Transtheoretical Model for Physical Activity in Older Adults: Systematic Review

 ,
,  ,
,  ,
, 
Abstract
:1. Introduction
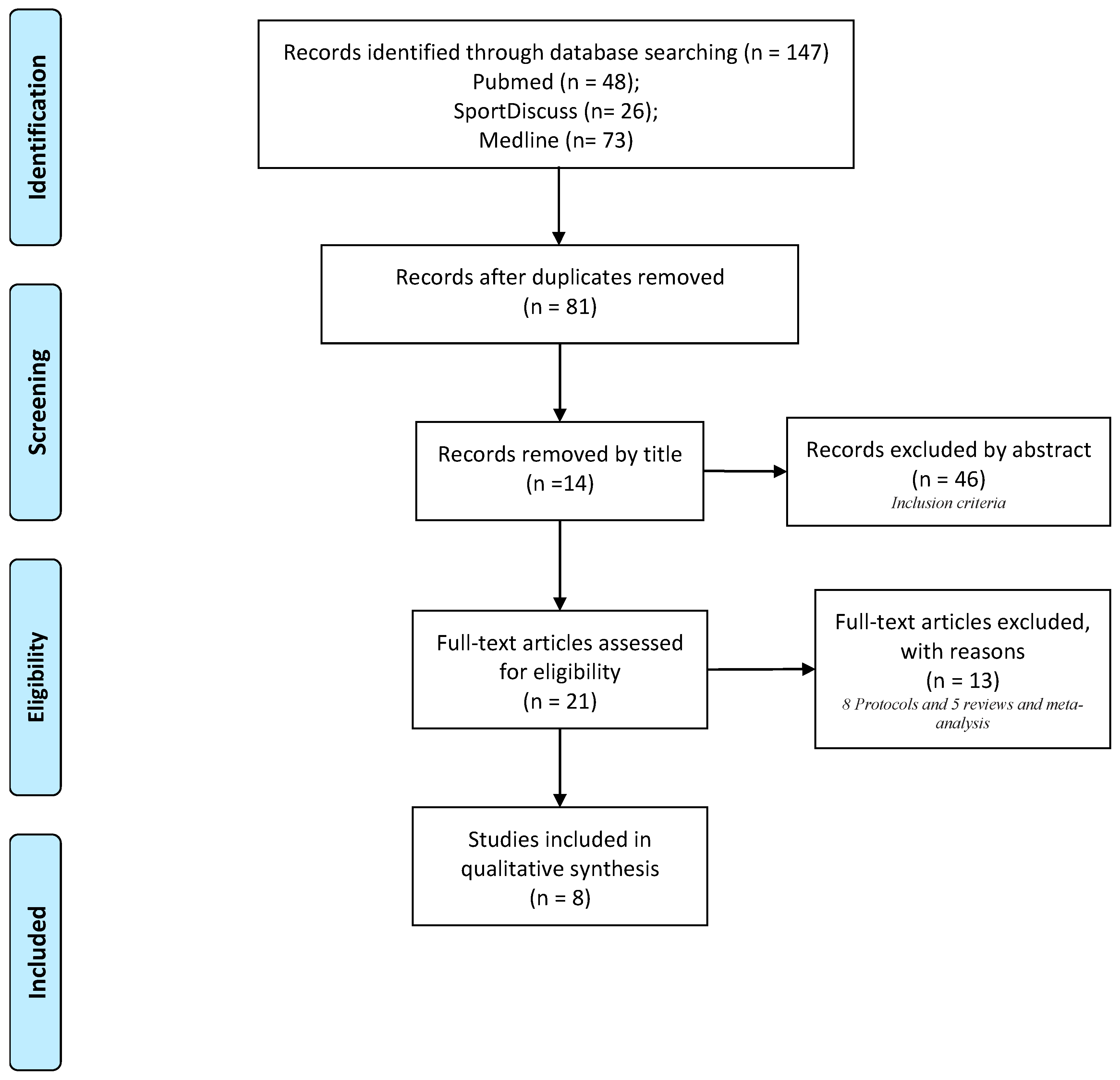
2. Materials and Methods
2.1. Information Sources and Search Strategies
2.2. Study Eligibility Criteria
2.3. Data Items
3. Results/Overview
3.1. Stages of Change (SoC)
3.2. Processes of Change (PC)
3.3. Decisional Balance (DB)
3.4. Self-Efficacy (SE)
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Rhodes, R.E.; Janssen, I.; Bredin, S.S.D.; Warburton, D.E.R.; Bauman, A. Physical activity: Health impact, prevalence, correlates and interventions. Psychol. Health 2017, 32, 942–975. [Google Scholar] [CrossRef] [PubMed]
- Warburton, D.E.; Charlesworth, S.; Ivey, A.; Nettlefold, L.; Bredin, S.S. A systematic review of the evidence for Canada’s Physical Activity Guidelines for Adults. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paterson, D.H.; Warburton, D.E. Physical activity and functional limitations in older adults: A systematic review related to Canada’s Physical Activity Guidelines. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kesaniemi, A.; Riddoch, C.J.; Reeder, B.; Blair, S.N.; Sorensen, T. Advancing the future of physical activity guidelines in Canada: An independent expert panel interpretation of the evidence. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Warburton, D.E.R.; Bredin, S.S.D. Health benefits of physical activity: A systematic review of current systematic reviews. Curr. Opin. Cardiol. 2017, 32, 541–556. [Google Scholar] [CrossRef] [PubMed]
