Occupational Therapy Interventions in Adults with Multiple Sclerosis or Amyotrophic Lateral Sclerosis: A Scoping Review


Abstract
:1. Introduction
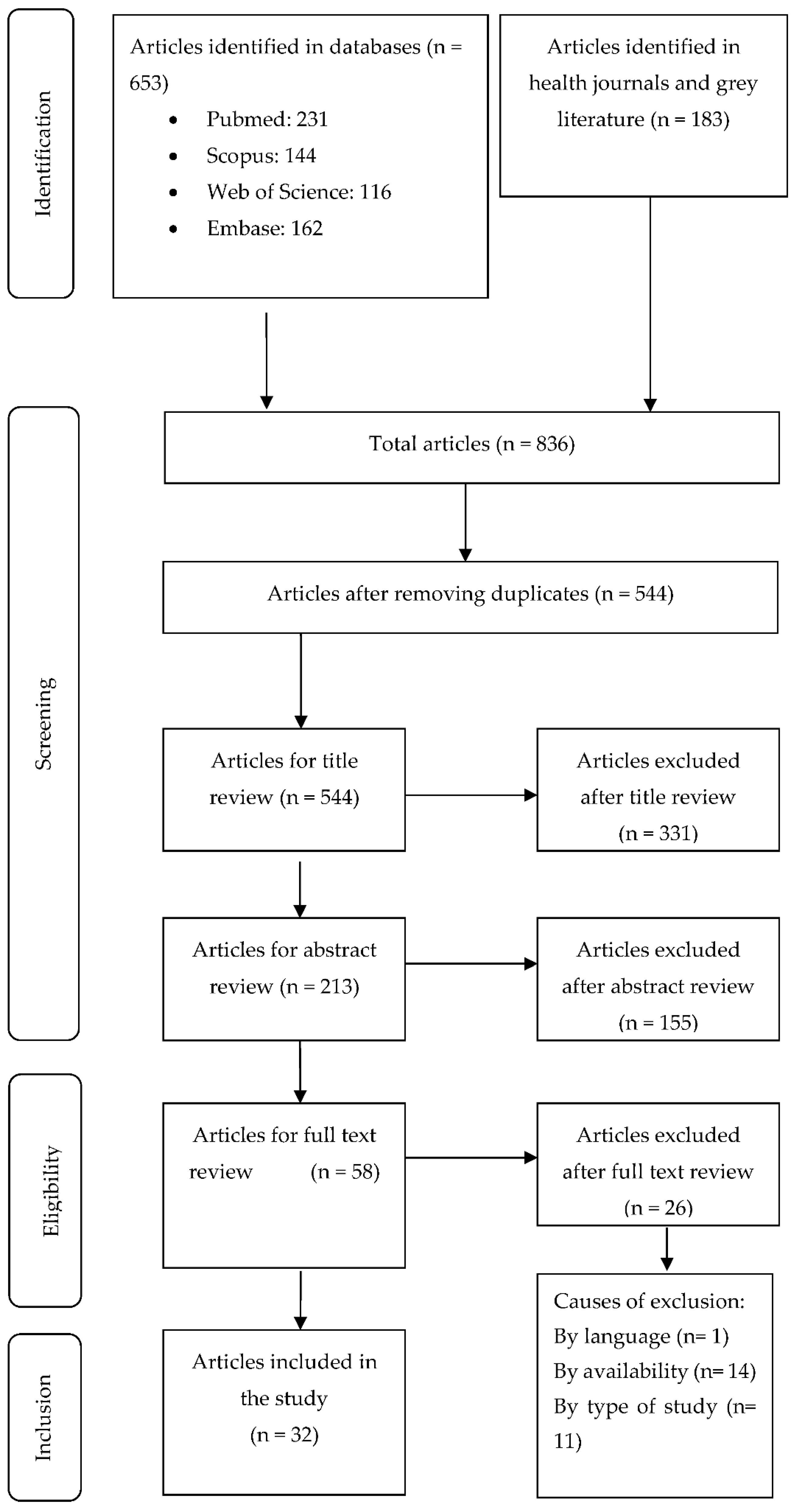
2. Materials and Methods
3. Results
3.1. Interventions in Fatigue and Energy Conservation
3.2. Cognitive Interventions
3.3. Physical Interventions

{kind=link}
| Authors, Year, Country | Objective | Sample (n), Disease | Intervention | Results | Conclusions |
|---|---|---|---|---|---|
| Eyssen et al. [55], 2013, Netherlands | To evaluate the effectiveness of a client-centred occupational therapy. | 269, MS | Client-centred occupational therapy | The IG results were not significant and in the second measuring results were negative. | There was no improvement in disability, participation and autonomy in IG. |
| Eyssen et al. [56], 2014, Netherlands | To check whether client-centred practice spends more time on assessment than on intervention. | 269, MS | Client-centred occupational therapy | The results showed a significant increase in time dedication on the diagnostic process in the IG. | The client-centred practice devotes too much time to the evaluation process with no improvements. |
| Block et al. [57], 2009, United States | To evaluate the effectiveness of the development of capacities and the health promotion in self-efficacy and ability to achieve objectives. | 35, MS | Health promotion in self-efficacy and empowerment | The results showed significant improvements in self-efficacy and ability to achieve objectives. | The program could took action in multiple areas of intrapersonal, interpersonal, and behavioral functioning. |
| Raglio et al. [58], 2016, Italy | To evaluate the effectiveness of a music therapy and its influence on anxiety, depression or QoL. | 30, ALS | Music therapy | There were only improvements in Mc Gill Quality of life Questionnaire. | The music therapy program showed an improvement in the QoL. |
| Reilly y Hynes. [42], 2018, Ireland | To evaluate the efectiveness of an occupation-based cognitive program in improving daily life and cognitive decline. | 12, MS | Cognitive intervention (CI) for managing employment and daily life. | There were significant improvements in all areas. | CI is considered the most appropriate intervention. It can be more effective in newly diagnosed people. |
| Chiaravalloti et al. [43], 2018, United States | To examine the efectiveness of a SPT. | 21, MS | Cognitive intervention in SPT. | The group that received SPT obtained better results than the CG in processing speed, learning and memory, and performance. | Results provide support of SPT in treating processing speed deficits in persons with MS. |
| Goverover et al. [20], 2017, United States | To examine the effectiveness of a self-generated program of memory and learning strategies. | 35, MS | Cognitive intervention to improve memory and learning | The IG improved learning, memory, self-regulation, metacognition, depression, functional status, and QoL. | Results provides evidence that the intervention improves memory and affective symptomatology. |
| Schettini et al. [41], 2015, Italy | To evaluate the feasibility and usability of an assistive technology prototype for communication. | 8, ALS | Cognitive intervention in usability of an assistive technology prototype for communication and home control | There were no significant differences between the different measures. | The study shows the feasibility and usability of assistive technology prototype. |
| Gentry. [19], 2008, United States | To evaluate the effectiveness of a PDA training program, as the assistive technology. | 21, MS | Cognitive intervention with de use of PDAs to improve occupational performance. | Functional performance increased significantly with PDA use. | PDA still work as a compensatory measure for their deficit in executive functions, but it does not improve memory. |
| Shevil et al. [44], 2009, Israel-United States | To increase knowledge of cognitive impairments, increase levels of self-efficacy and increase use of management strategies. | 35, MS | Cognitive intervention with a program (Mind over Matter) for the knowledge and management of the cognitive deficits. | Participants significantly increased knowledge of cognitive impairments and levels of self-efficacy in their ability to manage cognitive difficulties. | The results support benefits of self-management cognitive perspective to improve cognitive symptoms. |
| Gómez-Fernández et al. [54], 2001, Cuba | To examine the effect of multifactorial treatment in health. | 6, ALS | Multifactorial physical intervention with intensive rehabilitation programme. | People improved significantly on forced vital capacity and Functional Rating Scales. | Multifactorial rehabilitation works well for the health and survival. |
| Yang et al. [53], 2019, United States | To explore if patients can adapt to imbalances after a program of training in falls on a treadmill. | 13, MS | Physical intervention to improve stability and falls prevention. | There was a significant reduction in falls and significant improvements in stability and position. | With this training, people with MS may be able to improve their postural adjustments to prevent falls. |
| Kamm et al. [46], 2014, Switzerland | To evaluate the effectiveness of home-based program to improve manual dextery. | 39, MS | Physical intervention with manual dextery training. | People improved significantly manual dextery and no significant differences in strength straining | Home manual dextery training improved fine mobility in relation with activities of daily living. |
| Lamers et al. [45], 2019, Belgium | To evaluate the effectiveness of a task-oriented upper limb program. | 20, MS | Physycal intervention with task-oriented upper limb training by individualizing the intensity of training. | There were significant improvements of Action research arm test, Manual Ability Measure-36. | All participants performed the task-oriented training at their individualized intensity without any adverse effects. |
