Strategies for Delivering Mental Health Services in Response to Global Climate Change: A Narrative Review


Abstract
:1. Introduction
Aims
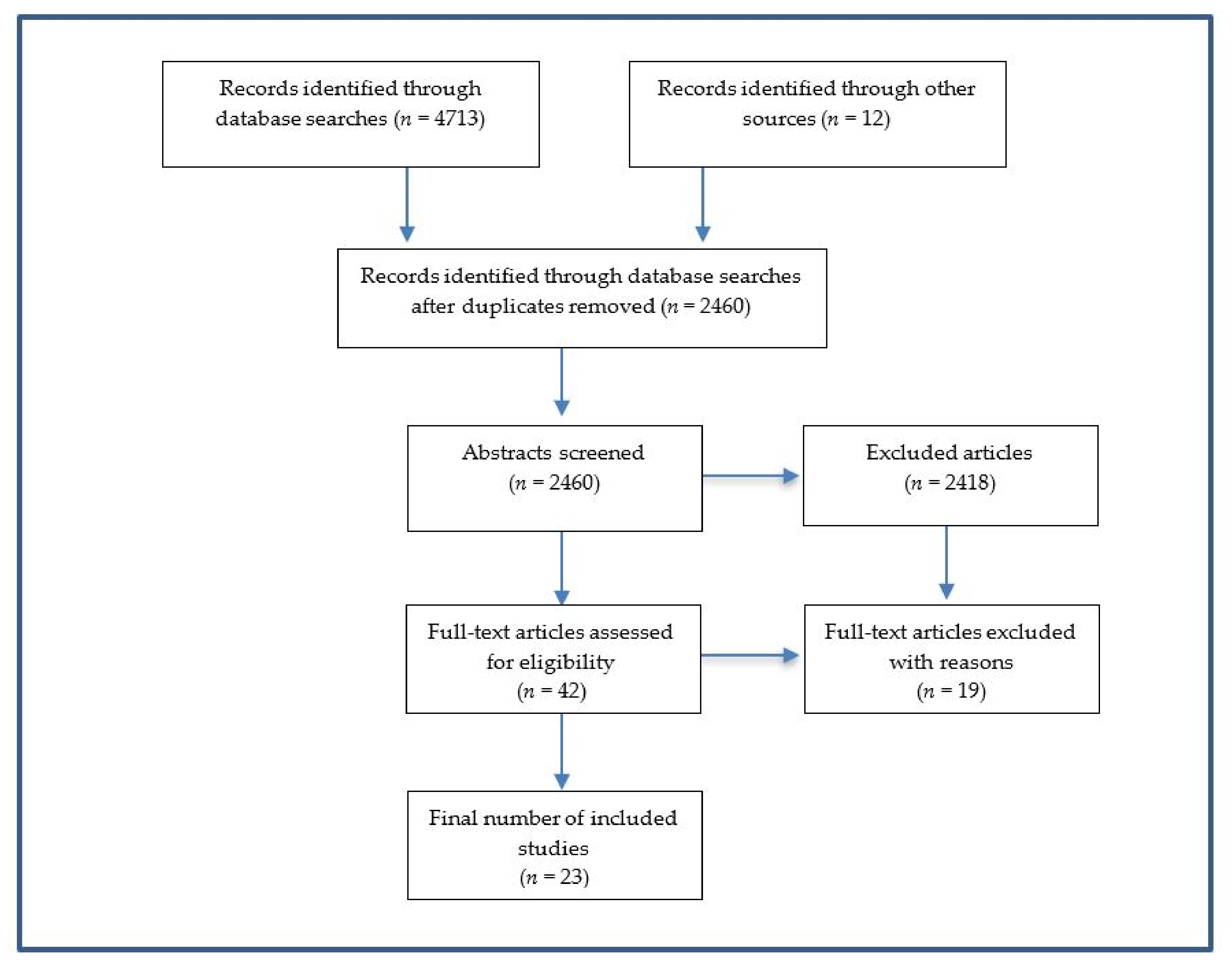
2. Methods
2.1. Eligibility Criteria
2.2. Data Collection
2.3. Ratings of Scientific Evidence
- Multiple site replication and follow-up: At least two rigorous randomized controlled trials (RCTs) with nonoverlapping analytic samples that were carried out in usual care or practice settings have found the program to be superior to an appropriate comparison program on outcomes specified in the criteria for that particular topic area. In at least one of these RCTs, the program has shown to have a sustained effect at least one year beyond the end of treatment, when compared to a control group. The RCTs have been reported in published, peer-reviewed literature;
- Outcome measures must be reliable and valid, and administered consistently and accurately across all subjects;
- The overall weight of the published, peer-reviewed research evidence supports the benefit of the program for the outcomes specified in the criteria for that particular topic area.
- There is no case data suggesting a risk of harm that: (a) was probably caused by the program and (b) was severe or frequent;
- There is no legal or empirical basis suggesting that, compared to its likely benefits, the program constitutes a risk of harm to those receiving it;
- The program has a book, manual, and/or other available writings that specify components of the service and describe how to administer it.
3. Results
3.1. Mental Health Services for Acute Events
3.2. Guideline and Intervention Development and Implementation
3.3. Development and Training of Disaster Responders
- Tier 1: General training in core knowledge, attitudes, and skills (required by all responders and professionals who work in the context of disasters and major incidents);
- Tier 2: More advanced training for those who deliver psychological first aid, basic psychological therapies, and assessment of people who may require more specialized mental healthcare;
- Tier 3: Specialist training required by staff who deliver the functions of Levels 3 and 4 in the model of care in which a personal approach to particular people’s needs is based on the assessment of their needs. This includes training to supervise staff whose work includes delivering psychosocial care at Levels 1 and 2 in a stepped care model;
- Tier 4: Advanced specialist training for professionals who are appointed to provide advice to major incident response commanders at strategic, operational, and tactical levels. These appointments require not only disaster-related training in psychosocial and mental healthcare but also training in major incident management, consultative skills, and selected aspects of strategic leadership and management (pp. 1–109, [33]).