- Amireault, S.; Baier, J.M.; Spencer, J.R. Physical Activity Preferences Among Older Adults: A Systematic Review. J. Aging Phys. Act. 2018, 1–12. [Google Scholar] [CrossRef]
- Forte, G.; Favieri, F.; Casagrande, M. Heart Rate Variability and Cognitive Function: A Systematic Review. Front. Neurosci. 2019, 13, 710. [Google Scholar] [CrossRef]
- Sodergren, M. Lifestyle predictors of healthy ageing in men. Maturitas 2013, 75, 113–117. [Google Scholar] [CrossRef]
- World Health Organization. WHO Guidelines Approved by the Guidelines Review Committee. In Global Recommendations on Physical Activity for Health; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Bauman, A.; Merom, D.; Bull, F.C.; Buchner, D.M.; Fiatarone Singh, M.A. Updating the Evidence for Physical Activity: Summative Reviews of the Epidemiological Evidence, Prevalence, and Interventions to Promote “Active Aging”. Gerontologist 2016, 56 (Suppl. 2), S268–S280. [Google Scholar] [CrossRef]
- Sparling, P.B.; Howard, B.J.; Dunstan, D.W.; Owen, N. Recommendations for physical activity in older adults. BMJ Br. Med. J. 2015, 350, h100. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Global Strategy on Diet, Physical Activity and Health. Available online: https://www.who.int/dietphysicalactivity/pa/en/ (accessed on 20 February 2020).
