Risk of Acquired Cholesteatoma and External Auditory Canal Stenosis in Traumatic Brain Injury: A Nationwide Population-Based Cohort Study

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources
2.2. Variable Definitions
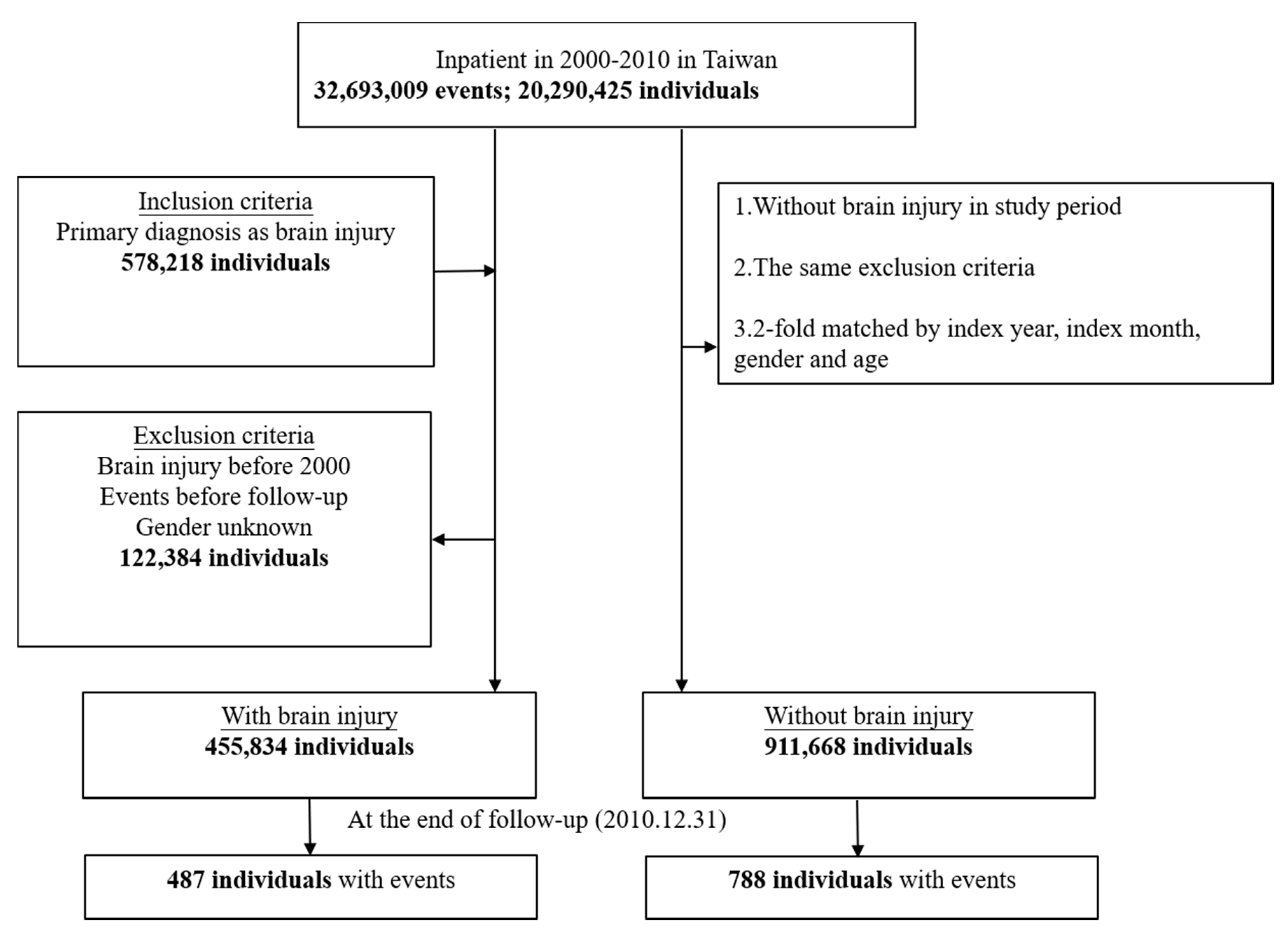
2.3. Study Sample Selection and Tracking
2.4. Statistical Analysis
2.5. Data Availability
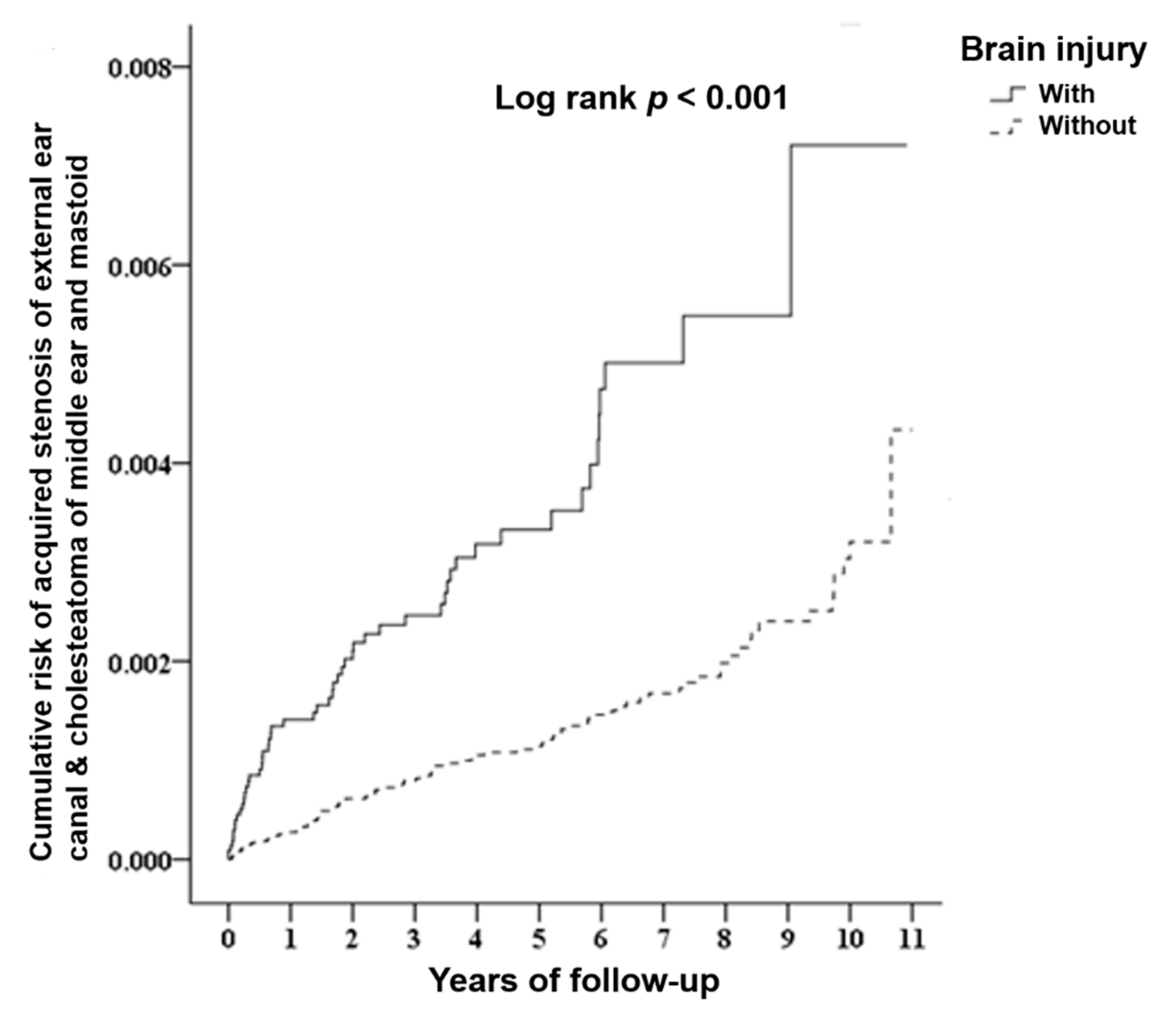
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Greinwald, J.H., Jr.; Kelly, K.E.; Tami, T.A. Temporal bone and skull base trauma. Neurotology 2005, 1070–1088. [Google Scholar] [CrossRef]
- Dahiya, R.; Keller, J.D.; Litofsky, N.S.; Bankey, P.E.; Bonassar, L.J.; Megerian, C.A. Temporal bone fractures: Otic capsule sparing versus otic capsule violating clinical and radiographic considerations. J. Trauma. 1999, 47, 1079. [Google Scholar] [CrossRef] [PubMed]
- Luong, A.; Roland, P.S. Acquired external auditory canal stenosis: Assessment and management. Curr. Opin. Otolaryngol. Head Neck Surg. 2005, 13, 273–276. [Google Scholar] [CrossRef] [PubMed]
- Brookes, G.B.; Graham, M.D. Post-traumatic cholesteatoma of the external auditory canal. Laryngoscope 1984, 94, 667–670. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.C.; Lin, C.L.; Huang, W.Y.; Shangkuan, W.C.; Kang, B.H.; Chu, Y.H.; Lee, J.C.; Fan, H.C.; Kao, C.H. The use of adjunctive traditional Chinese medicine therapy and survival outcome in patients with head and neck cancer: A nationwide population-based cohort study. QJM 2015, 108, 959–965. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shangkuan, W.C.; Lin, H.C.; Shih, C.P.; Cheng, C.A.; Fan, H.C.; Chung, C.H.; Lin, F.H.; Tsao, C.H.; Chien, W.C. Increased long-term risk of hearing loss in patients with traumatic brain injury: A nationwide population-based study. Laryngoscope 2017, 127, 2627–2635. [Google Scholar] [CrossRef] [PubMed]
- De Silva, M.J.; Roberts, I.; Perel, P.; Edwards, P.; Kenward, M.G.; Fernandes, J.; Shakur, H.; Patel, V. Patient outcome after traumatic brain injury in high-, middle-and low-income countries: Analysis of data on 8927 patients in 46 countries. Int. J. Epidemiol. 2009, 38, 452–458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Louw, L. Acquired cholesteatoma pathogenesis: Stepwise explanations. J. Laryngol. Otol. 2010, 124, 587–593. [Google Scholar] [CrossRef] [PubMed]