3.4. Needs Assessments
3.5. Mental Health Services for Sub-Acute Events
3.6. Mental Health Services for Long-Lasting Events
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Berry, H.L.; Bowen, K.; Kjellstrom, T. Climate Change and Mental Health: A Causal Pathways Framework. Int. J. Public Health 2010, 55, 123–132. [Google Scholar] [CrossRef] [PubMed]
- Palinkas, L.A.; Wong, M. Global Climate Change and Mental Health. Curr. Opin. Psychol. 2020, 32, 12–16. [Google Scholar] [CrossRef]
- Bourque, F.; Cunsolo Willox, A. Climate Change: The Next Great Challenge for Public Mental Health? Int. Rev. Psychiatry 2014, 26, 415–422. [Google Scholar] [CrossRef] [PubMed]
- Clayton, S.; Manning, C.; Hodge, C. Beyond Storms and Droughts: The Psychological Impacts of Climate Change; American Psychological Association and ecoAmerica: Washington, DC, USA, 2014. [Google Scholar]
- Dodgen, D.; Donato, D.; Kelly, N.; La Greca, A.M.; Morganstein, J.; Reser, J.P.; Ruzek, J.; Schweitzer, S.; Shimamoto, M.M.; Tart, K.T.; et al. Chapter 8. Mental health and well-being. In The Impacts of Climate Change on Human Health in the United States: A Scientific Assessment; Balbus, A.J., Gamble, J.L., Beard, C.B., Bell, J.E., Dodgen, D., Eisen, R.J., Fann, N., Hawkins, M.D., Herring, S.C., Eds.; U.S. Global Change Research Program: Washington, DC, USA, 2016; pp. 217–246. Available online: http://dx.doi.org/10.7930/J0TX3C9H (accessed on 5 May 2019).
- Doherty, T.J.; Clayton, S. The Psychological Impacts of Global Climate Change. Am. Psychol. 2011, 66, 265–276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fritze, J.; Blashki, G.; Burke, S.; Wiseman, J. Hope, Despair and Transformation: Climate Change and Promotion of Mental Health and Wellbeing. Int. J. Ment. Health Syst. 2008, 2, 13. [Google Scholar] [CrossRef] [Green Version]
- Galea, S.; Brewin, C.R.; Gruber, M.; Jones, R.T.; King, D.W.; King, L.A.; McNally, R.J.; Ursano, R.J.; Petukhova, M.; Kessler, R.C. Exposure to Hurricane Related Stressors and Mental Illness after Hurricane Katrina. Arch. Gen. Psychiatry 2007, 64, 1427–1434. [Google Scholar] [CrossRef]
- Obradovich, N.; Migliorini, R.; Paulus, M.P.; Rahwan, I. Empirical Evidence of Mental Health Risks Posed by Climate Change. Proc. Natl. Acad. Sci. USA 2018, 115, 10953–10958. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayes, K.; Blashki, G.; Wiseman, J.; Burke, S.; Reifels, L. Climate Change and Mental Health: Risks, Impacts and Priority Actions. Int. J. Ment. Health Sys. 2018, 12, 28. [Google Scholar] [CrossRef]
- Trombley, J.; Chalupka, S.; Anderko, L. Climate Change and Mental Health. Am. J. Nurs. 2017, 117, 44–52. [Google Scholar] [CrossRef]
- Orengo-Aguayo, R.; Stewart, R.W.; de Arellano, M.A.; Suarez-Kindy, J.L.; Young, J. Disaster Exposure and Mental Health Among Puerto Rican Youths after Hurricane Maria. JAMA Netw. Open 2019, 2, e192619. [Google Scholar] [CrossRef] [Green Version]
- Nahar, N.; Blomstedt, Y.; Wu, B.; Kandarina, I.; Trisnantoro, L.; Kinsman, J. Increasing the Provision of Mental Health Care for Vulnerable, Disaster-Affected People in Bangladesh. BMC Public Health 2014, 14, 708. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernandez, A.; Black, J.; Jones, M.; Wilson, L.; Salvador-Carulla, L.; Astell-Burt, T.; Black, D. Flooding and Mental Health: A Systematic Mapping Review. PLoS ONE 2015, 10, e0119929. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bryant, R.; Waters, E.; Gibbs, L.; Pattison, P.; Lusher, D.; MacDougall, C.; Harms, L.; Block, K.; Sinnott, V.; Ireton, G.; et al. Psychological Outcomes Following the Victorian Black Saturday Bushfires. Aust. N. Z. J. Psychiatry 2014, 48, 634–643. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Basu, R.; Gavin, L.; Pearson, D.; Ebisu, K.; Malig, B. Examining the Association Between Apparent Temperature and Mental Health-Related Emergency Room Visits in California. Am. J. Epidemiol. 2018, 187, 726–735. [Google Scholar] [CrossRef] [Green Version]
- Schmeltz, M.T.; Gamble, J.L. Risk Characterization of Hospitalizations for Mental Illness and/or Behavioral Disorders with Concurrent Heat-Related Illness. PLoS ONE 2017, 12, e0186509. [Google Scholar] [CrossRef]
- Hanigan, I.C.; Butler, C.D.; Kokic, P.N.; Hutchinson, M.F. Suicide and Drought in New South Wales, Australia, 1970–2007. Proc. Natl. Acad. Sci. USA 2012, 109, 13950–13955. [Google Scholar] [CrossRef] [Green Version]
- Vins, H.; Bell, J.; Saha, S.; Hess, J.J. The Mental Health Outcomes of Drought: A Systematic Review and Causal Process Diagram. Int. J. Environ. Res. Public Health 2015, 12, 13251–13275. [Google Scholar] [CrossRef] [Green Version]
