Current Perceptions and Improvement Approaches of Pharmaceutical Care Capacity of Community Pharmacists: A Quantitative Analysis Based on Survey Data at Chinese Chain Pharmacies


Abstract
:1. Introduction
2. Methods
2.1. Questionnaire/Instrument Design
2.2. Data Collection
2.3. Data Analysis
3. Results
3.1. Demographics
3.2. Impact of Incapacity
3.3. Attitude in Capacity Enhancement
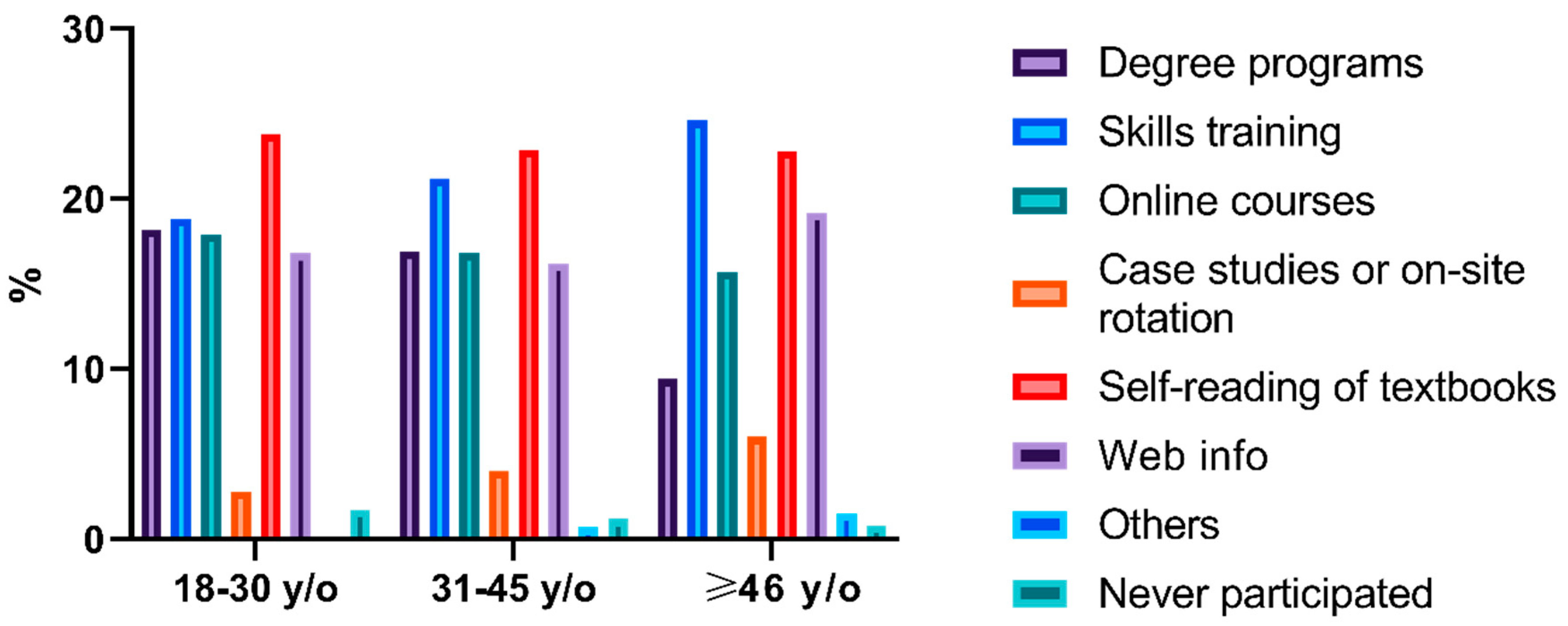