| Finlayson et al. [52], 2009, United States | To evaluate “Safe at Home BAASE” program for the management of falls risk. | 30, MS | Physical intervention with the “Safe at Home BAASE” program. | Significant improvements in knowledge, prevention and manage of falls risk with 5:6 sessions. | The program has potential to improve knowledge, skills and behavior associated with reduced personal fall risk. |
| Ortiz et al. [50], 2013, Spain | To examine postural control and balance with a virtual reality telerehabilitation program. | 50, MS | Physical intervention with a telerrehabilitation program to improve balance and postural control. | Significant improvement in balance, visual preference, the contribution of vestibular information, mean response time and Tinetti test yielded. | The rehabilitation program with virtual reality could be an alternative to standard rehabilitation programmes. |
| Waliño-Paniagua et al. [47], 2019, Spain | To compare the conventional occupational therapy treatment by virtual reality in manual dexterity training. | 16, MS | Physical intervention with virtual reality training in manual dexterity. | Program showed no significant differences in manual dexterity. Improvements were found in precision, execution times, and the efficiency of functional tasks. | This therapy with virtual reality can be complementary to conventional intervention. |
| Bovend´Eerdt et al. [51], 2010, United Kingdom | To evaluate the effectiveness of a motor imagery program compared with OT. | 30, MS | Physical intervention with a motor imagery program. | Compliance with advised treatment was poor in 85% of the therapists and in 72% of the patients. | Therapist and patient compliance was low, restricting the conclusions of the effectiveness of the imagery program |
| Kalron et al. [48], 2013, Israel | To evaluate the effectiveness of a sensory home-based hand re-education and manual dextery program. | 18, MS | Physical intervention with a sensory hand re-education and manual dextery program. | There were significant improvements in the IG on nine-hole peg test and functional dexterity test. | Sensory re-education training at an early stage of the disease can slow the progression of manual dexterity deterioration. |
| Bansi et al. [49], 2013, Switzerland | To investigate the impact of endurance training in health-related quality of life and fatigue | 60, MS | Physical intervention with endurance training with cycle-ergometer/aquatic-bike on QoL and fatigue. | Endurance training affects QoL and fatigue. Cardiorespiratory fitness and short-term TH2 were associated with better QoL. | Endurance training impacts on QoL and fatigue independently of the type of training (cycle-ergometer or aquatic-bike). |
| Vanage et al. [29], 2003, United States | To evaluate the effectiveness of an energy conservation program on fatigue. | 37, MS | Energy conservation program | Fatigue was and physical, cognitive, and psychosocial measures were improved. | The program was effective and reduced levels of fatigue in people with moderate-severe MS. |
| Rietberg et al. [36], 2014, Netherlands | To evaluate a multidisciplinary rehabilitation program for chronic fatigue compared to a nursing consultation program. | 48, MS | Multidisciplinary fatigue intervention | There were no significant differences in most fatigue measures. | Multidisciplinary rehabilitation was not more effective in reducing self-reported fatigue compared to nurse consultation. |
| Mathiowetz et al. [30], 2001, United States | To evaluate the efectiveness of an energy conservation program for its impact on fatigue, self-efficacy and quality of life. | 54, MS | Energy conservation program | Participants reported significantly less fatigue impact, increased self-efficacy, and improved quality of life. | The energy conservation program is effective in improving fatigue. |
| Ghahari et al. [34], 2009, Iran | To evaluate the effectivenes of a fatigue self-management program. | 23, MS | Fatigue intervention with an online self-manegement program | Participants exposed to pilot 3 (forums, activities online and quiz) improved significantly on the fatigue impact scale. | The results show that the online fatigue self-management program is a viable complex intervention. |
| D´hooghe et al. [36], 2018, Belgium | To evaluate the feasibility of a TeleCoach progam for the improvement of physical activity and fatigue levels. | 75, MS | Fatigue intervention with TeleCoach program through smartphone. | There were significant improvements in Fatigue Scale for Motor and Cognitive Functions. | The TeleCoach program is viable as complementary training to conventional treatment. |
| Kos et al. [38], 2007, Belgium | To evaluate the effectiveness of a fatigue management program. | 51, MS | Multidisciplinary fatigue intervention. | A reduction of Modified Fatigue Impact Scale was found in 17% of IG compared to 44% after the placebo intervention programme | The multidisciplinary fatigue management programme showed no efficacy in reducing the impact of fatigue compared to a placebo intervention programme |
| Sauter et al. [35], 2008, Austria | To examine the effectiveness of fatigue management and energy conservation strategies. | 32, MS | Fatigue intervention | Significant improvements were found in people’s physical and cognitive fatigue. There were less fewer signs of depression and the quality of sleep improved | Fatigue cannot be completely eliminated, but there were improvements in fatigue management and energy conservation |
| Mathiowetz et al. [32], 2005, United States | To evaluate the effectiveness of an energy conservation course. | 169, MS | Energy conservation program | There were significants effects on reducing the physical and social subscales of fatigue and on increasing QoL. | The energy conservation program is effective in improving fatigue, self-efficacy and quality of life in people with moderate-severe MS |