- Thompson, R.; Hornigold, R.; Page, L.; Waite, T. Associations between High Ambient Temperatures and Heat Waves with Mental Health Outcomes: A Systematic Review. Public Health 2018, 61, 171–191. [Google Scholar] [CrossRef]
- Burke, M.B.; Hsiang, S.; Miguel, E. Global Non-Linear Effect of Temperature on Economic Production. Nature 2015, 527, 225–235. [Google Scholar] [CrossRef]
- Shultz, J.M.; Rechkemmer, A.; Rai, A.; McManus, K.T. Public Health and Mental health Implications of environmentally induced forced migration. Dis. Med. Public Health Prep. 2019, 13, 116–122. [Google Scholar] [CrossRef] [Green Version]
- Gleick, P.H. Water, Drought, Climate Change, and Conflict in Syria. Weather Clim. Soc. 2014, 6, 331–340. [Google Scholar] [CrossRef]
- Hsiang, S.M.; Meng, K.C.; Cane, M.A. Civil Conflicts are Associated with Global Climate. Nature 2011, 476, 438–440. [Google Scholar] [CrossRef] [PubMed]
- Levy, B.S.; Sidel, V.W.; Patz, J. Climate Change and Collective Violence. Annu. Rev. Public Health 2017, 38, 241–257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fuller, T.; Flavelle, C. A Climate Reckoning in Wildfire-Stricken California. New York Times. 10 September 2020, p. A1. Available online: https://www.nytimes.com/2020/09/10/us/climate-change-california-wildfires.html?action=click&module=Well&pgtype=Homepage§ion=Climate%20and%20Environment (accessed on 16 September 2020).
- Warzel, C. I Need You to Care that our Country is on Fire. New York Times. 9 September 2020, p. A23. Available online: https://www.nytimes.com/2020/09/09/opinion/california-fires.html (accessed on 16 September 2020).
- Institute of Medicine. Reducing Risks for Mental Disorders: Frontiers for Preventive Intervention Research; The National Academies Press: Washington, DC, USA, 1994. [Google Scholar] [CrossRef]
- Ferreri, R. Writing Narrative Style Literature Reviews. Med. Writ. 2015, 24, 230–235. [Google Scholar] [CrossRef]
- World Health Organization Regional Office for South-East Asia. Framework for Mental Health and Psychosocial Support after Tsunami; WHO: New Delhi, India, 2005; Available online: http://www/searo.who.int/entity/emergencies/documents/sea_earthquake_and_tsunami_framewor.pdf?ua=1 (accessed on 5 May 2019).
- Inter-Agency Standing Committee (IASC). IASC Guidelines on Mental Health and Psychosocial Support in Emergency Settings; IASC: Geneva, Switzerland, 2007; Available online: https://www.who.int/mental_health/emergencies/guidelines_iasc_mental_health_psychosocial_june_2007.pdf (accessed on 6 May 2019).
- United Nations Office for Disaster Risk Reduction. Sendai Framework for Disaster Risk Reduction 2015–2030. 2015. Available online: https://www.undrr.org/publication/sendai-framework-disaster-risk-reduction-2015-2030 (accessed on 3 November 2020).
- NATO Joint Medical Committee (NATO). Psychosocial Care for People Affected by Disaster and Major Incidents: A Model for Designing, Delivering and Managing Psychosocial Services for People Involved in Major Incidents, Conflict, Disasters and Terrorism; NATO: Brussels, Belgium, 2008; Available online: https://www.coe.int/t/dg4/majorhazards/ressources/virtuallibrary/materials/Others/NATO_Guidance_Psychosocial_Care_for_People_Affected_by_Disasters_and_Major_Incidents.pdf (accessed on 5 August 2020).
- California Evidence-Based Clearing House for Child Welfare. Scientific Rating Scales. Updated 13 May 2019. Available online: https://www.cebc4cw.org/ratings/scientific-rating-scale/ (accessed on 3 November 2020).
- Albrecht, G. Chronic Environmental Change: Emerging ‘Psychoterratic’ Syndromes. In Climate Change and Human Well-Being: Global Challenges and Opportunities; Weissbecker, I., Ed.; Springer: New York, NY, USA, 2011; pp. 43–56. [Google Scholar]
- Clayton, S. Climate Anxiety: Psychological Responses to Climate Change. J. Anxiety Disord. 2020, 74, 102263. [Google Scholar] [CrossRef]
- Palinkas, L.A.; Wong, M. Social Sustainability and Global Climate Change: A New Challenge for Social work. In Social Work and Sustainability in Asia: Facing the Challenges of Global Environmental Changes; Chong, A., Chi, I., Eds.; Routledge: London, UK, 2019; pp. 33–47. [Google Scholar]
- United Nations Department of Economic and Social Affairs. Transforming Our World: The 2030 Agenda for Sustainable Development. 2015. Available online: https://sustainabledevelopment.un.org/content/documents/21252030%20Agenda%20for%20Sustainable%20Development%20web.pdf (accessed on 3 November 2020).
- United Nations. United Nations Framework Convention on Climate Change (UNFCCC or Paris Agreement). 2015. Available online: https://unfccc.int/files/essential_background/convention/application/pdf/english_paris_agreement.pdf (accessed on 3 November 2020).
