Effects of Elastic Band Exercise on Functional Fitness and Blood Pressure Response in the Healthy Elderly


Abstract
:1. Introduction
2. Method
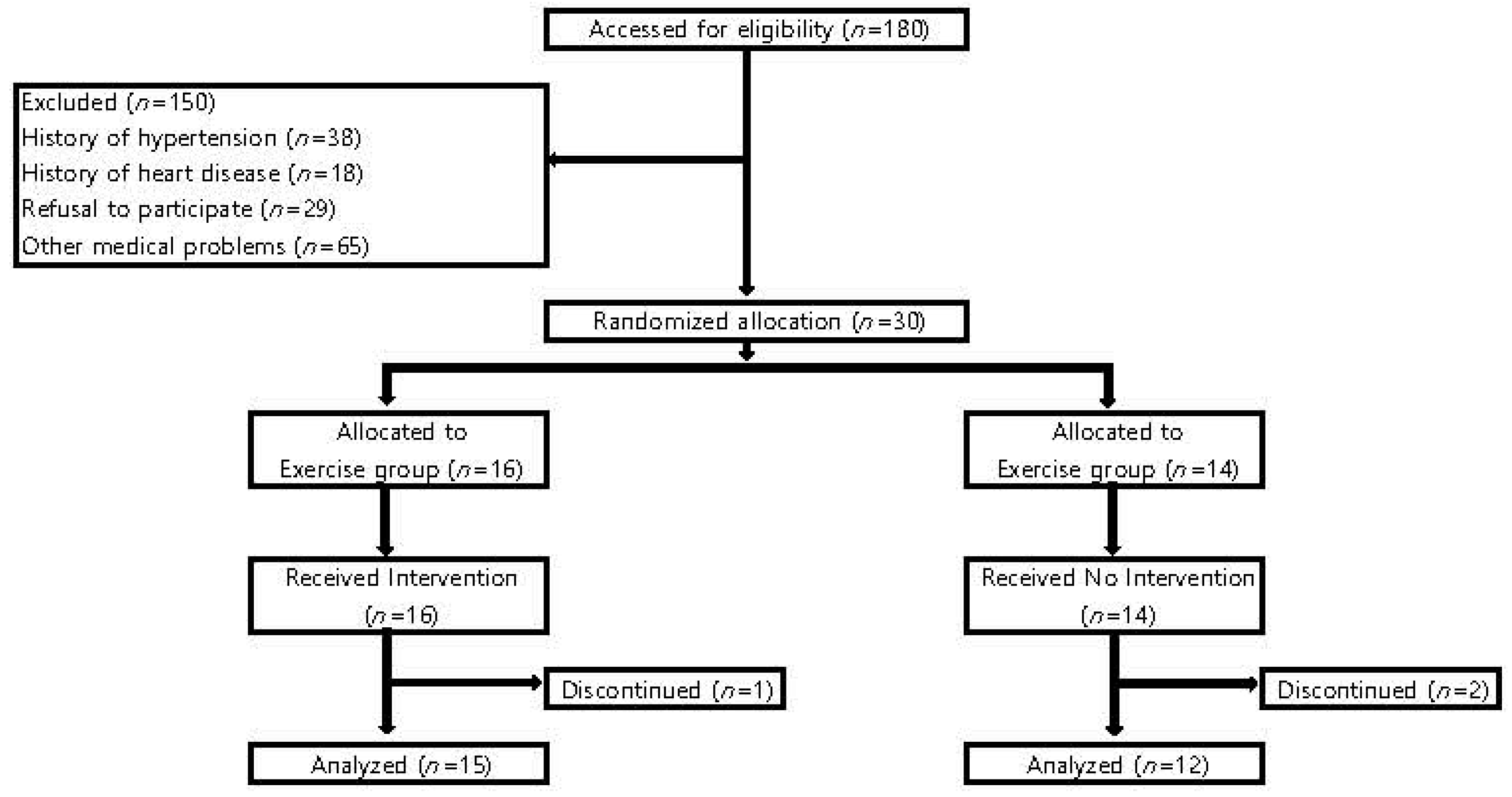
2.1. Study Design and Participants
2.2. Elastic Band Exercise
2.3. Measurement of Body Composition
2.4. Measurement of Blood Pressure
2.5. Measurement of Physical Activity
2.6. Measurement of Functional Fitness
2.6.1. Muscular Strength
2.6.2. Muscular Endurance
2.6.3. Flexibility
2.6.4. Balance
2.7. Statistical Analysis
3. Results
4. Discussion
4.1. Blood Pressure Responses
4.2. Functional Fitness
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Social Indicators in 2014. Available online: File:///C:/Users/MDPI/AppData/Local/Temp/si2014.pdf (accessed on 24 August 2018).