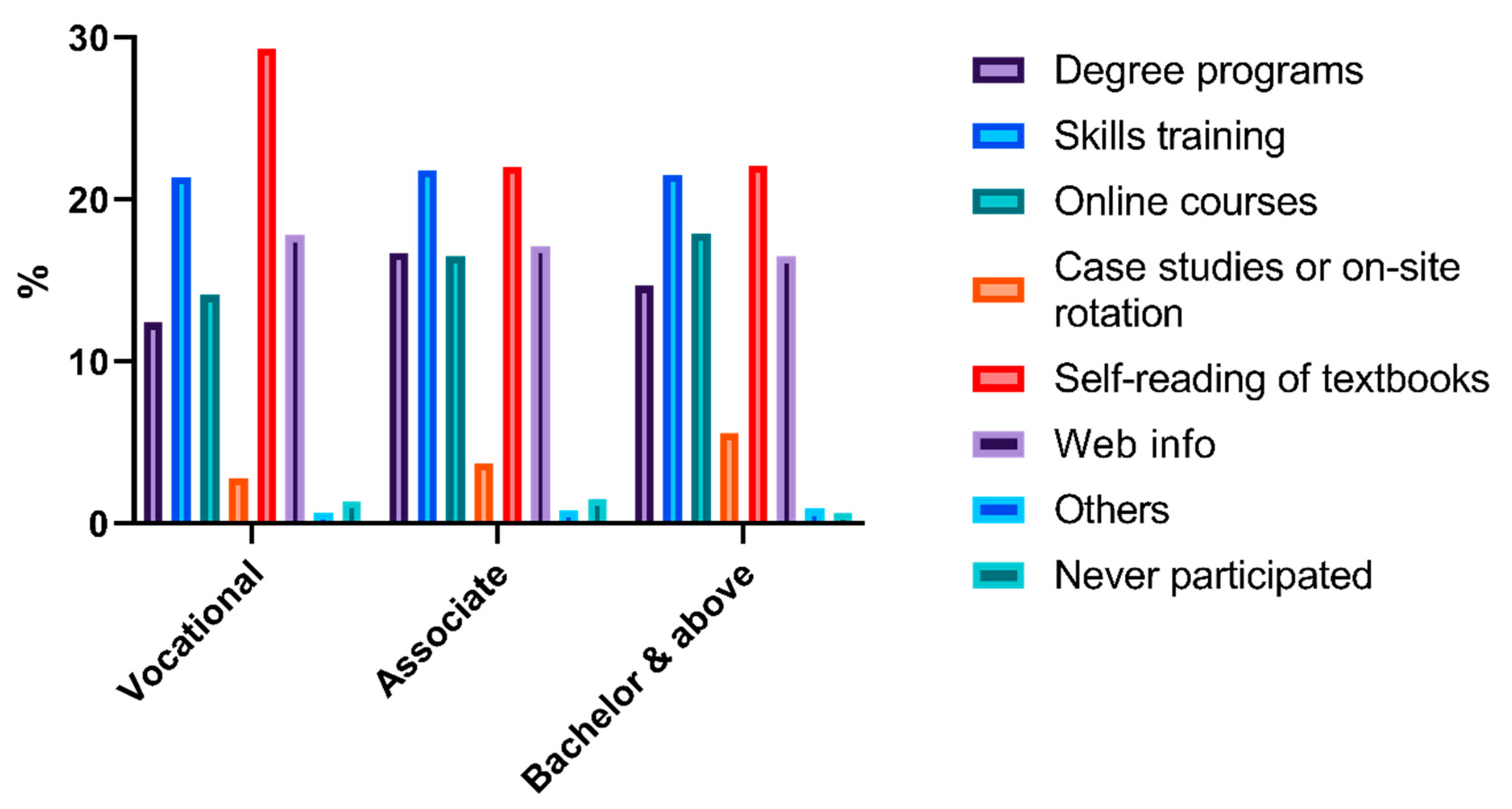
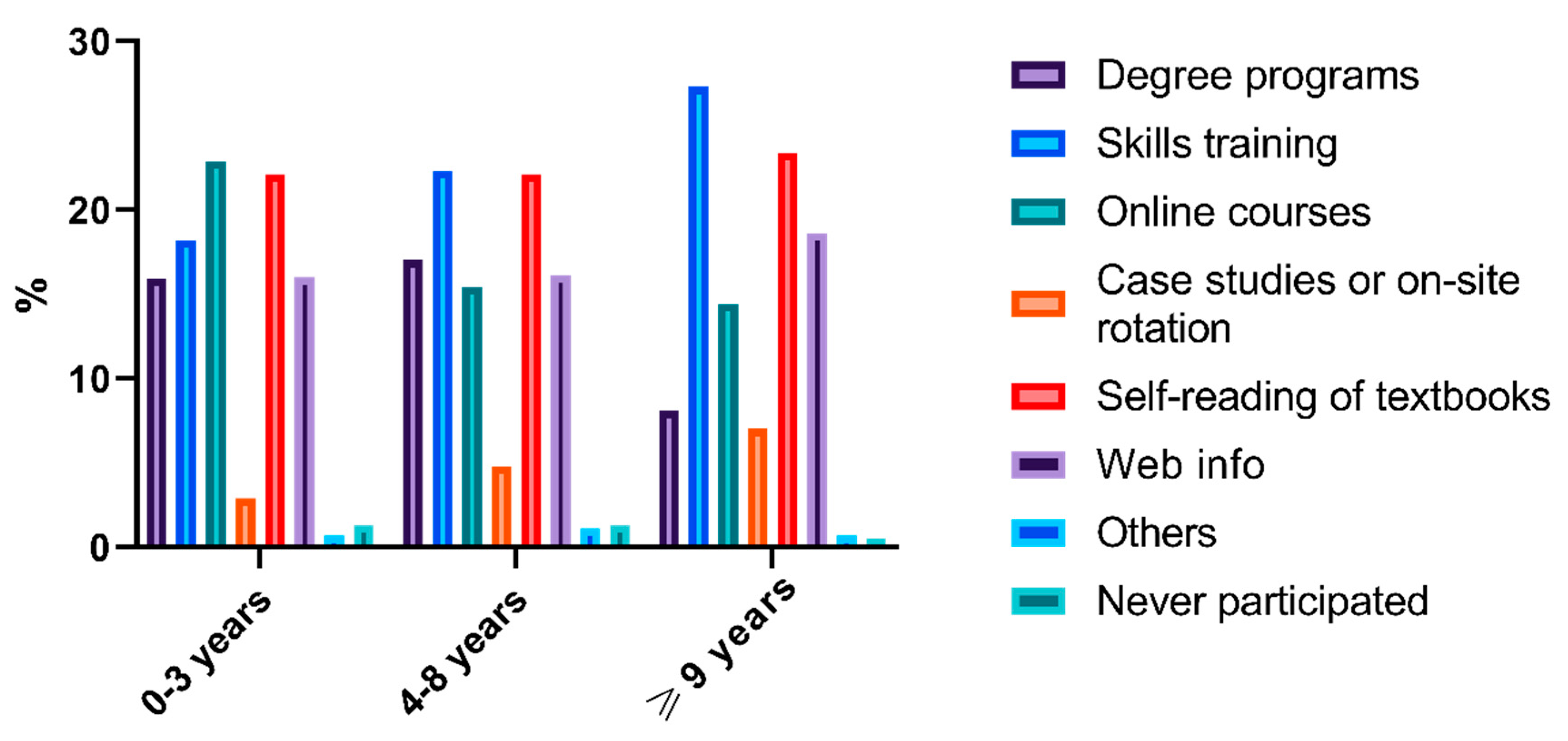
3.4. Previous Attempts and Current Practice
3.5. Barriers in Capacity Enhancement
3.6. Facilitators in Capacity Enhancement
4. Discussion
5. Strengths and Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Farris, K.B.; Fernandez-Llimos, F.; Benrimoj, S.I. Pharmaceutical care in community pharmacies: Practice and research from around the world. Ann. Pharmacother. 2005, 39, 1539–1541. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hepler, C.D.; Strand, L.M. Opportunities and responsibilities in pharmaceutical care. Am. J. Hosp. Pharm. 1990, 47, 533–543. [Google Scholar] [CrossRef] [PubMed]
- Draft statement on pharmaceutical care. ASHP Council on Professional affairs. American Society of Hospital Pharmacists. Am. J. Hosp. Pharm. 1993, 50, 126–128.