- Bisson, J.I.; Tavakoly, B.; Witteveen, A.B.; Ajdukovic, D.; Jehel, L.; Johansen, V.J.; Nordanger, D.; Garcia, F.O.; Punamaki, R.L.; Schnyder, U.; et al. TENTS Guidelines: Development of Post-Disaster Psychosocial Care Guidelines Though a Delphi Process. Br. J. Psychiatry 2010, 196, 69–74. [Google Scholar] [CrossRef]
- Cohen, G.H.; Tamraker, S.; Lowe, S.; Sampson, L.; Ettman, C.; Linas, B.; Ruggiero, K.; Galea, S. Comparison of Simulated Treatment and Cost-Effectiveness of a Stepped Care Case-Finding Intervention vs Usual Care for Posttraumatic Stress Disorder After a Natural Disaster. JAMA Psychiatry 2017, 74, 1251–1258. [Google Scholar] [CrossRef]
- World Health Organization (WHO). mhGAP Intervention Guide for Mental, Neurological and Substance Use Disorders in Non-Specialized Health Settings, Version 2.0; World Health Organization: Geneva, Switzerland, 2016; Available online: https://www.who.int/publications/i/item/mhgap-intervention-guide---version-2.0 (accessed on 5 May 2019).
- Van Ginneken, N.; Tharyan, P.; Lewin, S.; Rao, G.N.; Meera, S.M.; Pian, J.; Chandrashekar, S.; Patel, V. Non-Specialist Health Worker Interventions for the Care of Mental, Neurological and Substance-Abuse Disorders in Low- and Middle-Income Countries. Cochrane Database Syst. Rev. 2013, 19, CD009149. [Google Scholar] [CrossRef] [Green Version]
- Weaver, A.; Lapidos, A. Mental Health Interventions with Community Health Workers in the United States: A Systematic Review. J. Health Care Poor Underserved 2018, 29, 159–180. [Google Scholar] [CrossRef]
- Hoeft, T.J.; Fortney, J.C.; Patel, V.; Unützer, J. Task-Sharing Approaches to Improve Mental Health Care in Rural and Other Low-Resource Settings: A Systematic Review. J. Rural Health 2018, 34, 48–62. [Google Scholar] [CrossRef]
- Barnett, M.L.; Gonzalez, A.; Miranda, J.; Chavira, D.A.; Lau, A.S. Mobilizing Community Health Workers to Address Mental Health Disparities for Underserved Populations: A Systematic Review. Adm. Policy Ment. Health 2018, 45, 195–211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takahashi, S.; Takagi, Y.; Fukuo, Y.; Arai, T.; Watari, M.; Tachikawa, H. Acute Mental Health Needs Duration during Major Disasters: A Phenomenological Experience of Disaster Psychiatric Assistance Teams (DPATs) in Japan. Int. J. Environ. Res. Public Health. 2020, 17, 1530. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Forbes, D.; Lewis, V.; Varker, T.; Phelps, A.; O’Donnell, M.; Wade, D.J.; Ruzek, J.I.; Watson, P.; Bryant, R.A.; Creamer, M. Psychological First Aid Following Trauma: Implementation and Evaluation Framework for High-Risk Organizations. Psychiatry 2011, 74, 224–239. [Google Scholar] [CrossRef] [PubMed]
- National Child Traumatic Stress Network (NCTSN). Psychological First Aid (PFA) Field Operations Guide, 2nd ed.; NCTSN: Los Angeles, CA, USA, 2006; Available online: https://www.nctsn.org/sites/default/files/resources//pfa_field_operations_guide.pdf (accessed on 2 February 2018).
- Cain, D.S.; Plummer, C.A.; Fisher, R.M.; Bankstrom, T.Q. Weathering the Storm: Persistent Effects and Psychological First Aid with Children Displaced by Katrina. J. Child Adolesc. Trauma 2010, 3, 330–343. [Google Scholar] [CrossRef]
- Fox, J.H.; Burkle, F.M., Jr.; Bass, J.; Pia, F.A.; Epstein, J.L.; Markenson, D. The Effectiveness of Psychological First Aid as a Disaster Intervention Tool: Research Analysis of Peer-Reviewed Literature from 1990–2010. Disaster Med. Public Health Prep. 2012, 6, 247–252. [Google Scholar] [CrossRef]
- Dieltjens, T.; Moonens, I.; Van Praet, K.; De Buck, E.; Vandekerckhove, P. A Systematic Literature Search on Psychological First Aid: Lack of Evidence to Develop Guidelines. PLoS ONE 2014, 9, e114714. [Google Scholar] [CrossRef]
- Springgate, B.F.; Arevian, A.C.; Wennerstrom, A.; Johnson, A.J.; Eisenman, D.P.; Sugarman, O.K.; Haywood, C.G.; Trapido, E.J.; Shelbourne, C.D.; Everett, A.; et al. Community Resilience Learning Collaborative and Research Network (C-LEARN): Study Protocol with Participatory Planning for a Randomized Comparative Effectiveness Trial. Int. J. Environ. Res. Public Health 2018, 15, 1683. [Google Scholar] [CrossRef] [Green Version]
- Kumpfer, K.L.; Molgaard, V.; Spoth, R. The Strengthening Families Program for Prevention of Delinquency and Drug Use in Special Populations. In Childhood Disorders, Substance Abuse, and Delinquency: Prevention and Early Intervention Approaches; Peters, R.D., McMahon, R.J., Eds.; Sage Publications: Newbury Park, CA, USA, 1996. [Google Scholar]