| Finlayson et al. [33], 2011, United States | To evaluate the effectiveness of a teleconference-delivered program on fatigue management | 181, MS | Fatigue intervention through teleconference | There were significant improvements in fatigue and quality of life. | The results support for the viability of teleconference-delivered fatigue management education. |
| Kos et al. [40], 2016, Belgium | To evaluate the effectiveness of an individual SMOoTh vs relaxation on the performance of and satisfaction with relevant daily activities. | 31, MS | Fatigue Intervention with the SMOoTh program | There were significant improvements in COPM. | Both interventions showed improvements in the satisfaction and performance of activities. |
| Lamb et al. [31], 2004, United States | To evaluate the effectiveness of an energy conservation program vs self-study material at home in a missed session | 92, MS | Energy conservation program | There were no significant differences between groups. | The self-study material is just as effective if the person miss a session, but it would not work as the only method of treatment. |
| Hersche et al. [39], 2019, Switzerland | To evaluate the effectiveness of the inpatient energy management education (IEME) | 47, MS | Fatigue intervention through IEME program | There were significant improvements in fatigue in both groups. The IEME alone resulted in significant improvements in self-efficacy regarding energy conservation strategies. | The IEME program was effective at improving self-efficacy in performance and fatigue management strategies. |
| Author, Year, Country | Intervention Category | Intervention | CG/IG | Duration (Weeks) | Sessions | Measurment Instruments | Intervention Manager |
|---|---|---|---|---|---|---|---|
| Eyssen et al. [55], 2013, Netherlands | Other categories | Client-centred OT | CG: Traditional therapy for the patient.The client-centred framework and tools were not available. IG: OTs encouraged participants to choose, organise and perform activities the patients found useful and meaningful in their environment. The client-centred process model was based on the Canadian practice process framework. | 52 | NS | EDSS, DIP, IPA, 9HPT, MFIS, PES, SF36, COPM, ECGP | OT |
| Eyssen et al. [56], 2014, Netherlands | Other categories | Client-centred OT | CG: Traditional therapy for the patient. The client-centred framework and tools were not available IG: OTs encouraged participants to choose, organise and perform activities the patients found useful and meaningful in their environment. The client-centred process model was based on the Canadian practice process framework. | 104 | NS | EDSS | OT |
| Raglio et al. [58], 2016, Italy | Other categories * | Music therapy * | CG: Participants received physical and speech rehabilitation, OT an psychological support IG: Music therapy sessions. OTs stimulates patients to communicate using instruments and express emotions. | 4 | Three-weekly half-hour sessions | ALSFRS-R, HADS, MQoL-it, MTRS | OT |
| Block et al. [57], 2009, United States | Other categories | Health-promotion and self-efficacy management | CG: Nontreatment IG: A variety of indoor and outdoor activities for indepent living and health promotion like using public transport or recreational activities included sailing or cycling. | 23 | Ten full day/sessions, twice a month | GSE, PAL | OT, psichologist |
| Reilly y Hynes. [42], 2018, Ireland | Cognitive intervention | Cognitive Occupation- Based Programe (COB-MS) | IG: Compensatory strategies and new routines and techniques about employment and daily life. There are seven group session and one individual session. Participants increase their knowledge about cognition, sleep, motivation and future goals. Pre-test/post-test were done. | 8 | Once-weekly sixty minutes sessions | GAS, OSA-DLS, CVLT-II, BVMT-R, SDMT, TMT, BRIEF-A, EMQ-R | OT |
| Chiaravalloti et al. [43], 2018, United States | Cognitive intervention | Speed of Processing Training (SPT) | CG: Nontreatment IG: Three tasks about speed of processing, divided attention and selective attention on a computer. First, participants practice a discrimination task with targets. In task 2, participants have to locate a peripheral target while they are doing task 1. In task 3, they have to do the same at task 2 but with distracters. | 5 | Twice-weekly thirty to forty minutes sessions | WAIS-III, LC, PC, CVLT-II, TIADL | OT, neuropsychologists |
| Goverover et al. [20], 2017, United States | Cognitive intervention | Self-generation learning program (self-GEN trial) | CG: Memory and learning tasks. Participants have to learn an items list. IG: Memory and learning task with techniques to improve this skills. Participants have to learn the same list but it has pictures, sentences or a word pair. Participants can choose whose the most useful technique to learn words is. | 3 | Twice-weekly sixty minutes sessions | CMT, SRSI, MIST, CVLT-II, MFQ, AQ, FBP, CMDI, FAMS | OT |
| Schettini et al. [41], 2015, Italy | Cognitive intervention * | Assistive technology prototype for communication and home control * | IG1: Participants were asked to control a standalone P300-speller based BCI to test the ability to control a BCI system and to subsequently compare the performance obtained with the BCI with that observed while controlling the assistive technology prototype with the BCI channel. IG2: Users, who operated via a conventional or an alternative input device (eg, mouse, buttons) that best matched their residual motor abilities controlling the assistive technology. Two task: Self-managed environmental control task: and Self-managed communication task. IG3: Assistive technology. The prototype visual interface consisted of several menus. Stimulation timing and number of stimulus repetitions for each item were the same as in condition Two tasks: Copy environmental control task: and Copy communication task. | 3 | Once-weekly ninety minutes session | BCI online copy accuracy, BCI offline accuracy, AT prototype online accuracy during self managed tasks). BCI offline Writen Symbol Rate, AT prototype time for correct selection). VAS, System Usability Scale. | OT, engineer, neurologist |