- International pharmacists adopt statement on pharmaceutical care. Am. J. Health Syst. Pharm. 1998, 55, 2598. [CrossRef] [PubMed]
- Losada-Camacho, M.; Guerrero-Pabon, M.F.; Garcia-Delgado, P.; Martinez-Martinez, F. Impact of a pharmaceutical care programme on health-related quality of life among women with epilepsy: A randomised controlled trial (IPHIWWE study). Health Qual. Life Outcomes 2014, 12, 162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hughes, R.G.; Ortiz, E. Medication errors: Why they happen, and how they can be prevented. J. Infus. Nurs. 2005, 28, 14–24. [Google Scholar] [CrossRef] [PubMed]
- Juanes, A.; Garin, N.; Mangues, M.A.; Herrera, S.; Puig, M.; Faus, M.J.; Baena, M.I. Impact of a pharmaceutical care programme for patients with chronic disease initiated at the emergency department on drug-related negative outcomes: A randomised controlled trial. Eur. J. Hosp. Pharm. 2018, 25, 274–280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aslani, P.; Lucero, E.; Dimitrow, M.; Guirguis, L.M.; Hämeen-Anttila, K.; Laurikainen, A.; Leikola, S.; Norris, P.; Buabeng, K.O.; Parkkamäki, S.; et al. Counselling, Concordance and Communication: Innovative Education for Pharmacists; International Pharmaceutical Students’ Federation (IPSF) and International Pharmaceutical Federation (FIP): The Hague, The Netherlands, 2012. [Google Scholar]
- Dalton, K.; Byrne, S. Role of the pharmacist in reducing healthcare costs: Current insights. Integr. Pharm. Res. Pract. 2017, 6, 37–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steltenpohl, E.A.; Barry, B.K.; Coley, K.C.; McGivney, M.S.; Olenak, J.L.; Berenbrok, L.A. Point-of-Care Testing in Community Pharmacies: Keys to Success from Pennsylvania Pharmacists. J. Pharm. Pract. 2018, 31, 629–635. [Google Scholar] [CrossRef] [PubMed]
- Kijlstra, N.; Ridge, K.; Walser, S. Pharmaceutical Care: Where Do We stand—Where Should We Go? European Directorate for the Quality of Medicines & HealthCare: Strasbourg, France, 2009. [Google Scholar]
- Fang, Y.; Yang, S.; Zhou, S.; Jiang, M.; Liu, J. Community pharmacy practice in China: Past, present and future. Int. J. Clin. Pharm. 2013, 35, 520–528. [Google Scholar] [CrossRef] [PubMed]
- Xi, X.; Huang, Y.; Lu, Q.; Ung, C.O.L.; Hu, H. Community pharmacists’ opinions and practice of pharmaceutical care at chain pharmacy and independent pharmacy in China. Int. J. Clin. Pharm. 2019, 41, 478–487. [Google Scholar] [CrossRef] [PubMed]
- Jiang, J.H.; Liu, Y.; Wang, Y.J.; Liu, X.; Yang, M.; Zeng, Y.; Deng, P.; Li, Q.G. Clinical pharmacy education in China. Am. J. Pharm. Educ. 2011, 75, 57c. [Google Scholar] [CrossRef] [PubMed]
- Mossialos, E.; Courtin, E.; Naci, H.; Benrimoj, S.; Bouvy, M.; Farris, K.; Noyce, P.; Sketris, I. From “retailers” to health care providers: Transforming the role of community pharmacists in chronic disease management. Health Policy 2015, 119, 628–639. [Google Scholar] [CrossRef] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |




{kind=link}
{kind=link}
{kind=link}