- Annan, J.; Sim, A.; Puffer, E.S.; Salhi, C.; Betancourt, T.S. Improving Mental Health Outcomes of Burmese Migrant and Displaced Children in Thailand: A Community-Based Randomized Controlled Trial of a Parenting and Family Skills Intervention. Prev. Sci. 2017, 18, 793–803. [Google Scholar] [CrossRef]
- James, L.E.; Welton-Mitchell, C.; Noel, J.R.; James, A.S. Integrating Mental Health and Disaster Preparedness in Intervention: A Randomized Controlled Trial with Earthquake and Flood-Affected Communities in Haiti. Psychol. Med. 2020, 50, 342–352. [Google Scholar] [CrossRef] [Green Version]
- Dawson, K.S.; Bryant, R.A.; Harper, M.; Tay, A.K.; Rahman, A.; Schafer, A.; van Ommeren, M. Problem Management Plus (PM+): A WHO Transdiagnostic Psychological Intervention for Common Mental Health Problems. World Psychiatry 2015, 14, 354–357. [Google Scholar] [CrossRef]
- Rahman, A.; Hamdani, S.U.; Awan, N.R.; Bryant, R.A.; Dawson, K.S.; Khan, M.F.; Azeemi, M.M.; Akhtar, P.; Sijbranij, M.; Wang, D.; et al. Effect of a Multicomponent Behavioral Intervention in Adults Impaired by Psychological Distress in a Conflict-Affected Area of Pakistan: A Randomized Controlled Trial. JAMA 2016, 316, 2609–2617. [Google Scholar] [CrossRef] [PubMed]
- Bryant, R.A.; Schafer, A.; Dawson, K.S.; Anjuri, D.; Mulili, C.; Ndogoni, L.; Koyiet, P.; Sijbrandij, M.; Ulate, J.; Shehadeh, M.H.; et al. Effectiveness of a Brief Behavioural Intervention on Psychological Distress Among Women with a History of Gender-Based Violence in Urban Kenya: A Randomised Clinical Trial. PLoS Med. 2017, 14, e1002371. [Google Scholar] [CrossRef] [PubMed]
- Rahman, A.; Khan, M.N.; Hamdani, S.U.; Chiumento, A.; Akhtar, P.; Nazir, H.; Nisar, A.; Masood, A.; Din, I.U.; Khan, N.A.; et al. Effectiveness of a Brief Group Psychological Intervention for Women in a Post-Conflict Setting in Pakistan: A Single-Blind, Cluster, Randomised Controlled Trial. Lancet 2019, 393, 1733–1744. [Google Scholar] [CrossRef]
- Berkowitz, S.; Bryant, R.; Brymer, M.; Hamblen, J.; Jacobs, A.; Layne, C.; Macy, R.; Osofsky, H.; Pynoos, R.; Ruzek, J.; et al. Skills for Psychological Recovery: Field Operations Guide. 2010. Available online: https://www.ptsd.va.gov/professional/treat/type/SPR/SPR_Manual.pdf (accessed on 18 August 2020).
- Gibson, K.; Forbes, D.; O’Donnell, M.L. Skills for Life Adjustment and Resilience (SOLAR)—A Pilot Study in Tuvalu. In Proceedings of the 7th World Congress of Asian Psychiatry, Sydney, Australia, 21–24 February 2019. [Google Scholar]
- O’Donnell, M.L.; Lau, W.; Fredrickson, J.; Gibson, K.; Bryant, R.A.; Bisson, J.; Burke, S.; Busuttil, W.; Coghlan, A.; Creamer, M.; et al. An Open Label Pilot Study of a Brief Psychosocial Intervention for Disaster and Trauma Survivors. Front. Psychiatry 2020, 11, 483. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J.A.; Mannarino, A.P.; Deblinger, E. Treating Trauma and Traumatic Grief in Children and Adolescents; The Guilford Press: New York, NY, USA, 2006. [Google Scholar]
- Jaycox, L.H.; Cohen, J.A.; Mannarino, A.P.; Walker, D.W.; Langley, A.K.; Gegenheimer, K.L.; Scott, M.; Schonlau, M. Children’s Mental Health Care Following Hurricane Katrina: A Field Trial of Trauma-Focused Psychotherapies. J. Trauma. Stress 2010, 23, 223–231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Resick, P.A.; Monson, C.M.; Chard, K.M. Cognitive Processing Therapy for PTSD: A Comprehensive Manual; The Guilford Press: New York, NY, USA, 2017. [Google Scholar]
- Bolton, P.; Bass, J.K.; Zagana, G.A.S.; Kamal, T.; Murray, S.M.; Kaysen, D.; Lejuez, C.W.; Lindgren, K.; Pagoto, S.; Murray, L.K.; et al. A Randomized Controlled Trial of Mental Health Interventions for Survivors of Systematic Violence in Kurdistan, Northern Iraq. BMC Psychiatry 2014, 14, 360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Catani, C.; Kohiladevy, N.; Ruf, M.; Schnauer, E.; Elbert, T.; Neuner, F. Treating Children Traumatized by War and Tsunami: A Comparison Between Exposure Therapy and Meditation-Relaxation in North-East Sri Lanka. BMC Psychiatry 2009, 9, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crombach, A.; Siehl, S. Impact and Cultural Acceptance of the Narrative Exposure Therapy in the Aftermath of a Natural Disaster in Burundi. BMC Psychiatry 2018, 18, 233. [Google Scholar] [CrossRef] [Green Version]