| Gentry. [19], 2008, United States | Cognitive intervention | 0T therapy using PDAs as assistive technology | IG: Participants learn to use PDAs for three weeks (week 10 to 12) and the OT measure eight weeks before and eight weeks later. They learn about calendar reminders, use of contacts, troubleshoot and train in use of additional features. | 21 | Two sixty minutes sessions and two ninety minutes sessions | RBMT-E, COPM, CHART-R | OT |
| Shevil et al. [44], 2009, Israel-United States | Cognitive intervention | Program: Mind over Matter.knolwedge and management. | IG: OTs teach to participantes about cognitive impairments and how to manage their symptoms. about how increase participant´s self-efficacy and the use of cognitive strategies. | 5 | Once-weekly two hours sessions | Knowledge quizzes, CMSEQ, CSQ | OT |
| Gómez-Fernández et al. [54], 2001, Cuba | Physical intervention * | Multifactorial intervention * | IG: Participants received a multifactorial treatment with breathing exercises; face, mouth and neck exercises, balance and walk exercises. OTs have to avoid participants fatigue in the treatment. Pre-test/post-test. | 4 | Monday to Friday seven hours’ sessions. Saturday three hours sessions | FVC, ALSFRS | OT, Neurologists, physiotherapists, logopaedits, defectologists, psychologists and physicians |
| Yang et al. [53], 2019, United States | Physical intervention | ActiveStep treadmill to improve stability and falls risk | IG: Participants walk on the treadmill with a safety harness and they have to adapt to unexpected slips. | Five sessions | Number of falls, COM, quality of steps | OT, kinesiologist, mathematical | |
| Kamm et al. [46], 2014, Switzerland | Physical intervention | A home-based program to improve manual dexterity in ADL | IG1: Participants are in two randomized groups. The first group practice a dexterity program (finger tapping, turning coins, modeling clay). IG2: The second group practice a theraband program with strength exercises. Pre-test/post-test. | 4 | Five weekly thirty minutes sessions | CRT, NHPT, JAMAR, CAHAI, | OT, neurologist |
| Lamers et al. [45], 2019, Belgium | Physical intervention | A task-oriented program to upper limb | CG: Conventional occupational therapy IG: Participants train the task-oriented program at individualized intensity. They have to practice unilateral and bilateral tasks in their daily life and the difficulty is increased throughout the program. | 8 | Five weekly sixty minutes sessions | NHPT, ARAT, BBT, TEMPA, MAM-36 | OT |
| Finlayson et al. [52], 2009, United States | Physical intervention | “Safe at Home BAASE” a fall risk management program. | IG: Participants train the program to increase the knowledge about falls and to learn skills to manage falls. There are 14 fall prevention strategies. In post-intervention, participants report whether they use the strategies. Pre-test/post-test. | 6 | Once weekly two hours sessions | FCS, FMS, FPMQ, FPSS, FES | OT |
| Ortiz et al. [50], 2013, Spain | Physical intervention | A virtual reality rehabilitation to improve balance and postural control | CG: Participants received physiotherapy treatment with strength exercises, propioception exercises, gait facilitation and muscle-tendon stretching. IG: Participants received telerehabilitation treatment using the Xbox 360® console monitored via videoconference following activities that have a certain difficulty and intensity (hitting object with hands and feet, imitating postures, obstacles). | 10 | Four weekly twenty minutes sessions | CDP, SOT, MCT | Multidisciplinar: physiotherapist/ OT |
| Waliño-Paniagua et al. [47], 2019, Spain | Physical intervention | OT virtual reality compared to conventional OT | CG: Conventional occupational therapy. IG: Participants received OT and virtual reality include leisure activities (play cards, play hockey, fishing) | 10 | Twice weekly thirty minutes sessions | PPT, JPT, GPT | OT |
| Bovend´Eerdt et al. [51], 2010, United Kingdom | Physical intervention | An integrated motor imagery program | CG: Participants watch a film with physical practice, Then, They have conventional OT and physiotherapy. IG: Participants watch a different film than CG and then, OTs train with patients with imagery strategies in particular tasks. | 7 | Two to three weekly six hours and a half the total time spent | GAS, BI, RMI, ARAT, NEADLS | OT, Physiotherapy |
| Kalron et al. [48], 2013, Israel | Physical intervention | A sensory re-education program on hand sensibility and manual dexterity | CG: Participants received OT sessions with non specific exposure via grasping objects. IG: Participants received two tasks. In the first task, participants are blindfolded and they have to recognize the object. In the second task, all objects are on a table and OTs describe the object. They have to discriminate it. | 10 | Five weekly twenty minutes sessions. | NHPT, FDT, TDP, S-W monofilaments | OT |
| Bansi et al. [49], 2013, Switzerland | Physical intervention | Effects of a endurance training in quality life and fatigue | IG: Participants in two groups performed a 3 weeks endurance exercise training on a cyclo-ergometer or an aquatic bike with different phases. | 3 | Four daily thirty to forty minutes sessions | FSMC, MFIS, SF-36 | OT, physiotherapist, neurophysicologist |
| Vanage et al. [29], 2003, United States | Fatigue intervention | An energy conservation course | CG: Participants received 8 weeks control treatment and then, they received 8 weeks energy conservation course. IG: Participants received 8 weeks energy conservation course and then, they received 8 weeks control treatment. | 8 | Once weekly sixty minutes sessions | FSS, FIS, MCA | OT |