- Ghajar, J. Traumatic brain injury. Lancet 2000, 356, 923–929. [Google Scholar] [CrossRef]
- Becker, B.C.; Tos, M. Postinflammatory acquired atresia of the external auditory canal: Treatment and results of surgery over 27 years. Laryngoscope 1998, 108, 903–907. [Google Scholar] [CrossRef] [PubMed]
- Goldfarb, A.; Gross, M.; Eliashar, R.; Elidan, J. Middle cranial fossa cholesteatoma following blast trauma. Ann. Otol. Rhinol. Laryngol. 2001, 110, 1084–1086. [Google Scholar] [CrossRef] [PubMed]
- Reineke, U.; Ebmeyer, J.; Sudhoff, H. Acquired postinflammatory stenosis of the external auditory canal. Laryngo Rhino Otologie 2010, 89, 235. [Google Scholar] [CrossRef] [PubMed]
- McKennan, K.X.; Chole, R.A. Traumatic external auditory canal atresia. Am. J. Otol. 1992, 13, 80–81. [Google Scholar] [CrossRef] [PubMed]
- Magliulo, G. Acquired atresia of the external auditory canal: Recurrence and long-term results. Ann. Otol. Rhinol. Laryngol. 2009, 118, 345–349. [Google Scholar] [CrossRef] [PubMed]
- Lozano, D.; Gonzales-Portillo, G.S.; Acosta, S.; Pena, I.; Tajiri, N.; Kaneko, Y.; Borlongan, C. Neuroinflammatory responses to traumatic brain injury: Etiology, clinical consequences, and therapeutic opportunities. Neuropsychiatr. Dis. Treat. 2015, 11, 97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Louw, L. Acquired cholesteatoma: Summary of the cascade of molecular events. J. Laryngol. Otol. 2013, 127, 542–549. [Google Scholar] [CrossRef] [PubMed]
- Maniu, A.; Harabagiu, O.; Perde Schrepler, M.; Cătană, A.; Fănuţă, B.; Mogoantă, C.A. Molecular biology of cholesteatoma. Rom. J. Morphol. Embryol. 2014, 55, 7–13. [Google Scholar] [PubMed]
- Jayakumar, A.R.; Tong, X.Y.; Ruiz-Cordero, R.; Bregy, A.; Bethea, J.R.; Bramlett, H.M.; Norenberg, M.D. Activation of NF-κB mediates astrocyte swelling and brain edema in traumatic brain injury. J. Neurotrauma 2014, 31, 1249–1257. [Google Scholar] [CrossRef] [PubMed]