- Hamblen, J.L.; Norris, F.H.; Pietrusczkiewicz, S.; Gibson, L.E.; Naturale, A.; Louis, C. Cognitive Behavioral Therapy for Postdisaster Distress: A Community Based Treatment Program for Survivors of Hurricane Katrina. Adm. Policy Ment. Health 2009, 36, 206–214. [Google Scholar] [CrossRef]
- Chemtob, C.M.; Nakashima, J.; Carlson, J.G. Brief Treatment for Elementary School Children with Disaster-Related Posttraumatic Stress Disorder: A Field Study. J Clin Psychol 2002, 58, 99–112. [Google Scholar] [CrossRef] [Green Version]
- Jaycox, L. Cognitive Behavioral Intervention for Trauma in Schools (CBITS); Lopris West: Longmont, CO, USA, 2004. [Google Scholar]
- Ruggiero, K.J.; Price, M.; Adams, Z.; Stauffacher, K.M.; McCauley, J.; Danielson, C.K.; Knapp, R.; Hanson, R.F.; Davidson, T.M.; Amstadter, A.B.; et al. Web Intervention for Adolescents Affected by Disaster: Population-Based Randomized Controlled Trial. J. Acad. Child Adolesc. Psychiatry 2015, 54, 709–717. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gilmore, A.K.; Price, M.; Bountress, K.E.; Zuromski, K.L.; Ruggiero, K.; Resnick, H.J. A Longitudinal Examination of Interpersonal Violence Exposure, Concern for Loved Ones during a Disaster, and Web-Based Intervention Effects on Posttraumatic Stress Disorder among Adolescent Victims of the Spring 2011 Tornadoes. Interpers Violence 2018, 886260518791236. [Google Scholar] [CrossRef] [PubMed]
- Berger, R.; Gelkopf, M. School-Based Intervention for the Treatment of Tsunami-Related Distress in Children: A Quasi-Randomized Controlled Trial. Psychother. Psychosom. 2009, 78, 364–371. [Google Scholar] [CrossRef] [PubMed]
- Chemtob, C.M.; Nakashima, J.P.; Hamada, R.S. Psychosocial Intervention for Postdisaster Trauma Symptoms in Elementary School Children: A Controlled Community Field Study. Arch. Pediatr. Adolesc. Med. 2002, 156, 211–216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salloum, A.; Overstreet, S. Evaluation of Individual and Group Grief and Trauma Interventions for Children Post Disaster. J. Clin. Child Adolesc. Psychol. 2008, 37, 495–507. [Google Scholar] [CrossRef] [PubMed]
- Salloum, A.; Overstreet, S. Grief and Trauma Intervention for Children After Disaster: Exploring Coping Skills Versus Trauma Narration. Behav. Res. Ther. 2012, 50, 169–179. [Google Scholar] [CrossRef]
- Hardin, S.B.; Weinrich, S.; Weinrich, M.; Garrison, C.; Addy, C.; Hardin, T.L. Effects of a Long-Term Psychosocial Nursing Intervention on Adolescents Exposed to Catastrophic Stress. Issues Ment. Health Nurs. 2002, 23, 537–551. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence. Generalised Anxiety Disorder and Panic Disorder in Adults: Management Clinical Guideline. 2019. Available online: www.nice.org.uk/guidance/cg113.https://www.apa.org/depression-guideline/guideline.pdf (accessed on 18 August 2020).
- American Psychological Association Guideline Development Panel for the Treatment of Depressive Disorders. Clinical Practice Guideline for the Treatment of Depression across Three Age Cohorts. 2019. Available online: https://www.apa.org/depression-guideline/guideline.pdf (accessed on 20 August 2020).
- Sirey, J.A.; Raue, P.J.; Solomonov, N.; Scher, C.; Chalfin, A.; Zanotti, P.; Berman, J.; Alexopoulos, A. Community Delivery of Brief Therapy for Depressed Older Adults Impacted by Hurricane Sandy. Translat. Behav. Med. 2020, 10, 539–545. [Google Scholar] [CrossRef]
- Grolnick, W.S.; Schonfeld, D.J.; Schreiber, M.; Cohen, J.; Cole, V.; Jaycox, L.; Lochman, J.; Pfefferbaum, B.; Ruggiero, K.; Wells, K.; et al. Improving Adjustment and Resilience in Children Following a Disaster: Addressing Research Challenges. Am. Psychol. 2018, 73, 215–229. [Google Scholar] [CrossRef]
- Suzuki, Y.; Fukasawa, M.; Nakajima, S.; Narisawa, T.; Keiko, A.; Kim, Y. Developing a Consensus-Based Definition of “Kokoro-no Care” or Mental Health Services and Psychosocial Support: Drawing from Experiences of Mental Health Professionals Who Responded to the Great East Japan Earthquake. PLoS Curr. Disasters 2015, 1. [Google Scholar] [CrossRef]
- Seto, M.; Nemoto, H.; Kobayashi, N.; Kikuchi, S.; Honda, N.; Kim, Y.; Kelman, I.; Tomita, H. Post-Disaster Mental Health and Psychosocial Support in the Areas Affected by the Great East Japan Earthquake: A Qualitative Study. BMC Psychiatry 2019, 19, 261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Substance Abuse and Mental Health Services Administration (SAMHSA). Online Disaster Behavioral Health Trainings. 2018. Available online: https://www.samhsa.gov/dbhis-collections/online-trainings (accessed on 20 August 2020).