| Characteristics | No. of Pharmacists, n (%) | Characteristics | No. of Pharmacists, n (%) |
|---|---|---|---|
| Q1. Age | Q8. Academic degrees | ||
| 18–30 y/o (young) | 138 (11.0%) | Satisfied, no plans | 207 (16.4%) |
| 31–45 y/o (middle-aged) | 859 (68.2%) | Satisfied, with further plan | 435 (34.5%) |
| ≥46 y/o (older) | 263 (20.9%) | Unsatisfied, in plan now | 312 (24.8%) |
| Q2. Education level | Unsatisfied, have plans but were not implemented | 177 (14.0%) | |
| Vocational | 183 (14.5%) | Unsatisfied, no plans | 71 (5.6%) |
| Associate | 605 (48.0%) | Never thought of | 57 (4.5%) |
| Bachelor or above | 471 (37.4%) | ||
| Q3. Seniority | Q9. Biggest barriers | ||
| 0–3 years (low) | 644 (51.1%) | Cost | 70 (5.6%) |
| 4–8 years (middle) | 406 (32.2%) | Conflict with daily work | 446 (35.4%) |
| ≥9 years (high) | 210 (16.7%) | Conflict with family life | 276 (21.9%) |
| Q4. Willingness | Poor memories | 193 (15.3%) | |
| Very willing | 1081 (85.8%) | Do not know how to improve | 83 (6.6%) |
| A bit willing | 156 (12.4%) | No motivation or stimulus | 41 (3.3%) |
| Not very willing | 4 (0.3%) | Others | 22 (1.7%) |
| Definitely not willing | 1 (0.1%) | No barriers | 128 (10.2%) |
| Never thought of | 17 (1.3%) | ||
| Q5. Previous attempts | Q10. Facilitators | ||
| Degree programs | 521 (41.3%) | Adult education | 197 (15.6%) |
| Skills training | 733 (58.2%) | Skills training | 358 (28.4%) |
| Online courses | 567 (45.0%) | Online resources | 256 (20.3%) |
| Case studies or on-site rotation | 146 (11.6%) | Textbooks/publications | 132 (10.5%) |
| Self-reading of textbooks | 778 (61.7%) | Case-study | 97 (7.7%) |
| Web info | 574 (45.6%) | Rotation/internship | 112 (8.9%) |
| Others | 28 (2.2%) | New drug info | 42 (3.3%) |
| Never participated | 40 (3.2%) | Public health promotion | 40 (3.2%) |
| Others | 6 (0.5%) | ||
| Never thought of | 20 (1.6%) | ||
| Q6. Frequency of feeling incapable | Q11. Benefits of traditional practice | ||
| Very often | 205 (16.2%) | Lots of help | 590 (46.9%) |
| Occasionally | 849 (67.4%) | Some but limited help | 617 (49.1%) |
| Seldom | 168 (13.3%) | Very little/no help | 44 (3.5%) |
| Never | 38 (3.0%) | Never thought of | 6 (0.5%) |
| Q7. Impact of insufficient abilities | Q12. Benefits of continuing education | ||
| Review prescriptions | 47 (3.7%) | Lots of help | 483 (38.4%) |
| Medication guidance | 491 (39.0%) | Some but limited help | 697 (55.4%) |
| Answer questions | 261(20.7%) | Very little/no help | 66 (5.3%) |
| Communicate | 167 (13.3%) | Never participated | 13 (1.0%) |
| Job promotion | 62 (4.9%) | ||
| Find other jobs | 35 (2.8%) | ||
| Others | 26 (2.1%) | ||
| None | 171 (13.6%) |
| Characteristics | Groups | Test Value | Degrees of Freedom | p | Gamma Coefficient | ||
|---|---|---|---|---|---|---|---|
| Q6 | Age | All | 11.298 | 2 | 0.004 | 0.001 (p = 0.990) | |
| 18–30 y/o vs. | 31–45 y/o | −29.771 | 0.897 | ||||
| ≥46 y/o | 92.459 | 0.013 | |||||
| 31–45 y/o vs. | ≥46 y/o | 62.687 | 0.009 | ||||
| Education level | All | 1.031 | 2 | 0.597 | −0.015 (p = 0.771) | ||