- Findorff, M.J.; Wyman, J.F.; Gross, C.R. Predictors of long-term exercise adherence in a community-based sample of older women. J. Womens Health 2009, 18, 1769–1776. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Picorelli, A.M.; Pereira, L.S.; Pereira, D.S.; Felicio, D.; Sherrington, C. Adherence to exercise programs for older people is influenced by program characteristics and personal factors: A systematic review. J. Physiother. 2014, 60, 151–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stralen, M.; de Vries, H.; Mudde, A.; Bolman, C.; Lechner, L. Determinants of initiation and maintenance of physical activity among older adults: A literature review. Health Psychol. Rev. 2009, 3, 147–207. [Google Scholar] [CrossRef]
- Chase, J.A. Interventions to Increase Physical Activity Among Older Adults: A Meta-Analysis. Gerontologist 2015, 55, 706–718. [Google Scholar] [CrossRef] [Green Version]
- Gourlan, M.; Bernard, P.; Bortolon, C.; Romain, A.J.; Lareyre, O.; Carayol, M.; Ninot, G.; Boiché, J. Efficacy of theory-based interventions to promote physical activity. A meta-analysis of randomised controlled trials. Health Psychol. Rev. 2016, 10, 50–66. [Google Scholar] [CrossRef]
- Prochaska, J.O.; DiClemente, C.C. Stages and processes of self-change of smoking: Toward an integrative model of change. J. Consult. Clin. Psychol. 1983, 51, 390–395. [Google Scholar] [CrossRef]
- Spencer, L.; Adams, T.B.; Malone, S.; Roy, L.; Yost, E. Applying the transtheoretical model to exercise: A systematic and comprehensive review of the literature. Health Promot. Pract. 2006, 7, 428–443. [Google Scholar] [CrossRef]
- Lindahl, J.; Stenling, A.; Lindwall, M.; Colliander, C. Trends and knowledge base in sport and exercise psychology research: A bibliometric review study. Int. Rev. Sport Exerc. Psychol. 2015, 8, 71–94. [Google Scholar] [CrossRef]
- Prochaska, J.O.; Redding, C.A.; Evers, K.E. The transtheoretical model and stages of change. In Health Behavior: Theory, Research, and Practice; Jossey-Bass: San Francisco, CA, USA, 2015. [Google Scholar]
- Marcus, B.H.; Forsyth, L.H. Motivating People to Be Physically Active; Human Kinetics: Champaign, IL, USA, 2008. [Google Scholar]
- Marcus, B.H.; Dubbert, P.M.; Forsyth, L.H.; McKenzie, T.L.; Stone, E.J.; Dunn, A.L.; Blair, S.N. Physical activity behavior change: Issues in adoption and maintenance. Health Psychol. 2000, 19, 32–41. [Google Scholar] [CrossRef]
- Bunton, R.; Baldwin, S.; Flynn, D.; Whitelaw, S. The ‘stages of change’ model in health promotion: Science and Ideology. Crit. Public Health 2000, 10, 55–70. [Google Scholar] [CrossRef]
- Marshall, S.J.; Biddle, S.J. The transtheoretical model of behavior change: A meta-analysis of applications to physical activity and exercise. Ann. Behav. Med. 2001, 23, 229–246. [Google Scholar] [CrossRef] [PubMed]
- Ntoumanis, N.; Thørgersen-Ntoumani, C.; Quested, E.; Chatzisarantis, N. Theoretical Approaches to Physical Activity Promotion; Oxford University Press: Oxford, UK, 2018. [Google Scholar]
- Romain, A.J.; Caudroit, J.; Hokayem, M.; Bernard, P. Is there something beyond stages of change in the transtheoretical model? The state of art for physical activity. Can. J. Behav. Sci. Rev. Can. Sci. Comport. 2018, 50, 42–53. [Google Scholar] [CrossRef]
- Romain, A.J.; Bortolon, C.; Gourlan, M.; Carayol, M.; Decker, E.; Lareyre, O.; Ninot, G.; Boiché, J.; Bernard, P. Matched or nonmatched interventions based on the transtheoretical model to promote physical activity. A meta-analysis of randomized controlled trials. J. Sport Health Sci. 2018, 7, 50–57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Janis, I.L.; Mann, L. Decision Making: A Psychological Analysis of Conflict, Choice, and Commitment; Free Press: New York, NY, USA, 1977. [Google Scholar]
- Marcus, B.H.; Owen, N. Motivational Readiness, Self-Efficacy and Decision-Making for Exercise1. J. Appl. Soc. Psychol. 1992, 22, 3–16. [Google Scholar] [CrossRef] [Green Version]
- Bandura, A. Social Foundations of Thought and Action; Prentice Hall: Englewood Cliffs, NJ, USA, 1986; Volume 1986. [Google Scholar]
- Notthoff, N.; Reisch, P.; Gerstorf, D. Individual Characteristics and Physical Activity in Older Adults: A Systematic Review. Gerontology 2017, 63, 443–459. [Google Scholar] [CrossRef] [Green Version]
- French, D.P.; Olander, E.K.; Chisholm, A.; Mc Sharry, J. Which Behaviour Change Techniques Are Most Effective at Increasing Older Adults’ Self-Efficacy and Physical Activity Behaviour? A Systematic Review. Ann. Behav. Med. 2014, 48, 225–234. [Google Scholar] [CrossRef] [Green Version]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. PLoS Med. 2007, 4, e296. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. 10 Facts on Ageing and Health. Available online: https://www.who.int/features/factfiles/ageing/en/ (accessed on 20 February 2020).