| Rietberg et al. [36], 2014, Netherlands | Fatigue intervention | Multidisciplinary rehabilitation on chronic fatigue | CG: Participants received nurse consultation IG: Participants received physiotherapy, OT or social work sessions when they need. Physiotherapy sessions were determinate in 45 min sessions. | 12 | Number of sessions was on an as-needed basis, with a mínimum of 2 sessions | CIS-20R, MFIS FSS, FIM, DIP, IPA, MSIS-29, SF-36 | OT, physiotherapy, social worker |
| Mathiowetz et al. [30], 2001, United States | Fatigue intervention | An energy conservation course on fatigue impact | CG: Participants received 6 weeks control intervention with support and discussing about MS topics. IG: Participants received the energy conservation course learning about rest, communication, ergonomic principles, activity and balance lifestyle. | 6 | Once weekly two hours sessions | FIS, SEG, SF-36 | OT |
| Ghahari et al. [34], 2009, Iran | Fatigue intervention | An online fatigue self-management program | IG: Reachers transform the Energy Conservation Course into a online self-management program through sharing stories, information and activities. With an online version, patients can practice the program at home. | 6 | Once weekly two hours sessions | PW-BI, FIS, ACS, FSS, GES, DASS | OT |
| D´hooghe et al. [36], 2018, Belgium | Fatigue intervention | TeleCoach program by smartphone | IG: Participants received in their smartphones motivational messages focusing on energy management and monitoring the physical activities to improve fatigue levels. | 12 | NS | FSMC, MFIS | OT, neurologist, neuroscientist |
| Kos et al. [38], 2007, Belgium | Fatigue intervention | Multidisciplinary fatigue management program. | CG: Participants received information about topics that did not concern to fatigue (car adaptation, communication skills or general information abpur MS) IG: Participants received information about pharmacological treatment, diet, rest, strategies to manage fatigue or adaptation to work or home. | 4 | Once weekly two hours sessions | MFIS, FSS | OT, Multidisciplinary team |
| Sauter et al. [35], 2008, Austria | Fatigue intervention | A course of energy conservation for people with MS | CG: Participants did not receive treatment IG: Participants received information about different topics like rest, self care, communication, work or leisure tasks. | 6 | Once weekly two hours sessions | FSS, MFIS, MS-SFS, EDSS, MSFC, PSQI S-RSD | OT |
| Mathiowetz et al. [32], 2005, United States | Fatigue intervention | A course of energy conservation for people with MS | CG: Participants received 6 weeks control intervention with support and discussing about MS topics. IG: Participants received the energy conservation course learning about rest, communication, ergonomic principles, activity and balance lifestyle. | 6 | Once weekly two hours sessions | SEG, FIS, SF-36 | OT |
| Finlayson et al. [33], 2011, United States | Fatigue intervention | A teleconference- delivered fatigue management program for people with MS | IG: Participants were divided in two groups and they received the treatment in different weeks by teleconference. The intervention consist in teaching sessions, discussing and homework about topics like communication, fatigue, rest, ergomonics and balanced life. | 6 | Once weekly seventy minutes sessions | SF-36, FIS, FSS, SECQ | OT |
| Kos et al. [40], 2016, Belgium | Fatigue intervention | A self-management fatigue program (SMOoTh) | CG: Participants received physiotherapy sessions with relaxing techniques and some information. IG: Participant received information about fatigue, levels of activity, communication, use of wheelchairs, obstacles and facilitators at home and some strategies. | 3 | Once weekly thirty to ninety minutes sessions | SF-36, MFIS, COPM, CIS-20R, | OT |
| Lamb et al. [31], 2004, United States | Fatigue intervention | Energy conservation. | CG: Conventional OT. Participants did not receive any modules of treatment IG: Participants divided in three groups and they received one module, two modules, or more than two modules. Evaluators tried to check the course efficacy if participants do not receive some sessions. | 6 | Once weekly two hours sessions | SF-36, FIS, SEA, ECSS | OT |
| Hersche et al. [39], 2019, Switzerland | Fatigue intervention | An energy management education program. | CG: Participant received progressive muscles relaxation or group sessions. IG: Participants discussed and work about topics such as occupational balance, activity, fatigue, energy account, goals or effective communication. | 3 | Once weekly Two hours sessions | MFIS, SF-36, UWSES, SEPECSA | OT |
3.4. Other Interventions
4. Discussion
4.1. Fatigue Interventions and Energy Conservation
4.2. Cognitive Interventions
4.3. Physical Interventions
4.4. Other Interventions
4.5. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ramsaransing, G.S.M.; De Keyser, J. Benign course in multiple sclerosis: A review. Acta Neurol. Scand. 2006, 113, 359–369. [Google Scholar] [CrossRef] [PubMed]
- Talbott, E.; Malek, A.; Lacomis, D. The Epidemiology of Amyotrophic Lateral Sclerosis; Elsevier: Amsterdam, The Netherlands, 2016; Volume 138, pp. 225–238. [Google Scholar]
- Longinetti, E.; Fang, F. Epidemiology of amyotrophic lateral sclerosis. Curr. Opin. Neurol. 2019, 32, 771–776. [Google Scholar] [CrossRef]
- Hirst, C.; Ingram, G.; Pickersgill, T.; Swingler, R.; Compston, D.A.S.; Robertson, N.P. Increasing prevalence and incidence of multiple sclerosis in South East Wales. J. Neurol. Neurosurg. Psychiatry 2008, 80, 386–391. [Google Scholar] [CrossRef]
- Ford, H.L.; Gerry, E.; Johnson, M.; Williams, R. A prospective study of the incidence, prevalence and mortality of multiple sclerosis in Leeds. J. Neurol. 2000, 249, 260–265. [Google Scholar] [CrossRef] [PubMed]
- World Report on Disability. Available online: https://www.who.int/teams/noncommunicable-diseases/disability-and-rehabilitation/world-report-on-disability (accessed on 5 January 2021).