- Hamajima, Y.; Komori, M.; Preciado, D.A.; Choo, D.I.; Moribe, K.; Murakami, S.; Ondrey, F.G.; Lin, J. The role of inhibitor of DNA-binding (Id1) in hyperproliferation of keratinocytes: The pathological basis for middle ear cholesteatoma from chronic otitis media. Cell Prolif. 2010, 43, 457–463. [Google Scholar] [CrossRef] [PubMed]
- Vennix, P.P.; Kuijpers, W.; Tonnaer, E.L.; Peters, T.A.; Ramaekers, F.C. Cytokeratins in induced epidermoid formations and cholesteatoma lesions. Arch. Otolaryngol. Head Neck Surg. 1990, 116, 560–565. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Brain Injury | Total | With | Without | p | |||
|---|---|---|---|---|---|---|---|
| Variables | n | % | n | % | n | % | |
| Total | 1367,502 | 455,834 | 33.33 | 911,668 | 66.67 | ||
| Events | <0.001 | ||||||
| Without | 1366,227 | 99.91 | 455,347 | 99.89 | 910,880 | 99.91 | |
| With | 1275 | 0.09 | 487 | 0.11 | 788 | 0.09 | |
| Subgroup of events | <0.001 | ||||||
| Without | 1366,227 | 99.91 | 455,347 | 99.89 | 910,880 | 99.91 | |
| Acquired stenosis of external ear canal | 355 | 0.03 | 166 | 0.04 | 189 | 0.02 | |
| Cholesteatoma of middle ear and mastoid | 883 | 0.06 | 304 | 0.07 | 579 | 0.06 | |
| Both | 37 | 0.00 | 17 | 0.00 | 20 | 0.00 | |
| Gender | 0.999 | ||||||
| Male | 811,257 | 59.32 | 270,419 | 59.32 | 540,838 | 59.32 | |
| Female | 556,245 | 40.68 | 185,415 | 40.68 | 370,830 | 40.68 | |
| Age (years) (mean ± SD) | 44.41 ± 24.61 | 42.90 ± 22.18 | 45.17 ± 25.71 | 0.007 | |||
| Low-income | <0.001 | ||||||
| Without | 1344,640 | 98.33 | 447,731 | 98.22 | 896,909 | 98.38 | |
| With | 22,862 | 1.67 | 8103 | 1.78 | 14,759 | 1.62 | |
| Catastrophic illness | <0.001 | ||||||
| Without | 1193,522 | 87.45 | 414,727 | 91.52 | 778,795 | 85.43 | |
| With | 171,280 | 12.55 | 38,407 | 8.48 | 132,873 | 14.57 | |
| CCI (mean ± SD) | 0.84 ± 2.25 | 0.42 ± 1.43 | 1.05 ± 2.53 | <0.001 | |||
| Cause of injury | <0.001 | ||||||
| Traffic injuries | 282,937 | 61.50 | 233,142 | 66.73 | 49,795 | 44.99 | |
| Poisoning | 1833 | 0.40 | 401 | 0.11 | 1432 | 1.29 | |
| Falls | 95,781 | 20.82 | 74,447 | 21.31 | 21,334 | 19.27 | |
| Burns and fires | 519 | 0.11 | 40 | 0.01 | 479 | 0.43 | |
| Drowning | 122 | 0.03 | 24 | 0.01 | 98 | 0.09 | |
| Suffocation | 636 | 0.14 | 24 | 0.01 | 612 | 0.55 | |