- Kang, J.Y.; Choi, Y.J. Effects of a Psychosocial First Aid Simulated Training for Pregnant Flood Victims on Disaster Relief Workers’ Knowledge, Competency, and Self-Efficacy. Appl. Nurs. Res. 2020, 151348. [Google Scholar] [CrossRef] [PubMed]
- Sijbrandij, M.; Horn, R.; Esliker, R.; O’May, F.; Reiffers, R.; Ruttenberg, L.; Stam, K.; de Jong, J.; Ager, A. The Effect of Psychological First Aid Training on Knowledge and Understanding about Psychosocial Support Principles: A Cluster-Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2020, 17, 484. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wade, D.; Crompton, D.; Howard, A.; Stevens, N.; Metcalf, O.; Brymer, M.; Ruzek, J.; Watson, P.; Bryant, R.; Forbes, D. Skills for Psychological Recovery: Evaluation of a Post-Disaster Mental Health Training Program. Disaster Health 2014, 2, 138–145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ciccone, A.; Bodley, G.; Hansel, T.; McDonough, M.; McShan, L.; Osofsky, H.; Osofsky, J.; Reuther, E.; Schuster, L.; Speier, A.; et al. Disaster Psychosocial Assessment and Surveillance Toolkit (Disaster-PAST): Methods to Enhance Disaster Preparedness, Response and Recovery; Louisiana State University Health Sciences Center Department of Psychiatry: New Orleans, LA, USA, 2014. [Google Scholar]
- Norris, F.H.; Friedman, M.J.; Watson, P.J.; Byrne, C.M.; Diaz, E.; Kaniasty, K. 60,000 Disaster Victims Speak: Part 1. An Empirical Review of the Empirical Literature, 1981–2001. Psychiatry 2002, 65, 207–239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rataj, E.; Kunzweiler, K.; Garthus-Niegel, S. Extreme Weather Events in Developing Countries and Related Injuries and Mental Health Disorders—A Systematic Review. BMC Public Health 2016, 16, 1020. [Google Scholar] [CrossRef] [Green Version]
- Jones, S.; Walker, C.; Miles, A.C.; De Silva, E.; Zimitat, C. A Rural, Community-Based Suicide Awareness and Intervention Program. Rural Remote Health 2015, 15, 2972. [Google Scholar] [CrossRef]
- Sartore, G.M.; Kelly, B.; Stain, H.J.; Fuller, J.; Fragar, L.; Tonna, A. Improving Mental Health Capacity in Rural Communities: Mental Health First Aid Delivery in Drought-Affected Rural New South Wales. Aust. J. Rural Health 2008, 16, 313–318. [Google Scholar] [CrossRef]
- Jorm, A.F.; Kitchener, B.A.; O’Kearney, R.; Dear, K. Mental Health First Aid Training of the Public in a Rural Area: A Cluster Randomised Trial. BMC Psychiatry 2004, 4, 33. [Google Scholar] [CrossRef] [Green Version]
- Hamel, L.; Lopez, L.; Munana, C.; Brodie, M. The Kaiser Family Foundation/ Washington Post Climate Change Survey; Kaiser Family Foundation: San Francisco, CA, USA, 2019; Available online: https://www.kff.org/report-section/the-kaiser-family-foundation-washington-post-climate-change-survey-main-findings/ (accessed on 7 July 2020).
- Howe, P.D.; Marlon, J.R.; Wang, X.; Leiserowitz, A. Public Perceptions of the Health Risks of Extreme Heat Across US States, Counties, and Neighborhoods. Proc. Natl. Acad. Sci. USA 2019, 116, 6743–6748. [Google Scholar] [CrossRef] [Green Version]
- Fischhoff, B.; Brewer, N.T.; Downs, J. Communicating Risks and Benefits: An Evidence-Based User’s Guide; Food and Drug Administration: Washington, DC, USA, 2011. [Google Scholar]
- Arvai, J.; Rivers, L., III (Eds.) Effective Risk Communication; Routledge: New York, NY, USA, 2013. [Google Scholar]
- Mah, A.Y.J.; Chapman, D.A.; Markowitz, E.M.; Lickel, B. Coping with Climate Change: Three Insights for Research, Intervention, and Communication to Promote Adaptive Coping to Climate Change. J. Anxiety Disord. 2020, 75, 102282. [Google Scholar] [CrossRef] [PubMed]
- Doherty, T. Theoretical and Empirical Foundations for Ecotherapy. In Ecotherapy: Theory, Research and Practice; Jordan, M., Hinds, J., Eds.; Palgrave: New York, NY, USA, 2016; pp. 12–31. [Google Scholar]
- Hasbach, P.H. Therapy in the face of climate change. Ecopsychology 2015, 7, 205–210. [Google Scholar] [CrossRef]
- Keniger, L.E.; Gaston, K.J.; Irvine, K.N.; Fuller, R.A. What are the Benefits of Interacting with Nature? Int. J. Environ. Res. Public Health 2013, 10, 913–935. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maas, J.; Verheij, R.; Groenewegen, P.; de Vries, S.; Spreeuwenberg, P. Green Space, Urbanity and Health: How Strong is the Relationship? J. Epidemiol. Community Health 2006, 60, 587–592. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weissbecker, I. (Ed.) Climate Change and Human Well-Being: Global Challenges and Opportunities; Springer: New York, NY, USA, 2011. [Google Scholar]
- MacIntyre, E.; Khanna, S.; Darychuk, A.; Copes, R.; Schwartz, B. Evidence Synthesis—Evaluating Risk Communication During Extreme Weather and Climate Change: A Scoping Review. Health Promot. Chronic Dis. Prev. Can. 2019, 39, 142–156. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Inclusion Criteria Item | Description | Justification |
|---|---|---|
| Population | Persons aged 5–85 | Age limits were based on two considerations: (1) populations exposed to climate change, and therefore, at risk for adverse mental health impacts include all age groups [1,2,3,4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20]; and (2) target populations of interventions designed to prevent and treat these outcomes including those targeting school-aged youth, adults, and older adults. |