- Harirchian, M.H.; Fatehi, F.; Sarraf, P.; Honarvar, N.M.; Bitarafan, S. Worldwide prevalence of familial multiple sclerosis: A systematic review and meta-analysis. Mult. Scler. Relat. Disord. 2018, 20, 43–47. [Google Scholar] [CrossRef]
- Maver, A.; Lavtar, P.; Ristić, S.; Stopinšek, S.; Simčič, S.; Hočevar, K.; Sepčić, J.; Drulović, J.; Pekmezović, T.; Novaković, I.; et al. Identification of rare genetic variation of NLRP1 gene in familial multiple sclerosis. Sci. Rep. 2017, 7, 1–8. [Google Scholar] [CrossRef]
- Biernacki, T.; Sandi, D.; Kincses, Z.T.; Füvesi, J.; Rózsa, C.; Mátyás, K.; Vécsei, L.; Bencsik, K. Contributing factors to health-related quality of life in multiple sclerosis. Brain Behav. 2019, 9, e01466. [Google Scholar] [CrossRef]
- D’Amico, E.; Ba, M.P.; Lee, Y.-W.; Weimer, L.; Mitsumoto, H. Clinical evolution of pure upper motor neuron disease/dysfunction (PUMMD). Muscle Nerve 2012, 47, 28–32. [Google Scholar] [CrossRef] [PubMed]
- Yu, C.-H.; Mathiowetz, V. Systematic review of occupational therapy-related interventions for people with multiple sclerosis: Part 1. Activity and participation. Am. J. Occup. Ther. 2013, 68, 27–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amatya, B.; Khan, F.; Galea, M. Rehabilitation for people with multiple sclerosis: An overview of Cochrane Reviews. Cochrane Database Syst. Rev. 2019, 1. [Google Scholar] [CrossRef]
- Arbesman, M.; Sheard, K. Systematic review of the effectiveness of occupational therapy-related interventions for people with amyotrophic lateral sclerosis. Am. J. Occup. Ther. 2013, 68, 20–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oskarsson, B.; Gendron, T.F.; Staff, N.P. Amyotrophic lateral sclerosis: An update for 2018. Mayo Clin. Proc. 2018, 93, 1617–1628. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kubsik, A.; Klimkiewicz, P.; Klimkiewicz, R.; Janczewska, K.; Woldańska-Okońska, M. Rehabilitation in multiple sclerosis. Adv. Clin. Exp. Med. 2017, 26, 709–715. [Google Scholar] [CrossRef]
- Lincoln, N.; Bradshaw, L.; Constantinescu, C.S.; Day, F.; Drummond, A.; Fitzsimmons, D.; Harris, S.; Montgomery, A.; Das Nair, R. Group cognitive rehabilitation to reduce the psychological impact of multiple sclerosis on quality of life: The CRAMMS RCT. Heal. Technol. Assess. 2020, 24, 1–182. [Google Scholar] [CrossRef]
- Bombardier, C.H.; Cunniffe, M.; Wadhwani, R.; Gibbons, L.E.; Blake, K.D.; Kraft, G.H. The efficacy of telephone counseling for health promotion in people with multiple sclerosis: A randomized controlled trial. Arch. Phys. Med. Rehabil. 2008, 89, 1849–1856. [Google Scholar] [CrossRef] [PubMed]
- Kalina, J.T.; Hinojosa, J.; Strober, L.; Bacon, J.; Donnelly, S.; Goverover, Y. Randomized controlled trial to improve self-efficacy in people with multiple sclerosis: The community reintegration for socially isolated patients (Crisp) Program. Am. J. Occup. Ther. 2018, 72. [Google Scholar] [CrossRef]
- Gentry, T. PDAs as cognitive aids for people with multiple sclerosis. Am. J. Occup. Ther. 2008, 62, 18–27. [Google Scholar] [CrossRef] [Green Version]
- Goverover, Y.; Chiaravalloti, N.; Genova, H.; DeLuca, J. A randomized controlled trial to treat impaired learning and memory in multiple sclerosis: The self-GEN trial. Mult. Scler. J. 2017, 24, 1096–1104. [Google Scholar] [CrossRef]
- Maitra, K.; Hall, C.; Kalish, T.; Anderson, M.; Dugan, E.; Rehak, J.; Rodríguez, V.; Tamas, J.; Zeitlin, D. Five-year retrospective study of inpatient occupational therapy outcomes for patients with multiple sclerosis. Am. J. Occup. Ther. 2010, 64, 689–694. [Google Scholar] [CrossRef] [Green Version]
- Patti, F.; Ciancio, M.R.; Reggio, E.; Lopes, R.; Palermo, F.; Cacopardo, M.; Reggio, A. The impact of outpatient rehabilitation on quality of life in multiple sclerosis. J. Neurol. 2002, 249, 1027–1033. [Google Scholar] [CrossRef]
- Quinn, É.; Hynes, S. Occupational therapy interventions for multiple sclerosis: A scoping review. Scand. J. Occup. Ther. 2020, 1–16. [Google Scholar] [CrossRef]
- Soofi, A.Y.; Bello-Haas, V.D.; Kho, M.E.; Letts, L. The impact of rehabilitative interventions on quality of life: A qualitative evidence synthesis of personal experiences of individuals with amyotrophic lateral sclerosis. Qual. Life Res. 2018, 27, 845–856. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.S.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions, 2nd ed.; John Wiley & Sons: Chichester, UK, 2019. [Google Scholar]
- Peters, M.; Godfrey, C.; McInerney, P.; Munn, Z.; Trico, A.; Khalil, H. Chapter 11: Scoping Reviews. In JBI Manual for Evidence Synthesis; Aromataris, E., Munn, Z., Eds.; JBI: Miami, FL, USA, 2020. [Google Scholar]
- Tricco, A.; Lillie, E.; Zarin, W.; O’Brien, K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [Green Version]
- Packer, T.; Brink, N.; Sauriol, A. Managing Fatigue: A Six-Week Course for Energy Conservation; Therapy Skill Builders: Tucson, AZ, USA, 1995; ISBN 0761643680. [Google Scholar]
- Vanage, S.M.; Gilbertson, K.K.; Mathiowetz, V. Effects of an energy conservation course on fatigue impact for persons with progressive multiple sclerosis. Am. J. Occup. Ther. 2003, 57, 315–323. [Google Scholar] [CrossRef] [Green Version]
- Mathiowetz, V.; Matuska, K.M.; Murphy, M.E. Efficacy of an energy conservation course for persons with multiple sclerosis. Arch. Phys. Med. Rehabil. 2001, 82, 449–456. [Google Scholar] [CrossRef]