| Crushing/Cutting/Piercing | 27,002 | 5.87 | 13,773 | 3.94 | 13,229 | 11.95 | |
| Other unintentional injuries | 22,822 | 4.96 | 5963 | 1.71 | 16,859 | 15.23 | |
| Suicide | 2055 | 0.45 | 248 | 0.07 | 1807 | 1.63 | |
| Homicide/Abuse | 25,162 | 5.47 | 20,872 | 5.97 | 4290 | 3.88 | |
| Intention unknown | 1174 | 0.26 | 422 | 0.12 | 752 | 0.68 | |
| Intentionality of injury | <0.001 | ||||||
| Unintentional injury | 382,674 | 93.89 | 295,298 | 93.64 | 87,376 | 94.76 | |
| Intentional injury | 0.00 | 6.11 | 20,050 | 6.36 | 4835 | 5.24 | |
| Urbanization level | <0.001 | ||||||
| High | 414,921 | 30.34 | 114,667 | 25.16 | 300,254 | 32.93 | |
| Middle | 585,726 | 42.83 | 189,281 | 41.52 | 396,445 | 43.49 | |
| Low | 366,855 | 26.83 | 151,886 | 33.32 | 214,969 | 23.58 | |
| Level of care | <0.001 | ||||||
| Hospital center | 419,434 | 30.67 | 111,842 | 24.54 | 307,592 | 33.74 | |
| Regional hospital | 555,404 | 40.61 | 201,180 | 44.13 | 354,224 | 38.85 | |
| Local hospital | 392,664 | 28.71 | 142,812 | 31.33 | 249,852 | 27.41 | |
| Surgery | <0.001 | ||||||
| Without | 854,414 | 62.48 | 313,931 | 68.87 | 540,483 | 59.29 | |
| With | 513,088 | 37.52 | 141,903 | 31.13 | 371,185 | 40.71 | |
| Length of days (mean ± SD) | 7.32 ± 9.60 | 7.54 ± 10.13 | 6.89 ± 8.41 | <0.001 | |||
| Medical costs (NT$) (mean ± SD) | 46,252.58 ± 84,924.68 | 48,896.69 ± 90,655.82 | 40,964.37 ± 71,818.28 | <0.001 | |||
| Prognosis | <0.001 | ||||||
| Survive | 1281,971 | 93.75 | 440,530 | 96.64 | 841,441 | 92.30 | |
| Mortality | 85,531 | 6.25 | 15,304 | 3.36 | 70,227 | 7.70 | |
| Variables | Crude HR | 95% CI | 95% CI | p | Adjusted HR | 95% CI | 95% CI | p |
|---|---|---|---|---|---|---|---|---|
| Brain injury | ||||||||
| Without | Reference | Reference | ||||||
| With | 2.827 | 2.518 | 3.174 | <0.001 | 2.742 | 2.380 | 3.160 | <0.001 |
| Gender | ||||||||
| Male | 1.121 | 1.003 | 1.253 | 0.044 | 1.152 | 1.029 | 1.290 | 0.014 |
| Female | Reference | Reference | ||||||
| Age (years) | 0.984 | 0.882 | 1.007 | 0.723 | 0.993 | 0.890 | 1.015 | 0.160 |
| Low-income | ||||||||
| Without | Reference | Reference | ||||||
| With | 0.848 | 0.579 | 1.241 | 0.396 | 1.334 | 0.910 | 1.957 | 0.140 |