- Choi, J.Y.; Yang, K.; Chu, S.H.; Youm, Y.; Kim, H.C.; Park, Y.R.; Son, Y.J. Social activities and health-related quality of life in rural older adults in South Korea: A 4-year longitudinal analysis. Int. J. Environ. Res. Public Health 2020, 17, 5553. [Google Scholar]
- Lin, Y.-T.; Chen, M.; Ho, C.-C.; Lee, T.-S. Relationships among Leisure Physical Activity, Sedentary Lifestyle, Physical Fitness, and Happiness in Adults 65 Years or Older in Taiwan. Int. J. Environ. Res. Public Health 2020, 17, 5235. [Google Scholar]
- Tu, P.-C.; Cheng, W.-C.; Hou, P.-C.; Chang, Y.-S. Effects of Types of Horticultural Activity on the Physical and Mental State of Elderly Individuals. Int. J. Environ. Res. Public Health 2020, 17, 5225. [Google Scholar]
- American College of Sports Medicine; Chodzko-Zajko, W.J.; Proctor, D.N.; Singh, F.M.A.; Minso, C.T.; Nigg, C.R.; Salem, G.J.; Skinner, J.S. American College of Sports Medicine Position Stand. Exercise and Physical Activity for Older Adults. Med. Sci. Sports Exerc. 2009, 41, 1510–1530. [Google Scholar]
- Huang, G.; Shi, X.; Davis-Brezette, J.A.; Osness, W.H. Resting heart rate changes after endurance training in older adults: A meta-analysis. Med. Sci. Sports Exerc. 2005, 37, 1381–1386. [Google Scholar]
- Paoli, A.; Moro, T.; Marcolin, G.; Neri, M.; Bianco, A.; Palma, A.; Grimaldi, K. High-Intensity Interval Resistance Training (HIRT) Influences Resting Energy Expenditure and Respiratory Ratio in Non-Dieting Individuals. J. Transl. Med. 2012, 10, 237. [Google Scholar]
- Giné, G.M.; Guerra, M.; Unnithan, V.B. The effect of functional circuit training on self-reported fear of falling and health status in a group of physically frail older individuals: A randomized controlled trial. Aging Clin. Exp. Res. 2013, 25, 329–336. [Google Scholar]
- Patterson, R.; Jansen, C.W.S.; Hogan, H.A.; Nassif, M.D. Material Properties of Thera-Band Tubing. Phys. Ther. 2001, 81, 1437–1445. [Google Scholar] [CrossRef]
- Galvão, D.A.; Taaffe, D.R. Resistance Exercise Dosage in Older Adults: Single- versus Multiset Effects on Physical Performance and Body Composition. J. Am. Geriatr. Soc. 2005, 53, 2090–2097. [Google Scholar] [CrossRef]
- Park, S.; Sunoo, S. The effects of elastic band training on blood pressure, blood lipids concentration and ADL (activities of daily living) of elderly women by hypertensive for 10 weeks. Korean J. Phys. Edu. 2003, 13, 115–127. [Google Scholar]
- Kim, H.G.; Nam, H.K. The effect of thera band exercise on muscular flexibility, balance ability, muscular strength in elderly women. J. Korean Acad. Community Health Nurs. 2011, 22, 451–457. [Google Scholar]
- Figueroa, A.; Park, S.Y.; Seo, D.Y.; Sanchez-Gonzalez, M.A.; Baek, Y.H. Combined resistance and endurance exercise training improves arterial stiffness, blood pressure, and muscle strength in postmenopausal women. Menopause 2011, 18, 980–984. [Google Scholar] [CrossRef]
- Damush, T.M.; Damush, J. The effects of strength training on strength hand health-related quality of life in older adult women. J. Am. Geriatr. Soc. 1999, 39, 705–710. [Google Scholar]
- Centers for Disease Control and Prevention. Adult participation in aerobic and muscle-strengthening physical activities—United States, 2011. Morb. Mortal. Wkly. Rep. 2013, 62, 326–330. [Google Scholar]