- Lamb, A.L.; Finlayson, M.; Mathiowetz, V.; Chen, H.Y. The outcomes of using self-study modules in energy conservation education for people with multiple sclerosis. Clin. Rehabil. 2005, 19, 475–481. [Google Scholar] [CrossRef]
- Mathiowetz, V.G.; Finlayson, M.L.; Matuska, K.M.; Chen, H.Y.; Luo, P. Randomized controlled trial of an energy conservation course for persons with multiple sclerosis. Mult. Scler. J. 2005, 11, 592–601. [Google Scholar] [CrossRef]
- Finlayson, M.; Preissner, K.; Cho, C.C.; Plow, M. Randomized trial of a teleconference-delivered fatigue management program for people with multiple sclerosis. Mult. Scler. J. 2011, 17, 1130–1140. [Google Scholar] [CrossRef] [PubMed]
- Ghahari, S.; Packer, T.L.; Passmore, A.E. Development, standardisation and pilot testing of an online fatigue self-management program. Disabil. Rehabil. 2009, 31, 1762–1772. [Google Scholar] [CrossRef]
- Sauter, C.; Zebenholzer, K.; Hisakawa, J.; Zeitlhofer, J.; Vass, K. A longitudinal study on effects of a six-week course for energy conservation for multiple sclerosis patients. Mult. Scler. J. 2008, 14, 500–505. [Google Scholar] [CrossRef]
- D’Hooghe, M.B.; Van Gassen, G.; Kos, P.D.; Bouquiaux, O.; Cambron, M.; Decoo, D.; Lysandropoulos, A.; Van Wijmeersch, B.; Willekens, B.; Penner, I.-K.; et al. Improving fatigue in multiple sclerosis by smartphone-supported energy management: The MS TeleCoach feasibility study. Mult. Scler. Relat. Disord. 2018, 22, 90–96. [Google Scholar] [CrossRef] [Green Version]
- Rietberg, M.B.; Van Wegen, E.E.H.; Eyssen, I.C.J.M.; Kwakkel, G.; the MS Study Group. Effects of multidisciplinary rehabilitation on chronic fatigue in multiple sclerosis: A randomized controlled trial. PLoS ONE 2014, 9, e107710. [Google Scholar] [CrossRef]
- Kos, P.D.; Duportail, M.; D’Hooghe, M.B.; Nagels, G.; Kerckhofs, E. Multidisciplinary fatigue management programme in multiple sclerosis: A randomized clinical trial. Mult. Scler. J. 2007, 13, 996–1003. [Google Scholar] [CrossRef] [PubMed]
- Hersche, R.; Weise, A.; Michel, G.; Kesselring, J.; Della Bella, S.; Barbero, M.; Kool, J. Three-week inpatient energy management education (IEME) for persons with multiple sclerosis-related fatigue: Feasibility of a randomized clinical trial. Mult. Scler. Relat. Disord. 2019, 35, 26–33. [Google Scholar] [CrossRef] [PubMed]
- Kos, D.; Duportail, M.; Meirte, J.; Meeus, M.; D’Hooghe, M.; Nagels, G.; Willekens, B.; Meurrens, T.; Ilsbroukx, S.; Nijs, J. The effectiveness of a self-management occupational therapy intervention on activity performance in individuals with multiple sclerosis-related fatigue. Int. J. Rehabil. Res. 2016, 39, 255–262. [Google Scholar] [CrossRef] [Green Version]
- Schettini, F.; Riccio, A.; Mattia, D.; Cincotti, F.; Simione, L.; Liberati, G.; Caruso, M.; Frasca, V.; Calabrese, B.; Mecella, M.; et al. Assistive device with conventional, alternative, and brain-computer interface inputs to enhance interaction with the environment for people with amyotrophic lateral sclerosis: A feasibility and usability study. Arch. Phys. Med. Rehabil. 2015, 96, S46–S53. [Google Scholar] [CrossRef]
- Reilly, S.; Hynes, S. A cognitive occupation-based programme for people with multiple sclerosis: A study to test feasibility and clinical outcomes. Occup. Ther. Int. 2018, 2018, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Chiaravalloti, N.D.; Goverover, Y.; Costa, S.L.; DeLuca, J. A cognitive occupation-based programme for people with multiple sclerosis: A study to test feasibility and clinical outcomes. Front. Neurol. 2018, 9. [Google Scholar] [CrossRef]
- Shevil, E.; Finlayson, M. Pilot study of a cognitive intervention program for persons with multiple sclerosis. Heal. Educ. Res. 2009, 25, 41–53. [Google Scholar] [CrossRef] [Green Version]
- Lamers, I.; Raats, J.; Spaas, J.; Meuleman, M.; Kerkhofs, L.; Schouteden, S.; Feys, P. Intensity-dependent clinical effects of an individualized technology-supported task-oriented upper limb training program in Multiple Sclerosis: A pilot randomized controlled trial. Mult. Scler. Relat. Disord. 2019, 34, 119–127. [Google Scholar] [CrossRef] [PubMed]
- Kamm, C.P.; Mattle, H.P.; Müri, R.M.; Heldner, M.R.; Blatter, V.; Bartlome, S.; Lüthy, J.; Imboden, D.; Pedrazzini, G.; Bohlhalter, S.; et al. Home-based training to improve manual dexterity in patients with multiple sclerosis: A randomized controlled trial. Mult. Scler. J. 2015, 21, 1546–1556. [Google Scholar] [CrossRef]
- Waliño-Paniagua, C.N.; Gómez-Calero, C.; Jiménez-Trujillo, M.I.; Aguirre-Tejedor, L.; Bermejo-Franco, A.; Ortiz-Gutiérrez, R.M.; Cano-De-La-Cuerda, R. Effects of a game-based virtual reality video capture training program plus occupational therapy on manual dexterity in patients with multiple sclerosis: A randomized controlled trial. J. Heal. Eng. 2019, 2019, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kalron, A.; Greenberg-Abrahami, M.; Gelav, S.; Achiron, A. Effects of a new sensory re-education training tool on hand sensibility and manual dexterity in people with multiple sclerosis. Neurorehabilitation 2013, 32, 943–948. [Google Scholar] [CrossRef] [Green Version]