| Vocational vs. | Associate | * | * | ||||
| Bachelor or above | * | * | |||||
| Associate vs. | Bachelor or above | * | * | ||||
| Seniority | All | 21.809 | 2 | 0.000 | −0.032 (p = 0.494) | ||
| 0–3 years vs. | 4–8 years | −37.589 | 0.148 | ||||
| ≥9 years | 111.134 | 0.000 | |||||
| 4–8 years vs. | ≥9 years | 73.546 | 0.012 | ||||
| Q7 | Age | All | 35.429 | 14 | 0.001 | ||
| 18–30 y/o vs. | 31–45 y/o | 8.854 | 7 | 0.263 | |||
| ≥46 y/o | 24.089 | 7 | 0.001 | ||||
| 31–45 y/o vs. | ≥46 y/o | 21.753 | 7 | 0.003 | |||
| Education level | All | 60.288 | 14 | 0.000 | |||
| Vocational vs. | Associate | 15.870 | 7 | 0.026 | |||
| Bachelor or above | 57.776 | 7 | 0.000 | ||||
| Associate vs. | Bachelor or above | 28.024 | 7 | 0.000 | |||
| Seniority | All | 27.746 | 14 | 0.015 | |||
| 0–3 years vs. | 4–8 years | 12.145 | 7 | 0.096 | |||
| ≥9 years | 16.320 | 7 | 0.022 | ||||
| 4–8 years vs. | ≥9 years | 13.088 | 7 | 0.070 | |||
| Characteristics | Groups | Test Value | Degrees of Freedom | p | Gamma Coefficient | ||
|---|---|---|---|---|---|---|---|
| Q4 | Age | All | 16.937 | 2 | 0.000 | 0.210 (p = 0.011) | |
| 18–30 y/o vs. | 31–45 y/o | 0.790 | 1.000 | ||||
| ≥46 y/o | 59.757 | 0.022 | |||||
| 31–45 y/o vs. | ≥46 y/o | 60.547 | 0.000 | ||||
| Education level | All | 0.474 | 2 | 0.789 | 0.028 (p = 0.699) | ||
| Vocational vs. | Associate | * | * | ||||
| Bachelor or above | * | * | |||||
| Associate vs. | Bachelor or above | * | * | ||||
| Seniority | All | 15.956 | 2 | 0.000 | 0.252 (p = 0.001) | ||
| 0–3 years vs. | 4–8 years | −27.980 | 0.105 | ||||
| ≥9 years | 64.957 | 0.000 | |||||
| 4–8 years vs. | ≥9 years | 36.977 | 0.118 | ||||
| Q8 | Age | All | 90.519 | 10 | 0.000 | ||
| 18–30 y/o vs. | 31–45 y/o | 0.679 | 5 | 0.984 | |||
| ≥46 y/o | 34.696 | 5 | 0.000 | ||||
| 31–45 y/o vs. | ≥46 y/o | 84.650 | 5 | 0.000 | |||
| Education level | All | 303.985 | 10 | 0.000 | |||
| Vocational vs. | Associate | 111.628 | 5 | 0.000 | |||
| Bachelor or above | 136.084 | 5 | 0.000 | ||||
| Associate vs. | Bachelor or above | 101.449 | 4 | 0.000 | |||
| Seniority | All | 120.590 | 10 | 0.000 | |||
| 0–3 years vs. | 4–8 years | 23.304 | 5 | 0.000 | |||
| ≥9 years | 112.496 | 5 | 0.000 | ||||
| 4–8 years vs. | ≥9 years | 41.217 | 5 | 0.000 | |||
| Characteristics | Groups | Test Value | Degrees of Freedom | p | Gamma Coefficient | ||
|---|---|---|---|---|---|---|---|
| Q11 | Age | All | 0.494 | 2 | 0.781 | −0.037 (p = 0.491) | |
| 18–30 y/o vs. | 31–45 y/o | * | * | ||||
| ≥46 y/o | * | * | |||||
| 31–45 y/o vs. | ≥46 y/o | * | * | ||||
| Education level | All | 8.601 | 2 | 0.014 | 0.135 (p = 0.004) | ||
| Vocational vs. | Associate | −44.103 | 0.293 | ||||
| Bachelor or above | −78.757 | 0.013 | |||||
| Associate vs. | Bachelor or above | 34.654 | 0.230 | ||||
| Seniority | All | 9.863 | 2 | 0.007 | −0.090 (p = 0.054) | ||
| 0–3 years vs. | 4–8 years | 8.049 | 1.000 | ||||
| ≥9 years | 71.986 | 0.014 | |||||
| 4–8 years vs. | ≥9 years | 80.035 | 0.009 | ||||