- Moschny, A.; Platen, P.; Klaaßen-Mielke, R.; Trampisch, U.; Hinrichs, T. Barriers to physical activity in older adults in Germany: A cross-sectional study. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 121. [Google Scholar] [CrossRef] [Green Version]
- Jancey, J.; Howat, P.A.; Lee, A.; Clarke, A.; Shilton, T.; Fisher, J.; Iredell, H. Effective Recruitment and Retention of Older Adults in Physical Activity Research: PALS Study. Am. J. Health Behav. 2006, 30, 626–635. [Google Scholar] [CrossRef]
- Buch, A.; Kis, O.; Carmeli, E.; Keinan-Boker, L.; Berner, Y.; Barer, Y.; Shefer, G.; Marcus, Y.; Stern, N. Circuit resistance training is an effective means to enhance muscle strength in older and middle aged adults. Ageing Res. Rev. 2017, 37, 16–27. [Google Scholar] [CrossRef]
- Batrakoulis, A.; Loules, G.; Georgakouli, K.; Tsimeas, P.; Draganidis, D.; Chatzinikolaou, A.; Papanikolaou, K.; Deli, C.K.; Syrou, N.; Comoutos, N.; et al. High-intensity interval neuromuscular training promotes exercise behavioral regulation, adherence and weight loss in inactive obese women. Eur. J. Sport Sci. 2019, 16, 1–10. [Google Scholar] [CrossRef]
- Myers, T.R.; Schneider, M.G.; Schmale, M.S.; Hazell, T.J. Whole-Body Aerobic Resistance Training Circuit Improves Aerobic Fitness and Muscle Strength in Sedentary Young Females. J. Strength Cond. Res. 2015, 29, 1592–1600. [Google Scholar]
- Takeshima, N.; Rogers, M.E.; Islam, M.M.; Yamauchi, T.; Watanabe, E.; Okada, A. Effect of concurrent aerobic and resistance circuit exercise training on fitness in older adults. Eur. J. Appl. Physiol. 2004, 93, 173–182. [Google Scholar]
- American College of Sports Medicine. ACSM’s Guidelines for Exercise Testing and Prescription, 10th ed.; Lippincott, Williams & Wilkins: Philadelphia, PA, USA, 2018. [Google Scholar]
- Pollock, M.L.; Franklin, B.A.; Balady, G.J.; Chaitman, B.L.; Fleg, J.L.; Fletcher, B.; Limacher, M.; PiñaI, L.; Stein, R.A.; Williams, M.; et al. Resistance Exercise in Individuals with and without Cardiovascular Disease. Circulation 2000, 101, 828–833. [Google Scholar] [CrossRef]
- Rogers, M.E.; Sherwood, H.S.; Rogers, N.L.; Bohlken, R.M. Effects of Dumbbell and Elastic Band Training on Physical Function in Older Inner-City African-American Women. Women Health 2002, 36, 33–41. [Google Scholar] [CrossRef]
- Gorman, E.; Hanson, H.M.; Yang, P.H.; Khan, K.M.; Liu-Ambrose, T.; Ashe, M.C. Accelerometry analysis of physical activity and sedentary behavior in older adults: A systematic review and data analysis. Eur. Rev. Aging Phys. Act. 2013, 11, 35–49. [Google Scholar] [CrossRef] [Green Version]
- Jones, C.; Rikli, R. The application of Fullerton’s Functional Fitness Test for older adults in a group setting. Sci. Sports 2000, 15, 194–197. [Google Scholar] [CrossRef]
- Ramos, J.S.; Dalleck, L.C.; Tjonna, A.E.; Beetham, K.S.; Coombes, J.S. The Impact of High-Intensity Interval Training Versus Moderate-Intensity Continuous Training on Vascular Function: A Systematic Review and Meta-Analysis. Sports Med. 2015, 45, 679–692. [Google Scholar] [CrossRef]
- Currie, K.D.; Bailey, K.J.; Jung, M.E.; McKelvie, R.S.; Macdonald, M.J. Effects of resistance training combined with moderate-intensity endurance or low-volume high-intensity interval exercise on cardiovascular risk factors in patients with coronary artery disease. J. Sci. Med. Sport 2015, 18, 637–642. [Google Scholar] [CrossRef] [Green Version]
- Choi, M.; Ha, S.; Kim, D. Effects of elastic band exercise on body composition, blood lipids and AMPK in the elderly women. J. Korean Appl. Sci. Tech. 2019, 36, 995–1007. [Google Scholar]