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [Green Version]
- Bradley, J.M.; Wilson, J.J.; Hayes, K.; Kent, L.; McDonough, S.; Tully, M.A.; Bradbury, I.; Kirk, A.; Cosgrove, D.; Convery, R.; et al. Sedentary behaviour and physical activity in bronchiectasis: A cross-sectional study. BMC Pulm. Med. 2015, 15, 61. [Google Scholar] [CrossRef] [Green Version]
- Abbaspour, S.; Farmanbar, R.; Njafi, F.; Ghiasvand, A.M.; Dehghankar, L. Decisional balance and self-efficacy of physical activity among the elderly in Rasht in 2013 based on the transtheoretical model. Electron. Phys. 2017, 9, 4447–4453. [Google Scholar] [CrossRef] [Green Version]
- Koo, K.M.; Park, C.H.; Kim, C.J. Development of strategies for changing in physical activity behaviors on older adults with disabilities. J. Exerc. Rehabil. 2017, 13, 676–683. [Google Scholar] [CrossRef] [PubMed]
- Guicciardi, M.; Lecis, R.; Anziani, C.; Corgiolu, L.; Porru, A.; Pusceddu, M.; Spanu, F. Type 2 diabetes mellitus, physical activity, exercise self-efficacy, and body satisfaction. An application of the transtheoretical model in older adults. Health Psychol. Behav. Med. 2014, 2, 748–758. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilson, J.J.; Kirk, A.; Hayes, K.; Bradbury, I.; McDonough, S.; Tully, M.A.; O’Neill, B.; Bradley, J.M. Applying the Transtheoretical Model to Physical Activity Behavior in Individuals With Non-Cystic Fibrosis Bronchiectasis. Respir. Care 2016, 61, 68–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, H.Y.; Lin, Y.S.; Chuang, Y.C.; Lin, W.H.; Kuo, L.Y.; Chen, J.C.; Hsu, C.L.; Chen, B.Y.; Tsai, H.Y.; Cheng, F.H.; et al. Application of the Transtheoretical Model to Exercise Behavior and Physical Activity in Patients after Open Heart Surgery. Acta Cardiol. Sin. 2015, 31, 202–208. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.J.; Chen, K.M.; Chen, M.D.; Wu, H.C.; Chang, W.J.; Wang, Y.C.; Huang, H.T. Applying the transtheoretical model to promote functional fitness of community older adults participating in elastic band exercises. J. Adv. Nurs. 2015, 71, 2338–2349. [Google Scholar] [CrossRef] [PubMed]
- Harada, K.; Shibata, A.; Lee, E.; Oka, K.; Nakamura, Y. Associations between perceived health benefits and barriers to strength training, and stages of change for strength-training behavior among older Japanese adults. J. Phys. Act. Health 2014, 11, 801–809. [Google Scholar] [CrossRef]
- Franco, M.R.; Tong, A.; Howard, K.; Sherrington, C.; Ferreira, P.H.; Pinto, R.Z.; Ferreira, M.L. Older people’s perspectives on participation in physical activity: A systematic review and thematic synthesis of qualitative literature. Br. J. Sports Med. 2015, 49, 1268–1276. [Google Scholar] [CrossRef]
- De Menezes, M.C.; Bedeschi, L.B.; Santos, L.C.; Lopes, A.C. Interventions directed at eating habits and physical activity using the Transtheoretical Model: A systematic review. Nutr. Hosp. 2016, 33, 586. [Google Scholar] [CrossRef] [Green Version]
- Lewis, B.A.; Marcus, B.H.; Pate, R.R.; Dunn, A.L. Psychosocial mediators of physical activity behavior among adults and children. Am. J. Prev. Med. 2002, 23, 26–35. [Google Scholar] [CrossRef]
- Rhodes, R.E.; Dickau, L. Moderators of the intention-behaviour relationship in the physical activity domain: A systematic review. Br. J. Sports Med. 2013, 47, 215. [Google Scholar] [CrossRef]
