time | 1.039 (0.507–2.127) | 0.918 | 1.196 (0.604–2.368) | 0.608 | 1.540 (1.014–2.339) | 0.043 | 1.854 (1.233–2.788) | 0.003 |
| Volume of the headphones ≥40% of the total volume | 1.948 (0.807–4.703) | 0.138 | 1.219 (0.520–2.857) | 0.649 | 2.416 (1.351–4.320) | 0.003 | 2.224 (1.275–3.882) | 0.005 |
| Sleeping with headphones for listening to music or radio | 1.605 (0.759–3.392) | 0.216 | 2.554 (1.184–5.509) | 0.017 | 1.725 (1.107–2.689) | 0.016 | 1.991 (1.284–3.088) | 0.002 |
| Probability of increasing headphone volume in noisy environment ≥50% | 1.014 (0.458–2.243) | 0.972 | 1.037 (0.496–2.169) | 0.923 | 1.032 (0.676–1.576) | 0.884 | 1.453 (0.967–2.184) | 0.072 |
| Using in-ear type headphones | 0.884 (0.333–2.348) | 0.805 | 1.062 (0.408–2.763) | 0.902 | 1.065 (0.626–1.812) | 0.816 | 1.386 (0.812–2.364) | 0.231 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, D.; Li, C.; Wang, Y.; Wang, S.; Wu, S.; Zhang, S.; Xu, L. Health Education Intervention on Hearing Health Risk Behaviors in College Students. Int. J. Environ. Res. Public Health 2021, 18, 1560. https://doi.org/10.3390/ijerph18041560
Wang D, Li C, Wang Y, Wang S, Wu S, Zhang S, Xu L. Health Education Intervention on Hearing Health Risk Behaviors in College Students. International Journal of Environmental Research and Public Health. 2021; 18(4):1560. https://doi.org/10.3390/ijerph18041560
Chicago/Turabian StyleWang, Dahui, Chenhui Li, Yi Wang, Shichang Wang, Shuang Wu, Shiyan Zhang, and Liangwen Xu. 2021. "Health Education Intervention on Hearing Health Risk Behaviors in College Students" International Journal of Environmental Research and Public Health 18, no. 4: 1560. https://doi.org/10.3390/ijerph18041560