| Catastrophic illness | ||||||||
| Without | Reference | Reference | ||||||
| With | 0.328 | 0.263 | 0.410 | <0.001 | 0.964 | 0.755 | 1.232 | 0.772 |
| CCI | 0.493 | 0.449 | 0.542 | <0.001 | 0.702 | 0.642 | 0.767 | <0.001 |
| Intentionality of injury | ||||||||
| Unintentional injury | Reference | Reference | ||||||
| Intentional injury | 0.814 | 0.539 | 1.229 | 0.327 | 0.779 | 0.516 | 1.176 | 0.234 |
| Urbanization level | ||||||||
| High | 3.318 | 2.760 | 3.989 | <0.001 | 1.660 | 1.347 | 2.045 | <0.001 |
| Middle | 2.657 | 2.219 | 3.181 | <0.001 | 1.706 | 1.408 | 2.066 | <0.001 |
| Low | Reference | Reference | ||||||
| Level of care | ||||||||
| Hospital center | 8.280 | 6.487 | 10.568 | <0.001 | 7.254 | 5.624 | 9.358 | <0.001 |
| Regional hospital | 3.994 | 3.114 | 5.123 | <0.001 | 4.253 | 3.311 | 5.462 | <0.001 |
| Local hospital | Reference | Reference | ||||||
| Surgery | ||||||||
| Without | Reference | Reference | ||||||
| With | 10.417 | 8.897 | 12.196 | <0.001 | 7.408 | 6.309 | 8.699 | <0.001 |
| Length of days | 0.962 | 0.954 | 0.971 | <0.001 | 0.984 | 0.975 | 0.993 | <0.001 |
| Medical costs (NT$) | 1.000 | 0.999 | 1.001 | 0.063 | Medical cost had collinearity with length of days | |||
| Brain Injury | With | Without | Ratio | Adjusted HR | 95%CI | 95%CI | p | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Variables | Event | PYs | Rate (per 105 PYs) | Event | PYs | Rate (per 105 PYs) | |||||
| Total | 487 | 671,019.80 | 72.58 | 788 | 2089,637.43 | 37.71 | 1.925 | 2.742 | 2.380 | 3.160 | <0.001 |
| Gender | |||||||||||
| Male | 294 | 367,891.58 | 79.91 | 453 | 1308,410.45 | 34.62 | 2.308 | 2.916 | 2.439 | 3.486 | <0.001 |
| Female | 193 | 303,128.22 | 63.67 | 335 | 781,226.98 | 42.88 | 1.485 | 2.403 | 1.898 | 3.043 | <0.001 |
| Low-income | |||||||||||
| Without | 479 | 653,341.38 | 73.32 | 769 | 2037,529.18 | 37.74 | 1.943 | 2.815 | 2.440 | 3.248 | <0.001 |
| With | 88 | 17,678.44 | 497.78 | 19 | 52,108.25 | 36.46 | 13.652 | 1.764 | 0.279 | 2.092 | 0.601 |
| Catastrophic illness | |||||||||||
| Without | 449 | 580,954.43 | 77.29 | 742 | 1698,403.77 | 43.69 | 1.769 | 2.659 | 2.298 | 3.078 | <0.001 |