- Clark, P.G.; Riebe, D.; Blissmer, B.J.; Lees, F.D.; Greaney, M.L. Psychosocial Factors Associated With Physical Activity in Older Adults. Annu. Rev. Gerontol. Geriatr. 2016, 36, 273–291. [Google Scholar] [CrossRef]


{kind=link}
| TTM Construct | Description |
|---|---|
| Stages of change | |
| Precontemplation | Inactive. No intention to engage in regular PA in the next 6 months. |
| Contemplation | Inactive but intend to engage in regular PA in the next 6 months. |
| Preparation | Started to commitment to engage in regular PA. |
| Action | Established engagement in regular PA but have done so for less than 6 months. |
| Maintenance | Maintained engagement of regular PA for longer than 6 months. |
| Process of change | |
| Cognitive Processes of change | |
| Consciousness raising (CR) | Increasing knowledge about benefits of PA. |
| Dramatic relief (DR) | Awareness of health risk of lack PA. |
| Environmental re-evaluation (ER) | Analyze how the physical inactivity affects to your interpersonal relationships. |
| Self-reevaluation (SR) | Recognize the benefits of being physically active. |
| Social liberation (SL) | Show different ways to be active. |
| Behavioral processes of change | |
| Counter conditioning (CC) | Change inactive habits for healthy actions. |
| Helping relationship (HR) | Search social support in sports practice to facilitate change. |
| Reinforcement management (RM) | Reward yourself for being physically active. |
| Self-liberation (SeL) | Create commitment to be active and plan activities. |
| Stimulus control (SC) | Use of stimulus to maintain PA levels. |
| Decisional Balance | |
| Pros | Perceived benefits of engaging in regular PA. |
| Cons | Perceived barriers of engaging in regular PA. |
| Self-Efficacy | Confidence in one’s ability to perform specific behaviors (regular PA) in specific situations (Tired, in bad mood, do have not time, on vacation and bad weather). |
| Reference | Transtheoretical Model Constructs | |||
|---|---|---|---|---|
| Stages of Change | Processes of Change | Decisional Balance | Self-Efficacy | |
| Bradley, J.M., et al. (2015) [37] | x | x | x | x |
| Abbaspour, S., et al. (2017) [38] | x | x | x | |
| Koo, K.M., Park, C.H., and Kim, C.J. (2017) [39] | x | x | ||
| Guicciardi, M., et al. (2014) [40] | x | x | ||
| Wilson, J.J., et al. (2016) [41] | x | x | x | x |
| Huang, H. Y., et al. (2015) [42] | x | |||
| Yang, H.J., et al. (2015) [43] | x | |||
| Harada, K., et al. (2014) [44]. | x | |||
| Reference | Journal | Country Territory | Study Periods | Study Population | Study Design | Aims | Important Findings |
|---|---|---|---|---|---|---|---|
| Bradley, J.M., et al. (2015) [37] | BMC Pulmonary Medicine | Ireland | N: 55 Age: 63 ± 10 Gender: 22 male (40%) 33 female (60%) Pathology: Bronchiectasis | Descriptive cross-sectional study | Aim: Explore the patterns and correlates of sedentary behavior and PA in bronchiectasis. |
| |
| Abbaspour, S., Farmanbar, R., Njafi, F., Ghiasvand, A.M., and Dehghankar, L. (2017) [38] | Electronic Physician | Iran | 2013 | N: 262 Age: 64.95 ± 5.03 Gender: 141 male (53.8%) 121 female (46.2%) Pathology: No specific. | Descriptive cross-sectional study | Aim: To identify the relationship between DB and SE in physical activities using the TTM in the members of a retirement center. |
|