| Intervention | Universal, selective, and indicated interventions designed to prevent or mitigate symptoms of posttraumatic stress, depression, anxiety, or any forms of psychosocial dysfunction. Interventions designed to treat individuals meeting diagnostic criteria for PTSD, depressive, or anxiety disorders. | Selection of interventions was based on the classification of interventions provided by the National Academy of Sciences [28] and guidelines and recommendations provided by international bodies for addressing mental health outcomes of disasters and other emergencies. These included the World Health Organization [30], United Nations [31,32], and North Atlantic Treaty Organization (NATO) Joint Medical Committee [33] |
| Comparisons and outcomes | All reported assessments of mental health outcomes using validated measures | Assessments of efficacy or effectiveness require the use of standardized and validated measures of mental health status to ensure results are valid, replicable, and generalizable. |
| Study design | Qualitative, mixed methods and quantitative studies such as descriptive studies, research case studies, pre-post trials, RCTs, and evaluation studies | Few interventions have been designed specifically to address the mental health impacts of climate change; hence a decision was made to include exploratory investigations of potential interventions as well as investigations of interventions developed to prevent and treat mental health problems associated with other traumatic events (i.e., civil conflicts, terrorism, manmade disasters, earthquakes). |
| Articles | English-language articles published in academic journals that follow a peer-review publication process | Although this review did not assess the risk of bias, it did seek to identify studies that adhered to the World Medical Association Declaration of Helsinki—Ethical Principles for Medical Research Involving Human Subjects. The selection of peer-reviewed publications helped to ensure a baseline for evaluation of the quality of scientific evidence. |
| Publication date | 2000–2020 | A preliminary review of literature reviewed no peer-reviewed publications on the topic appearing prior to 2000. |
| IOM Service Categories and Approaches | Climate-Related Events | |||
|---|---|---|---|---|
| Acute | Subacute | Long-Lasting | ||
| Prevention | Universal | PFA IMHD Mapping Tier 1–2 training SFP | MHFA CORES Advocacy Adaptation Mapping Tier 1–2 training | Risk communication Ecotherapy Psychosocial resilience Tier 1–2 training |
| Selective | SFP Tier 1–2 training | Suicide prevention Heat exposure interventions Tier 1–2 training | ||
| Indicated | Tier 1–3 training PM+ SPR SOLAR | Tier 1–3 training PM+ SPR SOLAR | Tier 1–3 training PM+ SPR SOLAR | |
| Treatment | Standard | CBITS BBN TF-CBT CPT CBT-PD NET EMDR CBT for Anxiety and Depression Tier 3-4 training | CBITS BBN TF-CBT (conflict) CPT (conflict) CBT-PD (conflict) NET (conflict) EMDR (conflict) CBT for Anxiety and Depression Tier 3-4 training | CBITS BBN CBT for Anxiety and Depression Tier 3–4 training |
| Intervention | Ratings of Scientific Evidence | |||||
|---|---|---|---|---|---|---|
| Acute Events | Refs | Sub-Acute Events | Refs | Long-Term Events | Refs | |
| Universal and selective interventions | ||||||
| Psychological first aid | 2 * | Kang, J.Y. et al., 2020; Sijbrandij, M. et al., 2020 | NR | NR | ||
| Mental health first aid | NR | 2 * | Sartore, G.M. et al., 2008; Jorm, A.F. et al., 2004 | NR | ||
| Ecotherapy | NR | NR | NR | |||
| Strengthening families program | NR | NR | NR | |||
| Integrated mental health and disaster preparedness | 2 | James, L.E. et al., 2020 | NR | NR | ||
| Community response to eliminating suicide | NR | NR | NR | |||
| Indicated interventions | ||||||
| Problem management plus | NR | NR | NR | |||
| Skills for psychological recovery | 3 | Bisson, J.I. et al., 2010 | NR | NR | ||
| SOLAR | 3 | Gibson, K. et al., 2019, O’Donnell, M.L. et al., 2020 | NR | NR | ||
| Treatment interventions | ||||||
| School-based interventions | 1 | Jaycox, L.H. et al., 2010; Jaycox, L., 2004; Ruggiero, K.J. et al., 2015; Gilmore, A.K. et al., 2018; Berger, R. et al., 2009; Chemtob, C.M. et al., 2002; Salloum, A. et al., 2008; Salloum, A. et al., 2012; Hardin, S.B. et al., 2002 | NR | NR | ||
| Trauma focused-cognitive behavioral therapy | 2 | Jaycox, L.H. et al., 2010 | NR | NR | ||
| Cognitive-behavioral therapy-Post disaster | 3 | Hamblen, J.L. et al., 2009 | NR | NR | ||
| Cognitive processing therapy | NR | NR | NR | |||
| Cognitive-behavioral therapy for depression or anxiety | 2 | Bisson, J.I. et al., 2010; American Psychological Association Guideline Development Panel for the Treatment of Depressive Disorders, 2019 | NR | |||
| Narrative exposure therapy | 2 | Catani, C. et al., 2009; Crombach, A. et al., 2018 | NR | NR | ||
| Eye movement desensitization and reprocessing | 2 | Chemtob, C.M. et al., 2002 | NR | NR | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Palinkas, L.A.; O’Donnell, M.L.; Lau, W.; Wong, M. Strategies for Delivering Mental Health Services in Response to Global Climate Change: A Narrative Review. Int. J. Environ. Res. Public Health 2020, 17, 8562. https://doi.org/10.3390/ijerph17228562
Palinkas LA, O’Donnell ML, Lau W, Wong M. Strategies for Delivering Mental Health Services in Response to Global Climate Change: A Narrative Review. International Journal of Environmental Research and Public Health. 2020; 17(22):8562. https://doi.org/10.3390/ijerph17228562
Chicago/Turabian StylePalinkas, Lawrence A., Meaghan L. O’Donnell, Winnie Lau, and Marleen Wong. 2020. "Strategies for Delivering Mental Health Services in Response to Global Climate Change: A Narrative Review" International Journal of Environmental Research and Public Health 17, no. 22: 8562. https://doi.org/10.3390/ijerph17228562