- Kato, M.; Green, F.N.; Hotta, K.; Tsukamoto, T.; Kurita, Y.; Kubo, A.; Takagi, H. The Efficacy of Stretching Exercises on Arterial Stiffness in Middle-Aged and Older Adults: A Meta-Analysis of Randomized and Non-Randomized Controlled Trials. Int. J. Environ. Res. Public Health 2020, 17, 5643. [Google Scholar] [CrossRef]
- Jain, S.; Khera, R.; Corrales-Medina, V.; Townsend, R.R.; Chirinos, J.A. Inflammation and arterial stiffness in humans. Atherosclerosis 2014, 237, 381–390. [Google Scholar] [CrossRef]
- Nasi, M.; Patrizi, G.; Pizzi, C.; Landolfo, M.; Boriani, G.; Cas, A.D.; Cicero, A.F.; Fogacci, F.; Rapezzi, C.; Sisca, G.; et al. The role of physical activity in individuals with cardiovascular risk factors. J. Cardiovasc. Med. 2019, 20, 631–639. [Google Scholar]
- Kim, H.S. Functional fitness and cardiorespiratory response to exercise training with dumbbell in the elderly. Korean J. Phys. Edu. 2000, 39, 432–442. [Google Scholar]
- Fukumoto, Y.; Tateuchi, H.; Ikezoe, T.; Tsukagoshi, R.; Akiyama, H.; So, K.; Kuroda, Y.; Ichihashi, N. Effects of high-velocity resistance training on muscle function, muscle properties, and physical performance in individuals with hip osteoarthritis: A randomized controlled trial. Clin. Rehabil. 2013, 28, 48–58. [Google Scholar] [CrossRef]
- Kabiri, S.; Halabchi, F.; Angoorani, H.; Yekaninejad, M.S. Comparison of three modes of aerobic exercise combined with resistance training on the pain and function of patients with knee osteoarthritis: A randomized controlled trial. Phys. Ther. Sport 2018, 32, 22–28. [Google Scholar] [CrossRef]
- Tanaka, R.; Ozawa, J.; Kito, N.; Moriyama, H. Efficacy of strengthening or aerobic exercise on pain relief in people with knee osteoarthritis: A systematic review and meta-analysis of randomized controlled trials. Clin. Rehabil. 2013, 27, 1059–1071. [Google Scholar] [CrossRef]
- Lee, H.J.; Han, S.W. Effects of lower extremity muscular strengthening exercise using elastic resistance on balance on elderly women. J. Korean Acad. Community Health Nurs. 2009, 20, 59–66. [Google Scholar]
- Rooks, D.S.; Kiel, D.P.; Parsons, C.; Hayes, W.C. Self-paced resistance training and walking exercise in community-dwelling older adults: Effects on neuromotor performPance. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 1997, 52, M161–M168. [Google Scholar] [CrossRef]
- Wilder, R.P.; Greene, J.A.; Winters, K.L.; Long, W.B.; Gubler, K.D.; Edlich, R.F. Physical Fitness Assessment: An Update. J. Autom. Inf. Sci. 2006, 16, 193–204. [Google Scholar] [CrossRef]
- García-Garro, P.A.; Hita-Contreras, F.; Martínez-Amat, A.; Pt, A.A.; Jiménez-García, J.D.; Cruz-Díaz, D.; Aibar-Almazán, A. Effectiveness of a Pilates Training Program on Cognitive and Functional Abilities in Postmenopausal Women. Int. J. Environ. Res. Public Health 2020, 17, 3580. [Google Scholar] [CrossRef]
- Barbosa, A.R.; Santarém, J.M.; Filho, W.J.; Marucci, M.F.N. Effects of resistance training on the sit-and-reach test in elderly women. J. Strength Cond. Res. 2002, 16, 14–18. [Google Scholar]
- Lord, S.R.; Castell, S. Physical activity program for older persons: Effect on balance, strength, neuromuscular control, and reaction time. Arch. Phys. Med. Rehabil. 1994, 75, 648–652. [Google Scholar] [CrossRef]