| With | 38 | 90,065.37 | 42.19 | 46 | 391,233.66 | 11.76 | 3.588 | 4.448 | 2.511 | 7.881 | <0.001 |
| Cause of injury | |||||||||||
| Traffic injuries | 269 | 330,660.04 | 81.35 | 45 | 111,516.58 | 40.35 | 2.016 | 3.718 | 2.298 | 4.400 | <0.001 |
| Poisoning | 0 | 846.72 | 0.00 | 1 | 3465.09 | 28.86 | 0.000 | 0.000 | - | - | 0.936 |
| Falls | 59 | 114,645.04 | 51.46 | 10 | 50,033.79 | 19.99 | 2.575 | 4.308 | 2.172 | 8.543 | <0.001 |
| Burns and fires | 0 | 71.50 | 0.00 | 1 | 972.75 | 102.80 | 0.000 | 0.000 | - | - | 0.993 |
| Drowning | 0 | 63.78 | 0.00 | 0 | 142.27 | 0.00 | - | - | - | - | - |
| Suffocation | 0 | 43.58 | 0.00 | 1 | 1164.33 | 85.89 | 0.000 | 0.000 | - | - | 0.994 |
| Crushing/Cutting/Piercing | 16 | 19,105.02 | 83.75 | 21 | 25,836.71 | 81.28 | 1.030 | 1.952 | 0.957 | 3.980 | 0.066 |
| Other unintentional injuries | 5 | 8249.28 | 60.61 | 20 | 42,490.77 | 47.07 | 1.288 | 2.119 | 0.776 | 5.791 | 0.143 |
| Suicide | 0 | 479.98 | 0.00 | 3 | 4477.30 | 67.00 | 0.000 | 0.000 | - | - | 0.986 |
| Homicide / Abuse | 21 | 35,091.05 | 59.84 | 3 | 7653.63 | 39.20 | 1.527 | 2.758 | 0.803 | 9.475 | 0.107 |
| Intention unknown | 1 | 944.27 | 105.90 | 0 | 1774.84 | 0.00 | - | - | - | - | - |
| Intentionality of injury | |||||||||||
| Unintentional injury | 318 | 406,063.25 | 78.31 | 89 | 188,840.93 | 47.13 | 1.662 | 2.745 | 2.145 | 3.513 | <0.001 |
| Intentional injury | 20 | 33,727.89 | 59.30 | 4 | 11,337.65 | 35.28 | 1.681 | 2.576 | 0.841 | 7.889 | 0.098 |
| Urbanization level | |||||||||||
| High | 181 | 165,497.50 | 109.37 | 329 | 613,218.28 | 53.65 | 2.038 | 2.839 | 2.272 | 3.549 | <0.001 |
| Middle | 229 | 280,303.89 | 81.70 | 393 | 929,405.03 | 42.29 | 1.932 | 2.447 | 1.991 | 3.009 | <0.001 |
| Low | 77 | 225,218.41 | 34.19 | 69 | 546,951.12 | 12.62 | 2.710 | 3.743 | 2.487 | 5.633 | <0.001 |
| Level of care | |||||||||||
| Hospital center | 239 | 162,375.45 | 147.19 | 472 | 667,553.56 | 70.71 | 2.082 | 2.764 | 2.281 | 3.350 | <0.001 |
| Regional hospital | 213 | 311,469.03 | 68.39 | 280 | 916,963.67 | 30.54 | 2.240 | 2.611 | 2.082 | 3.275 | <0.001 |
| Local hospital | 35 | 197,175.33 | 17.75 | 36 | 505,120.20 | 7.13 | 2.491 | 3.425 | 1.919 | 6.112 | <0.001 |
| Surgery | |||||||||||