| Koo, K.M., Park, C.H. and Kim, C.J. (2017) [39] | Journal of Exercise Rehabilitation | Korea | 2014 | N: 81 Age: >60 years Gender: 43 male (53%) 38 female (47%) Pathology: Physical disability or brain injury | Descriptive cross-sectional study | Aim: To develop strategies for promoting PA for the disabled older adults who were in the TTM of precontemplation, contemplation, and preparation stages about participating physical activities for promoting healthy life-styles. |
|
| Guicciardi, M., Lecis, R., Anziani, C., Corgiolu, L., Porru, A., Pusceddu, M. and Spanu, F. (2014) [40] | Health Psychology and Behavioral Medicine | Italy | N: 308 Age: 65.24 ± 8.31 years Gender: 172 male (56%) 136 female (44%) Pathology: Type II Diabetes | Descriptive cross-sectional study | Aim: To investigate the relationships between self-reported PA and exercise SE and body satisfaction in a sample of older adults with Type 2 diabetes classified in different Soc. |
| |
| Wilson, J.J., Kirk, A., Hayes, K., Bradbury, I., McDonough, S., Tully, M.A., et al. (2016) [41] | Respiratory Care | Ireland | N: 55 Age: 63 ± 10 Gender: 22 male (40%) 33 female (60%) Pathology: Non-cystic fibrosis bronchiectasis | Descriptive cross-sectional study | Aim: To examine patterns of (1) PA and (2) mediators of behavior change (SE, DB, and PC) across SoC in individuals with non-cystic fibrosis bronchiectasis. |
| |
| Huang, H.Y., et al. (2015) [42] | Acta Cardiologica Sinica | Taiwan | 2010–2011 | N: 130 Age: 61.0 ± 12.2 years Gender: 92 male (70.8%) 38 female (29.2%) Pathology: Patients after Open Heart Surgery | Design: Prospective cohort study Duration: 6 months. | Aim: To assess exercise behavior and PA levels using TTM in patients undergoing open heart surgery. |
|
| Yang, H.J., Chen, K.M., Chen, M.D., Wu, H.C., Chang, W.J., Wang, Y.C. and Huang, H.T. (2015) [43] | Journal of Advanced Nursing | Taiwan | 2011 | N: 169 Age: 71.28 ± 5.54 years Gender: 54 male (32%) 115 female (68%) Arms: Control (n = 85) Intervention (n = 84) Pathology: No specific | Design: Quasi-experimental design Duration: 6 months. | Aim: To test the effects of the group SEB exercises on the functional fitness of community older adults in the contemplation and preparation SoC |
|
| Harada, K., Shibata, A., Lee, E., Oka, K. and Nakamura, Y. (2014) [44] | Journal of Physical Activity and Health | Japan | 2009 | N: 1244 Age: 60–74 years Gender: 638 male (51.5%), 600 female (48.5%) Pathology: No specific. | Design: cross-sectional study | Aim: Examined the associations among the perceived health benefits of strength training, perceived barriers to strength straining, and SoC for strength-training behavior. |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jiménez-Zazo, F.; Romero-Blanco, C.; Castro-Lemus, N.; Dorado-Suárez, A.; Aznar, S. Transtheoretical Model for Physical Activity in Older Adults: Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 9262. https://doi.org/10.3390/ijerph17249262
Jiménez-Zazo F, Romero-Blanco C, Castro-Lemus N, Dorado-Suárez A, Aznar S. Transtheoretical Model for Physical Activity in Older Adults: Systematic Review. International Journal of Environmental Research and Public Health. 2020; 17(24):9262. https://doi.org/10.3390/ijerph17249262
Chicago/Turabian StyleJiménez-Zazo, Fabio, Cristina Romero-Blanco, Nuria Castro-Lemus, Alberto Dorado-Suárez, and Susana Aznar. 2020. "Transtheoretical Model for Physical Activity in Older Adults: Systematic Review" International Journal of Environmental Research and Public Health 17, no. 24: 9262. https://doi.org/10.3390/ijerph17249262