- Bansi, J.; Bloch, W.; Gamper, U.; Riedel, S.; Kesselring, J. Endurance training in MS: Short-term immune responses and their relation to cardiorespiratory fitness, health-related quality of life, and fatigue. J. Neurol. 2013, 260, 2993–3001. [Google Scholar] [CrossRef]
- Ortiz-Gutiérrez, R.; Del Río, F.G.; De La Cuerda, R.C.; Alguacil-Diego, I.M.; González, R.A.; Page, J.C.M. A telerehabilitation program by virtual reality-video games improves balance and postural control in multiple sclerosis patients. Neurorehabilitation 2013, 33, 545–554. [Google Scholar] [CrossRef]
- Bovend’Eerdt, T.J.; Dawes, H.; Sackley, C.; Izadi, H.; Wade, D.; Sackley, C. An integrated motor imagery program to improve functional task performance in neurorehabilitation: A single-blind randomized controlled trial. Arch. Phys. Med. Rehabil. 2010, 91, 939–946. [Google Scholar] [CrossRef] [PubMed]
- Finlayson, M.; Peterson, E.W.; Cho, C. Pilot study of a fall risk management program for middle aged and older adults with MS. Neurorehabilitation 2009, 25, 107–115. [Google Scholar] [CrossRef] [PubMed]
- Yang, F.; Su, X.; Wen, P.-S.; Lazarus, J. Adaptation to repeated gait-slip perturbations among individuals with multiple sclerosis. Mult. Scler. Relat. Disord. 2019, 35, 135–141. [Google Scholar] [CrossRef] [PubMed]
- Fernández, L.G.; Calzada-Sierra, D.J. The importance of multifactorial rehabilitation treatment in amyotrophic lateral sclerosis. Rev. Neurol. 2001, 32, 423–426. [Google Scholar]
- Eyssen, I.C.J.M.; Steultjens, M.; De Groot, V.; Steultjens, E.M.J.; Knol, D.L.; Polman, C.H.; Dekker, J. A cluster randomised controlled trial on the efficacy of client-centred occupational therapy in multiple sclerosis: Good process, poor outcome. Disabil. Rehabil. 2013, 35, 1636–1646. [Google Scholar] [CrossRef]
- Eyssen, I.C.J.M.; Dekker, J.; Groot, V.; Steultjens, E.; Knol, D.; Polman, C.; Steultjens, M. Client-centred therapy in multiple sclerosis: More intensive diagnostic evaluation and less intensive treatment. J. Rehabil. Med. 2014, 46, 527–531. [Google Scholar] [CrossRef] [Green Version]
- Block, P.; Vanner, E.A.; Keys, C.B.; Rimmer, J.H.; Skeels, S.E. Project Shake-It-Up: Using health promotion, capacity building and a disability studies framework to increase self efficacy. Disabil. Rehabil. 2009, 32, 741–754. [Google Scholar] [CrossRef] [PubMed]
- Raglio, A.; Giovanazzi, E.; Pain, D.; Baiardi, P.; Imbriani, C.; Imbriani, M.; Mora, G. Active music therapy approach in amyotrophic lateral sclerosis. Int. J. Rehabil. Res. 2016, 39, 365–367. [Google Scholar] [CrossRef] [PubMed]
- Finlayson, M.; Holberg, C. Evaluation of a teleconference-delivered energy conservation education program for people with multiple sclerosis. Can. J. Occup. Ther. 2007, 74, 337–347. [Google Scholar] [CrossRef]
- D’Amico, E.; Haase, R.; Ziemssen, T. Review: Patient-reported outcomes in multiple sclerosis care. Mult. Scler. Relat. Disord. 2019, 33, 61–66. [Google Scholar] [CrossRef]
- D’Amico, E.; Leone, C.; Hayrettin, T.; Patti, F. Can we define a rehabilitation strategy for cognitive impairment in progressive multiple sclerosis? A critical appraisal. Mult. Scler. J. 2016, 22, 581–589. [Google Scholar] [CrossRef] [PubMed]
- Patti, F.; Leone, C.; D’Amico, E. Treatment options of cognitive impairment in multiple sclerosis. Neurol. Sci. 2010, 31, 265–269. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]

| Database | Strategy |
|---|---|
| Pubmed | “occupational therapy” [All Fields] AND (“methods” [MeSH Terms] OR “methods” [All Fields] OR “intervention” [All Fields]) AND “sclerosis” [All Fields] |
| Scopus | TITLE-ABS-KEY (“occupational therapy” AND intervention AND “sclerosis”) |
| Embase | (‘occupational therapy’/exp OR ‘occupational therapy’) AND (‘intervention’/exp OR intervention) AND (‘sclerosis’/exp OR sclerosis) |
| Web of Science | (“occupational therapy” AND intervention AND sclerosis) |
| Teseo | (“occupational therapy” AND intervention AND sclerosis) |
| Journal of Occupational Rehabilitation | ‘“occupational therapy” AND intervention AND sclerosis’ |
| Physical & Occupational Therapy In Pediatrics | [All: “occupational therapy”] AND [All: intervention] AND [All: sclerosis] AND [in Journal: Physical & Occupational Therapy In Pediatrics] |
| American Journal of Occupational Therapy | “occupational therapy” AND intervention AND sclerosis |
| Occupation, Participation and Health | [All “occupational therapy”] AND [All intervention] AND [All sclerosis] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
De-Bernardi-Ojuel, L.; Torres-Collado, L.; García-de-la-Hera, M. Occupational Therapy Interventions in Adults with Multiple Sclerosis or Amyotrophic Lateral Sclerosis: A Scoping Review. Int. J. Environ. Res. Public Health 2021, 18, 1432. https://doi.org/10.3390/ijerph18041432
De-Bernardi-Ojuel L, Torres-Collado L, García-de-la-Hera M. Occupational Therapy Interventions in Adults with Multiple Sclerosis or Amyotrophic Lateral Sclerosis: A Scoping Review. International Journal of Environmental Research and Public Health. 2021; 18(4):1432. https://doi.org/10.3390/ijerph18041432
Chicago/Turabian StyleDe-Bernardi-Ojuel, Luis, Laura Torres-Collado, and Manuela García-de-la-Hera. 2021. "Occupational Therapy Interventions in Adults with Multiple Sclerosis or Amyotrophic Lateral Sclerosis: A Scoping Review" International Journal of Environmental Research and Public Health 18, no. 4: 1432. https://doi.org/10.3390/ijerph18041432