- Sandler, R.B.; Burdett, R.; Zaleskiewicz, M.; Sprowls-Repcheck, C.; Harwell, M. Muscular strength as an indicator of the habitual level of physical activity. Med. Sci. Sports Exerc. 1991, 23, 1375–1381. [Google Scholar]
- Coquart, J.B.; Garcin, M.; Parfitt, G.; Tourny-Chollet, C.; Eston, R.G. Prediction of Maximal or Peak Oxygen Uptake from Ratings of Perceived Exertion. Sports Med. 2014, 44, 563–578. [Google Scholar] [CrossRef]
- AlGhatrif, M.; Lakatta, E.G. The conundrum of arterial stiffness, elevated blood pressure, and aging. Curr. Hypertens. Rep. 2015, 17, 12. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Variables | EG (n = 15) | CTG (n = 12) | p |
|---|---|---|---|
| Age (years) | 75.1 ± 1.4 | 72.3 ± 1.4 | 0.060 |
| Fat mass (kg) | 19.4 ± 1.5 | 21.3 ± 0.8 | 0.059 |
| Fat free mass (kg) | 24.1 ± 1.1 | 26.8 ± 1.3 | 0.062 |
| Body mass index (kg/m2) | 25.3 ± 0.5 | 25.5 ± 0.4 | 0.088 |
| Systolic blood pressure (mmHg) | 126.8 ± 2.7 | 130.4 ± 3.3 | 0.163 |
| Diastolic blood pressure (mmHg) | 78.7 ± 1.9 | 78.6 ± 3.1 | 0.456 |
| Physical activity (steps) | 5414.1 ± 2.3 | 5368.3 ± 2.5 | 0.487 |
| Variables | Groups | Pre-Test | Post-Test | ∆(%) | F | p |
|---|---|---|---|---|---|---|
| Systolic blood pressure (mmHg) | EG (n = 15) | 126.8 ± 2.2 | 121.3 ± 1.7 #,† | −5.5 | 8.240 | 0.006 * |
| CTG (n = 12) | 130.4 ± 3.3 | 135.7 ± 2.8 | 4.1 | |||
| Diastolic blood pressure (mmHg) | EG (n = 15) | 78.7 ± 1.7 | 75.3 ± 1.9 #,† | −5.0 | 10.454 | 0.003 * |
| CTG (n = 12) | 78.6 ± 3.1 | 80.2 ± 2.3 | 2.0 | |||
| Mean arterial pressure (mmHg) | EG (n = 15) | 95.7 ± 1.5 | 90.8 ± 1.6 #,† | −5.2 | 11.720 | 0.001 * |
| CTG (n = 12) | 96.5 ± 3.1 | 100.0 ± 2.0 | 3.6 | |||
| Pulse pressure (mmHg) | EG (n = 15) | 51.5 ± 2.0 | 46.9 ± 1.9 #,† | −8.9 | 7.384 | 0.010 * |
| CTG (n = 12) | 53.7 ± 1.4 | 53.5 ± 3.2 | −0.4 |
| Variables | Groups | Pre-Test | Post-Test | ∆(%) | F | p |
|---|---|---|---|---|---|---|
| Grip strength (kg) | EG (n = 15) | 24.6 ± 1.6 | 28.3 ± 2.1 #,† | 14.9 | 5.490 | 0.026 * |
| CTG (n = 12) | 21.7 ± 1.2 | 22.2 ± 1.2 | 2.7 | |||
| Chair stand (count/30 s) | EG (n = 15) | 14.2 ± 1.3 | 17.8 ± 1.3 # | 25.4 | 2.197 | 0.149 |
| CTG (n = 12) | 15.8 ± 1.0 | 17.3 ± 0.8 | 10.1 | |||
| Sit and reach (cm) | EG (n = 15) | 8.9 ± 1.7 | 11.0 ± 1.7 #,† | 24.8 | 4.250 | 0.048 * |
| CTG (n = 12) | 15.3 ± 2.3 | 15.0 ± 1.7 | −1.5 | |||
| One-leg stance (s) | EG (n = 15) | 26.0 ± 6.4 | 33.8 ± 5.9 #,† | 29.8 | 7.888 | 0.009 * |
| CTG (n = 12) | 22.4 ± 5.5 | 21.6 ± 5.4 | −3.8 | |||
| Timed up and go (s) | EG (n = 15) | 12.2 ± 3.5 | 6.9 ± 0.5 | −43.5 | 2.275 | 0.142 |
| CTG (n = 12) | 8.1 ± 0.7 | 8.0 ± 0.6 | −1.8 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, H.-M.; Hurr, C.; Kim, S. Effects of Elastic Band Exercise on Functional Fitness and Blood Pressure Response in the Healthy Elderly. Int. J. Environ. Res. Public Health 2020, 17, 7144. https://doi.org/10.3390/ijerph17197144
Choi H-M, Hurr C, Kim S. Effects of Elastic Band Exercise on Functional Fitness and Blood Pressure Response in the Healthy Elderly. International Journal of Environmental Research and Public Health. 2020; 17(19):7144. https://doi.org/10.3390/ijerph17197144
Chicago/Turabian StyleChoi, Hyun-Min, Chansol Hurr, and Sukwon Kim. 2020. "Effects of Elastic Band Exercise on Functional Fitness and Blood Pressure Response in the Healthy Elderly" International Journal of Environmental Research and Public Health 17, no. 19: 7144. https://doi.org/10.3390/ijerph17197144