| Q12 | Age | All | 0.482 | 2 | 0.786 | 0.037 (p = 0.493) | |
| 18–30 y/o vs. | 31–45 y/o | * | * | ||||
| ≥46 y/o | * | * | |||||
| 31–45 y/o vs. | ≥46 y/o | * | * | ||||
| Education level | All | 11.026 | 2 | 0.004 | −0.004 (p = 0.924) | ||
| Vocational vs. | Associate | −45.839 | 0.257 | ||||
| Bachelor or above | −87.532 | 0.004 | |||||
| Associate vs. | Bachelor or above | 41.692 | 0.096 | ||||
| Seniority | All | 1.559 | 2 | 0.459 | 0.057 (p = 0.223) | ||
| 0–3 years vs. | 4–8 years | * | * | ||||
| ≥9 years | * | * | |||||
| 4–8 years vs. | ≥9 years | * | * | ||||
| Characteristics | Groups | Test Value | Degrees of Freedom | p | ||
|---|---|---|---|---|---|---|
| Q9 | Age | All | 190.030 | 14 | 0.000 | |
| 18–30 y/o vs. | 31–45 y/o | 26.870 | 7 | 0.000 | ||
| ≥46 y/o | 82.572 | 7 | 0.000 | |||
| 31–45 y/o vs. | ≥46 y/o | 140.828 | 7 | 0.000 | ||
| Education level | All | 33.102 | 14 | 0.003 | ||
| Vocational vs. | Associate | 14.103 | 7 | 0.049 | ||
| Bachelor or above | 22.102 | 7 | 0.002 | |||
| Associate vs. | Bachelor or above | 16.423 | 7 | 0.022 | ||
| Seniority | All | 25.899 | 14 | 0.027 | ||
| 0–3 years vs. | 4–8 years | 6.997 | 7 | 0.429 | ||
| ≥9 years | 23.627 | 7 | 0.001 | |||
| 4–8 years vs. | ≥9 years | 9.397 | 7 | 0.225 | ||
| Characteristics | Groups | Test Value | Degrees of Freedom | p | ||
|---|---|---|---|---|---|---|
| Q10 | Age | All | 362.678 | 22 | 0.000 | |
| 18–30 y/o vs. | 31–45 y/o | 22.416 | 9 | 0.008 | ||
| ≥46 y/o | 31.725 | 9 | 0.000 | |||
| 31–45 y/o vs. | ≥46 y/o | 23.332 | 9 | 0.005 | ||
| Education level | All | 528.675 | 22 | 0.000 | ||
| Vocational vs. | Associate | 22.543 | 9 | 0.007 | ||
| Bachelor or above | 68.818 | 9 | 0.000 | |||
| Associate vs. | Bachelor or above | 46.342 | 9 | 0.000 | ||
| Seniority | All | 501.457 | 22 | 0.000 | ||
| 0–3 years vs. | 4–8 years | 15.019 | 9 | 0.090 | ||
| ≥9 years | 37.919 | 9 | 0.000 | |||
| 4–8 years vs. | ≥9 years | 18.021 | 9 | 0.035 | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tang, Z.; Lhamu, P.; Ye, H.; Hong, L.; Xiang, X. Current Perceptions and Improvement Approaches of Pharmaceutical Care Capacity of Community Pharmacists: A Quantitative Analysis Based on Survey Data at Chinese Chain Pharmacies. Int. J. Environ. Res. Public Health 2020, 17, 7482. https://doi.org/10.3390/ijerph17207482
Tang Z, Lhamu P, Ye H, Hong L, Xiang X. Current Perceptions and Improvement Approaches of Pharmaceutical Care Capacity of Community Pharmacists: A Quantitative Analysis Based on Survey Data at Chinese Chain Pharmacies. International Journal of Environmental Research and Public Health. 2020; 17(20):7482. https://doi.org/10.3390/ijerph17207482
Chicago/Turabian StyleTang, Zhijia, Pema Lhamu, Hua Ye, Lan Hong, and Xiaoqiang Xiang. 2020. "Current Perceptions and Improvement Approaches of Pharmaceutical Care Capacity of Community Pharmacists: A Quantitative Analysis Based on Survey Data at Chinese Chain Pharmacies" International Journal of Environmental Research and Public Health 17, no. 20: 7482. https://doi.org/10.3390/ijerph17207482