| Without | 111 | 402,565.91 | 27.57 | 69 | 1329,927.27 | 5.19 | 5.315 | 5.750 | 3.894 | 8.490 | <0.001 |
| With | 376 | 268,453.89 | 140.06 | 719 | 759,710.16 | 94.64 | 1.480 | 2.388 | 2.047 | 2.789 | <0.001 |
| Brain Injury | With | Without | Ratio | Adjusted HR | 95%CI | 95%CI | p | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Subgroup of Events | Event | PYs | Rate (per 105 PYs) | Event | PYs | Rate (per 105 PYs) | |||||
| Total | 487 | 671,019.80 | 72.58 | 788 | 2089,637.43 | 37.71 | 1.925 | 2.742 | 2.380 | 3.160 | <0.001 |
| Acquired stenosis of external ear canal | 166 | 671,019.80 | 24.74 | 189 | 2089,637.43 | 9.04 | 2.735 | 3.549 | 2.713 | 4.644 | <0.001 |
| Cholesteatoma of middle ear and mastoid | 304 | 671,019.80 | 45.30 | 579 | 2089,637.43 | 27.71 | 1.635 | 1.777 | 1.494 | 2.114 | <0.001 |
| Both | 17 | 671,019.80 | 2.53 | 20 | 2089,637.43 | 0.96 | 2.647 | 4.099 | 1.001 | 21.781 | 0.049 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, H.-C.; Shih, C.-P.; Chen, H.-C.; Cheng, C.-A.; Huang, Y.-S.; Lin, C.-S.; Chung, C.-H.; Huang, B.-R.; Lee, J.-C.; Shangkuan, W.-C.; et al. Risk of Acquired Cholesteatoma and External Auditory Canal Stenosis in Traumatic Brain Injury: A Nationwide Population-Based Cohort Study. Int. J. Environ. Res. Public Health 2020, 17, 6624. https://doi.org/10.3390/ijerph17186624
Lin H-C, Shih C-P, Chen H-C, Cheng C-A, Huang Y-S, Lin C-S, Chung C-H, Huang B-R, Lee J-C, Shangkuan W-C, et al. Risk of Acquired Cholesteatoma and External Auditory Canal Stenosis in Traumatic Brain Injury: A Nationwide Population-Based Cohort Study. International Journal of Environmental Research and Public Health. 2020; 17(18):6624. https://doi.org/10.3390/ijerph17186624
Chicago/Turabian StyleLin, Hung-Che, Cheng-Ping Shih, Hsin-Chien Chen, Chun-An Cheng, Yuahn-Sieh Huang, Chen-Shien Lin, Chi-Hsian Chung, Bor-Rong Huang, Jih-Chin Lee, Wei-Chuan Shangkuan, and et al. 2020. "Risk of Acquired Cholesteatoma and External Auditory Canal Stenosis in Traumatic Brain Injury: A Nationwide Population-Based Cohort Study" International Journal of Environmental Research and Public Health 17, no. 18: 6624. https://doi.org/10.3390/ijerph17186624